American Journal Cardiology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The
American
Journal
of
Cardiology ®
JUNE 15, 2004
Efficacy and Safety of Ezetimibe Co-
Administered With Simvastatin
Compared With Atorvastatin in Adults
With Hypercholesterolemia
Christie M. Ballantyne, MD, Michael A. Blazing, MD, Thomas R. King, MPH,
William E. Brady, MS, and Joanne Palmisano, MD
EXCERPTA MEDICADear Doctor: We are pleased to present to you the article, “Efficacy and Safety of Ezetimibe Co-Administered With Simvastatin Compared With Atorvastatin in Adults With Hypercholesterolemia,” by Christie Ballantyne et al, as published in The American Journal of Cardiology, Vol. 93, June 15, 2004. VYTORIN (ezetimibe/simvastatin) is indicated as adjunctive therapy to diet for the reduction of elevated TOTAL-C, LDL-C, Apo B, TG, and non–HDL-C, and to increase HDL-C in patients with primary (heterozygous familial and nonfamilial) hypercholesterolemia or mixed hyperlipidemia when diet alone is not enough. VYTORIN is contraindicated in patients with hypersensitivity to any component of this medication; active liver disease; unexplained persistent elevations of serum transaminases; and women who are pregnant, nursing, or may become pregnant. Skeletal Muscle: Myopathy sometimes takes the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria, and rare fatalities have occurred. The risk of myopathy/rhabdomyolysis is dose related. Tell patients to promptly report muscle pain, tenderness, or weakness. Discontinue drug if myopathy is suspected or CPK levels rise markedly. Myopathy Caused by Drug Interactions: Use of VYTORIN with itraconazole, ketoconazole, erythromycin, clarithromycin, telithromycin, HIV protease inhibitors, nefazodone, or large quantities of grapefruit juice (>1 quart daily) should be avoided because of the increased risk of myopathy, particularly at higher doses. The concomitant use of VYTORIN and fibrates should be avoided. The benefit of further alterations in lipid levels by the combined use of VYTORIN with niacin should be carefully weighed against the potential risks of myopathy. The dose of VYTORIN should not exceed 10/10 mg daily in patients receiving cyclosporine or danazol, and 10/20 mg daily in patients receiving amiodarone or verapamil. Liver: It is recommended that liver function tests be performed before the initiation of treatment and thereafter when clinically indicated. Additional tests are recommended prior to and 3 months after titration to the 10/80-mg dose, and semiannually for the first year thereafter. VYTORIN is not recommended in patients with moderate or severe hepatic insufficiency. In clinical trials, the most commonly reported side effects, regardless of cause, included headache (6.8%), influenza (2.6%), upper respiratory tract infection (3.9%), myalgia (3.5%), and extremity pain (2.3%). VYTORIN tablets contain ezetimibe and simvastatin: 10 mg of ezetimibe and 10, 20, 40, or 80 mg of simvastatin (VYTORIN 10/10, 10/20, 10/40, or 10/80, respectively). Before prescribing VYTORIN, please read the enclosed Prescribing Information. Sincerely, Harold Rupell Professional Services Enclosure: Prescribing Information for VYTORIN VYTORIN is a trademark of MSP Singapore Company, LLC. 20405754(5)-VYT VYR0011
Efficacy and Safety of Ezetimibe Co-
Administered With Simvastatin
Compared With Atorvastatin in Adults
With Hypercholesterolemia
Christie M. Ballantyne, MD, Michael A. Blazing, MD, Thomas R. King, MPH,
William E. Brady, MS, and Joanne Palmisano, MD
This study compared the efficacy and safety of co-admin- terol and HDL cholesterol) comparing co-administration of
istered ezetimibe ⴙ simvastatin with atorvastatin mono- 10/80 mg of ezetimibe ⴙ simvastatin with 80 mg of
therapy in adults with hypercholesterolemia. Seven hun- atorvastatin. Baseline LDL and HDL cholesterol levels were
dred eighty-eight patients were randomized 1:1:1 to 3 comparable between treatment groups. At the end of treat-
treatment groups; each group was force-titrated over four ment period 1, the mean decrease of LDL cholesterol was
6-week treatment periods: (1) 10 mg of atorvastatin as the significantly (pTABLE 1 Treatment Plan by Six-Week Treatment Periods
Period 1 Period 2 Period 3 Period 4
(wks 1–6) (wks 7–12) (wks 13–18) (wks 19–24)
Treatment group 1 Atorvastatin 10 mg Atorvastatin 20 mg Atorvastatin 40 mg Atorvastatin 80 mg
Treatment group 2 Ezetimibe 10 mg Ezetimibe 10 mg Ezetimibe 10 mg Ezetimibe 10 mg
⫹ simvastatin ⫹ simvastatin ⫹ simvastatin ⫹ simvastatin
10 mg 20 mg 40 mg 80 mg
Treatment group 3 Ezetimibe 10 mg Ezetimibe 10 mg Ezetimibe 10 mg Ezetimibe 10 mg
⫹ simvastatin ⫹ simvastatin ⫹ simvastatin ⫹ simvastatin
20 mg 40 mg 40 mg 80 mg
gram Adult Treatment Panel III guidelines1 were eli- tified central laboratory (Medical Research Laborato-
gible for enrollment if they met the following criteria: ries International, Highland Heights, Kentucky) ac-
established coronary heart disease or its risk equiva- cording to standards specified by the National Heart
lent, or with ⱖ2 risk factors conferring a 10-year risk Lung and Blood Institute and Centers for Disease
of ⬎20% for coronary heart disease (Framingham Control and Prevention.2 All lipid assessments were
score), and with LDL cholesterol ⱖ130 mg/dl; no blinded after randomization. Calculations of LDL
coronary heart disease or its risk equivalent, and with cholesterol levels were carried out with Friedewald’s
ⱖ2 risk factors conferring a 10-year risk of ⬍20% for equation.3
coronary heart disease, and with LDL cholesterol Data and statistical analyses: This study, with a
ⱖ160 mg/dl; and no coronary heart disease or its risk sample size of 180 patients per treatment group, had
equivalent with ⬍2 risk factors and with LDL choles- 90% power to detect a 5% difference in the mean
terol ⱖ190 mg/dl. Other criteria included fasting se- percent change from baseline in LDL cholesterol be-
rum triglyceride level ⱕ350 mg/dl, alanine amino- tween co-administration of 10/10 mg of ezetimibe ⫹
transferase or aspartate aminotransferase level ⬍1.5 simvastatin and 10 mg of atorvastatin, assuming an
times the upper limit of normal, serum creatinine level SD of 14.5% and a significance level of 0.05 (2-
ⱕ1.5 mg/dl, no active liver disease, creatine kinase sided). With 360 patients in the 10/80 mg ezetimibe ⫹
level ⬍1.5 times the upper limit of normal, and an simvastatin group (the 2 ezetimibe ⫹ simvastatin
hemoglobin A-1C level ⬍9% in patients with groups were combined in period 4) and 180 patients in
diabetes. the 80 mg atorvastatin group, this study had 86%
Efficacy and safety assessments: The primary effi- power to detect a 3.5% treatment difference in mean
cacy measure was mean percent change in LDL cho- percent change from baseline in HDL cholesterol,
lesterol from baseline to the end of the initial 6-week assuming a within-group SD of 12.5% and a signifi-
treatment period. Key secondary efficacy measures cance level of 0.05 (2-sided).
included percent change in LDL cholesterol from Analysis of the primary efficacy parameter was
baseline to the ends of the second and fourth (final) carried out by using a modified intention-to-treat ap-
6-week treatment periods and percent change in high- proach that included all randomized patients with a
density lipoprotein (HDL) cholesterol from baseline to valid baseline and ⱖ1 on-treatment measurement. Be-
the end of the final 6-week treatment period. Other cause patients received a larger statin dose in succes-
efficacy measures included percent changes across the sive treatment periods, the last available efficacy mea-
ezetimibe ⫹ simvastatin and atorvastatin dose ranges surement was not carried forward to subsequent
in other lipid parameters: apolipoprotein B, apoli- periods for patients who discontinued the study early.
poprotein A-I, apolipoprotein B/apolipoprotein A-I, The last available efficacy measurement within a treat-
total cholesterol, non-HDL cholesterol, and ment period was used in the analysis of percent
triglycerides. change from baseline to the end of that period.
Key safety variables were the incidence of any An analysis of variance model with terms for treat-
clinical or laboratory adverse event, serious adverse ment and baseline LDL cholesterol strata (ⱖ130 and
events, and drug-related adverse events. Investigators ⬍160 mg/dl, ⱖ160 and ⬍190 mg/dl, and ⱖ190 mg/
defined clinical adverse events based on signs, symp- dl) was used to compare treatments and provide esti-
toms, and similar observations; laboratory adverse mates of between-treatment differences. Within-treat-
events were based on laboratory test results. Drug- ment adjusted mean percent changes from baseline
related adverse events were identified by blinded in- and SEs obtained from the analysis of variance model
vestigators as being possibly, probably, or definitely are presented.
drug related. Prespecified safety variables included the A closed testing procedure, with 10/20 mg of
incidence of consecutive elevations of ⱖ3 times the ezetimibe ⫹ simvastatin versus 10 mg of atorvastatin
upper limit of normal for alanine aminotransferase or as the first step and 10/10 mg of ezetimibe ⫹ simva-
aspartate aminotransferase and creatine kinase eleva- statin versus 10 mg of atorvastatin as the second step,
tions ⱖ10 times the upper limit of normal, with or was used to address the primary hypothesis (10 mg of
without muscle symptoms. ezetimibe ⫹ simvastatin results in a greater mean
Laboratory methods: Analyses of samples for all decrease in LDL cholesterol than does 10 mg of
clinical laboratory measures were performed at a cer- atorvastatin at the end of treatment period 1). This
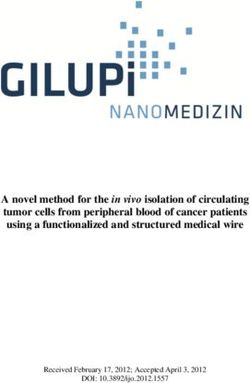
1488 THE AMERICAN JOURNAL OF CARDIOLOGY姞 VOL. 93 JUNE 15, 2004FIGURE 1. Number of patients randomized in the study and number of patients continuing into each period and completing the study
by treatment. *Atorvastatin, 10 mg start dose, titrated to 20, 40, and 80 mg through weeks 6, 12, 18, and 24. †Ezetimibe ⴙ simva-
statin: 10/10 mg start dose titrated to 10/20, 10/40, and 10/80 mg through weeks 6, 12, 18, and 24. ‡Ezetimibe ⴙ simvastatin:
10/20 mg start dose titrated to 10/40, 10/40, and 10/80 mg through weeks 6, 12, 18, and 24. AE ⴝ adverse event.
statistical process proceeded in a stepwise fashion statin treatment groups were combined. In analyses of
until lack of significance was observed to determine percent changes in LDL and HDL cholesterol aver-
the minimal detectable dose that was statistically sig- aged across all treatment periods, only patients in the
nificantly different from 10 mg of atorvastatin. The group receiving 10/10 mg of ezetimibe ⫹ simvastatin
procedure was discontinued at the step when lack of as the initial dose were compared with patients receiv-
significance was observed. ing atorvastatin, because only these 2 treatment arms
The analysis of variance model for the analysis of had equal doses of simvastatin and atorvastatin in all
the primary measure was also used for other efficacy 4 treatment periods. For the skewed distribution of
measurements: percent changes in LDL cholesterol triglycerides, the analysis of variance model was an-
from baseline to the ends of the second, third, and alyzed by using rank-transformed values using
fourth 6-week treatment periods; percent changes in Tukey’s normal scores.
HDL cholesterol and other lipids from baseline to the All patients who received ⱖ1 dose of double-blind
ends of each 6-week treatment period; and percent study medication (modified intention-to-treat popula-
changes in LDL and HDL cholesterol from baseline tion) were included in the safety analyses. An overall
averaged across all treatment periods. For analyses of summary of adverse events (including percentages of
LDL and HDL cholesterol in the third and fourth patients with ⱖ1 adverse events, drug-related adverse
6-week treatment periods, the 2 ezetimibe ⫹ simva- events, serious adverse events, and discontinuations
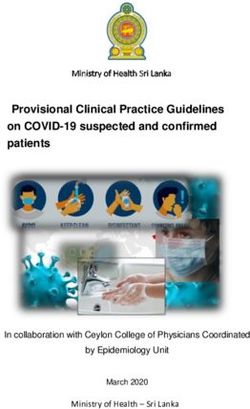
PREVENTIVE CARDIOLOGY/EZETIMIBE ⫹ SIMVASTATIN VS ATORVASTATIN FOR HYPERCHOLESTEROLEMIA 1489from baseline compared with 37.2%
TABLE 2 Baseline Patient Characteristics
for 10 mg of atorvastatin, a statisti-
Start Dose cally significant difference (⫺8.9%;
Atorvastatin Ezetimibe 10 mg ⫹ Ezetimibe 10 mg ⫹ 95% confidence interval ⫺11.1 to
10 mg* Simvastatin 10 mg† Simvastatin 20 mg‡ ⫺6.7, p ⬍0.001), and 10/20 mg of
(n ⫽ 262) (n ⫽ 263) (n ⫽ 263) ezetimibe ⫹ simvastatin resulted in a
Men 131 (50.0%) 141 (53.6%) 138 (52.5%) 50.3% mean decrease in LDL cho-
Women 131 (50.0%) 122 (46.4%) 125 (47.5%) lesterol from baseline, which was
Age (yrs)¶ 60.8 ⫾ 9.99 59.4 ⫾ 10.62 59.9 ⫾ 10.88 also significantly different (⫺13.1%,
Race 95% confidence interval ⫺15.2 to
White 234 (89.3%) 242 (92.0%) 236 (89.7%)
Black 10 (3.8%) 13 (4.9%) 13 (4.9%) ⫺10.9, p ⬍0.001) compared with 10
Hispanic 11 (4.2%) 5 (1.9%) 8 (3.0%) mg of atorvastatin (Table 3 and Fig-
Asian 5 (1.9%) 2 (0.8%) 3 (1.1%) ure 2). Mean percent decreases in
Other 2 (0.8%) 1 (0.4%) 3 (1.1%) LDL cholesterol from baseline for
Baseline lipid values# (mg/dl)
LDL cholesterol §
180.6 ⫾ 45.6 180.0 ⫾ 41.3 179.2 ⫾ 41.7
ezetimibe ⫹ simvastatin were also
HDL cholesterol§ 46.9 ⫾ 11.4 46.6 ⫾ 12.2 46.8 ⫾ 10.7 significantly greater compared with
Total cholesterol§ 266.8 ⫾ 49.8 265.5 ⫾ 45.9 264.0 ⫾ 43.7 atorvastatin for treatment periods 2
Triglycerides㛳 171.5 (94.0) 174.5 (93.5) 176.0 (108.8) and 3 and are listed in Table 3 and
Non-HDL cholesterol§ 219.8 ⫾ 48.3 218.9 ⫾ 43.9 217.2 ⫾ 41.5 displayed in Figure 2.
Apolipoprotein A-I §
151.9 ⫾ 26.4 150.3 ⫾ 28.1 149.7 ⫾ 23.2
Apolipoprotein B§ 169.7 ⫾ 33.8 171.5 ⫾ 33.4 169.1 ⫾ 30.7 At the end of treatment period 4
Apolipoprotein B/ 1.1 ⫾ 0.3 1.2 ⫾ 0.3 1.2 ⫾ 0.3 (24 weeks), treatment with 10/80 mg
apolipoprotein A-I§ of ezetimibe ⫹ simvastatin resulted
*Atorvastatin 10-mg start dose titrated to 20, 40, and 80 mg through weeks 6, 12, 18, and 24.
in a 59.4% mean decrease in LDL
†
Ezetimibe ⫹ simvastatin: 10/10-mg start dose titrated to 10/20, 10/40, and 10/80 mg through cholesterol from baseline compared
weeks 6, 12, 18, and 24. with 52.5% for 80 mg of atorvasta-
‡
Ezetimibe ⫹ simvastatin: 10/20-mg start dose titrated to 10/40, 10/40, and 10/80 mg through tin. This difference (⫺6.9%) was sta-
weeks 6, 12, 18, and 24.
§
Baseline values are means ⫾ SD.
tistically significant (95% confidence
㛳
Baseline values are medians (robust SD ⫽ interquartile range/1.075). interval ⫺9.2 to ⫺4.6, p ⬍0.001)
¶
Mean (SD). (Table 3 and Figure 2).
#
Baseline lipid values are for the modified intention-to-treat poulation. When averaged across the entire
dose range, mean percent decreases
in LDL cholesterol from baseline
were 52.4% for the ezetimibe ⫹ sim-
due to an adverse event) was presented by treatment vastatin group (treatment group 2) compared with
group. Fisher’s exact tests were used for analysis of 45.1% for the atorvastatin group, resulting in a statis-
the pairwise comparisons between treatment groups tically significant difference (⫺7.3%, 95% confidence
for the following predefined elevations: consecutive interval ⫺9.3 to ⫺5.3, p ⬍0.001).
elevations alanine aminotransferase and/or aspartate Mean HDL cholesterol levels for patients treated
aminotransferase ⱖ3 times the upper limit of normal, with 10/80 mg of ezetimibe ⫹ simvastatin increased
creatine kinase elevations ⱖ10 times the upper limit by 12.3% at the end of treatment period 4 compared
of normal, and creatine kinase elevations ⱖ10 times with 6.5% for patients treated with 80 mg of atorva-
the upper limit of normal with muscle symptoms. statin. This difference (5.9%) was statistically signif-
icant in favor of 10/80 mg of ezetimibe ⫹ simvastatin
RESULTS (95% confidence interval 3.5 to 8.2, p ⬍0.001) (Table
Demographic and baseline characteristics: Seventy- 3 and Figure 2).
eight study sites in the United States screened 1,901 When averaged across the entire dose range, mean
patients to randomize 788 (262 in the group receiving percent increases in HDL cholesterol from baseline
10 mg of atorvastatin as the initial dose, 263 in the were 9.5% for the ezetimibe ⫹ simvastatin group
group receiving 10/10 mg of ezetimibe/simvastatin as (treatment group 2) compared with 6.2% for the ator-
the initial dose, and 263 in the group receiving 10/20 vastatin group, a 3.2% difference that was statistically
of ezetimibe ⫹ simvastatin as the initial dose). Of the significant in favor of the co-administered drugs (95%
1,113 nonrandomized patients, 909 did not meet eli- confidence interval 1.2 to 5.3, p ⫽ 0.002).
gibility criteria and 139 withdrew consent before ran- Other lipid parameters (total cholesterol, apoli-
domization. The most frequent reasons for ineligibil- poprotein B, apolipoprotein A-I, apolipoprotein
ity were low LDL cholesterol levels or triglyceride B/apolipoprotein A-I, and non-HDL cholesterol) were
levels ⬎350 mg/dl. Patient disposition is shown in also significantly improved with ezetimibe ⫹ simva-
Figure 1. Treatment groups appeared well balanced statin compared with atorvastatin. Changes in triglyc-
with respect to baseline patient characteristics (Table erides did not differ significantly between treatment
2). groups (Table 3 and Figure 2).
Efficacy analyses: At the end of treatment period 1 Safety: The treatment groups were similar with
(6 weeks), 10/10 mg of ezetimibe ⫹ simvastatin re- regard to incidences of (1) any clinical adverse event,
sulted in a 46.1% mean decrease in LDL cholesterol (2) drug-related clinical adverse events, and (3) clin-
1490 THE AMERICAN JOURNAL OF CARDIOLOGY姞 VOL. 93 JUNE 15, 2004TABLE 3 Summary of Efficacy Results in the Modified Intention-to-treat Population (mean ⫾ [SE] percent change from baseline)†
Apolipoprotein
Total LDL HDL Non–HDL Apolipoprotein B/Apolipoprotein
Treatment Cholesterol Cholesterol Apolipoprotein B Cholesterol Triglycerides* Cholesterol A-I A-I
Wk 6
Atorvastatin 10 mg‡ ⫺28.1 (0.6) ⫺37.2 (0.8) ⫺31.7 (0.7) 5.1 (0.8) ⫺22.5 (1.8) ⫺35.1 (0.7) 1.6 (0.7) ⫺32.2 (0.7)
Ezetimibe ⫹ simvastatin 10/10 mg§ ⫺33.9 (0.6)¶ ⫺46.1 (0.8)¶ ⫺37.7 (0.7)¶ 8.0 (0.8)¶ ⫺26.3 (1.5) ⫺42.7 (0.7)¶ 4.1 (0.7)¶ ⫺39.7 (0.7)¶
Ezetimibe ⫹ simvastatin 10/20 mg㛳 ⫺36.2 (0.6)¶ ⫺50.3 (0.8)¶ ⫺41.2 (0.7)¶ 9.5 (0.8)¶ ⫺24.6 (2.0) ⫺46.2 (0.7)¶ 4.6 (0.7)¶ ⫺43.2 (0.7)¶
Wk 12
Atorvastatin 20 mg‡ ⫺33.1 (0.6) ⫺44.3 (0.9) ⫺37.7 (0.7) 6.9 (0.9) ⫺28.4 (1.7) ⫺41.6 (0.8) 2.0 (0.7) ⫺38.5 (0.8)
Ezetimibe ⫹ simvastatin 10/20 mg§ ⫺36.5 (0.6)¶ ⫺50.2 (0.8)¶ ⫺40.6 (0.7)¶ 9.0 (0.9) ⫺27.7 (1.9) ⫺46.2 (0.8)¶ 5.4 (0.7)¶ ⫺43.2 (0.8)¶
Ezetimibe ⫹ simvastatin 10/40 mg㛳 ⫺39.2 (0.6)¶ ⫺54.3 (0.8)¶ ⫺44.9 (0.7)¶ 12.4 (0.9)¶ ⫺30.8 (1.7) ⫺50.3 (0.8)¶ 6.0 (0.7)¶ ⫺47.4 (0.8)¶
Wk 18
Atorvastatin 40 mg‡ ⫺37.0 (0.7) ⫺49.1 (0.9) ⫺42.3 (0.8) 7.8 (1.0) ⫺31.2 (1.8) ⫺46.5 (0.8) 1.3 (0.8) ⫺42.2 (0.8)
Ezetimibe ⫹ simvastatin 10/40 mg§㛳# ⫺40.5 (0.5)¶ ⫺55.6 (0.6)¶ ⫺45.3 (0.5)¶ 11.4 (0.7)¶ ⫺32.0 (1.3) ⫺51.6 (0.5)¶ 4.9 (0.6)¶ ⫺47.3 (0.6)¶
Wk 24
Atorvastatin 80 mg‡ ⫺40.2 (0.7) ⫺52.5 (1.0) ⫺45.2 (0.8) 6.5 (1.0) ⫺34.8 (1.9) ⫺50.3 (0.9) ⫺1.2 (0.8) ⫺44.1 (0.8)
Ezetimibe ⫹ simvastatin 10/80 mg§㛳# ⫺43.3 (0.5)¶ ⫺59.4 (0.7)¶ ⫺48.6 (0.6)¶ 12.3 (0.7)¶ ⫺35.3 (1.2) ⫺55.3 (0.6)¶ 4.7 (0.6)¶ ⫺50.5 (0.6)¶
*For triglycerides, median percent change from baseline, with robust SE ⫽ (interquartile range/1.075)/n.
†
Baseline— on no lipid-lowering drug.
‡
Atorvastatin: 10-mg start dose titrated to 20 mg, 40 mg, and 80 mg through weeks 6, 12, 18, and 24.
§
Ezetimibe ⫹ simvastatin: 10/10-mg start dose titrated to 10/20 mg, 10/40 mg, and 10/80 mg through weeks 6, 12, 18, and 24.
㛳
Ezetimibe ⫹ simvastatin: 10/20-mg start dose titrated to 10/40 mg, 10/40 mg, and 10/80 mg through weeks 6, 12, 18, and 24.
¶
p ⱕ0.05 for difference with atorvastatin in the specified week.
#
Data pooled for common doses of ezetimibe ⫹ simvastatin at weeks 18 and 24.
PREVENTIVE CARDIOLOGY/EZETIMIBE ⫹ SIMVASTATIN VS ATORVASTATIN FOR HYPERCHOLESTEROLEMIA
1491FIGURE 2. Least-squares (adjusted) mean (ⴞSE) percent changes in (A) LDL cholesterol, (B) HDL cholesterol, (C) apolipoprotein B (apo B), (D) non-HDL cholesterol, (E) apolipoprotein A-I (apo A-I), and (F) median (ⴞrobust SE ⴝ [interquartile range/1.075/n]) percent changes in triglycerides by dose of atorvastatin and 10 mg of ezetimibe ⴙ simvastatin. Within each dose, only those patients treated within the same titration period are shown (i.e., period 1 for 10 mg, period 2 for 20 mg, period 3 for 40 mg, and period 4 for 80 mg). *p
served for ezetimibe ⫹ simvastatin
TABLE 4 Summary of Patients Exceeding the Predefined Limits of Change in
Alanine Aminotransferase, Aspartate Aminotransferase, and Creatine Kinase at compared with atorvastatin when av-
Any Point in the Study eraged across the entire dose range.
Changes in triglyceride levels were
Start Dose*
similar between ezetimibe ⫹ simvasta-
Ezetimibe 10 mg Ezetimibe 10 mg tin and atorvastatin, consistent with the
Atorvastatin ⫹ Simvastatin ⫹ Simvastatin mechanism of action of ezetimibe and
Laboratory Parameter 10 mg 10 mg 20 mg
its specific effect on intestinal absorp-
Alanine aminotransferase tion of cholesterol.6 – 8 Co-administra-
ⱖ3⫻ upper limit of normal, 6/252 (2.4) 6/256 (2.3) 5/255 (2.0) tion of 10 mg of ezetimibe and 80 mg
consecutive†
Aspartate aminotransferase of simvastatin compared with 80 mg
ⱖ3⫻ upper limit of normal, 2/252 (0.8) 3/256 (1.2) 0/255 (0.0) of atorvastatin and the averaged results
consecutive† for each treatment titrated across the
Alanine aminotransferase and/or dose range showed that ezetimibe ⫹
aspartate aminotransferase
ⱖ3⫻ upper limit of normal, 6/252 (2.4) 6/256 (2.3) 5/255 (2.0)
simvastatin was significantly more ef-
consecutive† fective than atorvastatin in increasing
Creatine kinase levels of HDL cholesterol from base-
ⱖ10⫻ upper limit of normal, without 0/252 (0.0) 1/256 (0.4)‡ 1/255 (0.4)§ line.
muscle symptoms
㛳
Ezetimibe ⫹ simvastatin was
ⱖ10⫻ upper limit of normal, with 0/252 (0.0) 1/256 (0.4) 0/255 (0.0)
muscle symptoms well tolerated in this study and did
not increase the risk of clinically sig-
*Number of patients with increased levels/number of patients tested (%).
†
nificant increases in muscle or liver
This category includes patients with (1) 2 consecutive measurements for alanine aminotransferase
and/or aspartate aminotransferase ⱖ3 times the upper limit of normal, (2) a single, last measurement
enzymes compared with atorvastatin,
ⱖ3 times the upper limit of normal, or (3) a measurement ⱖ3 times the upper limit of normal followed and there were no differences in clin-
by a measurement ⬍3 times the upper limit of normal that was taken more than 2 days after the last dose ical drug-related adverse events or
of study medication. study discontinuations due to drug-
‡
Occurred while patient was receiving 10/20 mg of ezetimibe ⫹ simvastatin.
§
Occurred while patient was receiving 10/40 mg of ezetimibe ⫹ simvastatin.
related adverse events between treat-
㛳
Symptoms occurred while patient was receiving 10/80 mg of ezetimibe ⫹ simvastatin. ment groups. Overall, these safety
results are consistent with those from
a previous trial studying co-adminis-
tration of ezetimibe ⫹ simvastatin.4
adverse events leading to discontinuation, there were By using a treatment strategy that inhibits cholesterol
5.7% (15 of 263) each in the groups receiving 10/10 synthesis and intestinal cholesterol absorption, co-ad-
and 10/20 mg of ezetimibe/simvastatin as the initial ministration of ezetimibe ⫹ simvastatin provided greater
doses and 3.8% (10 of 262) in the group receiving 10 efficacy in decreasing LDL cholesterol than did atorva-
mg of atorvastatin as the first dose. statin at every dose comparison studied.
There were no cases of rhabdomyolysis, and the
incidence of increases for the predefined limit for Acknowledgment: The investigators acknowledge
creatine kinase (ⱖ10 times the upper limit of normal) the contributions of the following clinical investiga-
did not differ significantly across treatment groups. tors for their work on the study on which this report is
All 3 treatment groups had similar incidences of con- based: John E. Angelo, MD, New Orleans, Louisiana;
secutive increases of ⱖ3 times the upper limit of Stanley L. Block, Jr., MD, Bardstown, Kentucky;
normal for alanine aminotransferase, aspartate amino- Harold E. Bays, MD, Louisville, Kentucky; Jacques
transferase, and alanine aminotransferase/aspartate R. Caldwell, MD, Daytona Beach, Florida; David
aminotransferase. Results for liver- and muscle-asso- Capuzzi, MD, PhD, Philadelphia, Pennsylvania; Al-
ciated safety parameters are presented in Table 4. bert A. Carr, MD, Augusta, Georgia; Shane Glade
Christensen, Salt Lake City, Utah; Teresa LeJeune
DISCUSSION Coats, MD, Austin, Texas; Scott E. Conard, MD,
Previous studies have shown that the co-adminis- Irving, Texas; Michael H. Davidson, MD, Chicago,
tration of ezetimibe ⫹ simvastatin is effective and Illinois; Margaret A. Drebohl, MD, San Diego, Cali-
well tolerated,4,5 and a single tablet containing fornia; Bassem M. El-Masri, MD, New York, New
ezetimibe in combination with simvastatin is currently York; Ronald D. Emkey, Jr., MD, Wyomissing, Penn-
under development. In this study, we used a forced sylvania; Mildred V. Farmer, MD, St. Petersburg,
titration design to compare co-administration of Florida; Darrell N. Fiske, MD, Stuart, Florida; David
ezetimibe ⫹ simvastatin with atorvastatin across their L. Fried, MD, Warwick, Rhode Island; Garo S.
respective dose ranges. Co-administration of ezetimibe Garibian, MD, Philadelphia, Pennsylvania; Lawrence
and simvastatin showed significantly greater efficacy I. Gilderman, MD, Pembroke Pines, Florida; Geoffrey
in decreasing levels of LDL cholesterol, non-HDL S. Gladstein, MD, Stamford, Connecticut; Anne Carol
cholesterol, apolipoprotein B, and total cholesterol Goldberg, MD, St. Louis, Missouri; Jonathan A. Har-
compared with atorvastatin at all time points during ris, MD, Endwell, New York; Alan M. Heller, MD,
the titration periods. In addition, significantly greater San Jose, California; Daniel C. Henry, MD, Salt Lake
decreases in these atherogenic lipoproteins were ob- City, Utah; Darrell T. Herrington, DO, San Angelo,
PREVENTIVE CARDIOLOGY/EZETIMIBE ⫹ SIMVASTATIN VS ATORVASTATIN FOR HYPERCHOLESTEROLEMIA 1493Texas; Andrew T. Torkelson, MD, Lebanon, New Fontana, California; James T. Farrell, DO, St. Peters,
Hampshire; Donald B. Hunninglake, MD, Minneapo- Missouri; Richard L. Weinstein, MD, Walnut Creek,
lis, Minnesota; William L. Isley, MD, Kansas City, California; Robert S. Greenfield, MD, Portland, Ore-
Missouri; Sam Lerman, MD, Hollywood, Florida; Ro- gon; Craig M. McCarthy, MD, Mesa, Arizona; Lydia
nald L. Karlsberg, MD, Beverly Hills, California; G. Corn, MD, Sarasota, Florida; Jerry W. Robinson,
Dearing W. Johns, MD, Charlottesville, Virginia; MD, Chester, South Carolina; Xiaohong Helen Wang,
Robert H. Knopp, MD, Seattle, Washington; John A. MD, Pittsburgh, Pennsylvania; Timothy S. Truitt,
Larry, MD, Columbus, Ohio; Dennis H. Linden, MD, MD, Palm Bay, Florida; Andrea C. Schimke, MD,
Medford, Oregon; Robert S. Lipetz, MD, Spring Val- Appleton, Wisconsin; Daniel A. Nadeau, MD, Hamp-
ley, California; Thomas W. Littlejohn III, MD, Win- ton, New Hampshire; James John Del Giorno, MD,
ston-Salem, North Carolina; Anthony P. Lovell, MD, Mesa, Arkansas; Neil J. Fraser, MD, Troy, Michigan;
Springfield, California; Catherine L. Lowder, MD, St. Deborah Matzura-Wolfe, BS, Kevin Gergich, MA,
Louis, Missouri; Antoinette Mangione, MD, Philadel- Rachel McGowen, BS, Heidi Hark, and Michelle
phia, Pennsylvania; Abe Marcadis, MD, Boynton Zhang, MBA. The investigators also thank Denise
Beach, Florida; James Frederick McNeer, MD, Tulsa, Stek, BS, for assistance in the preparation of this
Oklahoma; Michael Miller, MD, Baltimore, Mary- report.
land; Sandip Mukherjee, MD, Guilford, Connecticut;
Daniel A. Nadeau, MD, Bangor, Maine; Mark L.
Henderson, MD, Bangor, Maine; Puneet Narayan, 1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Choles-
MD, Springfield, Virginia; William P. Jennings, MD, terol in Adults. Executive summary of the third report of the National Cholesterol
Education Program (NCEP) expert panel on detection, evaluation, and treatment
San Antonio, Texas; Douglas H. Orchard, MD, Boise, of high blood cholesterol in adults (adult treatment panel III). JAMA 2001;285:
Idaho; Vasilios Papademetriou, MD, Washington, 2486 –2497.
DC; Robert Zorba Paster, MD, Oregon, Wisconsin; 2. Myers GL, Cooper GR, Winn CL, Smith SJ. The Centers for Disease Con-
trol—National Heart, Lung and Blood Institute Lipid Standardization Program.
Terry L. Poling, MD, Wichita, Kansas; James F. An approach to accurate and precise lipid measurements. Clin Lab Med 1989;9:
Quigley, DO, Encinitas, California; James Moody 105–135.
3. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of
Rhyne, MD, Statesville, Maryland; Jeffery B. Rosen, low-density lipoprotein cholesterol in plasma, without use of the preparative
MD, Coral Gables, Florida; Sidney Rosenblatt, MD, ultracentrifuge. Clin Chem 1972;18:499 –502.
Irvine, California; Paul G. Sandall, MD, Albuquerque, 4. Davidson MH, McGarry T, Bettis R, Melani L, Lipka LJ, LeBeaut AP, Suresh
R, Sun S, Veltri EP. Ezetimibe coadministered with simvastatin in patients with
New Mexico; William M. Seger, MD, Fort Worth, primary hypercholesterolemia. J Am Coll Cardiol 2002;40:2125–2134.
Texas; Ross J. Simpson, MD, Chapel Hill, North 5. Gagne C, Bays HE, Weiss SR, Mata P, Quinto K, Melino M, Cho M, Musliner
Carolina; Michael B. Rocco, MD, Cleveland, Ohio; TA, Gumbiner B. Ezetimibe Study Group. Efficacy and safety of ezetimibe added
to ongoing statin therapy for treatment of patients with primary hypercholester-
Jeffrey T. Whitmer, MD, PhD, Cincinnati, Ohio; Paul olemia. Am J Cardiol 2002;90:1084 –1091.
D. Thompson, MD, Hartford, Connecticut; Edward O. 6. Van Heek M, France CF, Compton DS, McLeod RL, Yumibe NP, Alton KB,
Tokatlian, MD, Phoenix, Arizona; Philip D. Toth, Sybertz EJ, Davis HR Jr. In vivo metabolism-based discovery of a potent
cholesterol absorption inhibitor, SCH58235, in the rat and rhesus monkey
MD, Indianapolis, Indiana; Barbara Troupin, MD, San through the identification of the active metabolites of SCH48461. J Pharmacol
Diego, California; Ralph M. Vicari, MD, Melbourne, Exp Ther 1997;283:157–163.
7. Van Heek M, Farley C, Compton DS, Hoos L, Alton KB, Sybertz EJ, Davis
Florida; Harry Wadsworth, MD, St. Louis, Missouri; HR Jr. Comparison of the activity and disposition of the novel cholesterol
William J. Wickenmeyer, MD, Des Moines, Iowa; absorption inhibitor, SCH58235, and its glucuronide, SCH60663. Br J Pharma-
Marco N. Diaz, MD, Portland, Maine; Troy Williams, col 2000;129:1748 –1754.
8. Knopp RH, Bays H, Manion CV, Lipka LJ, Melani L, LeBeaut AP, Suresh R,
MD, Peoria, Arkansas; James M. McKenney, Veltri EP, for the Ezetimibe Study Group. Effect of ezetimibe on serum concen-
PharmD, Richmond, Virginia; Edward A. Hess, MD, trations of lipid-soluble vitamins. Atherosclerosis 2001;2(suppl):90 (abstract).
1494 THE AMERICAN JOURNAL OF CARDIOLOGY姞 VOL. 93 JUNE 15, 2004TM VYTORINTM (ezetimibe/simvastatin) VYTORINTM (ezetimibe/simvastatin)
VYTORIN 10/10
(EZETIMIBE 10 MG/SIMVASTATIN 10 MG TABLETS) Pharmacokinetics (10 mg daily) in patients with moderate hepatic insufficiency, the mean AUC
TM Absorption for total ezetimibe and ezetimibe increased approximately 4-fold compared
VYTORIN 10/20 VYTORIN
VYTORIN is bioequivalent to coadministered ezetimibe and simvastatin.
to healthy subjects.
(EZETIMIBE 10 MG/SIMVASTATIN 20 MG TABLETS) Renal Insufficiency
TM Ezetimibe
VYTORIN 10/40 After oral administration, ezetimibe is absorbed and extensively conjugated
to a pharmacologically active phenolic glucuronide (ezetimibe-glucuronide).
Ezetimibe
After a single 10-mg dose of ezetimibe in patients with severe renal disease
(n=8; mean CrCl ≤30 mL/min/1.73 m2), the mean AUC for total ezetimibe and
(EZETIMIBE 10 MG/SIMVASTATIN 40 MG TABLETS) Effect of Food on Oral Absorption ezetimibe increased approximately 1.5-fold, compared to healthy subjects (n=9).
TM Ezetimibe
VYTORIN 10/80 Concomitant food administration (high-fat or non-fat meals) had no effect
on the extent of absorption of ezetimibe when administered as 10-mg tablets.
Simvastatin
Pharmacokinetic studies with another statin having a similar principal
(EZETIMIBE 10 MG/SIMVASTATIN 80 MG TABLETS) The Cmax value of ezetimibe was increased by 38% with consumption of high- route of elimination to that of simvastatin have suggested that for a given
fat meals. dose level higher systemic exposure may be achieved in patients with severe
renal insufficiency (as measured by creatinine clearance).
DESCRIPTION Simvastatin
Relative to the fasting state, the plasma profiles of both active and total
Drug Interactions (See also PRECAUTIONS, Drug Interactions)
VYTORIN contains ezetimibe, a selective inhibitor of intestinal cholesterol No clinically significant pharmacokinetic interaction was seen when
and related phytosterol absorption, and simvastatin, a 3-hydroxy-3- inhibitors of HMG-CoA reductase were not affected when simvastatin was
ezetimibe was coadministered with simvastatin. Specific pharmacokinetic
methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitor. administered immediately before an American Heart Association
drug interaction studies with VYTORIN have not been performed.
The chemical name of ezetimibe is 1-(4-fluorophenyl)-3(R)-[3-(4- recommended low-fat meal.
Cytochrome P450: Ezetimibe had no significant effect on a series of probe
fluorophenyl)-3(S)-hydroxypropyl]-4(S)-(4-hydroxyphenyl)-2-azetidinone. The Distribution drugs (caffeine, dextromethorphan, tolbutamide, and IV midazolam) known to
empirical formula is C24H21F2NO3 and its molecular weight is 409.4. Ezetimibe be metabolized by cytochrome P450 (1A2, 2D6, 2C8/9 and 3A4) in a “cocktail”
Ezetimibe is a white, crystalline powder that is freely to very soluble in Ezetimibe and ezetimibe-glucuronide are highly bound (>90%) to human study of twelve healthy adult males. This indicates that ezetimibe is neither an
ethanol, methanol, and acetone and practically insoluble in water. Its plasma proteins. inhibitor nor an inducer of these cytochrome P450 isozymes, and it is unlikely
structural formula is: Simvastatin that ezetimibe will affect the metabolism of drugs that are metabolized by
Both simvastatin and its β-hydroxyacid metabolite are highly bound these enzymes.
(approximately 95%) to human plasma proteins. When radiolabeled In a study of 12 healthy volunteers, simvastatin at the 80-mg dose had no
simvastatin was administered to rats, simvastatin-derived radioactivity effect on the metabolism of the probe cytochrome P450 isoform 3A4
crossed the blood-brain barrier. (CYP3A4) substrates midazolam and erythromycin. This indicates that
simvastatin is not an inhibitor of CYP3A4, and, therefore, is not expected to
Metabolism and Excretion affect the plasma levels of other drugs metabolized by CYP3A4.
Ezetimibe Simvastatin is a substrate for CYP3A4. Potent inhibitors of CYP3A4 can
Ezetimibe is primarily metabolized in the small intestine and liver via raise the plasma levels of HMG-CoA reductase inhibitory activity and
glucuronide conjugation with subsequent biliary and renal excretion. increase the risk of myopathy. (See WARNINGS, Myopathy/Rhabdomyolysis
Minimal oxidative metabolism has been observed in all species evaluated. and PRECAUTIONS, Drug Interactions.)
In humans, ezetimibe is rapidly metabolized to ezetimibe-glucuronide. Antacids: In a study of twelve healthy adults, a single dose of antacid
Ezetimibe and ezetimibe-glucuronide are the major drug-derived compounds (SupraloxTM 20 mL) administration had no significant effect on the oral
Simvastatin, an inactive lactone, is hydrolyzed to the corresponding detected in plasma, constituting approximately 10 to 20% and 80 to 90% of the
β-hydroxyacid form, which is an inhibitor of HMG-CoA reductase. Simvastatin total drug in plasma, respectively. Both ezetimibe and ezetimibe-glucuronide
bioavailability of total ezetimibe, ezetimibe-glucuronide, or ezetimibe based
is butanoic acid, 2,2-dimethyl-,1,2,3,7,8,8a-hexahydro-3,7-dimethyl-8-[2- on AUC values. The Cmax value of total ezetimibe was decreased by 30%.
are slowly eliminated from plasma with a half-life of approximately 22 hours
(tetrahydro-4-hydroxy-6-oxo-2H-pyran-2-yl)-ethyl]-1-naphthalenyl ester, for both ezetimibe and ezetimibe-glucuronide. Plasma concentration-time Cholestyramine: In a study of forty healthy hypercholesterolemic
[1S-[1α,3α,7β,8β(2S*,4S*),-8aβ]]. The empirical formula of simvastatin is profiles exhibit multiple peaks, suggesting enterohepatic recycling. (LDL-C ≥130 mg/dL) adult subjects, concomitant cholestyramine (4 g twice
C25H38O5 and its molecular weight is 418.57. daily) administration decreased the mean AUC of total ezetimibe and
Following oral administration of 14C-ezetimibe (20 mg) to human subjects, ezetimibe approximately 55% and 80%, respectively.
Simvastatin is a white to off-white, nonhygroscopic, crystalline powder total ezetimibe (ezetimibe + ezetimibe-glucuronide) accounted for approx-
that is practically insoluble in water, and freely soluble in chloroform, imately 93% of the total radioactivity in plasma. After 48 hours, there were no Cyclosporine: In a study of eight post-renal transplant patients with mildly
methanol and ethanol. Its structural formula is: detectable levels of radioactivity in the plasma. impaired or normal renal function (creatinine clearance of >50 mL/min), stable
doses of cyclosporine (75 to 150 mg twice daily) increased the mean AUC
Approximately 78% and 11% of the administered radioactivity were and Cmax values of total ezetimibe 3.4-fold (range 2.3- to 7.9-fold) and 3.9-fold
recovered in the feces and urine, respectively, over a 10-day collection (range 3.0- to 4.4-fold), respectively, compared to a historical healthy control
period. Ezetimibe was the major component in feces and accounted for 69% population (n=17). In a different study, a renal transplant patient with severe
of the administered dose, while ezetimibe-glucuronide was the major renal insufficiency (creatinine clearance of 13.2 mL/min/1.73 m2) who was
component in urine and accounted for 9% of the administered dose. receiving multiple medications, including cyclosporine, demonstrated a
Simvastatin 12-fold greater exposure to total ezetimibe compared to healthy subjects.
Simvastatin is a lactone that is readily hydrolyzed in vivo to the Fenofibrate: In a study of thirty-two healthy hypercholesterolemic
corresponding β-hydroxyacid, a potent inhibitor of HMG-CoA reductase. (LDL-C ≥130 mg/dL) adult subjects, concomitant fenofibrate (200 mg once
Inhibition of HMG-CoA reductase is a basis for an assay in pharmacokinetic daily) administration increased the mean Cmax and AUC values of total
studies of the β-hydroxyacid metabolites (active inhibitors) and, following ezetimibe approximately 64% and 48%, respectively. Pharmacokinetics of
base hydrolysis, active plus latent inhibitors (total inhibitors) in plasma fenofibrate were not significantly affected by ezetimibe (10 mg once daily).
following administration of simvastatin. The major active metabolites of Gemfibrozil: In a study of twelve healthy adult males, concomitant
simvastatin present in human plasma are the β-hydroxyacid of simvastatin administration of gemfibrozil (600 mg twice daily) significantly increased the
and its 6’-hydroxy, 6’-hydroxymethyl, and 6’-exomethylene derivatives. oral bioavailability of total ezetimibe by a factor of 1.7. Ezetimibe (10 mg once
Plasma concentrations of total radioactivity (simvastatin plus 14C-metabolites) daily) did not significantly affect the bioavailability of gemfibrozil.
VYTORIN is available for oral use as tablets containing 10 mg of peaked at 4 hours and declined rapidly to about 10% of peak by 12 hours Grapefruit Juice: Grapefruit juice contains one or more components that
ezetimibe, and 10 mg of simvastatin (VYTORIN 10/10), 20 mg of simvastatin postdose. Simvastatin undergoes extensive first-pass extraction in the liver, its inhibit CYP3A4 and can increase the plasma concentrations of drugs
(VYTORIN 10/20), 40 mg of simvastatin (VYTORIN 10/40), or 80 mg of simvastatin primary site of action, with subsequent excretion of drug equivalents in the bile. metabolized by CYP3A4. In one study1, 10 subjects consumed 200 mL of double-
(VYTORIN 10/80). Each tablet contains the following inactive ingredients: As a consequence of extensive hepatic extraction of simvastatin (estimated to strength grapefruit juice (one can of frozen concentrate diluted with one
butylated hydroxyanisole NF, citric acid monohydrate USP, croscarmellose be >60% in man), the availability of drug to the general circulation is low. rather than 3 cans of water) three times daily for 2 days and an additional
sodium NF, hydroxypropyl methylcellulose USP, lactose monohydrate NF, Following an oral dose of 14C-labeled simvastatin in man, 13% of the dose 200 mL double-strength grapefruit juice together with, and 30 and 90 minutes
magnesium stearate NF, microcrystalline cellulose NF, and propyl gallate NF. was excreted in urine and 60% in feces. The latter represents absorbed drug following, a single dose of 60 mg simvastatin on the third day. This regimen of
equivalents excreted in bile, as well as any unabsorbed drug. grapefruit juice resulted in mean increases in the concentration (as measured
In a single-dose study in nine healthy subjects, it was estimated that less by the area under the concentration-time curve) of active and total HMG-CoA
CLINICAL PHARMACOLOGY than 5% of an oral dose of simvastatin reaches the general circulation as reductase inhibitory activity [measured using a radioenzyme inhibition assay
Background active inhibitors. both before (for active inhibitors) and after (for total inhibitors) base
Clinical studies have demonstrated that elevated levels of total cholesterol hydrolysis] of 2.4-fold and 3.6-fold, respectively, and of simvastatin and its
(total-C), low-density lipoprotein cholesterol (LDL-C) and apolipoprotein B Special Populations β-hydroxyacid metabolite [measured using a chemical assay — liquid
(Apo B), the major protein constituent of LDL, promote human Geriatric Patients chromatography/tandem mass spectrometry] of 16-fold and 7-fold, respectively.
atherosclerosis. In addition, decreased levels of high-density lipoprotein Ezetimibe In a second study, 16 subjects consumed one 8 oz glass of single-strength
cholesterol (HDL-C) are associated with the development of atherosclerosis. In a multiple-dose study with ezetimibe given 10 mg once daily for grapefruit juice (one can of frozen concentrate diluted with 3 cans of water)
Epidemiologic studies have established that cardiovascular morbidity and 10 days, plasma concentrations for total ezetimibe were about 2-fold higher with breakfast for 3 consecutive days and a single dose of 20 mg simvastatin
mortality vary directly with the level of total-C and LDL-C and inversely with in older (≥65 years) healthy subjects compared to younger subjects. in the evening of the third day. This regimen of grapefruit juice resulted in a
the level of HDL-C. Like LDL, cholesterol-enriched triglyceride-rich Simvastatin mean increase in the plasma concentration (as measured by the area under the
lipoproteins, including very-low-density lipoproteins (VLDL), intermediate- In a study including 16 elderly patients between 70 and 78 years of age concentration-time curve) of active and total HMG-CoA reductase inhibitory
density lipoproteins (IDL), and remnants, can also promote atherosclerosis. who received simvastatin 40 mg/day, the mean plasma level of HMG-CoA activity [using a validated enzyme inhibition assay different from that used in
The independent effect of raising HDL-C or lowering triglycerides (TG) on reductase inhibitory activity was increased approximately 45% compared the first1 study, both before (for active inhibitors) and after (for total inhibitors)
the risk of coronary and cardiovascular morbidity and mortality has not with 18 patients between 18-30 years of age. base hydrolysis] of 1.13-fold and 1.18-fold, respectively, and of simvastatin
been determined. and its β-hydroxyacid metabolite [measured using a chemical assay —
Pediatric Patients liquid chromatography/tandem mass spectrometry] of 1.88-fold and 1.31-fold,
Ezetimibe respectively. The effect of amounts of grapefruit juice between those used in
Mode of Action In a multiple-dose study with ezetimibe given 10 mg once daily for 7 days, these two studies on simvastatin pharmacokinetics has not been studied.
VYTORIN the absorption and metabolism of ezetimibe were similar in adolescents
Plasma cholesterol is derived from intestinal absorption and endogenous (10 to 18 years) and adults. Based on total ezetimibe, there are no
synthesis. VYTORIN contains ezetimibe and simvastatin, two lipid-lowering pharmacokinetic differences between adolescents and adults. Pharma- ANIMAL PHARMACOLOGY
compounds with complementary mechanisms of action. VYTORIN reduces cokinetic data in the pediatric population≥
VYTORINTM (ezetimibe/simvastatin) VYTORINTM (ezetimibe/simvastatin) VYTORINTM (ezetimibe/simvastatin)
A series of acute preclinical studies was performed to determine the Table 4
selectivity of ezetimibe for inhibiting cholesterol absorption. Ezetimibe Summary of NCEP ATP III Guidelines
inhibited the absorption of 14C-cholesterol with no effect on the absorption of LDL Level LDL level
triglycerides, fatty acids, bile acids, progesterone, ethyl estradiol, or the fat- at Which to at Which to
soluble vitamins A and D. Initiate Therapeutic Consider
In 4- to 12-week toxicity studies in mice, ezetimibe did not induce cyto- Table 3 LDL Goal Lifestyle Changesa Drug Therapy
chrome P450 drug metabolizing enzymes. In toxicity studies, a pharma- Response to VYTORIN and Atorvastatin in Patients with Risk Category (mg/dL) (mg/dL) (mg/dL)
cokinetic interaction of ezetimibe with HMG-CoA reductase inhibitors (parents Primary Hypercholesterolemia CHD or CHD
or their active hydroxy acid metabolites) was seen in rats, dogs, and rabbits. (Meana % Change from Untreated Baselineb) risk equivalentsb 20%)c (100-129: drug optional)d
Treatment N Total-C LDL -C Apo B HDL -C TGa Non-HDL -C
2+ Risk factorse 10-year risk 10-20%: ≥130c
CLINICAL STUDIES Week 6 (10-year risk ≤20%)cVYTORINTM (ezetimibe/simvastatin) VYTORINTM (ezetimibe/simvastatin) VYTORINTM (ezetimibe/simvastatin)
• The risk of myopathy/rhabdomyolysis is dose related for simvastatin. The Interactions with lipid-lowering drugs that can cause myopathy when Ezetimibe
incidence in clinical trials, in which patients were carefully monitored and given alone A 104-week dietary carcinogenicity study with ezetimibe was conducted in
some interacting drugs were excluded, has been approximately 0.02% at See WARNINGS, Myopathy/Rhabdomyolysis. rats at doses up to 1500 mg/kg/day (males) and 500 mg/kg/day (females)
20 mg, 0.07% at 40 mg and 0.3% at 80 mg. The risk of myopathy is increased by gemfibrozil and to a lesser extent by (~20 times the human exposure at 10 mg daily based on AUC0-24hr for total
Consequently: other fibrates and niacin (nicotinic acid) (≥1 g/day). ezetimibe). A 104-week dietary carcinogenicity study with ezetimibe was
Other drug interactions also conducted in mice at doses up to 500 mg/kg/day (>150 times the human
1. Use of VYTORIN concomitantly with itraconazole, ketoconazole, exposure at 10 mg daily based on AUC0-24hr for total ezetimibe). There were
erythromycin, clarithromycin, telithromycin, HIV protease inhibitors, Danazol: The risk of myopathy/rhabdomyolysis is increased by
concomitant administration of danazol particularly with higher doses of no statistically significant increases in tumor incidences in drug-treated rats
nefazodone, or large quantities of grapefruit juice (>1 quart daily) should be or mice.
avoided. If treatment with itraconazole, ketoconazole, erythromycin, VYTORIN (see CLINICAL PHARMACOLOGY, Pharmacokinetics ; WARNINGS,
Myopathy/Rhabdomyolysis). No evidence of mutagenicity was observed in vitro in a microbial
clarithromycin or telithromycin is unavoidable, therapy with VYTORIN should mutagenicity (Ames) test with Salmonella typhimurium and Escherichia coli
be suspended during the course of treatment. Concomitant use with other Amiodarone or Verapamil: The risk of myopathy/rhabdomyolysis is
increased by concomitant administration of amiodarone or verapamil with with or without metabolic activation. No evidence of clastogenicity was
medicines labeled as having a potent inhibitory effect on CYP3A4 at observed in vitro in a chromosomal aberration assay in human peripheral
therapeutic doses should be avoided unless the benefits of combined higher doses of VYTORIN (see WARNINGS, Myopathy/Rhabdomyolysis).
blood lymphocytes with or without metabolic activation. In addition, there
therapy outweigh the increased risk. Cholestyramine: Concomitant cholestyramine administration decreased
was no evidence of genotoxicity in the in vivo mouse micronucleus test.
the mean AUC of total ezetimibe approximately 55%. The incremental LDL-C
2. There is an increased risk of myopathy when simvastatin is used reduction due to adding VYTORIN to cholestyramine may be reduced by this In oral (gavage) fertility studies of ezetimibe conducted in rats, there was
concomitantly with gemfibrozil or other fibrates; the safety and effective- interaction. no evidence of reproductive toxicity at doses up to 1000 mg/kg/day in male
ness of ezetimibe administered with fibrates have not been established. or female rats (~7 times the human exposure at 10 mg daily based on
Cyclosporine: Caution should be exercised when initiating VYTORIN in
Therefore, the concomitant use of VYTORIN and fibrates should be patients treated with cyclosporine due to increased exposure to ezetimibe. AUC0-24hr for total ezetimibe).
avoided. (See PRECAUTIONS, Drug Interactions, Other Drug Interactions, This exposure may be greater in patients with severe renal insufficiency. In
Fibrates.) Simvastatin
patients treated with cyclosporine, the potential effects of the increased In a 72-week carcinogenicity study, mice were administered daily doses
3. Caution should be used when prescribing lipid-lowering doses (≥1 g/day) exposure to ezetimibe from concomitant use should be carefully weighed of simvastatin of 25, 100, and 400 mg/kg body weight, which resulted in
of niacin with VYTORIN, as niacin can cause myopathy when given alone. against the benefits of alterations in lipid levels provided by ezetimibe. In a mean plasma drug levels approximately 1, 4, and 8 times higher than the
The benefit of further alterations in lipid levels by the combined use of pharmacokinetic study in post-renal transplant patients with mildly impaired mean human plasma drug level, respectively (as total inhibitory activity
VYTORIN with niacin should be carefully weighed against the potential or normal renal function (creatinine clearance of >50 mL/min), concomitant based on AUC) after an 80-mg oral dose. Liver carcinomas were
risks of this drug combination. cyclosporine administration increased the mean AUC and Cmax of total significantly increased in high-dose females and mid- and high-dose males
ezetimibe 3.4-fold (range 2.3- to 7.9-fold) and 3.9-fold (range 3.0- to 4.4-fold), with a maximum incidence of 90% in males. The incidence of adenomas
4. The dose of VYTORIN should not exceed 10/10 mg daily in patients
respectively. In a separate study, the total ezetimibe exposure increased of the liver was significantly increased in mid- and high-dose females.
receiving concomitant medication with cyclosporine or danazol. The
12-fold in one renal transplant patient with severe renal insufficiency Drug treatment also significantly increased the incidence of lung adenomas
benefits of the use of VYTORIN in patients receiving cyclosporine or danazol
receiving multiple medications, including cyclosporine. (See CLINICAL in mid- and high-dose males and females. Adenomas of the Harderian gland
should be carefully weighed against the risks of these combinations. (See PHARMACOLOGY, Drug Interactions and WARNINGS, Myopathy/
PRECAUTIONS, Drug Interactions, Other Drug Interactions, Cyclosporine.) (a gland of the eye of rodents) were significantly higher in high-dose
Rhabdomyolysis.) mice than in controls. No evidence of a tumorigenic effect was observed at
5. The dose of VYTORIN should not exceed 10/20 mg daily in patients Digoxin: Concomitant administration of a single dose of digoxin in healthy 25 mg/kg/day.
receiving concomitant medication with amiodarone or verapamil. The male volunteers receiving simvastatin resulted in a slight elevation (less than
combined use of VYTORIN at doses higher than 10/20 mg daily with In a separate 92-week carcinogenicity study in mice at doses up to
0.3 ng/mL) in plasma digoxin concentrations compared to concomitant 25 mg/kg/day, no evidence of a tumorigenic effect was observed (mean
amiodarone or verapamil should be avoided unless the clinical benefit is administration of placebo and digoxin. Patients taking digoxin should be
likely to outweigh the increased risk of myopathy. plasma drug levels were 1 times higher than humans given 80 mg
monitored appropriately when VYTORIN is initiated. simvastatin as measured by AUC).
6. All patients starting therapy with VYTORIN, or whose dose of VYTORIN Fibrates: The safety and effectiveness of VYTORIN administered with In a two-year study in rats at 25 mg/kg/day, there was a statistically
is being increased, should be advised of the risk of myopathy and told to fibrates have not been established. significant increase in the incidence of thyroid follicular adenomas in female
report promptly any unexplained muscle pain, tenderness or weakness. Fibrates may increase cholesterol excretion into the bile, leading to rats exposed to approximately 11 times higher levels of simvastatin than in
VYTORIN therapy should be discontinued immediately if myopathy is cholelithiasis. In a preclinical study in dogs, ezetimibe increased cholesterol humans given 80 mg simvastatin (as measured by AUC).
diagnosed or suspected. The presence of these symptoms, and/or a in the gallbladder bile (see ANIMAL PHARMACOLOGY). Coadministration
A second two-year rat carcinogenicity study with doses of 50 and
CK level >10 times the ULN indicates myopathy. In most cases, when patients of VYTORIN with fibrates is not recommended until use in patients
100 mg/kg/day produced hepatocellular adenomas and carcinomas (in
were promptly discontinued from simvastatin treatment, muscle symptoms is studied. (See WARNINGS, Myopathy/Rhabdomyolysis.)
female rats at both doses and in males at 100 mg/kg/day). Thyroid follicular
and CK increases resolved. Periodic CK determinations may be considered Warfarin: Simvastatin 20-40 mg/day modestly potentiated the effect of cell adenomas were increased in males and females at both doses; thyroid
in patients starting therapy with VYTORIN or whose dose is being increased, coumarin anticoagulants: the prothrombin time, reported as International follicular cell carcinomas were increased in females at 100 mg/kg/day. The
but there is no assurance that such monitoring will prevent myopathy. Normalized Ratio (INR), increased from a baseline of 1.7 to 1.8 and from increased incidence of thyroid neoplasms appears to be consistent with
7. Many of the patients who have developed rhabdomyolysis on therapy with 2.6 to 3.4 in a normal volunteer study and in a hypercholesterolemic patient findings from other HMG-CoA reductase inhibitors. These treatment levels
simvastatin have had complicated medical histories, including renal study, respectively. With other statins, clinically evident bleeding and/or represented plasma drug levels (AUC) of approximately 7 and 15 times
insufficiency usually as a consequence of long-standing diabetes mellitus. increased prothrombin time has been reported in a few patients taking (males) and 22 and 25 times (females) the mean human plasma drug
Such patients taking VYTORIN merit closer monitoring. Therapy with coumarin anticoagulants concomitantly. In such patients, prothrombin time
exposure after an 80 milligram daily dose.
VYTORIN should be temporarily stopped a few days prior to elective major should be determined before starting VYTORIN and frequently enough
during early therapy to insure that no significant alteration of prothrombin No evidence of mutagenicity was observed in a microbial mutagenicity
surgery and when any major medical or surgical condition supervenes. (Ames) test with or without rat or mouse liver metabolic activation. In
time occurs. Once a stable prothrombin time has been documented,
Liver Enzymes prothrombin times can be monitored at the intervals usually recommended addition, no evidence of damage to genetic material was noted in an in vitro
In three placebo-controlled, 12-week trials, the incidence of consecutive for patients on coumarin anticoagulants. If the dose of VYTORIN is alkaline elution assay using rat hepatocytes, a V-79 mammalian cell forward
elevations (≥3 X ULN) in serum transaminases was 1.7% overall for patients changed or discontinued, the same procedure should be repeated. mutation study, an in vitro chromosome aberration study in CHO cells, or an
treated with VYTORIN and appeared to be dose-related with an incidence Simvastatin therapy has not been associated with bleeding or with changes in vivo chromosomal aberration assay in mouse bone marrow.
of 2.6% for patients treated with VYTORIN 10/80. In controlled long-term in prothrombin time in patients not taking anticoagulants. There was decreased fertility in male rats treated with simvastatin for
(48-week) extensions, which included both newly-treated and previously- 34 weeks at 25 mg/kg body weight (4 times the maximum human exposure
treated patients, the incidence of consecutive elevations (≥3 X ULN) in Ezetimibe level, based on AUC, in patients receiving 80 mg/day); however, this effect
serum transaminases was 1.8% overall and 3.6% for patients treated with Fenofibrate: In a pharmacokinetic study, concomitant fenofibrate was not observed during a subsequent fertility study in which simvastatin
VYTORIN 10/80. These elevations in transaminases were generally administration increased total ezetimibe concentrations approximately was administered at this same dose level to male rats for 11 weeks (the
asymptomatic, not associated with cholestasis, and returned to baseline 1.5-fold. entire cycle of spermatogenesis including epididymal maturation). No
after discontinuation of therapy or with continued treatment. Gemfibrozil: In a pharmacokinetic study, concomitant gemfibrozil microscopic changes were observed in the testes of rats from either study.
It is recommended that liver function tests be performed before the administration increased total ezetimibe concentrations approximately At 180 mg/kg/day, (which produces exposure levels 22 times higher than
initiation of treatment with VYTORIN, and thereafter when clinically 1.7-fold. those in humans taking 80 mg/day based on surface area, mg/m2),
indicated. Patients titrated to the 10/80-mg dose should receive an additional Simvastatin seminiferous tubule degeneration (necrosis and loss of spermatogenic
test prior to titration, 3 months after titration to the 10/80-mg dose, and Propranolol: In healthy male volunteers there was a significant decrease epithelium) was observed. In dogs, there was drug-related testicular
periodically thereafter (e.g., semiannually) for the first year of treatment. in mean Cmax, but no change in AUC, for simvastatin total and active atrophy, decreased spermatogenesis, spermatocytic degeneration and giant
Patients who develop increased transaminase levels should be monitored inhibitors with concomitant administration of single doses of simvastatin and cell formation at 10 mg/kg/day, (approximately 2 times the human exposure,
with a second liver function evaluation to confirm the finding and be followed propranolol. The clinical relevance of this finding is unclear. The based on AUC, at 80 mg/day). The clinical significance of these findings
thereafter with frequent liver function tests until the abnormality(ies) return pharmacokinetics of the enantiomers of propranolol were not affected. is unclear.
to normal. Should an increase in AST or ALT of 3 X ULN or greater persist, CNS Toxicity Pregnancy
withdrawal of therapy with VYTORIN is recommended. Optic nerve degeneration was seen in clinically normal dogs treated with Pregnancy Category: X
VYTORIN should be used with caution in patients who consume simvastatin for 14 weeks at 180 mg/kg/day, a dose that produced mean See CONTRAINDICATIONS.
substantial quantities of alcohol and/or have a past history of liver disease. plasma drug levels about 12 times higher than the mean plasma drug level in VYTORIN
Active liver diseases or unexplained persistent transaminase elevations are humans taking 80 mg/day. As safety in pregnant women has not been established, treatment should
contraindications to the use of VYTORIN. A chemically similar drug in this class also produced optic nerve be immediately discontinued as soon as pregnancy is recognized. VYTORIN
degeneration (Wallerian degeneration of retinogeniculate fibers) in clinically should be administered to women of child-bearing potential only when such
PRECAUTIONS patients are highly unlikely to conceive and have been informed of the
normal dogs in a dose-dependent fashion starting at 60 mg/kg/day, a dose
Information for Patients that produced mean plasma drug levels about 30 times higher than the mean potential hazards.
Patients should be advised about substances they should not take plasma drug level in humans taking the highest recommended dose (as
concomitantly with VYTORIN and be advised to report promptly
Ezetimibe
measured by total enzyme inhibitory activity). This same drug also produced In oral (gavage) embryo-fetal development studies of ezetimibe conducted
unexplained muscle pain, tenderness, or weakness (see list below and vestibulocochlear Wallerian-like degeneration and retinal ganglion cell in rats and rabbits during organogenesis, there was no evidence of
WARNINGS, Myopathy/Rhabdomyolysis). Patients should also be advised chromatolysis in dogs treated for 14 weeks at 180 mg/kg/day, a dose that embryolethal effects at the doses tested (250, 500, 1000 mg/kg/day). In rats,
to inform other physicians prescribing a new medication that they are resulted in a mean plasma drug level similar to that seen with the increased incidences of common fetal skeletal findings (extra pair of
taking VYTORIN. 60 mg/kg/day dose. thoracic ribs, unossified cervical vertebral centra, shortened ribs) were
Hepatic Insufficiency CNS vascular lesions, characterized by perivascular hemorrhage and observed at 1000 mg/kg/day (~10 times the human exposure at 10 mg daily
Due to the unknown effects of the increased exposure to ezetimibe in edema, mononuclear cell infiltration of perivascular spaces, perivascular based on AUC0-24hr for total ezetimibe). In rabbits treated with ezetimibe, an
patients with moderate or severe hepatic insufficiency, VYTORIN is not fibrin deposits and necrosis of small vessels were seen in dogs treated with increased incidence of extra thoracic ribs was observed at 1000 mg/kg/day
recommended in these patients. (See CLINICAL PHARMACOLOGY, simvastatin at a dose of 360 mg/kg/day, a dose that produced mean plasma (150 times the human exposure at 10 mg daily based on AUC0-24hr for total
Pharmacokinetics, Special Populations.) drug levels that were about 14 times higher than the mean plasma drug ezetimibe). Ezetimibe crossed the placenta when pregnant rats and rabbits
Drug Interactions (See also CLINICAL PHARMACOLOGY, Drug levels in humans taking 80 mg/day. Similar CNS vascular lesions have been were given multiple oral doses.
Interactions) observed with several other drugs of this class. Multiple-dose studies of ezetimibe coadministered with HMG-CoA
VYTORIN There were cataracts in female rats after two years of treatment with reductase inhibitors (statins) in rats and rabbits during organogenesis result
CYP3A4 Interactions 50 and 100 mg/kg/day (22 and 25 times the human AUC at 80 mg/day, in higher ezetimibe and statin exposures. Reproductive findings occur at
Potent inhibitors of CYP3A4 (below) increase the risk of myopathy by respectively) and in dogs after three months at 90 mg/kg/day (19 times) and lower doses in coadministration therapy compared to monotherapy.
reducing the elimination of the simvastatin component of VYTORIN. at two years at 50 mg/kg/day (5 times).
Simvastatin
See WARNINGS, Myopathy/Rhabdomyolysis, and CLINICAL PHARMA- Carcinogenesis, Mutagenesis, Impairment of Fertility Simvastatin was not teratogenic in rats at doses of 25 mg/kg/day or
COLOGY, Pharmacokinetics, Drug Interactions. VYTORIN in rabbits at doses up to 10 mg/kg daily. These doses resulted in 3 times
Itraconazole No animal carcinogenicity or fertility studies have been conducted with ≥
(rat) or 3 times (rabbit) the human exposure based on mg/m2 surface
Ketoconazole the combination of ezetimibe and simvastatin. The combination of ezetimibe area. However, in studies with another structurally-related HMG-CoA
Erythromycin with simvastatin did not show evidence of mutagenicity in vitro in a microbial reductase inhibitor, skeletal malformations were observed in rats
Clarithromycin mutagenicity (Ames) test with Salmonella typhimurium and Escherichia coli and mice.
with or without metabolic activation. No evidence of clastogenicity was
Telithromycin Rare reports of congenital anomalies have been received following
observed in vitro in a chromosomal aberration assay in human peripheral
HIV protease inhibitors intrauterine exposure to HMG-CoA reductase inhibitors. In a review 2 of
blood lymphocytes with ezetimibe and simvastatin with or without metabolic
Nefazodone activation. There was no evidence of genotoxicity at doses up to 600 mg/kg
Cyclosporine with the combination of ezetimibe and simvastatin (1:1) in the in vivo mouse
2 Manson, J.M., Freyssinges, C., Ducrocq, M.B., Stephenson, W.P., Postmarketing
Surveillance of Lovastatin and Simvastatin Exposure During Pregnancy,
Large quantities of grapefruit juice (>1 quart daily) micronucleus test. Reproductive Toxicology, 10(6):439-446, 1996.You can also read