Diabetes Care Assessment, Planning, and Management during COVID-19
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Diabetes Care Assessment, Planning,
and Management during COVID-19
Credit Information
§ If you are a social worker in a National Association of Social Workers (NASW) state and
would like to receive CE credits through NASW for this event, please complete the pre-test
posted here: https://www.surveymonkey.com/r/DiabetesCOVIDPre
§ You will also be required to complete a post-test; a link to this test will appear at the end of the
presentation.
§ If you are a registered nurse and would like to receive CNE credits through the California
Board of Registered Nursing for this event, please complete the pre-test posted here:
https://www.surveymonkey.com/r/DiabetesCOVIDPre
§ You will also be required to complete a post-test; a link to this test will appear at the end of the
presentation.
Audio and Platform Information
§ The audio portion of the presentation will automatically stream through your computer
speakers. If you experience challenges with the audio, please click the phone icon at the
bottom of the screen for dial-in information.
§ If you are experiencing any technical difficulties with this platform, please use the Q&A
feature for assistance or click the help button for additional information.
0 https://www.ResourcesForIntegratedCare.com
May 5, 2021
Diabetes Care Assessment, Planning,
and Management during COVID-19
https://www.ResourcesForIntegratedCare.com
Overview
§ This session will include presentations, followed by live Q&A
with participants
§ Video replay and slide presentation are available after each
session at: https://www.resourcesforintegratedcare.com
2 https://www.ResourcesForIntegratedCare.com
Audio Options
§ There are two ways to listen to
today’s presentation
1. Audio should automatically
stream through your computer’s
speakers. Make sure that your
computer is connected to reliable
internet and that the speakers are
turned up.
2. If the computer audio option is not
working for you, there is a dial-in
option. To access this option at
any time, click on the black phone
widget at the bottom of the
screen. A phone number and
access code will appear. Calling
the number will allow you to listen
to the presentation through your
phone.
https://www.ResourcesForIntegratedCare.com
Accreditation
§ Individuals are strongly encouraged to check with their specific
regulatory boards or other agencies to confirm that courses taken
from these accrediting bodies will be accepted by that entity.
§ The American Geriatrics Society has been approved by the California
Board of Registered Nursing to provide continuing education.
§ The American Geriatrics Society is accredited by the National
Association of Social Workers (NASW) to provide continuing education
for social workers.
4 https://www.ResourcesForIntegratedCare.com
Continuing Education Information
If You Are A: Credit/Contact Hour Options Requirements
National Association of Social Workers & AGS Continuing Nursing Education Credits
The National Association of Social Workers designates this 1. Complete the pre-test at the
webinar for a maximum of 1 Continuing Education (CE) credit beginning of the webinar
hour. 2. Complete the post-test with
a score of 80% or higher by
Social Worker 11:59pm May 6, 2021
Please note: New York, Michigan, and West Virginia do not
accept National CE Approval Programs for Social Work. New
Jersey, Idaho, and Oregon do not recognize NASW National
Approval.
1. Complete the pre-test at the
The American Geriatrics Society designates this program beginning of the webinar
eligible for 1 nursing contact hour through the California Board 2. Complete the post-test with
Nurse a score of 70% or higher by
of Registered Nursing.
11:59pm May 6, 2021
5 https://www.ResourcesForIntegratedCare.com
Support Statement
§ This webinar is supported through the Medicare -Medicaid Coordination
Office (MMCO) in the Centers for Medicare & Medicaid Services (CMS)
to help beneficiaries dually eligible for Medicare and Medicaid have
access to seamless, high-quality health care that includes the full range
of covered services in both programs. To support providers in their efforts
to deliver more integrated, coordinated care to dually eligible
beneficiaries, MMCO is developing technical assistance and actionable
tools based on successful innovations and care models, such as this
webinar.
§ To learn more about current efforts and resources, visit Resources for
Integrated Care at: https://www.resourcesforintegratedcare.com or on
Twitter @Integrate_Care
6 https://www.ResourcesForIntegratedCare.com
Introductions
■ Vivian Cheng, PharmD, BCPS
Primary Care Clinical Pharmacy Specialist, Bowdoin Street Health
Center
■ Nicole Kohler MS, CDCES
Clinical Design Specialist, Gateway Health
■ Katie Sheridan MSW, LSW
Case Management, Gateway Health
7 https://www.ResourcesForIntegratedCare.com
Introductions
■ Vivian Nnacho Ayuk, PharmD, CDCES
Chief Executive Officer, Sorogi
■ Fontella Young
Consumer, Sorogi
8 https://www.ResourcesForIntegratedCare.com
Learning Objectives
§ Describe the disproportionate impact of COVID-19 on dually
eligible individuals with diabetes, particularly those from
communities of color
§ Identify approaches to providing both clinical management
and self-management education and support while adhering
to physical distancing protocols
§ Recognize barriers to telehealth for some members and
identify ways to successfully overcome them
§ Name strategies for effectively connecting members to
resources and supports, including food, medications, and
supplies, during COVID-19
9 https://www.ResourcesForIntegratedCare.comWebinar Outline § Polls § Overview of Diabetes Management § Diabetes Care Management and the Clinical Pharmacist Role During COVID-19 § Diabetes Management and Interventions During COVID-19 § Diabetes Care and Telehealth During COVID-19 § Audience Q&A § Evaluation 10 https://www.ResourcesForIntegratedCare.com
Dually Eligible Individuals
with Diabetes
§ Of the population of people dually eligible for Medicare and Medicaid, 23
percent of those 21-64 years and 25 percent of those 65 years and over
have a diabetes diagnosis1
§ Dually eligible individuals are disproportionally impacted by COVID-19, with
case rates 2.6 times higher than Medicare-only beneficiaries9
§ Diabetes rates for racial and ethnic minorities age 18+ are up to three
times higher than white adults2,3,4,5,6
§ Uncontrolled diabetes can lead to poor health outcomes, including
cardiovascular disease, nerve damage, and damage to various organs 7
§ Poorly controlled diabetes is also associated with poorer COVID-19
outcomes (1% vs 11% mortality)8
11 https://www.ResourcesForIntegratedCare.comImportance of Diabetes Management § Persistent elevation in blood sugar can cause damage to nerves and blood vessels, as well as to organs, including eyes and kidneys10 § Controlling blood sugar requires attention to diet and exercise, and may require the use of oral and injectable medications, including insulin11 § People with diabetes also need to adequately control their blood pressure and cholesterol to reduce cardiovascular risk, including heart disease or a stroke12 § The hemoglobin A1c (A1c) blood test is the best measure of a person's blood sugar control over the previous three months and should be monitored at least twice a year13 12 https://www.ResourcesForIntegratedCare.com
Diabetes Care Management and the Clinical
Pharmacist Role during COVID-19
Vivian Cheng,
PharmD, BCPS
Primary Care Clinical
Pharmacy Specialist
13 https://www.ResourcesForIntegratedCare.comAbout Bowdoin Street Health Center (BSHC)
§ Founded by community residents in 1972 in
Dorchester, MA (Boston’s largest and most
diverse neighborhood)
§ Licensed under Beth Israel Deaconess
Medical Center
§ Part of Beth Israel Lahey Health Performance
Network (clinically integrated network
focused on value-based, cost-effective care)
§ Serves all patients, regardless of insurance
or immigration status
§ Diverse health center staff speak many
languages, including Spanish, Portuguese,
Haitian Creole, and Cape Verdean Creole
§ Comprehensive services include adult and
family medicine, mental health, pediatrics,
and community health
14 https://www.ResourcesForIntegratedCare.comPatient Demographics
Demographics % of Patient Population
Adults with Type 2 diabetes 15.4%
Reside locally 66%
Black (% of whom who are
56% (22%)
Cape Verdean)
Other 22%
Race/Ethnicity Latino 7%
Asian 3%
White 4%
Unknown 8%
Under 18 22%
Age (years) 18-64 63%
65+ 15%
15 https://www.ResourcesForIntegratedCare.comBSHC Diabetes Initiatives
§ The goal of population health initiatives is to:
§ Proactively connect with patients with uncontrolled diabetes
§ Re-engage patients overdue for follow-up
§ Identify opportunities to optimize diabetes care management
§ Activities supporting population health initiatives related to diabetes include:
§ Staying up to date on evidence-based use of diabetes medicines
§ Tracking changes to insurance coverage and costs for diabetes medications
§ Analyzing patient data from electronic medical records and generating patient-level
reports to identify potential for medication regimen improvement
§ During COVID-19, proactive outreach and population health management is
even more critical for identifying members with uncontrolled diabetes
§ BSHC patient population disproportionately affected by COVID -19; many patients are afraid
of attending in-person appointments and are at risk of going without care
§ Proactive outreach remains critical as some patients, including non-English speaking
patients, may have challenges in scheduling appointments via phone
16 https://www.ResourcesForIntegratedCare.comBSHC Diabetes Care Approach
§ Multidisciplinary patient-centered
care through integrated care teams
§ (Pre-COVID) Diabetes group
education classes and Diabetes
Prevention Program
§ (Pre-COVID) Wellness center: two
exercise/activity rooms,
demonstration kitchen
§ Combination of health
education, physical activity,
and support
17 https://www.ResourcesForIntegratedCare.comThe Clinical Pharmacist Role
§ The clinical pharmacist, when designated by BSHC physicians, assists
with supporting BSHC patients with diabetes, hypertension, and high
cholesterol by:
§ Conducting frequent follow-up check-ins, via telehealth and in-person
§ Adjusting and optimizing medications to align with best-practice guidelines
and patient needs and preferences
§ Address patients' questions and concerns about medication cost
§ Ordering relevant lab work
§ Providing patient and provider education
18 https://www.ResourcesForIntegratedCare.comImpact of COVID-19 on People with Diabetes § Less physical activity, which can lead to weight gain and worsened blood sugar control § Decreased access to healthy foods, due to both financial constraints and reduced access to grocery stores § Financial stressors, which can prevent people from accessing medication and testing supplies § Concerns about COVID-19 exposure can result in hesitancy around coming in to the health center, and closures/limited hours of primary care providers also reduce access § Lack of technology access/barriers to using technology may impact ability to use telehealth services § Isolation, lack of social connections, and exacerbation of mental health conditions, which can also be worsened by the stress of managing diabetes 19 https://www.ResourcesForIntegratedCare.com
Supports for People with Diabetes
during COVID-19
§ Telehealth via phone (primarily) or video
§ Currently via third-party applications; Beth Israel Deaconess Medical Center-specific virtual
platform being rolled out
§ Telemonitoring of home blood sugars, blood pressures
§ Creative solutions: free blood pressure kits, scheduling patients for lab work when
appropriate
§ Weekly High Intensity Interval Training (HIIT), Zumba, and Cardio Blast classes
available via Zoom
§ Hosted a “Healthy at Home” virtual wellness fair in Fall 2020
§ Topics included understanding COVID-19, diabetes management/blood sugar management
at home, nutrition classes, and checking blood pressure at home
§ Nutrition and food access
§ Community health worker focused on food access helps connect members to SNAP
benefits, Fresh Truck, farm stand, “Bowdoin Bucks”
§ “Food for Health” delivery program
20 https://www.ResourcesForIntegratedCare.comClinical Management Considerations
§ Prioritize value-based, evidence-based medications
§ Medications with cardiovascular/renal benefit should be prioritized over those
without additional benefits, per the 2021 American Diabetes Association
Standards of Medical Care
§ Consider patient-specific factors
§ Past medical history
§ Dexterity for blood glucose testing and insulin administration
§ Language preference, literacy, and health literacy
§ Ask questions and confirm understanding, rather than making assumptions
§ Double check refill histories
§ Ask open-ended questions and avoid leading questions
§ Use teach-back technique to verify comprehension
§ Have shared-decision making discussions when setting goals and choosing
medications
§ Be flexible and empathetic; treat the patient, not the number
21 https://www.ResourcesForIntegratedCare.comClinical Management Considerations
(cont.)
§ Identify potential supports for individuals who are blind or
have low vision, or who are deaf or hard of hearing,
including:
§ Working with a family member or visiting nurse to keep a blood sugar
logbook
§ Simplifying medication regimens, and utilizing medications with low
risk for hypoglycemia
§ Using continuous glucose monitors to reduce need for frequent finger
pricks
§ When appropriate, use glucose monitors with audio alerts
22 https://www.ResourcesForIntegratedCare.comCase Example 1
§ Mr. M. is a 56-year-old Indian man who is dually eligible. His A1c was
10.3% in February 2020. He has a strong family history of cardiovascular
disease
§ Due to co-morbidities associated with an increased risk of severe illness
from COVID-19, Mr. M was fearful about going in to a provider office
§ First, the BSHC team re-engaged Mr. M. via telehealth and determined:
§ Mr. M. only checked his blood glucose when he felt unwell
§ Mr. M.’s prescribed medication brand wasn’t covered, leading to sporadic
medication adherence
§ Then, through frequent telehealth check-ins, BSHC provided education
on the importance of diet and frequent blood sugar testing. Also adjusted
Mr. M.’s medication to support medication adherence
§ Mr. M. was able to bring his blood glucose under control; A1c improved
to 8.4% by March 2021
23 https://www.ResourcesForIntegratedCare.comCase Example 2
§ Ms. B. is a 65-year-old Cape Verdean woman, also dually eligible, who
lives alone an hour away from the clinic
§ Her last test showed an A1c of 10.9% in July 2020
§ She cannot read or speak English, and was having difficulties checking
her blood sugar, as she didn’t understand the instructions for testing, or
what the numbers meant
§ Ms. B was also not taking her medication as prescribed, as she was
physically using her medication wrong (incorrectly dosing medication with
dial), and struggled with daily injections
§ Via telehealth and in-person visits with an interpreter, the BSHC team:
§ Connected with Ms. B.’s daughter (with permission), who was able to help
support her mother in taking her medication and checking her blood sugar
§ Enrolled Ms. B. in medication packaging service (a weekly bubble pack)
§ Simplified her diabetes medication (changed from a daily to weekly medication,
no dial mechanism)
§ Average fasting blood glucose now 140 mg/dL (estimated A1c ~6.5%)
24 https://www.ResourcesForIntegratedCare.comMoving Forward Post-COVID-19
§ Plans for BSHC’s diabetes care management post-COVID-
19, include:
§ Re-instituting in-person diabetes education classes and nutrition
classes
§ Continuing to offer virtual visit options, as telehealth and
telemonitoring likely become more popular and more integrated into
standard practice
§ For example, patients may not always have to come into the clinic for a
provider to review their glucometer; continue to do telephonic/virtual
visits to review home blood sugar readings
§ Construction of on-site clinic pharmacy, which will make it easier for
patients to get their medications
25 https://www.ResourcesForIntegratedCare.comDiabetes Management and Interventions During
COVID-19
Nicole Kohler, MS, Katie Sheridan, MSW,
CDCES LSW
Clinical Design Specialist Case Management
26 https://www.ResourcesForIntegratedCare.comAbout Gateway Health
§ Serves 340,000 members through Medicare Assured, a Dual
Eligible Special Needs Plan (D-SNP) and Pennsylvania
Medicaid Managed Care Organization
§ Headquartered in Pittsburgh, PA with over 1,500 staff
members
Our mission Our vision
Our mission is to care for the We see a future in which
whole person in all communities everyone has equal opportunity
where the need is the greatest. to achieve their best health.
27 https://www.ResourcesForIntegratedCare.comDiabetes Management Workgroup
§ Gateway Health’s interdisciplinary workgroup aims to
streamline development, implementation, and evaluation of
diabetes-related initiatives
§ Includes representatives from quality improvement, strategy and
innovation, medical management, case management, provider
teams, community engagement, analytics, and pharmacy
§ Discuss the spectrum of diabetes management and care,
including clinical outcomes and barriers to care
§ Identify opportunities and best practices to improve diabetes
management
§ Utilize HEDIS measures to inform outreach and to establish
understanding of population statistics and diabetes prevalence
§ During the COVID-19 pandemic, monitor specific health risks for
members with diabetes
28 https://www.ResourcesForIntegratedCare.comDiabetes Case Management
§ Gateway case managers are Licensed Registered Nurses or
Social Workers, and include both telephonic and field-based
case managers (all telephonic during COVID-19)
§ Case managers coordinate with other members of the
interdisciplinary care team, including providers and wellness
coaches
§ Wellness coaching for members with diabetes is available by
request through Certified Diabetes Care and Education
Specialists (CDCES); virtual during COVID-19
§ Members learn about wellness coaching from case managers
and by visiting the member portal
29 https://www.ResourcesForIntegratedCare.comCDCES Wellness Coaching
§ CDCES identify diabetes-related distress through a simple,
two-question screening and if positive, a longer assessment
§ Diabetes-related distress includes feeling overwhelmed with diabetes
management, fears/worries about potential complications, and feeling
discouraged about not meeting blood sugar goals
§ Wellness Coaches complete assessment and use a care plan to
set goals with the member. Coaches implement interventions and
measure members’ progress.
§ Assessments and clinical judgement guide CDCES
coaching; coaching may be complete after one call, or
continue for several months
§ CDCES work with members to identify self-care strategies, including
healthy coping, healthy eating, being active, self-monitoring, taking
medication, problem solving, and reducing risk
30 https://www.ResourcesForIntegratedCare.comAdjusting Diabetes Management
during COVID-19
§ COVID-19 pandemic resulted in changes to diabetes workgroup
processes, including:
§ Staff transition to virtual environment
§ Strategizing ways to engage members virtually
§ Additional changes to member outreach and education, including:
§ Formation of COVID-19 vaccine focused workgroup focused on
outreach to members who are high risk for COVID-19 complications,
including those with diabetes
§ Proactive outreach and education calls to members at high -risk of
adverse COVID-19 outcomes, including members with diabetes
§ Mailing at-home testing kits for A1c and nephropathy for members
overdue for testing at start of pandemic
§ Eventually worked with providers to mail kits to other members, as a
result of lab closures and member concerns about in-person testing
§ Transition of all field case managers to virtual engagement
environments
31 https://www.ResourcesForIntegratedCare.comCOVID-19 Outreach and Identifying
Barriers to Care
§ To identify the barriers to care that members are experiencing
during COVID-19, Gateway case managers are conducting
outreach calls
§ Specifically targeting members at high-risk of COVID-19 hospitalization,
including members with diabetes, HIV/AIDS, hypertension, COPD, and
congestive heart failure
§ Outreach calls provide an opportunity for case managers to:
§ Provide COVID-19 education and information on CDC guidelines
§ Assess needs around social determinants of health, barriers to care, and
physical and behavioral health needs
§ Offer wellness coaching
§ Discuss plans with members for what they will do if they have to
quarantine or get COVID-19
§ Provide information on COVID-19 vaccines, address vaccine hesitancy,
and support scheduling vaccinations for members and their families
32 https://www.ResourcesForIntegratedCare.comCOVID-19 Barriers to Care – Transportation Access
Concern
Members may forgo appointments or be unable to obtain medications and food
without adequate transportation
Potential Impact
Decline in members’ overall health and wellbeing, possible inpatient admission,
or risk of member not being able to maintain living in community
Interventions
§ Provide education on the supplemental transportation benefit for Medicare
members
§ Connect members to Gateway’s supplemental non-medical transportation
benefit for insulin-dependent members with diabetes
§ Connect members to the Medical Assistance Transportation Program
(MATP) for free transportation to medical visits through Pennsylvania’s
Medicaid program
§ Connect members to home delivery options for medications and food and
telehealth visits, including helping members make decisions on where to
seek care (e.g., telehealth, in-person)
33 https://www.ResourcesForIntegratedCare.comCOVID-19 Barriers to Care – Food Access
Concern
Lack of food affordability or availability leading to limited choices or not eating
Potential Impact
Unstable blood sugars, weight gain, wounds that will not heal (due to poor
nutrition, lack of protein in diet, etc.)
Interventions
§ Education on diet for diabetes, healthy eating on a budget, and accessing
food bank resources
§ Telephonic registered dietitian (RD) appointments
§ Helping members find food banks in their area and set up appointments to
pick up food
§ Referring members to home-delivered meal and grocery delivery services
and providing home-delivered meals after hospital discharge
§ Providing information on increased SNAP benefits and where to get
additional information on their increased benefits, if relevant
34 https://www.ResourcesForIntegratedCare.comCOVID-19 Barriers to Care – Provider Availability
Concern
• Without regular appointments, providers do not have regular in-person
contact to assess status, and members may not be able to address medical
or behavioral health needs.
• Members may also lack smartphone or computer/internet access to make or
access telehealth appointments, and lab closures may make it more difficult
to get bloodwork done.
Potential Impact
Decline in members’ overall health and wellbeing, possible inpatient admission,
or risk of member not being able to maintain living in community
Interventions
§ Encouraging member, provider, and caregiver collaboration, and ongoing
support for members in addressing needs with providers
§ Member education in regards to telehealth options
§ Sending members at-home HbA1c testing kits via mail
§ Blood pressure monitors approved at no cost and provided via a durable
medical equipment (DME) company
35
https://www.ResourcesForIntegratedCare.comCOVID-19 Barriers to Care – Medication Needs
Concern
Members may run out of medication, may lack access to transportation to pick
up refills on time, or may be concerned about COVID-19 exposure when
picking up medications
Potential Impact
Decline in members’ overall health and wellbeing, possible inpatient admission,
or risk of member not being able to maintain living in community
Interventions
§ Increased allowance of 90-day medication supply
§ Copays/fees waived for diabetic testing supplies (2020), no copays/fees for
diabetic supplies in 2021
§ Arranging pharmacy delivery and at-home medication packs
36 https://www.ResourcesForIntegratedCare.comCOVID-19 Barriers to Care – Mental Health
Concern
Due to social distancing restrictions, there is a greater risk of isolation
Potential Impact
Depression/anxiety and fear around leaving the home may result in lack of
consistency in diabetic medication adherence
Interventions
§ Arranging telehealth visits
§ Providing education on coping skills
§ Connecting members to behavioral health providers
§ Referring members to virtual support groups
37 https://www.ResourcesForIntegratedCare.comCOVID-19 Barriers to Care – Lack of Exercise
Concern
Limited options for places to exercise due to social distancing restrictions and
gym closures
Potential Impact
Weight gain, decrease in mobility, at risk for developing hypertension or
diabetic complications
Interventions
§ Silver Sneakers virtual options such as online classes
§ At-home programs: one kit that can be ordered once a year and contains
exercise equipment for various activities (walking – pedometer, toning –
ball, strength – resistance band, yoga – yoga strap)
38 https://www.ResourcesForIntegratedCare.comSuccess Story § Kendra, a member dually eligible for Medicare and Medicaid, was referred to case management after a recent in -patient hospital stay for uncontrolled diabetes with osteomyelitis (bone infection) of her foot § Kendra shared that her health had declined since the start of the COVID- 19 pandemic, as she was in fear of leaving her home – until she had to be hospitalized § An initial assessment, including conversations between Kendra’s Gateway case manager and her home health aide, identified needs, barriers, and possible interventions § Kendra also identified lack of transportation as a barrier to attending provider appointments, and indicated discomfort related to frequent blood sugar testing 39 https://www.ResourcesForIntegratedCare.com
Success Story (cont.)
§ Kendra’s case manager supported her in accessing:
§ Bathroom safety equipment (supplemental benefit) to reduce fall risks
associated with osteomyelitis. Safety equipment included grab bars, tub
rail, toilet seat riser, and a shower stool
§ Transportation (supplemental benefit), including assistance in making
transportation arrangements for follow-up appointments
§ Case manager also provided education around:
§ Alternative glucometers, including a continuous glucose monitor to
address discomfort related to frequent testing
§ Diabetic diet, and other information around maintaining a healthy lifestyle
at home during COVID-19
§ Kendra has since switched to a continuous glucose monitor and
implemented small changes to her diet, including using a food log,
and has reported regular blood sugar monitoring and a normal
blood sugar range
40 https://www.ResourcesForIntegratedCare.comDiabetes Care and Telehealth During
COVID-19
Vivian Nnacho Fontella Young
Ayuk, PharmD, Consumer
CDCES
Chief Executive Officer
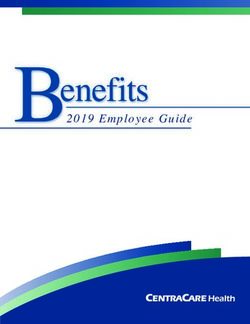
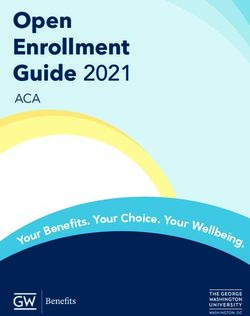
41 https://www.ResourcesForIntegratedCare.comAbout Sorogi
§ A health and wellness company
% of People with Diabetes*
committed to serving both the
people living with chronic health
conditions and the providers who
care for them
§ Community characteristics
§ Majority of participants are
residents of Wards 7 & 8 in
Washington DC
§ > 90% African American
§ High number of food deserts
§ Limited community education and * Behavioral Risk Factor Surveillance System
support programs Survey Data from DC Health’s Center for
Policy Planning and Evaluation
42 https://www.ResourcesForIntegratedCare.comDemographics – Participants with Diabetes
§ Age distribution
§ < 35 years – 6%
§ 35-64 years – 68%
§ ≥ 65 years – 26%
§ Gender
§ Female – 80%
§ Male – 20%
§ African Americans - 99%
§ Dually eligible for Medicare and Medicaid - 24%
43 https://www.ResourcesForIntegratedCare.comPrograms for Participants with Diabetes
§ Diabetes Self-Management Education and Support
(DSMES)
§ Evidence-based, cost-effective curriculum to improve behavioral
health and clinical outcomes for persons with diabetes
§ Diabetes Prevention Program (DPP)
§ Evidence-based (CDC) curriculum to prevent or delay Type 2
diabetes via weight management and increased physical activity
§ Remote patient monitoring (RPM)
§ Monitoring of participant-generated data to improve care via
Bluetooth devices
§ Available to participants in diabetes programs
44 https://www.ResourcesForIntegratedCare.comDiabetes Care Management Model § Participants in both the DSMES program and DPP choose their care team based on their goals and care plan; team members may include: 45 https://www.ResourcesForIntegratedCare.com
Diabetes Care Management Team Roles
§ Certified Diabetes Care and Education Specialist
§ Provides overall care management
§ Registered Dietitian
§ Provides group and one-on-one sessions for participants in DSMES
and DPP programs; provides personalized meal plans as needed
with follow up support
§ Pharmacist
§ Provides medication education and works with participants to
increase access to medications and devices needed to improve care
§ Peer Support Coach
§ Facilitates peer support sessions
§ Certified Lifestyle Coach
§ Facilitates DPP sessions and supports our CDCES
46 https://www.ResourcesForIntegratedCare.comSorogi’s Unique Diabetes Care
Management Virtual Support Model
EDUCATION
REMOTE MONITORING
Pre-diabetes
Diabetes Actionable patient data
Hypertension Monthly progress reports
Medication adherence
SUPPORT
FOLLOW-UP
Peer support group
Set short & long term goals
Incentive program
Accountability coach
Cooking demonstrations
Exercise program
47 https://www.ResourcesForIntegratedCare.comCOVID-19 Challenges § Switching to telehealth for group and individual sessions for the first time during COVID-19 § Maintaining participant engagement in DSMES program and DPP § Loss of community resources § Communicating with healthcare providers due to office closures, remote work, and reduction in office staff 48 https://www.ResourcesForIntegratedCare.com
COVID-19 Virtual Activities
§ In response to the COVID-19 pandemic, Sorogi developed a
telehealth approach for the following programs and activities:
§ Diabetes Prevention Program activities
§ Diabetes Self-Management Education and Support activities
§ All in-person activities became virtual, including:
§ Participant onboarding (e.g., how to use a blood glucose meter,
understanding the signs of hypoglycemia)
§ Education around healthy eating and nutrition, including cooking
demonstrations and grocery store tours
§ Peer support groups
49 https://www.ResourcesForIntegratedCare.comSupports for Participants with Diabetes
during COVID-19
§ Sorogi is supporting participants with diabetes by providing:
§ Education on how to access transportation options, via telehealth
§ Education on effective use of covered devices (e.g., blood glucose
devices and blood pressure monitors)
§ Grocery store cards to use for purchasing fresh fruits and vegetables
§ Virtual grocery store tours and cooking demonstrations
§ Sorogi also leverages partnerships with:
§ Local pharmacies and insurance providers to assist with access to
covered devices
§ A local fitness instructor to delivery weekly, virtual physical activity
sessions
50 https://www.ResourcesForIntegratedCare.comBarriers and Solutions to Telehealth
Barrier Solution
Lack of staff familiarity with • Provided staff training and revamped the
telehealth technology training curriculum to support virtual program
delivery
Lack of participant familiarity • Implemented pre-appointment check-ins to
with technology and telehealth ensure participants have necessary
format equipment/apps and answer questions
• Set ground rules during sessions to promote
respectful engagement
• Prepare for telehealth appointments by
ensuring staff has access to necessary patient
data prior to the call
Lack of participant access to • Provide support via telephone, rather than via
computer/internet-enabled computer
technology
51 https://www.ResourcesForIntegratedCare.comBarriers and Solutions to
Telehealth (cont.)
Barrier Solution
Keeping participants engaged via • Updated the curriculum to add visuals
telehealth, particularly during group and videos and shortened the time
sessions (e.g., reducing a one-hour session to
30 minutes)
• Add virtual physical activities and
cooking demos
Replacing engagement in person through • Creation of virtual DSMES peer
virtual strategies support group
52 https://www.ResourcesForIntegratedCare.comConsumer Experience § Ms. Fontella Young § Diagnosed with Type 2 Diabetes during COVID-19 § Sorogi was able to provide education and support on the proper use of her blood glucose device § Enrolled in Sorogi’s telehealth group sessions § Working with the Sorogi team to improve her understanding of diabetes and increase weekly physical activity 53 https://www.ResourcesForIntegratedCare.com
COVID-19 Adaptations and
Lessons Learned
§ Engaging hard-to-reach populations throughout COVID-19
by:
§ Building trust
§ Meeting participants where they are
§ Addressing immediate health needs
§ Supporting the care team with tools and resources
§ Invest in the right technology and development of effective workflows
§ Collaborate with other organizations to address needs of participants
not being met by the program
§ Continued staff education and support, including updated treatment
guidelines, emerging research, and information on culturally
competent services
54 https://www.ResourcesForIntegratedCare.comCOVID-19 Adaptations and
Lessons Learned (cont.)
§ Telehealth has allowed for increased participant
engagement
§ Ability to reach participants in other wards
§ Technology supports diabetes self-management
§ Virtual peer support group was effective in addressing diabetes
distress
§ A team-based approach works well; virtual team-based care is
possible
55 https://www.ResourcesForIntegratedCare.comFuture Directions for Sorogi
§ Implement a hybrid telehealth/in-person model for delivering
DSMES and DPP
§ Evaluate the role of technology and telehealth in providing
diabetes care management
§ Address barriers to technology to support self-management
§ Share findings from survey of participants regarding barriers to
technology (e.g., WiFi) with stakeholders (including health plans and DC
Health)
§ Partner with behavioral healthcare providers to provide team-
based care
§ Explore partnerships with non-medical organizations, including
libraries and recreation centers
§ Pilot in-person peer support group
56 https://www.ResourcesForIntegratedCare.comQuestions and Answers
Vivian Cheng, Nicole Kohler MS, Katie Sheridan
PharmD, BCPS CDCES MSW, LSW
Vivian Nnacho Fontella
Ayuk, PharmD, Young,
CDCES Consumer
57 https://www.ResourcesForIntegratedCare.comThank You for Attending!
§ The video replay and slide presentation will be available at:
https://www.resourcesforintegratedcare.com
§ If you are applying for CNE or NASW CE, you must complete the post-test in
order to receive credit:
§ NASW CE: https://www.surveymonkey.com/r/DiabetesCOVIDPost
§ CNE: https://www.surveymonkey.com/r/DiabetesCOVIDPre
§ You must earn a score of 80% or higher on the post-test to receive NASW CE or
70% or higher to receive CNE. You may take the post-test multiple times.
§ If you complete the requirements to earn NASW CE or CNE, we will email you a
certificate of achievement within 6-8 weeks of today’s event.
§ Questions? Please email RIC@lewin.com
§ Follow us on Twitter at @Integrate_Care to learn about upcoming webinars
and new products!
58 https://www.ResourcesForIntegratedCare.comWebinar Evaluation Form § Your feedback is very important! Please take a moment to complete a brief evaluation on the quality of the webinar. The survey will automatically appear on the screen approximately a minute after the conclusion of the presentation. § We would also like to invite you to provide feedback on other RIC products as well as suggestions to inform the development of potential new resources: https://www.research.net/r/MVGNWVJ 59 https://www.ResourcesForIntegratedCare.com
Resources § Managing Diabetes: Medicare Coverage & Resources: https://www.medicare.gov/sites/default/files/2020-09/12091-Managing- Diabetes.pdf § Improving Communication Access For Individuals Who Are Deaf Or Hard Of Hearing: https://www.cms.gov/files/document/audio-sensory- disabilities-brochure-508c.pdf § Improving Communication Access For Individuals Who Are Blind Or Have Low Vision: https://www.cms.gov/files/document/omh-visual- sensory-disabilities-brochure-508c.pdf § American Diabetes Association, Standards of Medical Care in Diabetes – 2021: https://care.diabetesjournals.org/content/diacare/suppl/2020/12/09/44 .Supplement_1.DC1/DC_44_S1_final_copyright_stamped.pdf § Diabetes Distress Screener: https://diabetesdistress.org/ 60 https://www.ResourcesForIntegratedCare.com
Resources
§ Centers for Disease Control and Prevention Resources:
§ National Diabetes Prevention Program:
https://www.cdc.gov/diabetes/prevention/index.html
§ To find a lifestyle change program near you:
https://nccd.cdc.gov/DDT_DPRP/Programs.aspx
§ Diabetes Self-Management Education and Support Toolkit:
https://www.cdc.gov/diabetes/dsmes-toolkit/index.html
§ Empowering People with Diabetes to Access DSMES:
https://www.cdc.gov/diabetes/dsmes-toolkit/referrals-participation/empowering.html
§ How people with Diabetes Benefit from DSMES: https://www.cdc.gov/diabetes/dsmes-
toolkit/background/benefits.html
§ When DSMES is Emergency Medicine: https://www.cdc.gov/diabetes/dsmes-
toolkit/staffing-delivery/DSMES-emergency-medicine.html
§ To find a diabetes education program near you:
https://www.diabeteseducator.org/living-with-diabetes/find-an-education-program
§ A Guide for Using Telehealth Technologies in DSMES and in the National Diabetes
Prevention Program Lifestyle Change Program:
https://www.cdc.gov/diabetes/pdfs/programs/E_Telehealth_translation_product_508.pd
f
61 https://www.ResourcesForIntegratedCare.comSources [1] Medicare Payment Advisory Commission and Medicaid and CHIP Payment and Access Commission (2018). Data Book: Beneficiaries Dually Eligible for Medicare and Medicaid. Retrieved from https://www.macpac.gov/wp-content/uploads/2020/07/Data-Book-Beneficiaries- Dually-Eligible-for-Medicare-and-Medicaid-January-2018.pdf. [2] U.S. Department of Health and Human Services (HHS) Office of Minority Health (OMH) (2019). Diabetes and Hispanic Americans. Retrieved from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=63. [3] HHS OMH. (2019). Diabetes and African Americans. Retrieved from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=18. [4] HHS OMH (2019). Diabetes and American Indians/Alaska Natives. Retrieved from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=33. [5] HHS OMH (2019). Diabetes and Asian Americans. Retrieved from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=48. [6] HHS OMH (2019). Diabetes and Native Hawaiians/Pacific Islanders. Retrieved from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=78. [7] Centers for Disease Control and Prevention (2019). Prevent Complications. Retrieved from https://www.cdc.gov/diabetes/managing/problems.html. [8] Zhu et al. (2020). Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metabolism, 31(6), 1068–1077.e3. https://doi.org/10.1016/j.cmet.2020.04.021 [9] Centers for Medicare & Medicaid Services. (2021). Preliminary Medicare COVID-19 Data Snapshot. Retrieved from https://www.cms.gov/files/document/medicare-covid-19-data-snapshot-fact-sheet.pdf [10] CDC (2019). Put the Brakes on Diabetes Complications. Retrieved from https://www.cdc.gov/diabetes/library/features/prevent- complications.html [11] American Diabetes Association. Oral Medication. Retrieved from https://www.diabetes.org/healthy-living/medication-treatments/oral- medication [12] CDC (2019). Prevent Complications. Retrieved from https://www.cdc.gov/diabetes/managing/problems.html [13] National Institute of Diabetes and Digestive and Kidney Diseases (2018). The A1C Test and Diabetes. Retrieved from https://www.niddk.nih.gov/health-information/diagnostic-tests/a1c-test 62 https://www.ResourcesForIntegratedCare.com
You can also read