Connecting Chronic Kidney - Disease: the link with Diabetes Primary Care Education Workshop - ADEA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Connecting
Chronic Kidney
Disease: the link with
Diabetes
Primary Care Education Workshop
This module was conceived and developed by PEAK*
Presented by:
1
V0617
Collaborators
*This Education was conceived and
developed by the ‘Primary Care Education
Advisory Committee for KHA’ (PEAK)
KHA’s Primary Care Education program is proudly supported by
unrestricted educational grants from:
2
Learning outcomes
At the end of this workshop participants will be able to:
State the major risk factors for developing chronic kidney
disease (CKD)
Determine the stage of chronic kidney disease (CKD)
through accurate interpretation of kidney function test
results
Outline the adverse outcomes of a combined diabetes and
CKD diagnosis (Diabetic Kidney Disease, DKD)
Explore the nurse's role in early detection, reducing the
modifiable risk factors and management of DKD
Develop a system to screen at risk patients that includes
CKD testing and management
3
What is CKD?
Chronic kidney disease is defined as:
Glomerular Filtration Rate (GFR) < 60
mL/min/1.73m2 for ≥3 months with or without
evidence of kidney damage.
OR
Evidence of kidney damage (with or without
decreased GFR) for ≥3 months:
• albuminuria
• haematuria after exclusion of urological
causes
• pathological abnormalities
• anatomical abnormalities
4 Chronic Kidney Disease (CKD) Management in General Practice, 3rd edition. Kidney Health Australia:
Melbourne, 2015
A snapshot of kidney disease
in Australia
It’s harmful
In the top 10 causes
It’s common of death2. Kills more
1 in 10 adults has people each year
at least one clinical than breast cancer,
sign of kidney prostate cancer and
disease1. road deaths.
It’s manageable
If detected early and
treated properly the
decline in kidney function
can be significantly
reduced.
1 Australian Health Survey, 2013
5 2 Australian Bureau of Statistics, Causes of Death, 2012
Australians living with signs
of CKD
> 12% of
population with
signs of CKD
8-11% of
population with
signs of CKD
< 7% of
population with
signs of CKD
No data available
6
State of the Nation Report 2016, Kidney Health Australia
General chemistry results
Combine eGFR, albuminuria and
underlying diagnosis to specify CKD stage
GENERAL CHEMISTRY
Sodium 144 mmol/L (136-146)
Pot. 4.3 mmol/L (3.5-5.2)
Chlor. 106 mmol/L (98-109)
Bicarb. 26 mmol/L (20-32)
Urea 6.5 mmol (3.0-9.0)
Creat. 55 µmol/L (40-85)
eGFR 84 mL/min/1.73m2
Urate 0.35 mmol/L (0.15-0.45)
*Gluc 9.5 mmol/L (Random: 30-6.9; Fasting: 3.0-5.4)
Albumin 40 g/L (35-50)
7
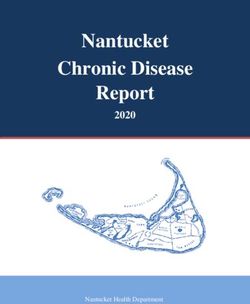
Staging CKD
Combine eGFR stage, albuminuria stage and underlying diagnosis to specify
CKD stage e.g. stage 3b CKD with microalbuminuria secondary to diabetic kidney disease
Albuminuria Stage
Normal Microalbuminuria Macroalbuminuria
GFR GFR
mL/min/1. urine ACR mg/mmol urine ACR mg/mmol urine ACR mg/mmol
Stage 73m2 Male: < 2.5 Male: 2.5-25 Male: > 25
Female: < 3.5 Female: 3.5-35 Female: > 35
1 ≥90 Not CKD unless
haematuria, structural
or pathological
2 60-89 abnormalities present
3a 45-59
3b 30-44
X
4 15-29
Connecting CKD and diabetes
Every second patient*
you see with Type 2 diabetes
WILL have CKD
A patient with diabetes has CKD if they
have 1 or more:
• Persistent microalbuminuria or proteinuria
• An eGFR < 60mL/min/1.73m2 and/or
• Haematuria after exclusion of urological
causes or structural abnormalities
9
*NEFRON Study 2007
Connecting CKD and diabetes
• Health care burden associated with DKD and DM-
ESKD in Australia is significant and expanding
• Diabetes is the leading cause of incident end-stage
kidney disease (DM-ESKD)
• The growing prevalence of T2DM in Australia,
indicates the prevalence of DKD will continue to grow
substantially
The first priority in screening for DKD should be
the detection of microalbuminuria
Pharmacological intervention in DKD is stabilising
the incidence of ESKD at the population level
10Connecting CKD and diabetes
• Monitoring for kidney disease must
be made a high priority for all people
with type 2 diabetes
• Concerted effort needs to made to
ensure that glucose control is
optimised, blood pressure and lipids
targets are met
• Opportunities for prevention across
the entire disease continuum
Sarah White and Steve Chadban, Kidney Research Node Royal Prince Alfred Hospital and Charles Perkins Centre, University of Sydney
11 AprilAn eGFR less than
60mL/min/1.73m2 indicates
• High risk of heart attack or stroke
• Decreased survival after a heart attack
• More common adverse drug reactions
• Slow wound healing
• Difficulty in achieving BP goals
• Difficult fluid control i.e. ankle swelling, fluid
retention
12
*NEFRON Study 2007An eGFR less than
60mL/min/1.73m2 indicates
Less than 1 in • Increased likelihood of
fractures with falls
every 20
• Increased likelihood of
patients with
hypoglycaemia
diabetes and
• Increased likelihood of
CKD will live hospitalisation in next 12
long enough to months
require dialysis • Increased likelihood of
or heart failure
transplantation*
13
*NEFRON Study 2007Diabetes’ affect on the body 14
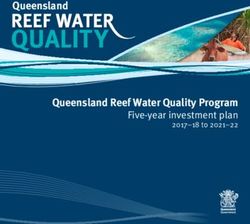
Diabetes progression to dialysis
In the last 10 years there has been a 60% increase in the
number of people with type 2 diabetes starting dialysis
New patients with ESKD due to diabetes starting on
dialysis
(Australia 1983-2014)
1200
1000
Number of patients per year
800
Type 2 Type 1
600
400
200
0
1983 1988 1993 1998 2003 2008 2013
15
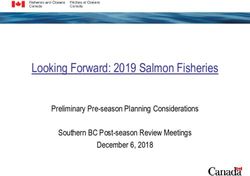
ANZDATA, Annual Reports. Available at www.anzdata.org.auDiabetes and dialysis
Diabetes is the cause of kidney failure that is
largely driving the increase in dialysis patients in
Australia
45
Diabetes Gn BP
40 Misc Uncertain PCK
35 Reflux Analg Nx
30
Rate pmp
25
20
15
10
5
0
1998 2000 2002 2004 2006 2008
16
ANZDATA RegistryDiabetic Kidney Disease (DKD)
• Diabetes causes damage to the kidneys;
called Diabetic Kidney Disease (DKD) or
diabetic nephropathy
• Worsens other complications from
diabetes such as nerve and eye damage
• Increases the risk of cardiovascular
disease
• Usually has no symptoms until it is well
advanced
17Diabetic Kidney Disease (DKD)
• most frequent cause of kidney failure
worldwide
• associated with increased morbidity and
mortality at all stages of CKD
• early detection and comprehensive
management is associated with improved
outcomes
• CKD management overlaps entirely with
diabetes management and cardiovascular
risk reduction
18Diabetic Kidney Disease (DKD)
• 20-40% of patients with Type 2 diabetes develop
nephropathy, which classically occurs in two stages:
• Early nephropathy: microalbuminuria and normal to high GFR
• Overt nephropathy: macroalbuminuria and progressive
decline in GFR
19Connecting CKD and diabetes
The presence of diabetes worsens
the outcomes in all stages of CKD:
• CVD outcomes
• Dialysis survival
• Post-transplant survival
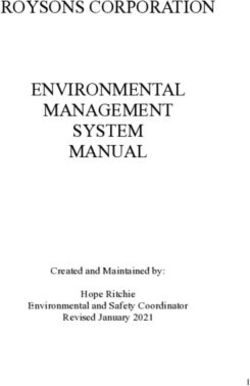
20CKD and diabetes, the connection
Diabetes multiplies the morbidity/mortality event rate in CKD
US Medicare (5% sample); Age >65, no RRT, followed 2yrs. n
=1,091,201
D- CKD- 80%
60
D+ CKD- 17%
50
Events/100 pt/yrs
D- CKD+ 2.2%
40
D+ CKD+ 1.6%
30
20
10
0
ASVD CHF RRT Death
ASVD, atherosclerotic vascular disease; CHF, chronic heart failure; RRT, renal
replacement therapy
21
Foley et al. JASN 16: 489-495, 2005Case study -
Peter
Background
• 62 years old
• Caucasian male
• Works full-time in business
management
Today
Peter presents at your general
practice with an acute cough with
yellow sputum
He has previously been seen at
your practice when he
accompanied his wife for an annual
flu vaccination
22History
1 packet per day for 40
Smoker: years
(40 pack-year history)
Alcohol: 7-10 drinks per week
Nutrition: Follows a “diabetic diet”
Type 2 diabetes, diagnosed
Medical
12 months ago after
conditions:
presenting with thirst
No regular medications,
Medications: takes occasional NSAIDS for
back pain
23Case study - Peter
Today’s visit
Test Result
Blood pressure 160/90 mmHg
Weight 102 kg
BMI 31 kg/m2
Waist circumference 110 cm
Consistent with bronchitis - no
Chest findings
clinical signs of COPD
24Case study – Question
Q1: Is Peter at increased risk of kidney
disease?
If so, why?
Today’s visit
Peter’s GP found some of his results and
history concerning. The GP has asked you
to review Peter’s case further, particularly
his potential risk for kidney disease.
25Risk factors for kidney disease
Peter has 5 of
the risk factors
Diabetes for CKD
Hypertension
• Established cardiovascular disease
• Family history of kidney failure
1 in 3
Obesity (BMI >30kg/m2) Australian
Smoker adults is at
• Aboriginal or Torres Strait Islander increased risk
origin of CKD due to
these risk
• History or acute kidney injury factors
Age over 60 years
RACGP Guidelines for preventive activities in general practice 8 th edition;
26 Chronic Kidney Disease (CKD) Management in General Practice, 3 rd edition. Kidney Health Australia: Melbourne,
2015Case study – Question
Q1a: What does Peter’s diabetes mean for his
CKD risk?
•20-40% of patients with Type 2 diabetes develop
nephropathy,
which classically* occurs in 2 stages:
Early nephropathy - microalbuminuria and
normal-high GFR
Overt nephropathy - macroalbuminuria and
progressive decline in GFR
* Recent data shows that 33% individuals with diabetes with
eGFRClassical stages of diabetic
kidney disease*
*Those with Type 2 diabetes may have overt nephropathy at presentation
GFR normal
normal
Albuminuria
0 5 10 15
Duration of Diabetes (years)
28Further reading
KinD Report 2014
www.kidney.org.au
29Case study – Question
Q1b: Peter has hypertension. What does
this mean for his CKD risk?
• Hypertension is extremely common among those
with type 2 diabetes, particularly those with DKD
• Among those with diabetes (and without), those
with hypertension are 5-8 times as likely to have
albuminuria
• Achieving BP control is one of the most effective
ways to delay the progression of kidney disease
30Hypertension
Adequate BP management delays the
progression of CKD
(reduces the GFR drop/year)
160/90mmHg
If Peter’s BP was consistently below
target, his GFR loss per year would
be reduced by 71%
31
Bakris et al., Am J Kid Disease, 2000Case study – Question
Q1c: Peter is obese. What impact does his weight
have on his risk of CKD?
• Overweight (BMI 25.1-30) and obese (BMI
>30) people are 40% and 80% more likely to
develop CKD compared to normal weight
individuals1
• Central obesity appears to be more important
than generalised
• Obesity contributes to the development of
albuminuria and proteinuria
• Obesity leads to greater difficulty in achieving
glycaemic control and BP control
32 1 Wang Y et al. Association between obesity and kidney disease: a systematic review and
meta-analysis. Kidney Int. 2008;73:19-33.Case study – Question
Q1d: How does smoking increase Peter’s risk of
CKD?
• Among individuals with diabetes, those who
smoke are more likely to get albuminuria and
among those with diabetic kidney disease,
smoking accelerates progression to failure1,2
• Even among the normal Australian population,
smoking has been associated with kidney
damage3
[1] Gambaro et al. Diabetes Nutr Metab 2001;14:337.
33 [2] Orth & Hallan. Clin J Am Soc Nephrol 2007.
[3] Briganti et al. Am J Kidney Dis 2002;40:704.Case study – Question
Q1e: Does Peter’s occasional NSAID use increase his
risk of CKD?
Probably not
• Chronic use of NSAIDs have not been proven
to lead to CKD in humans
• NSAID ingestion can aggravate underlying
kidney disease and hypertension and risk
of vascular events
• NSAIDs should be avoided in this setting
34Case study – Question
Q1f: Will Peter’s chest infection contribute
to his likelihood of CKD?
No
• Chest infection by itself has no relationship to
CKD
• Recurrent chest infections are more common
in smokers
• With his history of smoking Peter is highly
likely to develop COPD in the future
35CVD risk
Australian Absolute Cardiovascular Disease Risk
Calculator
**Peter is at increased risk of kidney disease and
therefore also at risk of having a cardiovascular event.
36 www.cvdcheck.org.auCVD risk
anyone with…
• eGFR < 45 mL/min/1.73m2 or persistent
proteinuria
• Diabetes and microalbuminuria
• Diabetes and age > 60 years
• Established cardiovascular disease
• Familial hypercholesterolemia or total cholesterol above
7.5
• Severe hypertension
– Systolic 180 mmHg or greater
– Diastolic 110 mmHg or greater
is already at the highest risk of a cardiovascular
event,
therefore the calculator should not be used
37
Guidelines for the management of Absolute cardiovascular disease risk: National Vascular Prevention Alliance.Cardiovascular risk reduction in
CKD
• CKD is one of the most potent known risk factors
for cardiovascular disease
• It is essential to clinically determine the risk of
CKD before using the Australian absolute
cardiovascular risk tool (www.cvdcheck.org.au )
to accurately calculate cardiovascular risk
• Individuals with CKD have a 2-3 fold greater risk
of cardiac death than individuals without CKD
• People with CKD are at least 20 times more
likely to die from cardiovascular disease than
survive to need dialysis or transplant
38
Chronic Kidney Disease (CKD) Management in General Practice, 3rd edition. Kidney Health Australia: Melbourne, 2015Resources
Guidelines for the assessment and management
of Absolute Cardiovascular Disease Risk
National Vascular Disease Prevention Alliance
Available at
www.cvdcheck.org.au
39Checking for kidney damage
Q2: What test results would you use as
evidence of kidney damage?
Peter is at increased risk of kidney disease and you
decide to test him for evidence of kidney damage.
? urine dipstick for blood and protein
? spot urine albumin/creatinine ratio (ACR)
? 24 hour urine protein
? serum creatinine
? eGFR
? renal ultrasound (kidney outline and size)
40Checking for kidney damage
? urine dipstick for blood and protein
spot urine albumin/creatinine ratio
(ACR)
? 24 hour urine protein
serum creatinine
eGFR
? renal ultrasound (kidney outline and size)
41Urine albumin /creatinine ratio
(ACR)
• The preferred urine test in all diabetics is to look for microalbuminuria
• This is best tested by a urine albumin:creatinine ratio (ACR)
• Preferably 1st morning void but a random sample can also be used
ACR result Test results range Recommended follow -up
Females 25
(to quantify protein excretion)
mg/mmol
42
NHMRC Guidelines 2009Glomerular filtration rate
• Glomerular filtration rate (GFR) best measure of
kidney function
• Can be estimated (eGFR) from serum creatinine
• eGFR automatically provided by pathology
laboratories when a creatinine is ordered (for adults
over 18 yrs)
• Reported as an actual numerical value or >
90mL/min/1.73m2
• eGFR is accurate at values 60 mL/min/1.73m2
• Creatinine alone will commonly under-estimate the
degree of reduction in kidney function, particularly in
small elderly women
Australasian Proteinuria Consensus Group, 2012
43
Chudleigh et al, Diabetes Care 2007;30:300-5.Comparing creatinine and
eGFR
Serum creatinine
CKD 1 & 2
CKD 3b CKD 3a
CKD 4
CKD 5
0 30 60 90 120
GFR mL/min
Dialysis Albuminuria
Normal Serum Creatinine level
44
Actual Serum Creatinine levelScreening for CKD
Indications for Recommended 1 in 3
Frequency
assessment* assessments Australia
Diabetes
n adults
Urine ACR, eGFR, blood is at
Hypertension
pressure increased
Established cardiovascular
disease** risk of
Family history of kidney If urine ACR positive repeat twice CKD due
Every 1-2
failure over 3 months (preferably first
morning void) years†
to these
Obesity (BMI ≥30 kg/m2) risk
If eGFR < 60mL/min/1.73m2
Smoker repeat within factors
Aboriginal or Torres Strait 7 days
Islander origin aged ≥ 30
years‡
History of acute kidney injury See recommendations in booklet
*Whilst being aged 60 years of age or over is considered to be a risk factor for CKD, in the absence of other risk factors it
is not necessary to routinely assess these individuals for kidney disease.
**Established cardiovascular disease is defined as a previous diagnosis of coronary heart disease, cerebrovascular disease
or peripheral vascular disease.
† Annually for individuals with diabetes or hypertension.
‡ Refer to booklet for more details regarding recommendations for testing in Aboriginal and Torres Strait Islander peoples.
45 Chronic Kidney Disease (CKD) Management in General Practice, 3rd edition. Kidney Health Australia: Melbourne,
2015Kidney Health Check
Kidney Health Check
Blood Test Urine Test BP Check
Albumin /
eGFR Creatinine Ratio Blood pressure
maintain
calculated from (ACR) consistently below
serum creatinine check for BP goal
albuminuria
CKD screening should be undertaken as a part of every
chronic disease & cardiovascular risk assessment
46 Chronic Kidney Disease (CKD) Management in General Practice, 3rd edition. Kidney Health Australia:
Melbourne, 2015Case study - Peter
You identify Peter as being at increased risk for CKD
and request he be recalled for further tests.
Peter's test results show the following:
Test Result
Creatinine 135 µmol/L
eGFR 46 mL/min/1.73m2
Urine ACR 44 mg/mmol (macroalbuminuria)
HbA1c 9.6% / 81 mmol/mol
Blood pressure 160/90 mmHg
47Case study - Peter
Q3: What can be done to improve Peter’s
control of his diabetes?
Good glycaemic control slows progression
of kidney failure*
• Prescribe exercise and diet
• 44% of patients are on a sulphonylurea
• Metformin okay to use in reduced doses when eGFR
is between 30 and 60 mL/min - avoid use if GFR
below 30 mL/min, due to risk of acidosis
• Consider referral to endocrinologist and diabetes
education centre
See Diabetes Australia website for
guidelines: www.diabetes.com.au
48
*UKPDS. Lancet 1998;352:837-53Drug therapy recommendations
for non-insulin hypoglycaemic drug therapy for
patients with stages 3b – 5 CKD
CLASS CKD Complications
Reduce dose
Biguanide (Metformin) Contraindicated GFR Lactic acidosisDrug class target sites
Pancreas
Liver -cell dysfunction
Hepatic glucose
overproduction
Sulphonylureas
Meglitinides Muscle and fat
GLP-1 analogs Insulin resistance
Biguanide DPP 4 inhibitors
TZDs
↓Glucose level
Kidney
Renal glucose Biguanides
TZDs
transport
SGLT2
Inhibitors -Glucosidase inhibitors
Gut
50 Glucose absorptionCase study – Peter
Q4: What can be implemented to reduce Peter’s
blood pressure?
a) Lifestyle modification?
b) Medications? ACE-inhibitor, ARB or
other drugs? Other?
c) Do more tests?
d) Refer on to an endocrinologist,
nephrologist?
51Hypertension in diabetes
Lifestyle approaches are the first
consideration in all people with diabetes
and high blood pressure - the key
elements are:
SNAP - smoking, nutrition, alcohol, physical activity
• Stop smoking
• A low salt diet
• A reduction in his alcohol intake
• An exercise program
• A low calorie diet to reduce his BMI
52
For more details General Practice Management of Type 2 diabetes 2014/15Lifestyle effects on BP
Modification Recommendation
Weight 4.4mmHg (for 5.1kg
BMI 18-24.9 kg/m2
reduction weight lost)
Dietary Reduce dietary sodium intake 4-7mmHg (for
sodium to no more than 2.4g sodium reduction by 6g in
restriction (or 6g salt) daily salt intake)
5.5-11.4mmHg (5.5
Fruit, vegies, low saturated for normotensives
DASH diet
and total fat 11.4 for
hypertensives)
Physical Aerobic activity for 30-
5mmHg
activity 60mins/day, 3-5 days/week
Moderate 3mmHg (for 67%
No more than 2 drinks per
alcohol reduction from
day (men) or 1 drink per day
consumption (women) baseline of 3-6
only drinks per day)
53 Tiberio MFrisoli et al Beyond salt; lifestyle modifications and blood pressure: European Heart Journal (2011) 32,
3081–3087 doi:10.1093/eurheartj/ehr379Hypertension in Diabetes
Medications may be needed to
lower blood pressure to target
levels
• The preferred anti-hypertensive
agents in diabetes are an ACE-
inhibitor or ARB
• These agents may also slow
progression of CKD
• Any other anti-hypertensive
agent that lowers blood pressure
will improve the patient’s disease
54
progressionCase study - Peter
Peter has stage 3b CKD with macroalbuminuria and
diabetes, so at high risk of a CVD event automatically
and his blood pressure should be maintained
consistently below 130/80mmHg
Flag with his GP to consider:
• Starting a clinical action plan
• Lifestyle modification
• Pharmacotherapy to treat his hypertension
• Monitor 6-12 weekly until sufficient
improvement
Maintain BP consistently
People with....
BELOW (mmHg)
AlbuminuriaOrange Clinical Action Plan
eGFR 30-59 mL/min/1.73m2 with microalbuminuria
OR eGFR 30-44 mL/min/1.73m2 with
normoalbuminuria
Goals of management
• Investigations to determine underlying cause
• Reduce progression of kidney disease
• Assessment of Absolute Cardiovascular Risk
• Avoidance of nephrotoxic medications or volume
depletion
• Early detection and management of complications
• Adjustment of medication doses to levels appropriate
for kidney function
• Appropriate referral to a nephrologist when indicated
56
Chronic Kidney Disease (CKD) Management in General Practice, 3rd edition. Kidney Health Australia: Melbourne, 2015Orange Clinical Action Plan
Frequency of
3 to 6 months
monitoring
Clinical Blood pressure
assessment Weight
Urine ACR
eGFR
Biochemical profile including urea, creatinine,
electrolytes
HbA1c (for people with diabetes)
Laboratory Fasting lipids
assessment Full blood count
Calcium and phosphate
Parathyroid hormone (6-12 monthly if eGFROrange Clinical Action Plan
eGFR 30-59 mL/min/1.73m2 with
microalbuminuria OR eGFR 30-44
mL/min/1.73m2 with normoalbuminuria
It is also important to consider…
• Absolute Cardiovascular Risk Assessment
(www.cvdcheck.org.au)
• Lifestyle modification
• Blood pressure reduction
• Lipid lowering treatments
• Glycaemic control
58 Chronic Kidney Disease (CKD) Management in General Practice, 3rd edition. Kidney Health Australia:
Melbourne, 2015Screening and assessments
Screening - search* for patients at risk and invite patients for a
health check
Health Assessments (Items 701, 703, 705, 707, 715)
Screen those at risk Assessments Health Checks
A type 2 diabetes risk
Diabetes 701 evaluation for people aged
Family history of kidney 40-49 years (inclusive) with a
703 high risk of developing type
failure
2 diabetes as determined by
Established CVD 705 the Australian Type 2
Diabetes Risk Assessment
High blood pressure 707 Tool – once every 3 years to
eligible patients
Obese (BMI >30kg/m2 715 A health assessment for
people aged 45-49 years
Smoker (inclusive) who are at risk of
developing chronic disease –
Aboriginal or Torres Strait once only to an eligible
Islander origin patient
For more information visit www.mbsonline.gov.au
*Use data management tools such as ‘PEN CAT’ to help find patients at risk
59Annual diabetes cycle of care
Item 2517
At least once every 12
Twice every 12 months Every 12 months Once every 2 years
months
Comprehensive eye
Weight Total Cholesterol Self Care education
examination
Height Triglycerides Diet
BMI HDL-C Physical activity
BP HbA1c Smoking evaluation
Feet examination Microalbuminuria Medication Review
eGFR
For more information visit www.mbsonline.gov.au
60
Diabetes Management in General Practice 14/15Chronic disease management
Medicare Australia has provided remuneration for
chronic disease management by the following item
numbers:
GP Management Plan Other Items
Items 721, 729 & 732 Items 723, 10997, 10986
For patient and GP management of chronic Item 715 for Aboriginal and Torres Strait
disease Islander Health Assessments
Incorporates patients goals, needs, Involves collaboration with other health
achievements and references to resources professionals in patient care
Electronic templates for specific conditions
are available
CKD template available at
www.kidney.org.au/health-professionals
61Monitoring and support
Item 10997 / 10986
For provision of monitoring and support to people with a chronic disease by a
practice nurse or registered Aboriginal Health Worker, on behalf of a GP.
Available for people who have a GPMP / TCA at a maximum of 5 services can be
claimed per patient per calendar year. With 15 services available to Aboriginal
or Torres Strait Islanders with a Health Assessment.
The item may be used to provide:
• Checks on clinical progress - eGFRs, ACR, BP
• Monitoring medication compliance - BP medication(s)
• Self management advice - personal goals
• Collection of information to support GP reviews of care
plans
For more information visit www.mbsonline.gov.au
62Resources
CKD patient fact sheets
Available along with more kidney health fact
sheets at www.kidney.org.au
63Case study – Peter
Q5: Who could you involve in Peter’s
management through a Team Care
Arrangement?
64Multidisciplinary Care Team
May include, but is not limited to:
Community Health
Exercise Family Members / -weight and diet
Dietitian Nephrologist
Physiologist carers programs specific
to local community
Optometrist/
Endocrinologist Diabetes Specialist Renal Nurse Nurse Practitioner
Ophthalmologist
Vascular/
Pharmacist Podiatrist Social Worker Cardiologist
Transplant Surgeon
*N.B not all listed here are eligible for TCA inclusion.
65Peter's management
Q6: What will you review at Peter’s next visit
and when?
The recommended period for a GPMP review
is every 3-6 months.
66Management reviews
History Examination Investigation Review
SNAP Weight HbA1c Goals
Patient’s record of
Waist circ. Intercurrent illnesses
home testing
Foot symptoms Height
BP
67
Diabetes Management in General Practice 14/15Nurse role in CKD
Reduce the impact of CKD
Screen for risks Manage disease Monitor patient progress
Using care plans and item
Using Kidney Health Check Using item numbers
numbers
Diabetes Promote self management Adherence to treatment
Hypertension Diabetes Nephrotoxic medications
Cardiovascular using
Absolute CVD Risk Hypertension
Calculator*
CKD
Other CKD risk factors
Using health checks & item Symptoms
numbers
*Refer to slide 36
68Summary
Optimal management of DKD
• Everyone with diabetes should have a kidney health
check every year
• Targets of therapy and management change in those
with DKD e.g. blood pressure, glycaemia etc.
• Major role for practice nurse in coordinating a
multidisciplinary approach
• Kidney disease is an integral part of chronic disease
management
• Overlap with diabetes management and CVD risk
reduction
• Encourage self management
Potential to halve the number of
69 patients presenting with kidney failureResources
CKD management in General Practice
2015 guidelines handbook
Available www.kidney.org.au/
at health-professionals
70Resources
Rated a
CKD-GO! Phone App ‘must have’ App
by Medical
Observer
Available on
iTunes and Google
Play app stores
All the best bits of the
‘CKD Management in
General Practice’ handbook
now in a handy app!
71Resources
My Kidneys, My Health Handbook & App
Free resource for patients newly diagnosed with early
stage CKD
App available on
iTunes and Google
Play app stores
Hardcopy books available
to order visit
72 www.kidney.org.auFactsheet
Urinary tract infections
Resources How to look after your kidneys
Healthshare fact sheets
Kidney Health Check up
GP only – Chronic Kidney Disease
Chronic Kidney Disease fact sheets All about Chronic Kidney Disease
for patients. Available for Medical Looking after yourself with CKD
Director and Best Practice software Kidney stones
Kidney transplant
Peritoneal dialysis
Consent and kidney tests
Kidney health tests
Kidney cysts
Access for dialysis
Kidney cancer
Treating kidney disease
Homes haemodialysis
Haemodialysis
Life with a single kidney
All about GFR
73Resources
Kidney Health Information Service
Free call information service for people living with /
affected by kidney disease
Kidney Community…
Members receive a monthly newsletter from KHA allowing you to access:
• Information and invitations to KHA's education and support activities
• Updates on medical research in kidney disease
• Information on advocacy opportunities and government relations issues
• Information on community and corporate events held by Kidney Health Australia
To join the kidney community, email
community@kidney.org.au
74Thankyou for
participating in this
workshop
Please complete your
evaluation form before
leaving.
75You can also read