Effectiveness of RADAR: An Innovative Model to Organize Diabetes Care in First Nations Communities
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FEATURE ARTICLE
Effectiveness of RADAR: An Innovative Model to
Organize Diabetes Care in First Nations Communities
Dean T. Eurich,1,2 Lisa A. Wozniak,1,2 Allison Soprovich,1,2 Jasjeet K. Minhas-Sandhu,1,2 Lynden Crowshoe,3
Jeffrey A. Johnson,1,2 and Salim Samanani4
Challenges exist for the management of diabetes care in FN people has led to suboptimal and fragmented care
First Nations populations. RADAR (Reorganizing the Ap- for people living both on and off reserves. Indeed, we
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
proach to Diabetes through the Application of Registries) previously found that such diabetes care was reactive,
is a culturally appropriate, innovative care model that in- relying on FN people to navigate a complicated health
corporates a disease registry and electronic health re- care system (8).
cord for local care provision with remote coordination,
tailored for First Nations people. This study assessed Within a chronic care model, one framework for organiz-
the effectiveness of RADAR on patient outcomes and dia- ing and delivering optimal diabetes care is called the 5Rs,
betes care organization in participating communities in which stands for Recognize (performing screening/risk
Alberta, Canada. It revealed significant improvements in factor assessment), Register (systematically tracking pa-
outcomes after 2 years, with 91% of patients achieving a tients), Relay (facilitating information-sharing), Recall
primary combined end point of a 10% improvement in or (providing timely review and reassessment), and Resource
persistence at target for A1C, systolic blood pressure, (supporting self-management) (7). Furthermore, FN-
and/or LDL cholesterol. Qualitative assessment showed specific clinical practice guidelines (CPGs) recommend
that diabetes care organization also improved. These mul- that diabetes prevention, care, and education be grounded
timethod findings support tailored diabetes care practices in communities’ social, cultural, and health service con-
in First Nations populations. texts (6). The organization of diabetes care (7) and the
principles of self-determination and governance of FN
In Canada, chronic diseases have reached critical imbal- communities (9) guided the development of RADAR
ances for First Nations (FN) people (1). Diabetes is (Reorganizing the Approach to Diabetes through the Appli-
three to five times more common in FN than in non-FN cation of Registries) (10), in partnership with FN commu-
populations (2,3). Higher rates of diabetes-related com- nities and OKAKI Health Intelligence, Inc., a private, social
plications are observed in FN populations (4,5). The enterprise in Alberta, Canada, with >12 years working
high burden of disease, complications, and comorbidity with FN communities.
that FN people with diabetes experience is compounded
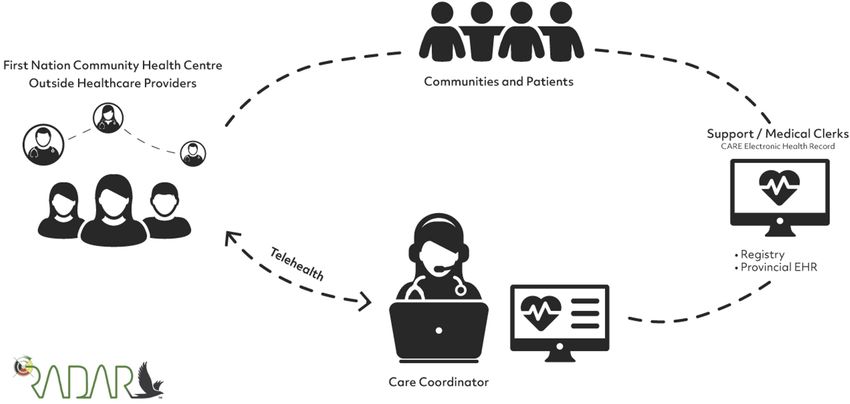
The RADAR model (10) uses remote care coordinators
by the significant and historical social, physical, and
(CCs), who are registered nurses or dietitians, to sup-
economic challenges they face (5,6).
port local health care providers (HCPs) (e.g., registered
Primary care for people with diabetes is typically deliv- nurses, licensed practical nurses, and dietitians) in FN
ered using a chronic care model (7), although its imple- communities through telehealth to 1) populate an elec-
mentation within FN communities is challenging. FN tronic medical record (EMR) diabetes registry called the
communities are often remote, with limited access to CARE platform, which was developed specifically for FN
comprehensive diabetes care. Current federal and pro- communities; 2) coordinate population-level care to
vincial approaches to managing diabetes care among identify priorities and gaps in care; and 3) apply current
1
School of Public Health, University of Alberta, Edmonton, Alberta, Canada; 2Alliance for Canadian Health Outcomes Research in Diabetes,
University of Alberta, Edmonton, Alberta, Canada; 3Cumming School of Medicine AND Indigenous, Local, and Global Health Office, University of
Calgary, Calgary, Alberta, Canada; 4OKAKI Health Intelligence, Inc., Calgary, Alberta, Canada
Corresponding author: Dean T. Eurich, deurich@ualberta.ca
This article contains supplementary material online at https://doi.org/10.2337/figshare.21872040.
https://doi.org/10.2337/cd22-0090
©2023 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational
and not for profit, and the work is not altered. More information is available at https://www.diabetesjournals.org/journals/pages/license.
1FEATURE ARTICLE Effectiveness of an Organized Diabetes Care Model
CPGs (11) through regular client review and case con- Possession) principles were followed (13,14). Findings
ferencing to consider therapeutic changes and coordi- were shared with FN health leadership to incorporate
nate referrals (Figure 1). their feedback. RADAR was approved by the University
of Alberta’s Health Research Ethics Board (Study ID
RADAR was implemented collaboratively with FN com-
Pro00048714).
munities from Treaty 6, 7, and 8 territories in Alberta,
Canada, where local HCPs found the model appropri-
Data Collection and Analysis
ate, acceptable, and valuable for both HCPs and pa-
tients (12). Here, we describe the effectiveness of The primary outcome was a 10% improvement in A1C,
RADAR with regard to patient outcomes and the organi- systolic blood pressure (SBP), or LDL cholesterol during
zation of diabetes care in these communities. the 2-year follow-up relative to baseline control periods,
representing a clinically important difference (15). For
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
Design and Methods patients who were already at target at baseline, we con-
sidered persistence at target (i.e., maintaining values
Design within 10% of baseline) as achieving the primary out-
We used a modified stepped-wedge design supple- come (10). Outcomes were measured continuously
mented with a descriptive qualitative assessment to throughout the follow-up period and at the time of each
evaluate RADAR’s effectiveness (10). Eligible patients community transition (i.e., step) as per traditional
were $18 years of age, diagnosed with type 2 diabetes, stepped-wedge designs.
and actively engaged in and received care from the
The primary outcome was first analyzed using an
FN health facility on a reserve and had provided verbal
intention-to-treat (ITT) framework, which included all
consent for HCPs to manage their diabetes (10). For
patients identified by the communities in their baseline
the qualitative assessment, we purposefully sampled re-
assessments, irrespective of the follow-up care they
mote care coordinators and local HCPs who were imple-
received. Additionally, we used a per-protocol (PP)
menting RADAR.
framework, removing patients who died, moved, or
The decision to participate in RADAR was made by FN subsequently refused care at FN community health cen-
leaders (e.g., chiefs and council, chief executive officers, ters. We fit a generalized linear mixed model with ran-
and/or community health directors) in each participat- dom effect for cluster (i.e., community) and fixed effect
ing community, who reviewed and endorsed the for each step (i.e., transitions from baseline to follow-
project. OCAP (Ownership, Control, Access, and up intervention) (16). We also included calendar year
FIGURE 1 RADAR Infographic.
2 D IA B E TE SJ OUR N A L S.OR G/ C L IN IC A LEURICH ET AL.
in our models as a fixed effect to control for any tempo-
TABLE 1 Clustered Baseline Demographics of RADAR
ral confounding effects, although calendar year was not
Participants (n = 516)
significant in the models (P >0.10). Patients with insuf-
ficient primary outcome data were assumed to be non- Characteristic Value
responders (i.e., individuals who had failed to achieve Age, years 60 ± 13.6
the primary end point). In addition, the mean change in
Female sex 292 (57)
A1C, SBP, and LDL was assessed for patients with A1C
$7.5% (58 mmol/mol), SBP $140 mmHg and LDL cho- Smoker 119 (23.1)
lesterol $$2.5 mmol/L (i.e., at-risk patients), after ac-
A1C, % 8.3 ± 2.0
counting for the baseline value, year, and community
clustering in alignment with Diabetes Canada CPGs Cholesterol, mmol/L
(10,11). Outcome data are not reported by community to LDL cholesterol 2.0 ± 0.9
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
HDL cholesterol 1.1 ± 0.4
maintain confidentiality as per our data-sharing agree- Triglycerides 2.5 ± 2.7
ments; however, the consistency of effects across the com- Total cholesterol-to-HDL cholesterol ratio 3.9 ± 1.8
munities was assessed and is expressed as ranges.
Estimated glomerular filtration rate, mL/min/1.73 m2*
Quantitative analyses were performed using Stata, v. 15–30 15 ± 3.1
14.2, statistical software (StataCorp, College Station, TX). 30–45 31 ± 6.5
45–60 44 ± 9.2
We used a descriptive qualitative approach (17) to as- 60–90 143 ± 29.9
sess the effectiveness of RADAR on the organization of >90 246 ± 51.4
diabetes care within participating communities, which Data are mean ± SD or n (%). *n = 479.
were diverse by treaty, geography, population, and
proximity to urban centers. Data sources included indi- was 91% (95% CI 89–94%) in the ITT population (n =
vidual interviews with remote CCs and local HCPs. 516), and 93% (95% CI 91–95%) in the PP population
Qualitative data were managed using ATLAS.ti, v. 8, (n = 419) (intracluster correlation q = 0.008). Within
software (Scientific Software Development, Berlin, Ger- the combined primary end point (ITT population), the
many) and analyzed using summative content analysis majority (377 of 465, or 80%) had a 10% improvement
within the 5Rs framework, including negative case anal- in any one parameter (A1C, SBP, or LDL cholesterol)
ysis for meaning saturation to understand the diversity over baseline, while 78% of the remaining patients (40
of experiences (18,19). We followed the Consolidated of 51) were persistently at target (Supplementary
Criteria for Reporting Qualitative Research framework Figure S1). When examining the primary combined out-
(Supplementary Table S1) (20). come by community, achievement ranged from 87 to
100% (Supplementary Figure S2).
Results
When examining the individual components of the pri-
Primary Outcomes mary end point, the biggest driver of the improvement
The quantitative assessment included seven communi- was A1C. Two-thirds of patients achieved a 10% reduc-
ties at the end of 2 years. At baseline, 516 patients with tion in or persistence at target for A1C (ITT 66% [95%
type 2 diabetes were registered in RADAR, ranging CI 55–77%] and PP 65% [95% CI 54–76]). The propor-
from 28 to 129 per community. The mean age was tion of patients achieving a 10% reduction (221 of 336,
60 years (SD 13.6 years, mean community range or 64%) was similar to the number of patients with
[MCR] 55–65 years), 57% were female (MCR 50–66%), persistence at target (130 of 180, or 71%) in the ITT
the mean A1C was 8.3% (67 mmol/mol) (SD 2.0%, population. The mean change in A1C during follow-up
MCR 8.0–8.7%), the mean SBP was 131 mmHg (SD was 0.93% (95% CI 0.59 to 1.28%, P = 0.001;
19.1 mmHg, MCR 122–137 mmHg), and the mean LDL MCR 1.26 to 0.16%). Among those with an A1C
cholesterol was 2.0 mmol/L (36 mg/dL) (SD 0.9, MCR $7.5% (58 mmol/mol) at baseline (mean 9.70%, SD
1.7–2.3 mmol/L [30.6–41.4 mg/dL] (Table 1). 1.66%; n = 303), mean change in A1C during follow-
up was 1.62% (95% CI 2.18 to 1.06%, PFEATURE ARTICLE Effectiveness of an Organized Diabetes Care Model
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
FIGURE 2 Primary combined end point of achieving a 10% reduction or maintaining values within 10% of target for A1C, SBP, or LDL
cholesterol during 2 years of follow-up.
and 58% (95% CI 46–69%) of the PP population, and LDL Organization of Diabetes Care
cholesterol improved for 40% (95% CI 32–48%) of the We conducted 21 semistructured interviews with 11 indi-
ITT population and 42% (95% CI 34–50% of the PP popu- vidual participants: three remote CCs and eight local HCPs
lation. Unlike A1C, achieving the SBP or LDL cholesterol (e.g., registered nurses, licensed practical nurses, and dieti-
target was driven by achieving a 10% reduction: 134 of tians) from May 2015 to February 2019 (Table 2). Overall,
187 (70%) for SBP and 159 of 236 (66%) for LDL choles- we found improvements in the organization of diabetes
terol in ITT populations, whereas a smaller proportion per- care by the 5Rs, as presented below, with illustrative
sisted at target for SBP (150 of 329 or 45%) or LDL quotes including position (i.e., CC or HCP) and anony-
cholesterol (55 of 280 or 18%). The mean change in SBP mous study code number for each participant.
during follow-up was 6.03 mmHg (95% CI 2.68 to
9.38 mmHg, P = 0.005; MCR 19.64 to 0.82 mmHg). Recognize and Register
Among those with an SBP $140 mmHg at baseline (mean Overall, RADAR facilitated the recognition and registra-
156 mmHg, SD 14.9 mmHg; n = 193), mean change in tion of patients with diabetes. RADAR “identified our
SBP during follow-up was 14.19 mmHg (95% CI 22.55 [diabetes] population” (HCP 5), including “younger
to 5.82; P = 0.006) (MCR 36.17 to 3.45 mmHg). The people that we didn’t know had diabetes” (HCP 4), thus
mean change in LDL cholesterol during follow-up was capturing “a lot more of the population” (HCP 7). Nev-
0.17 mmol/L (95% CI 0.10 to 0.24 mmol/L, P = ertheless, RADAR was limited in identifying new pa-
0.001; MCR 0.38 to 0.02 mmol/L). Among those tients because only physicians can diagnose. “I don’t
with LDL cholesterol $2.5 mmol/L at baseline (mean know if RADAR had any impact on recognizing clients
3.17 mmol/L, SD 0.57 mmol/L; n = 215), mean change . . . [because] we never can diagnose” (HCP 6). As such,
in LDL during follow-up was 0.33 mmol/L (95% CI 0.46 “the registry was only those [patients] already diag-
to 0.21 mmol/L, P = 0.01; MCR 0.71 to 0.03 mmol/L). nosed with type 2 diabetes” (HCP 3).
4 D IA B E TE SJ OUR N A L S.OR G/ C L IN IC A LEURICH ET AL.
TABLE 2 Interview Timing and Participant Roles
Participant Role Interviewed at 6 Months, n Interviewed at 24 Months, n Total, n (%)*
Remote CC 2 3 3 (27)†
Local dietitian 3 3 (27)
Local licensed practical nurse 2 2 (18)
Local registered nurse 3 3 (27)
*Percentages do not sum to 100 due to rounding. †Two CCs were interviewed at both 6 and 24 months.
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
Regardless, RADAR resulted in a “client registry that has communication between on- and off-reserve medical serv-
been created” (HCP 1). The act of centrally registering pa- ices,” but the CCs helped “connect us to the off-reserve
tients in CARE with CC support confirmed the type of dia- services, such as the physicians . . . [and] the communica-
betes for some patients because “many patients had been tion has become more open” (HCP 1). Furthermore,
indicated as ‘other’ diabetes because the HCPs weren’t CARE facilitated communication and coordinated diabetes
sure [of the diagnosis]” (CC 2). CCs helped identify type specialty care such as ophthalmology (HCP 7) and endo-
of diabetes by “looking on [the provincial EMR] through crinology (HCP 6) through report and letter templates.
discharge summaries to find data to support whether [pa- “I use the [patient] report summary, and I can easily fax
tients had] type 2 diabetes” (CC 2) or asking “the nurse to that to the [physician] clinic” (HCP 2). However, im-
confirm with [the patient’s] physician” (CC 1). However, proved relay of information was not reported in all com-
centrally registering patients also resulted in “increasing munities, indicating that more work is needed.
our overall client load” (HCP 1) or feeling overwhelmed
by “seeing my whole population and saying, ‘I should be Recall
doing all these things for everybody’” (HCP 6) in light of RADAR improved timely review and reassessment of pa-
limited resources. tients with diabetes by local HCPs through CARE’s fea-
tures (e.g., tasks, reminders, and patient summaries) and
Relay CC support. “You have very specific tasks that you need to
Overall, RADAR improved HCP access to and sharing accomplish to improve people’s health, and they’re right
of information. Within health centers, local HCPs in the forefront [in CARE]” (HCP 7). CCs facilitated recall
described efficient and comprehensive access to infor- by “looking at the total population, including the ones not
mation through CARE versus relying on patients’ recol- accessing care” (CC 1) and identifying for HCPs which pa-
lections or paper charts. “You don’t have to go into the tients “should be targeted at this time” (HCP 4). As a re-
[paper] chart every time. Even when you’re unfamiliar sult, “we have been able to reach out and connect with a
with a client, all that information is [in CARE] . . . . Be- lot more community members who may not have been
cause, sometimes, your clients are not great historians” utilizing our services for diabetes care” (HCP 1). In addi-
(HCP 7). CCs also enabled access of local HCPs to clini- tion, CCs reviewed “the diabetes guidelines and asked us
cal information contained in other EMRs. “It can take a to follow up on as much as we can with that client” (HCP
lot of time to get access to [the provincial EMR], if we 6). As a result, processes of care were completed. “Blood
are given it at all. With RADAR, [the CCs] populated pressures were taken; foot exams and lab work were
CARE with medical information that is important to the done” (CC 1). Recall support was crucial in the context of
level of care we can provide” (HCP 1). Moreover, CARE busy clinics. “It gets busy, and you get sidetracked, so it
resulted in “improved communication amongst the helps to have that person saying, ‘This is who you’ve got
team” (HCP 7), allowing local HCPs “to communicate to follow up with next; this person needs [this]’” (HCP 4).
everything you’ve done with a client” (HCP 5). This fea-
However, not all HCPs believed CARE improved recall
ture was especially important given staffing challenges.
beyond what existed “because we already set up regular
“We really have a good flow [of information] regardless
of the staff turnover” (CC 1). reminders, like [for A1Cs], foot exams, eye exams . . .
into the [physician] EMR” (HCP 3). Furthermore, in
Finally, RADAR improved communication with providers some communities, “we only case-reviewed half the pa-
outside the health centers. “Prior to RADAR, there was no tients” (CC 1), thus limiting recall. Some HCPs were
5FEATURE ARTICLE Effectiveness of an Organized Diabetes Care Model
uncomfortable recalling patients, saying, “That’s not Discussion
our job’” (CC 1). HCPs resisted recalling patients they
We found that RADAR improved patient-level outcomes
believed did not want their care. “Some of these clients
through improved organization of diabetes care in FN
that [the CCs] asked me to review were ones that don't
communities. In addition, we found significant achieve-
access care here regularly. We know their [glucose] is
ment of our primary outcomes for RADAR participants
high [and] that they have other things going on in their
over 2 years, with the largest effect observed for change
life, so they don't come in for appointments . . . . Chas-
in A1C. This finding is similar to an intervention study
ing them down, [is] not the best use of my time” (HCP
of rural (non-FN) patients with type 2 diabetes, in
3). Another HCP explained, “We tell [the CC] this per-
which improvements in SBP and/or LDL cholesterol
son is not engaged . . . and [to] just leave them alone”
were smaller than improvements in A1C (21). Although
(HCP 6).
glycemic control is essential, further improvements in
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
SBP and/or LDL cholesterol would provide substantial
Resource
macro- and microvascular benefits (22).
RADAR helped improve local HCPs’ ability to support pa-
tients’ diabetes self-management by informing patients of Our results also demonstrated improved diabetes care orga-
health center services and supports, developing care nization (8), which is foundational to improving patient-
plans, and increasing local HCPs’ diabetes knowledge. For level outcomes (7). With regard to the 5Rs, RADAR resulted
example, one respondent said, “Based on the registry, we in central registries, helping communities verify, visualize,
would call clients, introduce ourselves, [and] introduce and recall their diabetes population. The use of patient regis-
the program” (HCP 1) or inform patients that “we have a tries for diabetes management is associated with better pro-
diabetes management support system . . . [and ask] cesses and outcomes of care (23,24). Furthermore, FN
‘Would you like some help?’” (CC 2). This resulted in pa- health directors can use their own registry data as a resource
tients accessing services. “There’s probably 50% more to inform decision-making for local program planning, meet
people coming for their monthly foot care” (HCP 5). federal reporting requirements, and support funding re-
quests based on the needs of and trends in the local patient
Furthermore, CCs helped local HCPs develop care plans
population. RADAR allows for a community-led response
informed by CPGs. “[The CC] reviewed the guidelines
based in data sovereignty (25) and aligned with the princi-
with us and helped us incorporate them into our day-
ples of self-governance and self-determination (9).
to-day care with clients” (HCP 1). This, in part, helped
to increase local HCPs’ diabetes knowledge and “build Second, RADAR facilitated relay of clinical information
local capacity” (CC 1). For example, one respondent essential for continuity and coordination of team-based
said, “[The CC showed us] the gold standards for diabe- diabetes care (11). This included overcoming the re-
tes treatment . . . . I am not an expert on diabetes. I stricted access of local HCPs to patients’ provincial EMR
have learned so much” (HCP 7). Diabetes education data in the current fragmented system, with multiple
was especially valuable to HCPs who did not have time isolated technologies hindering clinical information-
or resources to stay current in their knowledge. “Even sharing necessary for diabetes care (26,27). Within
though we’re close to the nearest town and physicians, health centers, centralized compilation of patients’ clini-
you’re still isolated from information . . . . There may be cal information and care plans in CARE was crucial in
new information, and [the CC is] helpful that way, with the context of the high staff turnover that FN communi-
new stuff or if we have a question” (HCP 4). As a result, ties face (27). In addition, team-based care was en-
local HCPs reported increased confidence in their diabe- hanced through relationship-building among HCPs
tes knowledge. “[The CC] has made a huge difference through CCs’ professional networks, including diabetes
in my confidence with diabetes knowledge” (HCP 1). specialists. This was especially important for remote
However, not all HCPs believed RADAR improved their communities with irregular access to services necessary
diabetes knowledge. “I have a lot of knowledge in dia- for comprehensive diabetes care (11,27).
betes, so it is not anything new” (HCP 2). One respon-
dent noted that the community already had a certified Finally, RADAR increased local HCP capacity (i.e.,
diabetes care and education specialist (HCP 3). Finally, knowledge and confidence) to support diabetes self-
some HCPs requested further education, such as management (resource) through education (e.g., of cur-
“10-minute education sessions on new [CPGs] (HCP6), rent CPGs) and peer support, promoting the long-term
indicating an ongoing need for up-to-date diabetes sustainability of primary outcomes. This is important
knowledge. because lack of adequate diabetes knowledge among
6 D IA B E TE SJ OUR N A L S.OR G/ C L IN IC A LEURICH ET AL.
local HCPs is a barrier to diabetes care and is largely af- care targets within guidelines (11) and have been shown
fected by time/competing priorities, staff turnover, and in many large-scale randomized controlled trials (RCTs) to
changing guidelines (4,28). Furthermore, local HCPs, confer substantial benefits with regard to macro- or micro-
who are the experts in their communities, can apply vascular outcomes (11,21). Second, we designed a prag-
RADAR, including enhanced knowledge of diabetes matic, controlled, community-based intervention aimed at
care, with local patients in appropriate ways that recog- local HCPs as opposed to patients per se. Individual pa-
nize contextual and cultural factors (12). tients or local HCPs within the community could not be
randomized to care with and without RADAR because of
Although RADAR improved diabetes care organization the threat of “contamination” via exposure to some aspects
overall, challenges remain. Centrally registering patients of the intervention within the same community team or
does not necessarily recognize new patients through screen- health facility. Moreover, our community partners were
ing, thereby limiting the population health impact. Future not interested in a traditional RCT; a stepped-wedge de-
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
RADAR activities may include recommended earlier and sign was used, as few communities would accept being the
more frequent screening of type 2 diabetes for FN people control community for an extended duration. Although
(6). Furthermore, centrally registering patients with recall the participating FN communities were diverse, they may
functionality increased local HCPs’ workload, contributing not be representative of all FN communities. Additionally,
to feelings of stress. In addition, although RADAR encour- the participating local HCPs who were interviewed for the
aged local HCPs to actively engage or re-engage patients, qualitative component of the study are a sample of the
some HCPs resisted recalling patients, thus limiting the pro- health care workers involved in the implementation of
active care essential to improving patient outcomes (11). RADAR. Although almost all FN communities are dealing
This challenge is not unique to FN communities, as HCPs with similar issues in providing diabetes care, it is possible
must balance proactive care with patients’ right to decline that some of our findings may not be applicable to all com-
care. However, it can become a greater challenge in FN munities, depending on local resources.
communities, as patients may have competing priorities
that take precedence over diabetes self-management (re- Conclusion
source), such as housing or food insecurity related to his-
RADAR is an effective, tailored approach to support the
toric and social injustices (5,9). Although local HCPs are
organization of and capacity building in diabetes care for
experts in their communities, including knowing which pa-
FN communities. From our findings, it is reasonable to as-
tients want to engage or re-engage with diabetes care,
sume that this intervention could be applied to other in-
some HCPs may believe it is patients’ responsibility to seek
digenous populations in jurisdictions around the globe.
care and outside of their role as care providers to facilitate
patient engagement proactively. This opinion may be re-
ACKNOWLEDGMENTS
lated to local HCPs’ feelings of stress, which is understand-
The authors thank their FN partners for their ongoing and
able in the context of their limited resources. Nonetheless, generous support and recognize that this work was imple-
this belief may limit community-level comprehensive diabe- mented in the traditional territories of their Treaty 6, 7, and
tes care and requires further exploration. Indeed, we previ- 8 FN partners. The authors thank OKAKI for their support
ously found that the 5Rs of diabetes care organization are and participation in the evaluation of RADAR. They also ac-
knowledge the significant contribution of Dr. Sumit (Me2)
interrelated and influenced by financial and human resour- R. Majumdar, who died in 2018, to the study design.
ces (the sixth R) (8). Regardless, RADAR created the condi-
tions for local HCPs and patients to collaborate in diabetes FUNDING
self-management in this resource-challenged context.
This work was funded by the Canadian Institutes of Health
Research (MOP# 143562), Alberta Innovates Health Solu-
Strengths and Limitations tions, and The Lawson Foundation.
Our incorporation of quantitative and qualitative compo-
DUALITY OF INTEREST
nents to comprehensively measure effectiveness for both
No potential conflicts of interest relevant to this article
clinical outcomes and diabetes care organization is a
were reported.
strength. However, this study is not without limitations.
First, given our follow-up of 2 years, we used intermediate AUTHOR CONTRIBUTIONS
outcomes as opposed to hard clinical end points (e.g., oc- D.T.E. and S.S. conceived the study, designed its protocols, and
currence of heart attack or stroke). Nevertheless, A1C, received ethics approval and funding. D.T.E. led the quantitative
SBP, and LDL cholesterol are well established diabetes data collection and analysis, with support from J.K.M.-S. L.A.W.
7FEATURE ARTICLE Effectiveness of an Organized Diabetes Care Model
led the evaluation design and conducted qualitative data collec- analysis of contemporary First Nations research and some options
tion and analysis. D.T.E., L.A.W., and A.S. drafted the manuscript. for First Nations communities. J Aborig Health 2004;1:80–95
L.C. and J.A.J. actively contributed to the study design. All au- 14. First National Information Governance Centre. The First
thors read and approved the final manuscript. D.T.E. is the guar- Nations principles of OCAP. Available from https://fnigc.ca/
antor of this work and, as such, had full access to all the data in ocap-training. Accessed 24 May 2022
the study and takes responsibility for the integrity of the data
and the accuracy of the data analysis. 15. Majumdar SR, Guirguis LM, Toth EL, Lewanczuk RZ,
Lee TK, Johnson JA. Controlled trial of a multifaceted
intervention for improving quality of care for rural patients
REFERENCES
with type 2 diabetes. Diabetes Care 2003;26:3061–3066
1. King M. Chronic diseases and mortality in Canadian
16. Hussey MA, Hughes JP. Design and analysis of stepped wedge
Aboriginal peoples: learning from the knowledge. Prev
cluster randomized trials. Contemp Clin Trials 2007;28:182–191
Chronic Dis 2011;8:A07
17. Sandelowski M. What’s in a name? Qualitative
2. Oster R, Toth EL, King M, Crowshoe L. Diabetes and the
description revisited. Res Nurs Health 2010;33:77–84
Downloaded from http://diabetesjournals.org/clinical/article-pdf/doi/10.2337/cd22-0090/696889/cd220090.pdf by guest on 16 May 2023
Status Aboriginal Population in Alberta. Edmonton, Alberta,
Institute of Health Economics, 2011 18. Hsieh HF, Shannon SE. Three approaches to qualitative
content analysis. Qual Health Res 2005;15:1277–1288
3. Turin TC, Saad N, Jun M, et al. Lifetime risk of diabetes
among First Nations and non-First Nations people. CMAJ 19. Hennink MM, Kaiser BN, Marconi VC. Code saturation
2016;188:1147–1153 versus meaning saturation: how many interviews are
enough? Qual Health Res 2017;27:591–608
4. Harris SB, Naqshbandi M, Bhattacharyya O, Hanley AJ,
Esler JG; CIRCLE Study Group. Major gaps in diabetes 20. Tong A, Sainsbury P, Craig J. Consolidated criteria for
clinical care among Canada’s First Nations: results of the reporting qualitative research (COREQ): a 32-item checklist
CIRCLE study. Diabetes Res Clin Pract 2011;92:272–279 for interviews and focus groups. Int J Qual Health Care
2007;19:349–357
5. Oster RT, Virani S, Strong D, Shade S, Toth EL. Diabetes
care and health status of First Nations individuals with type 2 21. Johnson JA, Eurich DT, Toth EL, Lewanczuk RZ, Lee TK,
diabetes in Alberta. Can Fam Physician 2009;55:386–393 Majumdar SR. Generalizability and persistence of a
multifaceted intervention for improving quality of care for rural
6. Diabetes Canada Clinical Practice Guidelines Expert patients with type 2 diabetes. Diabetes Care 2005;28:783–788
Committee; Crowshoe L, Dannenbaum D, Green M, Henderson
R, Hayward MN, Toth E. Type 2 diabetes and indigenous 22. Diabetes Canada Clinical Practice Guidelines Expert
peoples. Can J Diabetes 2018;42(Suppl. 1):S296–S306 Committee; Stone JA, Houlden RL, Lin P, Udell JA, Verma
S. Cardiovascular protection in people with diabetes. Can J
7. Clement M, Filteau P, Harvey B, et al.; Diabetes Canada Diabetes 2018;42(Suppl. 1):S162–S169
Clinical Practice Guidelines Expert Committee. Organization
of diabetes care. Can J Diabetes 2018;42(Suppl. 1):S27–S35 23. Renders CM, Valk GD, Griffin SJ, Wagner EH, Eijk Van JT,
Assendelft WJJ. Interventions to improve the management of
8. Wozniak LA, Johnson JA, Eurich DT. Working towards a diabetes in primary care, outpatient, and community settings:
better understanding of type 2 diabetes care organization a systematic review. Diabetes Care 2001;24:1821–1833
with First Nations communities: a qualitative assessment.
24. Stroebel RJ, Scheitel SM, Fitz JS, et al. A randomized
Arch Public Health 2020;78:7
trial of three diabetes registry implementation strategies in
9. Katz A, Enns J, Kinew KA. Canada needs a holistic First a community internal medicine practice. Jt Comm J Qual
Nations health strategy. CMAJ 2017;189:E1006–E1007 Improv 2002;28:441–450
10. Eurich DT, Majumdar SR, Wozniak LA, et al. Addressing 25. Canadian Alliance for Healthy Hearts and Minds First Nations
the gaps in diabetes care in first nations communities with Cohort Research Team. “All about us”: indigenous data analysis
the reorganizing the approach to diabetes through the workshop—capacity building in the Canadian Alliance for Healthy
application of registries (RADAR): the project protocol. BMC Hearts and Minds First Nations cohort. CJC Open 2019;1:282–288
Health Serv Res 2017;17:117
26. Misra V, Sedig K, Dixon DR, Sibbald SL. Prioritizing
11. Diabetes Canada Clinical Practice Guidelines Expert coordination of primary health care. Can Fam Physician
Committee. Diabetes Canada 2018 Clinical Practice 2020;66:399–403
Guidelines for the Prevention and Management of Diabetes
27. Crowshoe LL, Henderson RI, Green ME, Jacklin KM,
in Canada. Can J Diabetes 2018;42(Suppl. 1):S1–S325
Walker LM, Calam B. Exploring Canadian physicians’
12. Wozniak LA, Soprovich AL, Johnson JA, Eurich DT. experiences with type 2 diabetes care for indigenous
Adopting and implementing an innovative model to organize patients. Can J Diabetes 2018;42:281–288
diabetes care within First Nations communities: a 28. Minore B, Boone M, Katt M, Kinch P, Birch S,
qualitative assessment. BMC Health Serv Res 2021;21:415 Mushquash C. The effects of nursing turnover on continuity
13. Schnarch B. Ownership, Control, Access, and Possession of care in isolated First Nation communities. Can J Nurs
(OCAP) or self-determination applied to research: a critical Res 2005;37:86–100
8 D IA B E TE SJ OUR N A L S.OR G/ C L IN IC A LYou can also read