Cura del diabete: non solo glicemia - Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale - Briefing Studio
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cura del diabete: non solo glicemia
Giuseppe Penno
Dipartimento di Medicina Clinica e Sperimentale
Azienda Ospedaliera Universitaria di Pisa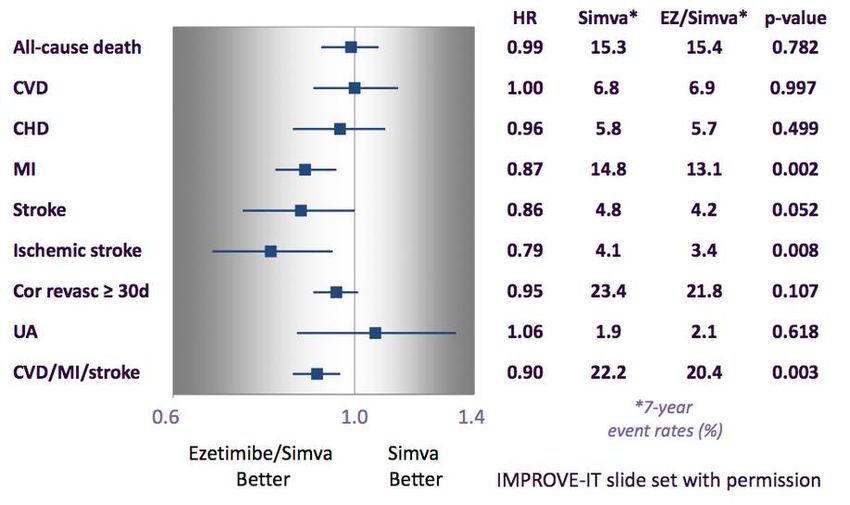
1. I numeri che contano
Type 2 diabetes is increasingly prevalent
Globally, 387 million people At least 68% of people >65 years
are living with diabetes1 with diabetes die of heart
disease2
Mortality risk associated
with diabetes (n=820,900)3
3
Hazard ratio (95% CI) (diabetes
vs no diabetes)
2
1
This will rise to 0
CV death All-cause
592 million by
mortality
20351
1. IDF Diabetes Atlas 6th Edition 2014 http://www.idf.org/diabetesatlas; 2. Centers for
Disease Control and Prevention 2011; 3. Seshasai et al. N Engl J Med 2011;364:829-41
Diabetes and cause-specific mortality
Evidence from 54,855 deaths in 690,700 adults between ages 35-89 in 44 studies
from the Prospective Studies Collaboration (13 million person-years of follow-up)
3 2,75
2,37 2,47
2,5
2 1,9 1,75
1,57
HR
1,5 1,13
1
0,5
0
Mortality
Gnatiuc L et al., EASD 2015
Diabetes is associated with significant
loss of life years
Men Women
7 7
Non-vascular
6 deaths 6
Vascular
5 5
Years of life lost
deaths
4 4
3 3
2 2
1 1
0 0
0 40 50 60 70 80 90 0 40 50 60 70 80 90
Age (years) Age (years)
On average, a 50-year-old individual with diabetes and no history of vascular
disease
.
will die 6 years earlier compared to someone without diabetes
Seshasai et al. N Engl J
Med 2011;364:829-41
1. I numeri che contano 2. Trattamento intensivo della glicemia
Questions addressed in RCT of Type 2
diabetes treatment
Question 1: Question 2:
Does treatment directed Does it matter which diabetes
lowering of HbA1c (below 6.0 to treatment is used to lower
6.5%) reduce endpoints HbA1c?
UKPDS P UKPDS P PROactive S
Long-term follow-up
RECORD P, S
ACCORD P, S Look AHEAD P, S ORIGIN P, S
ADVANCE P, S SAVOR-TIMI 53 P, S EXAMINE S
VADT P, S
TECOS S ELIXA S
ORIGIN P, S
EMPA-REG S
P, primary prevention; S, secondary prevention

First coprimary outcome: death from CV causes, nonfatal MI, nonfatal stroke; second Higher in Standard Therapy Higher in Intensive Therapy coprimary outcome: + revascularization, hospitalization for HF The ORIGIN Trial Investigators, N Engl J Med 367: 319-328, 2012
1. Numeri che contano 2. Trattamento intensivo della glicemia 3. Non solo glicemia: quale trattamento (parte 1)
Questions addressed in RCT of Type 2
diabetes treatment
Question 1: Question 2:
Does treatment directed Does it matter which diabetes
lowering of HbA1c (below 6.0 to treatment is used to lower
6.5%) reduce endpoints HbA1c?
UKPDS P UKPDS P PROactive S
Long-term follow-up
RECORD P, S
ACCORD P, S Look AHEAD P, S ORIGIN P, S
ADVANCE P, S SAVOR-TIMI 53 P, S EXAMINE S
VADT P, S
TECOS S ELIXA S
ORIGIN P, S
EMPA-REG S
P, primary prevention; S, secondary preventionPioglitazone and Risk of Cardiovascular Events in
Patients with Type 2 Diabetes Mellitus
A Meta-Analysis of Randomized Trials
19 trials enrolling 16,390 patients (1 year, 10 trials)
Control
Death, MI, stroke
-18%
Pioglitazone
Lincoff AM et al, JAMA 298: 1180-1188, 2007∆% HbA1c 0.22% The Look AHEAD Research Group, N Engl J Med 369: 145-154, 2013
Follow-up-time for each patient was at least 12 months
1. Numeri che contano 2. Trattamento intensivo della glicemia 3. Non solo glicemia: quale trattamento (parte 1) 4. Non solo glicemia: quale trattamento (parte 2)
Questions addressed in RCT of Type 2
diabetes treatment
Question 1: Question 2:
Does treatment directed Does it matter which diabetes
lowering of HbA1c (below 6.0 to treatment is used to lower
6.5%) reduce endpoints HbA1c?
UKPDS P UKPDS P PROactive S
Long-term follow-up
RECORD P, S
ACCORD P, S Look AHEAD P, S ORIGIN P, S
ADVANCE P, S SAVOR-TIMI 53 P, S EXAMINE S
VADT P, S
TECOS S ELIXA S
ORIGIN P, S
EMPA-REG S
P, primary prevention; S, secondary prevention∆% HbA1c 0.30% Scirica BM, et al., The SAVOR-TIMI 53 Investigators, N Engl J Med 369: 1317-1326, 2013
∆% HbA1c 0.36% White WB, et al., The EXAMINE Investigators, N Engl J Med 369: 1327-1335, 2013
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352
Primary Composite Cardiovascular
Outcome
CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina
PP Analysis for Non-inferiority
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352Primary Composite Cardiovascular
Outcome
Numbers of patients with events Sitagliptin Placebo
n=7332 n=7339
Primary composite CV Outcome 839 (11.4%) 851 (11.6%)
4.06 per 100 pyrs 4.17 per 100 pyrs
ITT HR=0.98 (0.89, 1.08), p=0.65
Individual components
• CV death 311 (4.2%) 291 (4.0%)
• Nonfatal MI 275 (3.8%) 286 (3.9%)
• Nonfatal stroke 145 (2.0%) 157 (2.1%)
• Hospitalization for unstable angina 108 (1.5%) 117 (1.6%)
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352All cause mortality
Sitagliptin n=7332 Placebo n=7339
All-cause mortality 547 (7.5%) 537 (7.3%)
2.48 per 100 pyrs 2.45 per 100 pyrs
ITT HR=1.01 (0.90, 1.14), p=0.88
Non-cardiovascular 167 (2.3%) 171 (2.3%)
Unknown* 109 (1.5%) 107 (1.5%)
Cardiovascular
• Sudden cardiac death 72 (1.0%) 73 (1.0%)
• Acute myocardial infarction 21 (0.3%) 27(0.4%)
• Heart failure 28 (0.4%) 35 (0.5%)
• Stroke 29 (0.4%) 36 (0.5%)
• Other cardiovascular 8 (0.1%) 5 (0.1%)
• Presumed cardiovascular 113 (1.5%) 83 (1.1%)
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352Hospitalization for heart failure * Adjusted for history of heart failure at baseline Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352
Hospitalization for heart failure
Numbers of patients with events Sitagliptin Placebo
n=7332 n=7339
Hospitalization for heart failure† 228 (3.1%) 229 (3.1%)
1.07 per 100 pyrs 1.09 per 100 pyrs
ITT HR=1.00 (0.83, 1.20), p=0.98
Hospitalization for heart failure or 538 (7.3%) 525 (7.2%)
cardiovascular death†
2.54 per 100 pyrs 2.50 per 100 pyrs
ITT HR=1.02, (0.90, 1.15), p=0.74
* Adjusted for history of heart failure at baseline
† Prespecified analyses
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352Primary Composite Cardiovascular
Outcome
CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352Recent trials of newer glucose-lowering agents
have been neutral on the primary CV outcome
HR: 1.0 SAVOR-TIMI HR: 0.98
(95% CI: 0.89, 1.12) (95% CI: 0.88, 1.09) TECOS
53
HR: 0.96
(95% CI: UL ≤1.16) EXAMINE
2013 2014 2015
HR: 1.02
(95% CI: 0.89, 1.17)
ELIXA
DPP-4
inhibitors*
Lixisenatide EMPA-REG
OUTCOMEÄ
Empagliflozin
CV, cardiovascular; HR, hazard ratio; DPP-4, dipeptidyl peptidase-4
*Saxagliptin, alogliptin, sitagliptin
Adapted from Johansen OE. World J Diabetes 2015;6:1092-96Number needed to treat (NNT) to prevent one death
across landmark trials in patients with high CV risk
Simvastatin1 Ramipril2 Empagliflozin
for 5.4 years for 5 years for 3 years
High CV risk High CV risk
T2DM with high CV risk
5% diabetes, 26% 38% diabetes, 46%
92% hypertension
hypertension hypertension
Pre-ACEi/ARB era >80% ACEi/ARB
Pre-statin era 75% statin
1994 2000 2015
1. 4S investigator. Lancet 1994; 344: 1383-89, http://www.trialresultscenter.org/study2590-
4S.htm;
2. HOPE investigator N Engl J Med 2000;342:145-53,
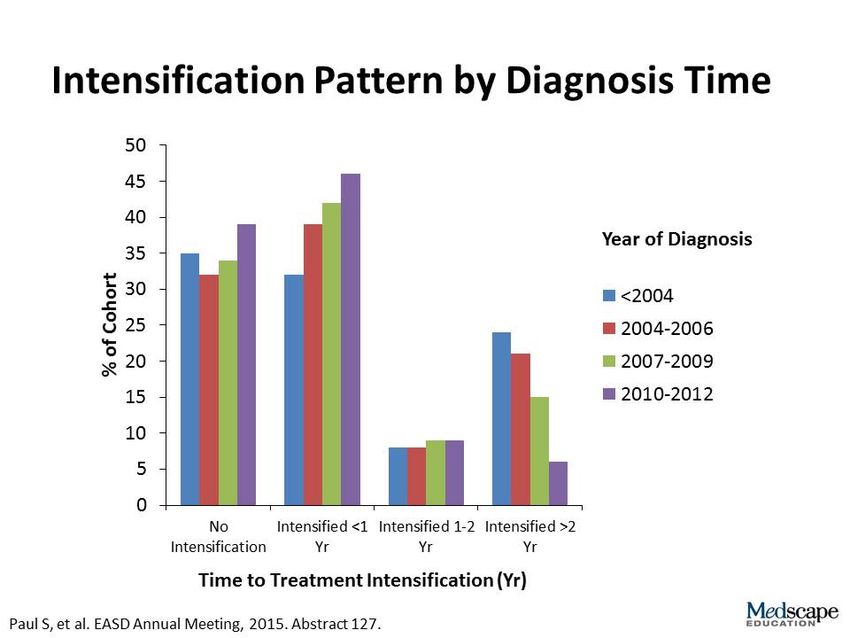
http://www.trialresultscenter.org/study2606-HOPE.htm1. Numeri che contano 2. Trattamento intensivo della glicemia 3. Non solo glicemia: quale trattamento (parte 1) 4. Non solo glicemia: quale trattamento (parte 2) 5. Tornando alla glicemia: l’inerzia terapeutica
TECOS CV Safety Trial:
Time-to-Initiation of Additional AHA Therapy
Sitagliptin Placebo
Intention-to-Treat Population N=7,332 N=7,339 HR (95% CI) P-value
Initiation of next antihyperglycemic medication, 1,591 (21.7); 2,046 (27.9);
0.72 (0.68, 0.77)TECOS CV Safety Trial:
Time-to-Initiation of Insulin Therapy
Sitagliptin Placebo
Intention-to-Treat Populationa N=5,608 N=5,655 HR (95% CI) P-value
Initiation of insulin , 542 (9.7) 744 (13.2);
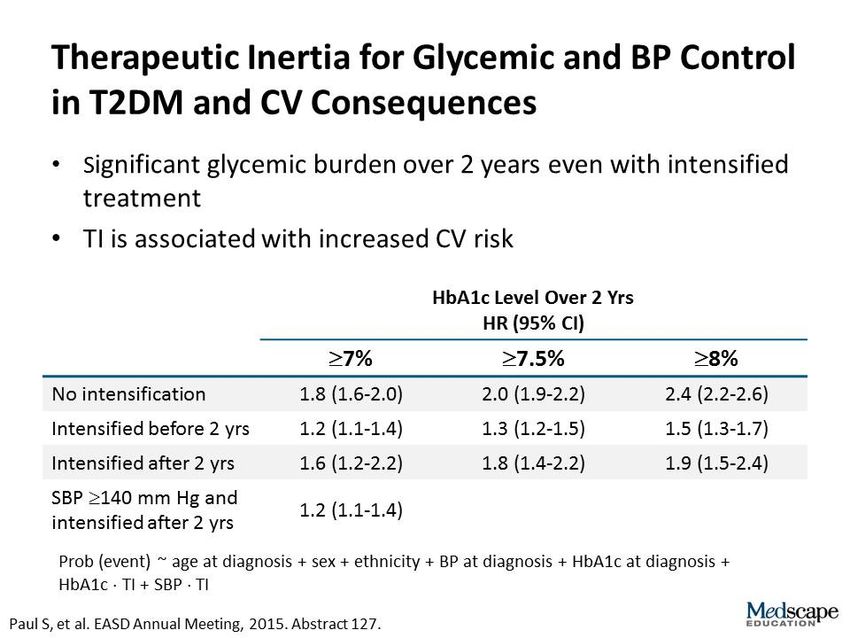
0.70 (0.63, 0.79)1. Numeri che contano 2. Trattamento intensivo della glicemia 3. Non solo glicemia: quale trattamento (parte 1) 4. Non solo glicemia: quale trattamento (parte 2) 5. Tornando alla glicemia: l’inerzia terapeutica 6. Veramente oltre la glicemia
Global, regional, and national comparative risk assessment of 79 behavioural,
environmental and occupational, and metabolic risks or clusters of risks in 188 countries,
1990-2013: a systematic analysis for the Global Burden of Disease study 2013
GBD 2013 Risk Factors Collaborators. Lancet, september 11, 2015Global, regional, and national comparative risk assessment of 79 behavioural,
environmental and occupational, and metabolic risks or clusters of risks in 188 countries,
1990-2013: a systematic analysis for the Global Burden of Disease study 2013
Ten leading risk factors in terms of attributable DALYs in 2013 for both sexes combined
1 2 3 4 5 6 7 8 9 10
Childhood Household
Blood Fasting Alcohol Unsafe Unsafe
Global Smoking BMI under- air Fruit
pressure nutrition glucose use water sex
pollution
GBD 2013 Risk Factors Collaborators. Lancet, september 11, 2015Global, regional, and national comparative risk assessment of 79 behavioural,
environmental and occupational, and metabolic risks or clusters of risks in 188 countries,
1990-2013: a systematic analysis for the Global Burden of Disease study 2013
Ten leading risk factors in terms of attributable DALYs in 2013 for both sexes combined
1 2 3 4 5 6 7 8 9 10
Childhood Household
Blood Fasting Alcohol Unsafe Unsafe
Global Smoking BMI under- air Fruit
pressure nutrition glucose use water sex
pollution
Blood Alcohol Fasting Total Physical
Developed BMI Smoking GFR Sodium Fruit
pressure use glucose chol. activity
GBD 2013 Risk Factors Collaborators. Lancet, september 11, 2015Global, regional, and national comparative risk assessment of 79 behavioural,
environmental and occupational, and metabolic risks or clusters of risks in 188 countries,
1990-2013: a systematic analysis for the Global Burden of Disease study 2013
Ten leading risk factors in terms of attributable DALYs in 2013 for both sexes combined
1 2 3 4 5 6 7 8 9 10
Childhood Household
Blood Fasting Alcohol Unsafe Unsafe
Global Smoking BMI under- air Fruit
pressure nutrition glucose use water sex
pollution
Blood Alcohol Fasting Total Physical
Developed BMI Smoking GFR Sodium Fruit
pressure use glucose chol. activity
Western Blood Fasting Alcohol Total Physical
Smoking BMI GFR Sodium Fruit
Europe pressure glucose use chol. activity
GBD 2013 Risk Factors Collaborators. Lancet, september 11, 2015Global, regional, and national comparative risk assessment of 79 behavioural,
environmental and occupational, and metabolic risks or clusters of risks in 188 countries,
1990-2013: a systematic analysis for the Global Burden of Disease study 2013
Ten leading risk factors in terms of attributable DALYs in 2013 for both sexes combined
1 2 3 4 5 6 7 8 9 10
Childhood Household
Blood Fasting Alcohol Unsafe Unsafe
Global Smoking BMI under- air Fruit
pressure nutrition glucose use water sex
pollution
Blood Alcohol Fasting Total Physical
Developed BMI Smoking GFR Sodium Fruit
pressure use glucose chol. activity
Western Blood Fasting Alcohol Total Physical
Smoking BMI GFR Sodium Fruit
Europe pressure glucose use chol. activity
Bone
Blood Fasting Total Alcohol Physical
Italy BMI Smoking GFR Sodium mineral
pressure glucose chol. use activity
density
GBD 2013 Risk Factors Collaborators. Lancet, september 11, 2015Ferguson LD and Sattar N. Diabetes, Obesity and Metabolism 15: 387-391, 2013
Ferguson LD and Sattar N. Diabetes, Obesity and Metabolism 15: 387-391, 2013
Efficacy of cholesterol-lowering therapy in 18.686
people with diabetes in 14 randomised trials of statins: a
meta-analysis.
Proportional effects on major vascular events per mmol/L
reduction in LDL cholesterol (39 mg/dl)
-22%
-21%
-21%
CTT Collaborators, Lancet 371: 117-125, 2008Efficacy of cholesterol-lowering therapy in 18.686
people with diabetes in 14 randomised trials of statins: a
meta-analysis.
Proportional effects on
major vascular events
per mmol/L
reduction in LDL
cholesterol (39 mg/dl)
by baseline lipid
profile
-21%
CTT Collaborators, Lancet 371: 117-125, 2008IMPROVE-IT A large scale (18,144 participants), multi-center RCT of high risk post Acute Coronary Syndrome (ACS) patients
IMPROVE-IT Individual Cardiovascular Endpoints and CVD/MI/Stroke
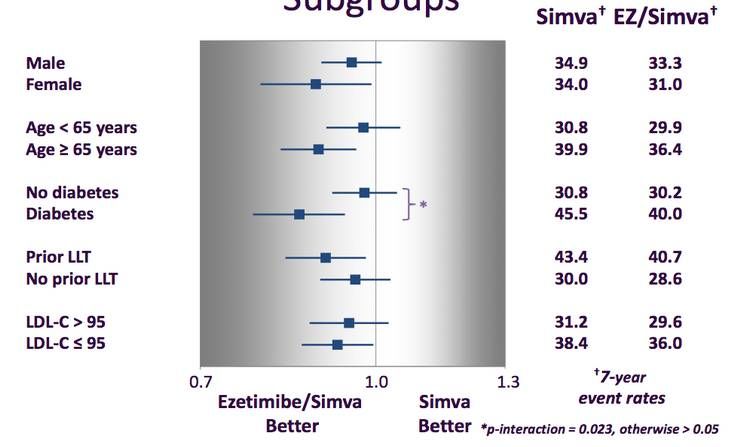
IMPROVE-IT Major Pre-specified Subgroups
1. Numeri che contano 2. Trattamento intensivo della glicemia 3. Non solo glicemia: quale trattamento (parte 1) 4. Non solo glicemia: quale trattamento (parte 2) 5. Tornando alla glicemia: l’inerzia terapeutica 6. Veramente oltre la glicemia 7. Conclusioni
Grazie per l’attenzione!
You can also read

















































