CURRENT THERAPY FOR IGA NEPHROPATHY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

BRIEF REVIEW www.jasn.org
Current Therapy for IgA Nephropathy
Jürgen Floege and Frank Eitner
Division of Nephrology and Immunology, RWTH University of Aachen, Aachen, Germany
ABSTRACT
IgA nephropathy (IgAN) is a very common glomerulonephritis worldwide. In this are detected in 5 to 20% of all cases. Full-
review, we discuss therapeutic options in four clinical scenarios encountered in blown IgAN with glomerular IgA plus C3
patients with IgAN: first is the patient with minor urinary abnormalities where the deposits as well as mesangioproliferative
mainstay of treatment is long-term, regular follow-up to detect renal progression changes were noted in 1.6% of Japanese
and hypertension. Second is the typical patient presenting with microhematuria, graft kidneys before implantation.2 Thus,
significant but non-nephrotic proteinuria, hypertension, and variable degrees of the majority of patients with IgAN must
renal failure. Here the mainstay of treatment is optimized supportive care. If this run a clinically inconspicuous course
does not lower proteinuria below 1 g/d, corticosteroid monotherapy may be and spontaneous remissions of the dis-
effective, as long as the GFR is above 50 ml/min. There is insufficient data to ease must exist. Indeed, in Chinese IgAN
advocate the use of other immunosuppressive drugs or even combination therapy patients with isolated microhematuria
in such patients. Third is the atypical patient with overt nephrotic syndrome, or followed for up to 12 years, microhema-
acute or rapidly progressive kidney injury where a possible vasculitic form of IgAN turia disappeared in 14%, and in less
should be sought and, if present, treated with immunosuppression. In other than one third, proteinuria increased
atypical patients with secondary IgAN, treatment should target the underlying above 1 g/d or GFR fell.3 Repeat biopsy
primary disease. And fourth is the transplanted patient with recurrent IgAN where studies confirm that glomerular changes,
the mainstay of treatment is optimized supportive care. including IgA deposits, can completely
disappear spontaneously or after treat-
J Am Soc Nephrol 22: 1785–1794, 2011. doi: 10.1681/ASN.2011030221
ment in both native4 – 6 and transplanted
kidneys.7,8 These studies have two im-
portant clinical implications: IgAN—at
Although IgA nephropathy (IgAN) is the who requires close follow-up and treat- least in early stages— can be spontane-
most common noninfectious glomeru- ment; atypical manifestations including ously reversible and patients with iso-
lonephritis worldwide, there are remark- overt nephrotic syndrome, acute or rap- lated urinary abnormalities, particular
ably few randomized controlled trials idly progressive kidney injury, or sec- those in whom IgAN has been con-
and very rarely do patient numbers ex- ondary forms of IgAN; and finally recur- firmed, need to be followed long-term, as
ceed 200. Consequently, most guidelines rent IgAN after renal transplantation. A there may be progressive disease in ap-
relating to IgAN in the KDIGO Clinical synopsis of our suggested approach is proximately 30%. Although such long-
Practice Guideline for Glomerulonephritis given in Figure 1. Supportive care term follow-up is often recommended,
(to be published in late 2011) will be throughout the manuscript refers to especially in young patients, at least in our
based on a low to very low level of evi- measures listed in Table 1, which are not experience it is rarely maintained through-
dence and, in many cases, suggestions specific for IgAN and which have been out the necessary 10 or more years. Auto-
cannot even be offered. Thus, the major- shown to retard progression of chronic
ity of patients will continue to be treated glomerular diseases.
based largely on opinion. This review will Published online ahead of print. Publication date
attempt to incorporate evidence-based available at www.jasn.org.
recommendations, but it will also cover THE SILENT MAJORITY Correspondence: Dr. Jürgen Floege, Department
areas founded exclusively on opinion. of Nephrology and Clinical Immunology, RWTH Uni-
We have based the review on four classi- Most IgAN Likely Goes Unnoticed, versity Hospital Aachen, Pauwelsstr. 30, 52074
Aachen, Germany. Phone: ⫹49 241 80 89530; Fax:
cal clinical scenarios encountered in Is Very Benign, and Does Not Need ⫹49 241 80 82446; E-mail: juergen.floege@rwth-
IgAN patients: that is, the coincidental Treatment aachen.de
discovery of minor urinary abnormali- In autopsy series1 and zero-hour allo- Copyright © 2011 by the American Society of
ties (the majority); the typical patient graft biopsies,2 glomerular IgA deposits Nephrology
J Am Soc Nephrol 22: 1785–1794, 2011 ISSN : 1046-6673/2210-1785 1785
BRIEF REVIEW www.jasn.org
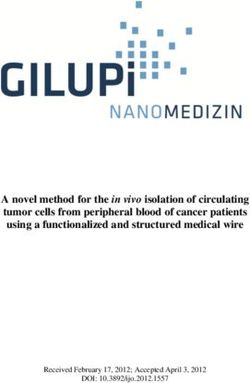
BIOPSY-PROVEN, PRIMARY IgAN
LOW RISK MODERATE TO HIGH RISK ACUTE OR RAPID
(minor urinary abnormalities, (proteinuria > 0.5–1 g/d and/or
GFR normal, no hypertension) GFR reduced and/or hypertension)
GFR LOSS
AKI due to macro-
Monitor annually Optimize supportive therapy hematuria or other
for at least 10 years common cause
Proteinuria >0.5–1 g/day
Nephrotic syndrome Supportive
GFR normal or slowly , GFR < 30–50 ml/min
or RPGN therapy
but > 30–50 ml/min
Continue supportive therapy
Continue supportive therapy
No immunosuppression Add immunosuppression
for at least 3–6 months
(except if RPGN)
Continue supportive Add corticosteroid,
therapy alone, if proteinuria > 1g/day or
if proteinuria < 1g/day and progressive GFR-loss
GFR-decline < 30%/6 months despite blood pressure control
Figure 1. Synopsis of suggested therapeutic approaches to patients with IgAN depending on the clinical setting.
mated reminder systems might provide year or at year 1.12 Uncontrolled hyper- are ongoing. Whether it is beneficial to
some help here. tension has an additive effect with protein- base clinical decisions on this classifica-
uria in driving progression of disease.9,11 tion system, in particular, the novel pa-
The third consistent indicator of risk is a rameters of mesangial and endocapillary
THE TYPICAL PATIENT WITH IgAN decrease in GFR at presentation.10 This is hypercellularity, has not yet been tested.
expected since loss of renal function likely Finally, how the presence of cellular cres-
Proteinuria, Hypertension, and GFR identifies the subgroup of IgAN patients cents in a patient who does not exhibit a
Are Key Determinants of the Type who are already progressive. Finally, renal rapidly progressive (vasculitic) course of
of Treatment prognosis is worse in obese IgAN pa- IgAN should ultimately affect treatment
The degree of proteinuria is one of the tients,13,14 possibly related to superim- modality is unresolved. There is relative
strongest predictors of outcome in posed obesity-related renal changes.15 consensus, however, that crescents in
IgAN.9 –11 The risk for renal failure in- Nonsurgical weight loss can indeed lead to ⬍50% of the glomeruli in an otherwise
creases with higher proteinuria. Vice a reduction of proteinuria.16 stable patient should not automatically
versa, lowering proteinuria markedly de- In terms of histologic parameters prompt immunosuppression since insti-
creases risk regardless of whether the ini- (Figure 2), the IgAN Oxford classifica- tution of adequate supportive therapy
tial proteinuria is mild or in the ne- tion17,18 may offer important advances may indeed lead to resolution of cres-
phrotic range.9,11 Whereas most studies by providing evidence that not only cents.
use a proteinuria cutoff of 1 g/d, above chronic fibrotic changes, particularly
which increased risk for renal failure de- glomerulosclerosis and tubulointersti- One Size Fits All: Optimized
velops,9 –11 others contend that an in- tial fibrosis, but also mesangial and en- Supportive Therapy Is the
creased risk starts above 0.5 g/d.12 Fur- docapillary hypercellularity predict Cornerstone for All Patients at Risk
thermore, it unresolved, which is the best prognosis. Various validation studies, of Progression
predictor, proteinuria at initial presenta- such as the VALIGA study of the Euro- There is no doubt that an optimized sup-
tion or the level maintained over the first pean Renal Association (ERA-EDTA), portive regimen constitutes the corner-
1786 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1785–1794, 2011
www.jasn.org BRIEF REVIEW
Table 1. Supportive therapy of IgAN warfarin [INR 1.3 to 1.5]) compared
Level 1 recommendations with no treatment, but angiotensin-
● Control blood pressure (sitting systolic BP in the 120s) converting enzyme (ACE) inhibitors
● ACE inhibitor or ARB therapy with uptitration of dosage or combination ACE inhibitor were avoided in these patients.27 Most
and ARB therapy other studies on this topic suffer from
● Avoid dihydropyridine calcium-channel blockers unless needed for BP control the fact that antiplatelet therapy was
● Control protein intake not standardized (aspirin, warfarin, or
Level 2 recommendations
dipyridamole were used), often com-
● Restrict NaCl intake/institute diuretic therapy
bined with immunosuppression, and
● Control fluid intake
● Non–dihydropyridine calcium-channel blocker therapy
were retrospective and nonrandom-
● Control each component of the metabolic syndrome ized. At present, no recommendation
● Aldosterone antagonist therapy on the use of such drugs is possible in
● Beta-blocker therapy IgAN patients.
● Smoking cessation Tonsillectomy, combined with im-
● Allopurinol therapy munosuppression, in patients at risk
● Empiric NaHCO3 therapy, independent of whether metabolic acidosis is present or not for progressive IgAN, is mostly recom-
Other measures to retard IgAN progression mended in Japan, based largely on ret-
● Avoid NSAIDs altogether, or no more than once or twice weekly at most rospective data.28,29 A recent small Jap-
● Avoid prolonged severe hypokalemia
anese study in transplanted patients
● Avoid phosphate cathartics
with recurrent IgAN30 reports that ton-
● Ergocalciferol therapy to correct vitamin D deficiency
● Control hyperphosphatemia and hyperparathyroidism; in animal models and in human
sillectomy reduces proteinuria from
studies, controlling hyperphosphatemia slows CKD progression 880 to 280 mg/d, whereas little change
Recommended supportive therapy options in patients with, or at risk of, progressive IgAN (modified after was noted in a non– operated control
reference 20). The goal is to implement all level 1 recommendations and as many level 2 group. Another recent Japanese study
recommendations as feasible. ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; in primary IgAN also reports that ton-
CKD, chronic kidney disease; NSAID, non-steroidal anti-inflammatory drug.
sillectomy combined with immuno-
suppression is more effective in induc-
ing remission of proteinuria and/or
stone of any therapeutic approach to there was a 75% probability of at least a hematuria than immunosuppression
IgAN patients at risk for progression. In minor effect.23 Long-term follow-up of alone.31 Limitations of both studies in-
fact, this will be the only area where there the largest randomized trial so far 24 clude their small size, nonrandomized
will be KDIGO recommendations (as op- noted a better preservation of renal nature, and nonsystematic renin-ang-
posed to suggestions with lower degree function in the fish oil group. In a iotensin blockade. Given that other
evidence). These measures are summa- smaller Italian randomized trial in pro- studies have been unable to document
rized in Table 1. In view of space limita- teinuric IgAN patients with preserved a benefit in IgAN patients who are
tions, we will not discuss this issue in de- renal function, proteinuria decreased Caucasian, 32,32a we feel that an ade-
tail. The reader is referred to excellent by 75% in the fish oil group but re- quately powered randomized con-
reviews on this topic.19 –21 Of note, most mained stable in controls;25 however, a trolled trial will be required before
randomized trials in IgAN suffer from tendency of the control group toward tonsillectomy can be routinely re-
lack of optimized and comprehensive worse prognostic features at baseline commended in the care of IgAN pa-
supportive care. We therefore initiated (numerically lower mean GFR, higher tients. An exception may be when there
the STOP-IgAN trial,22 which will test in proteinuria, and more men) was nota- is a clear temporal relationship be-
high-risk IgAN patients whether immu- ble. Essentially no side effects were tween tonsillitis episodes and bouts of
nosuppression exerts an added benefit noted. In contrast, another more re- macrohematuria.
after the supportive therapy has been op- cent randomized trial failed to detect a A recent Finnish study investigated
timized over 6 months. We recently fin- benefit from fish oil;26 whether this was the relationship between alcohol con-
ished recruitment and data are expected related to a slightly higher baseline sumption and progression of IgAN.33
by 2014. proteinuria in the fish oil group re- Better kidney function was associated
mains unresolved. At present, fish oil with light-to-moderate alcohol con-
Nonestablished and Controversial in IgAN is literally a matter of taste. sumption after correction for hyper-
Nonimmunosuppressive Treatment Antiplatelet and anticoagulant tension and 24-hour protein excretion.
Approaches drugs are mostly used in Asia for the Light consumption (one drink per day)
In a meta-analysis of fish oil therapy in treatment of IgAN. A small random- in women and moderate consumption
patients with IgAN, no statistically sig- ized trial suggested benefit from dipy- (1 to 3 drinks per day) in men appears
nificant benefit was noted, although ridamole (75 mg three times daily and optimal. Although this certainly does
J Am Soc Nephrol 22: 1785–1794, 2011 IgA Nephropathy 1787
BRIEF REVIEW www.jasn.org
Similarly, a low-dose corticosteroid reg-
A B
imen (20 mg/d, tapered over 2 years)
from Japan was ineffective in a random-
ized trial.38
Corticosteroid-related side effects, even
with the more aggressive Pozzi regimen,
were reported to be minor. This is in con-
trast to the orthopedic literature in which
9 g of methylprednisolone markedly ex-
ceeded the threshold of 2 g of methylpred-
nisolone administered within 3 months,
C D above which the incidence of aseptic osteo-
necrosis starts to rise.39,40
Supportive therapy in the IgAN pa-
tients was not optimal by current stan-
dards in the study of Pozzi et al.36; a sim-
ilar benefit was noted after instituting an
ACE inhibitor alone.41,42 This is consis-
tent with a retrospective analysis in 702
IgAN patients where corticosteroid pulse
therapy as well as ACE-inhibitor therapy
E F independently reduced progression of
disease.43 Both the trial of Manno et al.
and Lv et al. 35,34 (Table 2) suffer from
their study design, as patients were re-
quired to discontinue prior ACE inhibi-
tor or angiotensin receptor blocker
(ARB) therapy. Then, in the combina-
tion groups, they started receiving simul-
taneously an ACE inhibitor and cortico-
steroids. Consequently, a high number
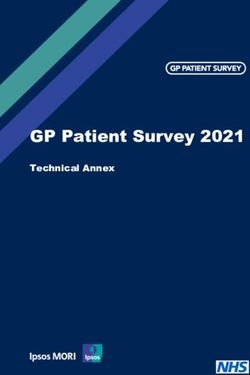
Figure 2. The range of histologic findings in IgA nephropathy with an evaluation based of patients who would have ended up in a
on the Oxford classification.17,18 All sections are PAS stains. (A) Glomerulus without low-risk category with ACE inhibitor
mesangial proliferation and matrix increase (M0 with the majority of glomeruli showing treatment alone were assigned additional
this phenotype). (B) Glomerulus with segmental mesangial hypercellularity (arrow) (M1 immunosuppression.44 In our own on-
with the majority of glomeruli showing such a phenotype). (C) Endocapillary hypercellu-
going STOP-IgAN study,22 we noted
larity (E1). (D) Glomerulus with segmental necrosis and extracapillary proliferation. (E)
Overview of a case with sclerotic and atrophic changes. Right-sided glomerulus with
that, during the 6-month run-in phase,
segmental glomerulosclerosis and a focal adhesion (arrow) surrounded by increased which is meant to uptitrate renin-angio-
interstitial matrix and tubules with segmental dedifferentiation (tubular atrophy) (S1 for tensin blockers to their maximum anti-
glomerular sclerosis and T1 for tubular atrophy and interstitial fibrosis). (F) Higher mag- proteinuric effect, proteinuria decreased
nification of the glomerulus illustrated in Figure 2E with segmental glomerulosclerosis to ⬍0.75 g/d in most patients with IgAN
and an adhesion (arrow) (S1). (unpublished data).
A pragmatic approach suggests first
not establish a causal or even therapeu- preserved renal function, and a GFR optimizing supportive therapy in IgAN
tic relationship, patients should be above 50 ml/min, can reduce proteinuria patients at risk for progression (see
made aware of these findings. and decrease the risk of subsequent renal above). If this is not sufficient to lower
failure.34 –37 Whereas corticosteroid ther- proteinuria below about 1 g/d, patients
Proteinuric Patients, Despite apy in the first trial consisted of com- should be offered a 6-month trial of cor-
Optimized Supportive Care, Should bined pulse and oral steroids, a purely ticosteroids as long as their GFR is higher
Be Given a 6-Month Course of oral regimen was used in the subsequent than 50 ml/min (Figure 1). Table 2 sug-
Corticosteroids If GFR Is Above trials and appeared effective as well (Ta- gests that strictly alternating or low-dose
50 ml/min ble 2). In contrast, in a smaller United corticosteroid therapy is ineffective. It is
Three randomized controlled trials have States trial,26 using a much longer but unresolved which of the three high-dose
shown that a 6-month course of cortico- strictly alternating steroid regimen, no daily regimens is more beneficial. The
steroids in IgAN patients with relatively benefit was noted at 2 years (Table 2). longest follow-up data are available for
1788 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1785–1794, 2011Table 2. Corticosteroid monotherapy
Trial Pozzi et al., Italy37,36 Katafuchi et al., Japan38 Hogg et al., United States26 Manno et al., Italy35 Lv et al., China34
Corticosteroid regimen Intravenous methylprednisolone 1 g/d Oral prednisolone 20 Oral prednisone every other Oral prednisone for 6 months Oral prednisone for 6–8
for 3 consecutive days at the mg/d tapered to 5 day 60 mg/m2 for 3 (1 mg/kg/day for 2 months, months (0.8–1 mg/kg/
beginning of months 1, 3, and 5, mg/d at 18 months months, then 40 mg/m2 then reduced by 0.2 mg/ day for 2 months,
plus oral prednisone 0.5 mg/kg for 9 months, and then 30 kg/day per month) then reduced by 5–10
every other day for 6 months mg/m2 for 12 months mg every 2 wk)
Control regimen Supportive only Dipyridamole Placebo Supportive only Supportive only
RAS blockade 14% at baseline, allowed during 2% at baseline; allowed Enalapril if hypertensive Ramipril in all patients Cilazapril in all patients
follow-up during follow-up
Key outcome in steroid Ten-year renal survival (⫽absent Significant reduction in No benefit in the steroid Mean annual loss of GFR 6.2 Significantly fewer
group versus control doubling of serum creatinine), 53% proteinuria but not group versus placebo at 2 ml/min in controls versus 0.6 patients with a 50%
J Am Soc Nephrol 22: 1785–1794, 2011
in controls versus 97% in the ESRD frequency years ml/min in the steroid group increase in serum
steroid group creatinine in the
steroid group
Therapeutic regimens and outcomes in randomized controlled trials in IgAN patients. RAS, renin-angiotensin system; ESRD, end-stage renal disease.
Table 3. Mycophenolate mofetil monotherapy
Trial Maes et al., Belgium48 Tang et al., China46,47 Frisch et al., United States49
MMF regimen 2 g/d for 3 years 1.5 to 2.0 g/d depending on body weight Titrated up to 2 g/d for 1 year
for 6 months
Control regimen Placebo Supportive only Placebo
RAS blockade All patients All patients All patients
Key outcome in MMF group No effect on GFR or Reduction in proteinuria, stabilization of No effect on GFR or proteinuria
versus control proteinuria GFR
Therapeutic regimens and outcomes in controlled trials in IgAN patients. MMF, mycophenolate mofetil; RAS, renin-angiotensin system.
Table 4. Immunosuppressive combination therapy
Trial Ballardie et al., United Kingdom66 Yoshikawa et al., Japan64 Yoshikawa et al., Japan65 Pozzi et al., Italy45
Combination regimen Oral prednisolone 40 mg/d reduced to Oral prednisolone (2 mg/kg per day, Oral prednisolone (2 mg/kg per day, Same as shown in Table 2 36 ⫹
10 mg (end of year 2) ⫹ oral maximum, 80 mg/d for 4 weeks maximum, 80 mg/d for 4 weeks oral azathioprine 1.5 mg/kg
cyclophosphamide 1.5 mg/kg per tapered to alternate steroid at 1 tapered to alternate steroid at 1 per day for 6 months
day for 3 months, and then oral mg/kg until end of year 2) ⫹ oral mg/kg until end of year 2) ⫹ oral
azathioprine 1.5 mg/kg per day for azathioprine (2 mg/kg per day for 2 azathioprine (2 mg/kg per day for 2
minimum 2 years and up to 6 years years) ⫹ anticoagulants (heparin years) ⫹ warfarin ⫹ dipyridamole
followed by warfarin and
www.jasn.org
dipyridamole)
Control regimen Supportive therapy only Supportive therapy ⫹ anticoagulants Above regimen without azathioprine Same as shown in Table 2 36
(see above)
IgA Nephropathy
RAS blockade Inconsistent Not reported Prohibited 45% at baseline
Key outcome in combination Marked improvement of renal survival Higher reduction in proteinuria and More complete remissions of No difference between groups
group versus control at 5 years percentage of sclerosed glomeruli proteinuria
Comment Study included pediatric patients only Study included pediatric patients only
BRIEF REVIEW
Therapeutic regimens and outcomes in controlled trials in IgAN patients. RAS, renin-angiotensin system.
1789BRIEF REVIEW www.jasn.org
the Pozzi regimen.37 Patient preferences, sufficient at present to suggest their use serum creatinine below 2 mg/dl and a
anticipated risk of side effects in a given in IgAN patients. Of note, as discussed proteinuria above 1 g/d, despite RAS
patient, and also local conditions should below, neither cyclosporine A, tacroli- blockade, were assigned to receive corti-
currently dictate the choice of regimen. mus, or sirolimus prevent recurrence of costeroids or additional oral azathio-
Successful re-treatments in patients who IgAN in a renal graft. prine. Outcome after a median of 4.9
experienced a relapse of proteinuria after years was not different between the two
steroid therapy have been reported.45 Immunosuppressive Combination groups.45
Therapy Is Not Recommended In general, side effects in the combi-
Data on Mycophenolate Mofetil A number of retrospective studies or case nation therapy groups are more frequent
(MMF) Monotheray in IgAN Are series, mostly from Asia, have reported and severe than those in monotherapy
Inconclusive beneficial outcomes in high-risk IgAN pa- groups and include, among others, glau-
Three randomized controlled trials, one tients treated with combinations of corti- coma, cataracts, and aseptic necrosis of
each from China,46,47 Belgium, and the costeroids plus cyclophosphamide or aza- the femoral head in children,65,64 my-
United States48,49 have assessed the value thioprine versus controls.57– 61 Selection elodepression,66 secondary diabetes,66
of MMF in high-risk patients with IgAN and observation bias as well as nonopti- pulmonary tuberculosis,66 and pneumo-
(Table 3); a fourth trial50 is ongoing. One mized supportive measures render an in- cystis pneumonia.45 In our ongoing STOP-
additional study, published in Chinese, terpretation of these studies difficult. In IgAN trial, one patient receiving immuno-
reports better proteinuria reduction with contrast, one trial from Singapore62 and suppressive combination therapy based
1 to 1.5 g/d MMF, reduced to 0.5 to 0.75 one from Australia63 found no evidence for on the Ballardie protocol66 died from
g/d within 12 months, as compared with a benefit of cyclophosphamide, dipyrid- pneumogenic sepsis (unpublished ob-
high-dose oral prednisone.51 Supportive amole, plus warfarin on renal function as servation). Clearly, this is a major con-
care and BP control were unclear, ren- compared with controls. cern in a slowly progressive disease such
dering an interpretation of this study dif- More recent prospective randomized as IgAN, which needs to be weighed
ficult. In the other Chinese trial, 2 g/d of controlled trials on immunosuppressive against the risk of losing renal function.
MMF, on top of an ACE inhibitor, led to combinations in IgAN have also yielded in- At present, we feel that immunosup-
better reduction of proteinuria and sta- consistent outcomes (Table 4). In two Jap- pressive combination therapy is not war-
bilization of renal function in 20 IgAN anese trials, both from the same group,64,65 ranted in IgAN patients unless there are
patients than ACE inhibitor alone.46,47 In children with IgAN and severe histologic features of rapidly progressive glomeru-
contrast, the Belgian and United States changes and/or significant proteinuria, yet lonephritis and/or a vasculitic course
trials in mostly Caucasian patients found normal GFR, received azathioprine plus (see below).
no effect on proteinuria48,49 despite a de- corticosteroids plus anticoagulants versus
sign similar to that in the latter Chinese anticoagulants alone.64 In the other trial, The Patient with GFR below 30 to
trial.46,47 Whether ethnic factors, the azathioprine plus corticosteroids plus anti- 50 ml/min: Comprehensive
higher dose of MMF per body weight in coagulants were tested against steroids Supportive Therapy Only
the Chinese trials, or other unidentified alone.65 In both cases, the combination Almost all randomized controlled trials
factors account for these striking differ- therapy led to higher rates of complete re- exclude IgAN patients with a GFR below
ences is unresolved.52 mission of proteinuria. 30 ml/min and contain very few patients
At present, it appears prudent to largely In 2002, Ballardie et al.66 published a with a GFR between 30 and 50 ml/min. A
restrict the use of MMF to patients of Asian small randomized trial comparing cyclo- case series in patients with a median GFR
origin who fail to respond to supportive phosphamide plus corticosteroids fol- of 22 ml/min reported benefits from se-
therapy and/or corticosteroids or in whom lowed by azathioprine plus corticoste- quential cyclophosphamide or steroid-
the use of steroids is problematic because roids versus controls. Renal survival at 5 bolus therapy followed by MMF,67 but a
of comorbidities or side effects. If MMF is years was 72% in the immunosuppressed randomized controlled trial using MMF
used in IgAN patients with a reduced GFR, group versus 6% in controls.66 RAS alone in advanced IgAN failed to induce
pneumocystis carinii prophylaxis is impor- blockade was infrequent and BP control any benefit.49 At present there is not
tant, given several deaths in Chinese IgAN not ideal by today’s standards. In addi- enough evidence to advocate immuno-
patients on MMF.53 tion, the patient group was highly select suppressive therapy in advanced IgAN
in that patients exhibited impaired renal once the patient has a serum creatinine
Other Immunosuppressive function at baseline with reciprocal se- above 2.5 to 3 mg/dl, that is, the thresh-
Monotherapy Approaches Are Not rum creatinine plots suggesting end- old that sometimes is referred to as the
Established stage renal failure within 5 years, pro- “point of no return.”68,69 Comprehen-
Some data have been published on alter- nounced proteinuria, and no advanced sive supportive therapy, however, must
native immunosuppressants in IgAN pa- tissue scarring. Finally in 2010, Pozzi et be continued in such patients as it can
tients, including mizoribine54 and cyclo- al.45 published a randomized controlled stabilize renal function for years at even
sporine A.55,56 None of the evidence is trial in which 207 IgAN patients with a very low levels.70 –72
1790 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1785–1794, 2011www.jasn.org BRIEF REVIEW
THE ATYPICAL PATIENT proteinuria; however, there was no effect images illustrating the Oxford classification
on GFR after about 3 years.79 of IgAN.
The Patient with Acute Kidney
Injury (AKI) or Rapidly Progressive The Patient with Secondary IgAN
Loss of Renal Function Secondary IgAN is most commonly seen DISCLOSURES
AKI resulting primarily from non– dis- in patients with chronic liver and inflam- None.
ease-specific causes is a common presen- matory bowel diseases; however, associ-
tation in the rare elderly patient with ations have been reported for numerous
IgAN.73 The cause is usually apparent other immunologic and infectious dis- REFERENCES
from the history and such patients eases.80 The treatment of secondary IgAN
should receive supportive therapy. In is primarily directed against the underlying 1. Waldherr R, Rambausek M, Duncker WD,
Ritz E: Frequency of mesangial IgA deposits
AKI associated with macroscopic hema- primary disease. In particular, in patients
in a non-selected autopsy series. Nephrol
turia, a repeat renal biopsy is indicated if with alcoholic liver disease, 80% of the pa- Dial Transplant 4: 943–946, 1989
renal function does not improve within a tients exhibit glomerular IgA deposits,81 2. Suzuki K, Honda K, Tanabe K, Toma H, Nihei
few days to differentiate acute tubular but progressive IgAN is very rare. A discus- H, Yamaguchi Y: Incidence of latent mesan-
necrosis with intratubular erythrocyte sion of current therapeutic concepts in He- gial IgA deposition in renal allograft donors
in Japan. Kidney Int 63: 2286 –2294, 2003
casts from crescentic and/or necrotizing noch-Schönlein purpura is beyond the
3. Szeto CC, Lai FM, To KF, Wong TY, Chow
IgAN. The former again requires sup- scope of our review. The reader is referred KM, Choi PC, Lui SF, Li PK: The natural
portive care only; macrohematuria lon- to recent reviews.82– 84 history of immunoglobulin a nephropathy
ger than 10 days, older age, and de- among patients with hematuria and minimal
creased baseline GFR are clinical proteinuria. Am J Med 110: 434 – 437, 2001
4. Nieuwhof C, Kruytzer M, Frederiks P, van
predictors of incomplete recovery from
RECURRENT IgAN IN THE Breda Vriesman PJ: Chronicity index and
AKI.74 mesangial IgG deposition are risk factors for
In case series of crescentic and/or ne- TRANSPLANT PATIENT
hypertension and renal failure in early IgA
crotizing IgAN and either AKI or a rap- nephropathy. Am J Kidney Dis 31: 962–970,
idly progressive course, there was a None of the currently available immuno- 1998
seeming benefit from treatment analo- suppressive drugs used after renal trans- 5. Shima Y, Nakanishi K, Kamei K, Togawa H,
plantation can prevent the histologic re- Nozu K, Tanaka R, Sasaki S, Iijima K, Yo-
gous to ANCA-associated vasculitis shikawa N: Disappearance of glomerular IgA
(steroids and cyclophosphamide).75–78 currence of IgAN.8,85 There is also no
deposits in childhood IgA nephropathy
Limitations of all these studies include clear evidence that the choice of immu- showing diffuse mesangial proliferation after
the lack of controls and their usually ret- nosuppression after renal transplanta- 2 years of combination/prednisolone ther-
rospective nature. Such rare patients tion affects the clinical manifestation or apy. Nephrol Dial Transplant 26: 163–169,
course of recurrent IgAN.8 2011
can also have anti-GBM antibodies or 6. Yoshikawa N, Iijima K, Matsuyama S, Suzuki
ANCAs and probably should be treated Relative consensus exists that patients
J, Kameda A, Okada S, Nakamura H: Repeat
analogously to Goodpasture’s syndrome or with recurrent IgAN should mainly re- renal biopsy in children with IgA nephropa-
ANCA vasculitis, respectively. ceive optimized supportive care. A small thy. Clin Nephrol 33: 160 –167, 1990
case series86 reported that without renin- 7. Cuevas X, Lloveras J, Mir M, Aubia J, Masra-
angiotensin blockade 4 out of 4 patients mon J: Disappearance of mesangial IgA de-
The Patient with Overt Nephrotic posits from the kidneys of two donors after
Syndrome with recurrent IgAN progressed to end-
transplantation. Transplant Proc 19: 2208–
Although nephrotic-range proteinuria is stage renal disease compared with 3 out 2209, 1987
not uncommon in IgAN patients, partic- of 9 in the group treated with an ARB. 8. Floege J: Recurrent IgA nephropathy after
ularly those with poorly controlled hy- Whether patients with recurrent IgAN renal transplantation. Semin Nephrol 24:
should also receive a tonsillectomy, as 287–291, 2004
pertension, a complete nephrotic syn- 9. Reich HN, Troyanov S, Scholey JW, Cattran
drome is distinctly uncommon. In such suggested by a recent small Japanese trial,
DC: Remission of proteinuria improves prog-
cases, coincidental IgAN with minimal- is currently unresolved.30 nosis in IgA nephropathy. J Am Soc Nephrol
change nephropathy should be excluded 18: 3177–3183, 2007
10. D’Amico G: Natural history of idiopathic IgA
by electron microscopy and, if present,
nephropathy and factors predictive of dis-
treatment should be analogous to mini- ACKNOWLEDGMENTS ease outcome. Semin Nephrol 24: 179 –196,
mal-change disease. A small randomized 2004
controlled trial from 1986 suggests that We thank Lee Hebert, The Ohio State Univer- 11. Berthoux F, Mohey H, Laurent B, Mariat C,
IgAN patients with nephrotic syndrome, sity, Columbus, Ohio, for his very helpful Afiani A, Thibaudin L: Predicting the risk of
dialysis or death in IgA nephropathy. J Am
particularly those with mild histologic suggestions in revising Table 1. We also thank
Soc Nephrol 2011, in press
changes, benefit from a 4-month course H.J. Gröne, Div. Cellular and Molecular Pathol- 12. Coppo R, D’Amico G: Factors predicting
of oral prednis(ol)one (40 to 60 mg/d ogy, Deutsches Krebsforschungszentrum, Heidel- progression of IgA nephropathies. J Neph-
starting dose) in terms of remission of berg, Germany, for providing the histologic rol 18: 503–512, 2005
J Am Soc Nephrol 22: 1785–1794, 2011 IgA Nephropathy 1791BRIEF REVIEW www.jasn.org
13. Bonnet F, Deprele C, Sassolas A, Moulin P, 22. Eitner F, Ackermann D, Hilgers RD, Floege merulonephritis. Nephrol Dial Transplant 25:
Alamartine E, Berthezene F, Berthoux F: Ex- J: Supportive versus immunosuppressive 2583–2589, 2010
cessive body weight as a new independent therapy of progressive IgA nephropathy 33. Kaartinen K, Niemela O, Syrjanen J, Porsti I,
risk factor for clinical and pathological pro- (STOP) IgAN trial: Rationale and study pro- Harmoinen A, Pasternack A, Huhtala H, Mu-
gression in primary IgA nephritis. Am J Kid- tocol. J Nephrol 21: 284 –289, 2008 stonen J: Alcohol consumption and kidney
ney Dis 37: 720 –727, 2001 23. Dillon JJ: Fish oil therapy for IgA nephrop- function in IgA glomerulonephritis. Nephron
14. Tanaka M, Tsujii T, Komiya T, Iwasaki Y, athy: Efficacy and interstudy variability. J Am Clin Pract 112: c86 –93, 2009
Sugishita T, Yonemoto S, Tsukamoto T, Fu- Soc Nephrol 8: 1739 –1744, 1997 34. Lv J, Zhang H, Chen Y, Li G, Jiang L, Singh
kui S, Takasu A, Muso E: Clinicopathological 24. Donadio JV Jr., Grande JP, Bergstralh EJ, Dart AK, Wang H: Combination therapy of pred-
influence of obesity in IgA nephropathy: RA, Larson TS, Spencer DC: The long-term nisone and ACE inhibitor versus ACE-inhib-
Comparative study of 74 patients. Contrib outcome of patients with IgA nephropathy itor therapy alone in patients with IgA ne-
Nephrol 157: 90 –93, 2007 treated with fish oil in a controlled trial. Mayo phropathy: A randomized controlled trial.
15. Tanaka M, Yamada S, Iwasaki Y, Sugishita T, Nephrology Collaborative Group. J Am Soc Am J Kidney Dis 53: 26 –32, 2009
Yonemoto S, Tsukamoto T, Fukui S, Takasu K, Nephrol 10: 1772–1777, 1999 35. Manno C, Torres DD, Rossini M, Pesce F,
Muso E: Impact of obesity on IgA nephropathy: 25. Ferraro PM, Ferraccioli GF, Gambaro G, Fu- Schena FP: Randomized controlled clinical
Comparative ultrastructural study between lignati P, Costanzi S: Combined treatment trial of corticosteroids plus ACE-inhibitors
obese and non-obese patients. Nephron Clin with renin-angiotensin system blockers and with long-term follow-up in proteinuric IgA
Pract 112: c71–c78, 2009 polyunsaturated fatty acids in proteinuric nephropathy. Nephrol Dial Transplant 24:
16. Navaneethan SD, Yehnert H, Moustarah F, IgA nephropathy: A randomized controlled 3694 –3701, 2009
Schreiber MJ, Schauer PR, Beddhu S: trial. Nephrol Dial Transplant 24: 156 –160, 36. Pozzi C, Bolasco PG, Fogazzi GB, Andrulli S,
Weight loss interventions in chronic kidney 2009 Altieri P, Ponticelli C, Locatelli F: Corticoste-
disease: A systematic review and meta-anal- 26. Hogg RJ, Lee J, Nardelli N, Julian BA, Cat- roids in IgA nephropathy: A randomised
ysis. Clin J Am Soc Nephrol 4: 1565–1574, tran D, Waldo B, Wyatt R, Jennette JC, Sib- controlled trial. Lancet 353: 883– 887, 1999
2009 ley R, Hyland K, Fitzgibbons L, Hirschman G, 37. Pozzi C, Andrulli S, Del Vecchio L, Melis P,
17. Cattran DC, Coppo R, Cook HT, Feehally Donadio JV Jr., Holub BJ: Clinical trial to Fogazzi GB, Altieri P, Ponticelli C, Locatelli
J, Roberts IS, Troyanov S, Alpers CE, evaluate omega-3 fatty acids and alternate F: Corticosteroid effectiveness in IgA ne-
Amore A, Barratt J, Berthoux F, Bonsib S, day prednisone in patients with IgA ne- phropathy: Long-term results of a random-
Bruijn JA, D’Agati V, D’Amico G, Emanci- phropathy: Report from the Southwest Pedi- ized, controlled trial. J Am Soc Nephrol 15:
pator S, Emma F, Ferrario F, Fervenza FC, atric Nephrology Study Group. Clin J Am 157–163, 2004
Florquin S, Fogo A, Geddes CC, Groene HJ, Soc Nephrol 1: 467– 474, 2006 38. Katafuchi R, Ikeda K, Mizumasa T, Tanaka H,
Haas M, Herzenberg AM, Hill PA, Hogg RJ, 27. Lee GS, Choong HL, Chiang GSC, Woo KT: Ando T, Yanase T, Masutani K, Kubo M,
Hsu SI, Jennette JC, Joh K, Julian BA, Kawa- Three year randomized controlled trial of Fujimi S: Controlled, prospective trial of ste-
mura T, Lai FM, Leung CB, Li LS, Li PK, Liu dipyridamole and low-dose warfarin in pa- roid treatment in IgA nephropathy: A limita-
ZH, Mackinnon B, Mezzano S, Schena FP, tients with IgA nephropathy and renal im- tion of low-dose prednisolone therapy. Am J
Tomino Y, Walker PD, Wang H, Weening JJ, pairment. Nephrology (Carlton) 3: 117–121, Kidney Dis 41: 972–983, 2003
Yoshikawa N, Zhang H: The Oxford classifi- 1997 39. Saisu T, Sakamoto K, Yamada K, Kashi-
cation of IgA nephropathy: Rationale, clini- 28. Xie Y, Nishi S, Ueno M, Imai N, Sakatsume wabara H, Yokoyama T, Iida S, Harada Y,
copathological correlations, and classifica- M, Narita I, Suzuki Y, Akazawa K, Shimada H, Ikenoue S, Sakamoto M, Moriya H: High
tion. Kidney Int 76: 534 –545, 2009 Arakawa M, Gejyo F: The efficacy of tonsil- incidence of osteonecrosis of femoral
18. Roberts IS, Cook HT, Troyanov S, Alpers CE, lectomy on long-term renal survival in pa- head in patients receiving more than 2 g of
Amore A, Barratt J, Berthoux F, Bonsib S, tients with IgA nephropathy. Kidney Int 63: intravenous methylprednisolone after re-
Bruijn JA, Cattran DC, Coppo R, D’Agati V, 1861–1867, 2003 nal transplantation. Transplant Proc 28:
D’Amico G, Emancipator S, Emma F, Fee- 29. Hotta O, Miyazaki M, Furuta T, Tomioka S, 1559 –1560, 1996
hally J, Ferrario F, Fervenza FC, Florquin S, Chiba S, Horigome I, Abe K, Taguma Y: 40. Drescher W, Schlieper G: Osteonecrosis.
Fogo A, Geddes CC, Groene HJ, Haas M, Tonsillectomy and steroid pulse therapy sig- Nephrol Dial Transplant 2011, in press
Herzenberg AM, Hill PA, Hogg RJ, Hsu SI, nificantly impact on clinical remission in pa- 41. Praga M, Gutierrez E, Gonzalez E, Morales
Jennette JC, Joh K, Julian BA, Kawamura tients with IgA nephropathy. Am J Kidney E, Hernandez E: Treatment of IgA nephrop-
T, Lai FM, Li LS, Li PK, Liu ZH, Mackinnon B, Dis 38: 736 –743, 2001 athy with ACE inhibitors: A randomized and
Mezzano S, Schena FP, Tomino Y, Walker 30. Kennoki T, Ishida H, Yamaguchi Y, Tanabe controlled trial. J Am Soc Nephrol 14: 1578 –
PD, Wang H, Weening JJ, Yoshikawa N, K: Proteinuria-reducing effects of tonsillec- 1583, 2003
Zhang H: The Oxford classification of IgA tomy alone in IgA nephropathy recurring 42. Coppo R, Peruzzi L, Amore A, Piccoli A,
nephropathy: Pathology definitions, correla- after kidney transplantation. Transplantation Cochat P, Stone R, Kirschstein M, Linne T:
tions, and reproducibility. Kidney Int 76: 88: 935–941, 2009 IgACE: A placebo-controlled, randomized
546 –556, 2009 31. Komatsu H, Fujimoto S, Hara S, Sato Y, trial of angiotensin-converting enzyme in-
19. Wilmer WA, Rovin BH, Hebert CJ, Rao SV, Yamada K, Kitamura K: Effect of tonsillec- hibitors in children and young people with
Kumor K, Hebert LA: Management of glo- tomy plus steroid pulse therapy on clinical IgA nephropathy and moderate proteinuria.
merular proteinuria: A commentary. J Am remission of IgA nephropathy: A controlled J Am Soc Nephrol 18: 1880 –1888, 2007
Soc Nephrol 14: 3217–3232, 2003 study. Clin J Am Soc Nephrol 3: 1301–1307, 43. Katafuchi R, Ninomiya T, Mizumasa T, Ikeda
20. Brown C, Haddad N, Hebert LA: Retarding 2008 K, Kumagai H, Nagata M, Hirakata H: The
progression of kidney disease. In: Compre- 32. Rasche FM, Schwarz A, Keller F: Tonsillec- improvement of renal survival with steroid
hensive Clinical Nephrology, edited by tomy does not prevent a progressive course pulse therapy in IgA nephropathy. Nephrol
Floege J, Feehally J, Johnson RJ, St. Louis, in IgA nephropathy. Clin Nephrol 51: 147– Dial Transplant 23: 3915–3920, 2008
Elsevier, 2010, pp 919 –926 152, 1999 44. Eitner F, Floege, J: Glomerular disease:
21. Abboud H, Henrich WL: Clinical practice. 32a.Piccoli A, Codognotto M, Tabbi MG, Favaro ACEIs with or without corticosteroids in
Stage IV chronic kidney disease. N Engl E, Rossi B: Influence of tonsillectomy on the IgA nephropathy? Nat Rev Nephrol 6:
J Med 362: 56 – 65, 2010 progression of mesangioproliferative glo- 252–254
1792 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1785–1794, 2011www.jasn.org BRIEF REVIEW
45. Pozzi C, Andrulli S, Pani A, Scaini P, Del 57. Sato M, Hotta O, Tomioka S, Horigome I, 69. Scholl U, Wastl U, Risler T, Braun N, Gra-
Vecchio L, Fogazzi G, Vogt B, De Cristofaro Chiba S, Miyazaki M, Noshiro H, Taguma Y: bensee B, Heering P, Schollmeyer P, Zauner
V, Allegri L, Cirami L, Procaccini AD, Loca- Cohort study of advanced IgA nephropathy: I, Stein G, Funfstuck R, Keller F: The “point
telli F: Addition of azathioprine to cortico- Efficacy and limitations of corticosteroids of no return” and the rate of progression in
steroids does not benefit patients with IgA with tonsillectomy. Nephron Clin Pract 93: the natural history of IgA nephritis. Clin
nephropathy. J Am Soc Nephrol 21: 1783– c137– c145, 2003 Nephrol 52: 285–292, 1999
1790, 2010 58. Goumenos DS, Davlouros P, El Nahas AM, 70. Komatsu H, Fujimoto S, Sato Y, Hara S,
46. Tang S, Leung JC, Chan LY, Lui YH, Tang Ahuja M, Shortland JR, Vlachojannis JG, Yamada K, Morita S, Eto T: “Point of no
CS, Kan CH, Ho YW, Lai KN: Mycophenolate Brown CB: Prednisolone and azathioprine in return (PNR)” in progressive IgA nephropa-
mofetil alleviates persistent proteinuria in IgA nephropathy - a ten-year follow-up study. thy: Significance of blood pressure and pro-
IgA nephropathy. Kidney Int 68: 802– 812, Nephron Clin Pract 93: C58–C68, 2003 teinuria management up to PNR. J Nephrol
2005 59. Chen KJ, Cheng CH, Wu MJ, Chen CH, Shu 18: 690 – 695, 2005
47. Tang SC, Tang AW, Wong SS, Leung JC, Ho KH: Effect of corticosteroid and cyclophos- 71. Ota F, Ueki K, Naruse T, Nojima Y: Patients
YW, Lai, KN: Long-term study of mycophe- phamide in IgA nephropathy patients with with IgA nephropathy whose renal function
nolate mofetil treatment in IgA nephropa- heavy proteinuria and/or moderate-severe remains stable for a long time even after ex-
thy. Kidney Int 77: 543–549 pathological changes. J Chin Med Assoc 66: ceeding the “point of no return”. Clin Nephrol
48. Maes BD, Oyen R, Claes K, Evenepoel P, 263–270, 2003 54: 175–176, 2000
Kuypers D, Vanwalleghem J, Van Damme B, 60. Hotta O, Taguma Y, Yoshizawa N, Oda T, 72. Hou FF, Zhang X, Zhang GH, Xie D, Chen
Vanrenterghem YF: Mycophenolate mofetil Nishiyama J, Yusa N, Chiba S, Horigome I, PY, Zhang WR, Jiang JP, Liang M, Wang GB,
in IgA nephropathy: Results of a 3-year pro- Sudo K, Tomioka S: Long-term effects of Liu ZR, Geng RW: Efficacy and safety of
spective placebo-controlled randomized intensive therapy combined with tonsillec- benazepril for advanced chronic renal insuf-
study. Kidney Int 65: 1842–1849, 2004 tomy in patients with IgA nephropathy. Acta ficiency. N Engl J Med 354: 131–140, 2006
49. Frisch G, Lin J, Rosenstock J, Markowitz G, Otolaryngol Suppl 523: 165–168, 1996 73. Rivera F, Lopez-Gomez JM, Perez-Garcia R:
D’Agati V, Radhakrishnan J, Preddie D, 61. Tsuruya K, Harada A, Hirakata H, Mitsuiki K, Clinicopathologic correlations of renal pa-
Crew J, Valeri A, Appel G: Mycophenolate Johko T, Kondoh H, Takechi S, Fujishima M: thology in Spain. Kidney Int 66: 898 –904,
mofetil (MMF) vs placebo in patients with Combination therapy using prednisolone 2004
moderately advanced IgA nephropathy: A and cyclophosphamide slows the progres- 74. Gutierrez E, Gonzalez E, Hernandez E, Mo-
double-blind randomized controlled trial. sion of moderately advanced IgA nephrop- rales E, Martinez MA, Usera G, Praga M:
Nephrol Dial Transplant 20: 2139 –2145, athy. Clin Nephrol 53: 1–9, 2000 Factors that determine an incomplete re-
2005 62. Woo KT, Lee GS, Lau YK, Chiang GS, Lim covery of renal function in macrohematu-
50. Dal Canton A, Amore A, Barbano G, Coppo R, CH: Effects of triple therapy in IgA nephritis: ria-induced acute renal failure of IgA ne-
Emma F, Grandaliano G, Klersy C, Perfumo F, A follow-up study 5 years later. Clin Nephrol phropathy. Clin J Am Soc Nephrol 2: 51–
Rizzoni G, Schena FP, Sepe V: One-year ang- 36: 60 – 66, 1991 57, 2007
iotensin-converting enzyme inhibition plus 63. Walker RG, Yu SH, Owen JE, Kincaid-Smith 75. Harper L, Ferreira MA, Howie AJ, Savage
mycophenolate mofetil immunosuppression P: The treatment of mesangial IgA nephrop- CO, Richards NT, Michael J, Adu D: Treat-
in the course of early IgA nephropathy: A athy with cyclophosphamide, dipyridamole ment of vasculitic IgA nephropathy. J Neph-
multicenter, randomised, controlled study. and warfarin: A two-year prospective trial. rol 13: 360 –366, 2000
J Nephrol 18: 136 –140, 2005 Clin Nephrol 34: 103–107, 1990 76. Roccatello D, Ferro M, Coppo R, Giraudo
51. Chen X, Chen P, Cai G, Wu J, Cui Y, Zhang 64. Yoshikawa N, Ito H, Sakai T, Takekoshi Y, G, Quattrocchio G, Piccoli G: Report on
Y, Liu S, Tang L: [A randomized control trial Honda M, Awazu M, Ito K, Iitaka K, Koit- intensive treatment of extracapillary glo-
of mycophenolate mofeil treatment in se- abashi Y, Yamaoka K, Nakagawa K, Naka- merulonephritis with focus on crescentic
vere IgA nephropathy]. Zhonghua Yi Xue Za mura H, Matsuyama S, Seino Y, Takeda N, IgA nephropathy. Nephrol Dial Transplant
Zhi 82: 796 – 801, 2002 Hattori S, Ninomiya M: A controlled trial of 10: 2054 –2059, 1995
52. Floege J: Is mycophenolate mofetil an effec- combined therapy for newly diagnosed se- 77. Tumlin JA, Lohavichan V, Hennigar R:
tive treatment for persistent proteinuria in vere childhood IgA nephropathy. The Japa- Crescentic, proliferative IgA nephropathy:
patients with IgA nephropathy? Nat Clin nese Pediatric IgA Nephropathy Treatment Clinical and histological response to meth-
Pract Nephrol 2: 16 –17, 2006 Study Group. J Am Soc Nephrol 10: 101– ylprednisolone and intravenous cyclo-
53. Lv J, Zhang H, Cui Z, Su T, Zhang Y, Wang H: 109, 1999 phosphamide. Nephrol Dial Transplant 18:
Delayed severe pneumonia in mycophenolate 65. Yoshikawa N, Honda M, Iijima K, Awazu M, 1321–1329, 2003
mofetil-treated patients with IgA nephropa- Hattori S, Nakanishi K, Ito H: Steroid treat- 78. Pankhurst T, Lepenies J, Nightingale P,
thy. Nephrol Dial Transplant 23: 2868–2872, ment for severe childhood IgA nephropathy: Howie AJ, Adu D, Harper L: Vasculitic IgA
2008 A randomized, controlled trial. Clin J Am nephropathy: Prognosis and outcome.
54. Yoshikawa N, Nakanishi K, Ishikura K, Hataya Soc Nephrol 1: 511–517, 2006 Nephron Clin Pract 112: c16 – c24, 2009
H, Iijima K, Honda M: Combination therapy 66. Ballardie FW, Roberts IS: Controlled pro- 79. Lai KN, Lai FM, Ho CP, Chan KW: Cortico-
with mizoribine for severe childhood IgA ne- spective trial of prednisolone and cytotoxics steroid therapy in IgA nephropathy with ne-
phropathy: A pilot study. Pediatr Nephrol in progressive IgA nephropathy. J Am Soc phrotic syndrome: A long-term controlled
23: 757–763, 2008 Nephrol 13: 142–148, 2002 trial. Clin Nephrol 26: 174 –180, 1986
55. Chabova V, Tesar V, Zabka J, Rychlik I, 67. Rasche FM, Keller F, von Muller L, Sailer LK, 80. Nasr SH, Fidler ME, Valeri AM, Cornell LD,
Merta M, Jirsa M Jr., Stejskalova A: Long- Karges W, Czock D: Mycophenolic acid ther- Sethi S, Zoller A, Stokes MB, Markowitz GS,
term treatment of IgA nephropathy with cy- apy after cyclophosphamide pulses in pro- D’Agati VD: Postinfectious glomerulone-
closporin A–a preliminary report. Nephrol gressive IgA nephropathy. J Nephrol 19: phritis in the elderly. J Am Soc Nephrol 22:
Dial Transplant 12: 2206 –2207, 1997 465– 472, 2006 187–195, 2011
56. Lai KN, Lai FM, Li PK, Vallance-Owen J: Cy- 68. D’Amico G, Ragni A, Gandini E, Fellin G: 81. Endo Y, Matsushita H, Nozawa Y, Nishikage
closporin treatment of IgA nephropathy: A Typical and atypical natural history of IgA S, Matsuya S, Hara M: Glomerulonephritis
short term controlled trial. BMJ (Clin Res Ed) nephropathy in adult patients. Contrib associated with liver cirrhosis. Acta Pathol
295: 1165–1168, 1987 Nephrol 104: 6 –13, 1993 Jpn 33: 333–346, 1983
J Am Soc Nephrol 22: 1785–1794, 2011 IgA Nephropathy 1793BRIEF REVIEW www.jasn.org
82. Saulsbury FT: Henoch-Schonlein pur- 84. Zaffanello M, Fanos V: Treatment-based lit- mycophenolate mofetil. Nephrol Dial Trans-
pura. Curr Opin Rheumatol 22: 598 – 602, erature of Henoch-Schonlein purpura ne- plant 20: 1214 –1221, 2005
2010 phritis in childhood. Pediatr Nephrol 24: 86. Courtney AE, McNamee PT, Nelson WE,
83. Chartapisak W, Opastirakul S, Hodson EM, 1901–1911, 2009 Maxwell AP: Does angiotensin bloc-
Willis NS, Craig JC: Interventions for pre- 85. Chandrakantan A, Ratanapanichkich P, Said kade influence graft outcome in renal
venting and treating kidney disease in He- M, Barker CV, Julian BA: Recurrent IgA ne- transplant recipients with IgA nephropa-
noch-Schonlein Purpura (HSP). Cochrane phropathy after renal transplantation de- thy? Nephrol Dial Transplant 21: 3550 –
Database Syst Rev CD005128, 2009 spite immunosuppressive regimens with 3554, 2006
1794 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1785–1794, 2011You can also read