Collaborating for the future: creating a new long-term strategic framework for health and social care workforce planning - Health ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Collaborating for the future:
creating a new long-term strategic
framework for health and social care
workforce planning
Welcome - why now and what are we aiming to achieve? Sir David Behan: Chair, Health Education England Oonagh Smyth: Chief Executive Officer, Skills for Care Dr Navina Evans: Chief Executive Officer, Health Education England
The second of three deliberative events 1 November 2021 9 December 2021 10 February 2022

FORECASTING FORESIGHT
Focus on a range of potential futures
Focus on expected future
Searching for signs of potential future
Identifying a future which is an
disruptions at the margins of the
extension of the present
current system (“weak signals”)
Estimates what will happen, Expands our thinking about what is
assuming that past trends will possible, helps us determine how we
continue to be solid indicators choose to prepare for and shape the
of future happenings future
Activity Format
1000 Welcome to the second deliberative event and our mission for this session: What we learnt from event one and from other forums, what we need to Plenary
achieve in event two, moving into event three and the final report – Sir David Behan, Oonagh Smyth and Navina Evans.
1020 How deliberative event two will work (including Menti polls). Plenary
1025 Our collective ambition for 2036: What we have concluded from deliberative event 1 and our other discussion forums. Plenary
Breakout 1: Re -familiarising ourselves with the collective ambitions and welcoming any new members of our foresight group Foresight
1035 • Does the collective ambition resonate? group
• Is there anything missing or shouldn’t be there?
1050 'The counterfactual’: What demand and supply might look like in 2036 if we do nothing different – Rob Smith. Plenary
1105 Tee up breakout 2: Three paradigms for thinking about service models that have radically different implications for our future workforce. Plenary
Breakout 2: Delivering our collective ambition and balancing the service model paradigms
1115 Recognising that the 3 paradigms are not either/or: Mixed
• How could services look in the future driven by some combination of these paradigms? group
• What are advantages and disadvantages of each paradigm and how might they work together?
1155 30-minute break
1225 Tee up breakout 3: Insights from other systems and contexts. Plenary
Breakout 3: Delivering our collective ambitions and the impact on the shape of the future workforce
1235 • What are the opportunities and implications of future service models, based on different paradigms, in how we develop our workforce? Mixed
• Looking backward and learning from the past, what barriers might we need to overcome to develop this future workforce? group
• What strengths and assets can we build on to create this future?
1320 10-minute break
1330 Review of outputs from breakouts 2 and 3. Plenary
Breakout 4: Delivering the future workforce: working from the future backwards
• What do we need to start doing NOW to deliver the future workforce?
• How do we define “workforce”?
1340 • Who do we need to recruit to do what? Foresight
• How should the workforce be trained, employed and organized? Group
• What are the potential implications for regulation and registration?
• What environmental factors - culture, OD and CPD and other support is needed for workforce to be successful and retained beyond recruitment?
• What key questions must we address in deliberative event 3?
1430 Review of outputs from breakout 4. Plenary
1440 Reflections on today’s second deliberative event and our next steps towards deliberative event 3 (10 February) – Sir David Behan. Plenary
1455 Feedback questions via Menti
1500 Close Plenary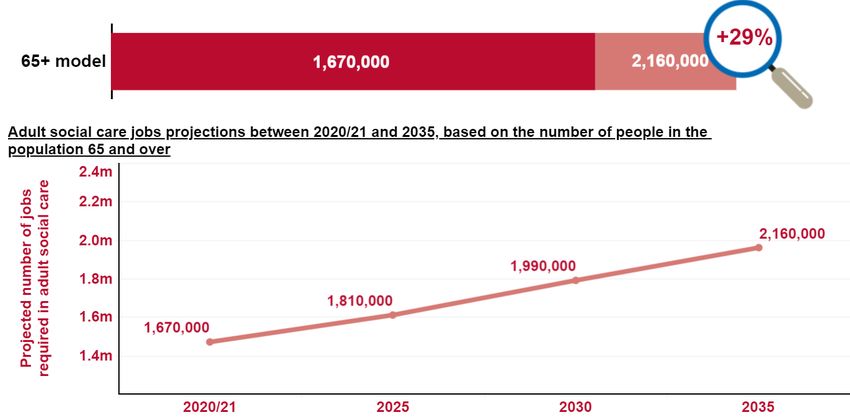
• Everyone has a voice
• The deliberative events are safe
and supportive spaces
• Contribute openly (comments
will not be attributed)
• Take collective responsibility
• Focus on strengths and
solutions
• Be kind
• Social media after today’s event
Convenors and facilitators have the licence to undertake
refreshment breaks for their breakout groups whenever they feel
it necessary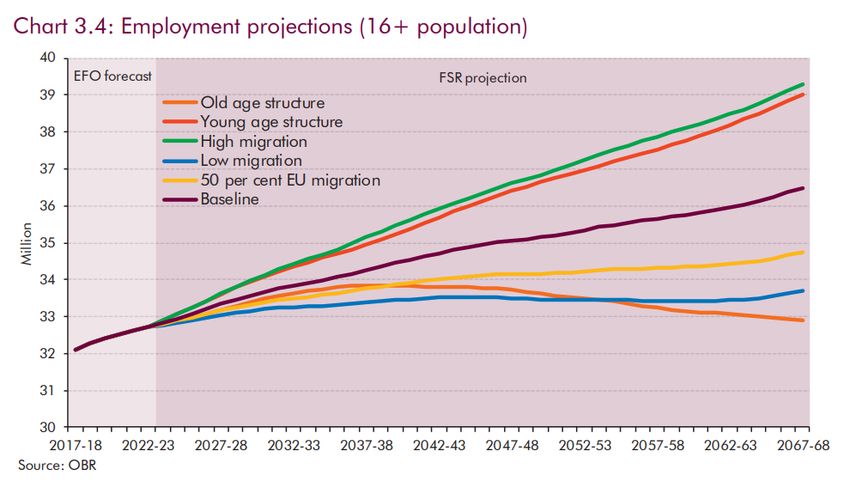
After the next input Kathryn Perera from the insight group is going to update us now on emerging ambitions for 2036 and insights from the process so far At the end of this, we will be moving into our foresight groups to reflect on the two questions: 1. Does the collective ambition resonate? 2. Is there anything missing or shouldn’t be there?
Deliberative Event 2 Our ambitions for 2036 Insights from the process so far
9
We are following a deliberate methodology to get to
the outcomes we seek by the end of this process
It resembles a funnel
RISK
APPETITE
Past trends; future
FORECASTING certainties, e.g.
demographics ENVISIONED
PROVISIONAL SELECTED
SYNTHESIS LHS FUTURE
CERTAINTIES SCENARIO(S)
GOAL
Imagined scenarios and
FORESIGHT influences
A Learning Health System
Amended forecasts approach mitigates choice
with consensus risk by allowing en route
certainties adjustment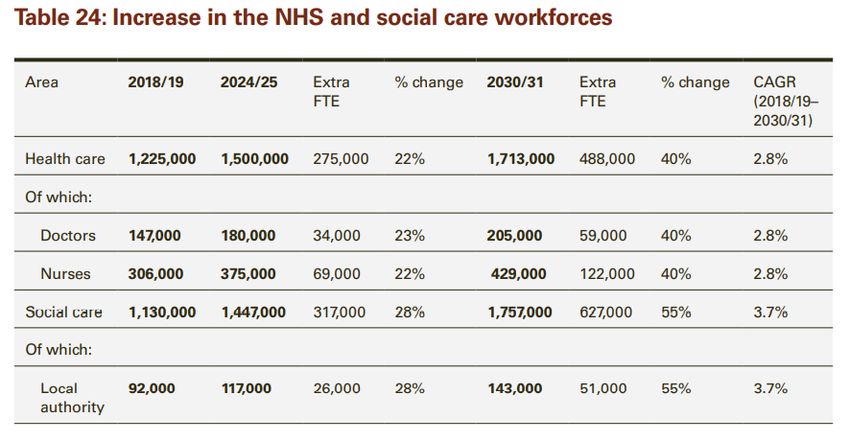
…which involves a whole series of actions: call for evidence, deliberative
events, roundtables, boards, research and crowdsourcing
Social Care
External Crowd
C O M P L E X I T Y
Call for Engagement Challenge sourcing
Evidence Workshops ICS/Regional
Knowledge, Survey (SfC) People
Boards Further
Call for Roundtables
Experience ICS/Regional Evidence
People Analysis
Evidence Boards
Starting Final
Analyst Review Event 1 Event 2 Event 3 Report
Thoughts Proposition
of Evidence
Concepts
Thought Future
Assumptions Patient/People
Leader
who need care
We
Round
Table and support are
Roundtable
here!
Further Research
August September October November December Jan 2022 Feb March AprilThe 290 responses to our Call for Evidence set out 15-year
ambitions for patients, people who need care & support and
the population:
Values-driven health and social care system
• Holistic and equitable
• Patient empowering, prevention focused
Processes in pursuit of values
• Health and care integration
• Primary and secondary integration
Enablers
• Health and social care parity
• Increased number of staff
• Flexibility for accessing care
analysed by Grant ThorntonThe 290 responses to our Call for Evidence set out 15-year
ambitions for our workforce including students and trainees:
Values that permeate the system apply to workforce
• Parity of esteem
• Sensitive to the needs of the individual
Processes in pursuit of values
• Equipped to play a part in integrated care
• Integration of health and care at workforce level
• Adequate number of ‘generalists’
• Ability to deploy across sectors and institutional boundaries
Enablers
• Increased numbers of well trained and remunerated staff
• Upskilling primary care to respond to demands and shift of care to
community
• ‘Transdisciplinary’ training
• ‘Line of sight’ on career pathways that also provide flexibilityAt the first deliberative event, 220 participants reviewed the evidence and described ambitions for people using health and social care services in 2036 Four big themes emerged: • A closer alignment between technology infrastructure and the patient pathways. • A greater focus on preventative support and a move towards proactive rather than reactive interventions. • Enhanced coordination of care and having someone who “holds the ring” on the mental/physical healthcare wrap around. Viewing needs holistically, taking into account family and wider community. • A strong theme around social and scientific personalisation and integration - and how this might be facilitated in the future by changes to pathways and advances in new treatments and genomics.
Participants stressed the need for different thinking about the future
We need a different mindset or
“paradigm” about the futureThese ambitions have been reinforced and enriched by several roundtable events ‘Round table’ conversations were held with: • An ‘advice and challenge expert group’, bringing together thought leaders in workforce from other sectors, generations and countries with extensive international experience • A Social Care thought leaders roundtable • An NHS thought leaders roundtable (with plans to bring together in the NY) • The Social Partnership Forum • The NHS Youth Forum • A specially convened roundtable with patients and people who need care and support, drawing on a range of expertise, diverse backgrounds and lived experiences • Future roundtables and “deep dives” are planned with science and technology and industry In all the conversations, participants encouraged us to think more radically about our future ambitions, and the different approach that might be needed to get there….
Feedback from the roundtable for people who need care and support
‘What do you hope the health and social care system will have achieved for patients/ people who need care
and support and the population served by 2036?’
Services that fit round A system that is proactive rather We also hope that those designing the system will have
people and not the other than reactive. Always available developed a greater understanding of the roles that services
way round. That enable and options outside of clinical or regulated care can play.
and flexible.
and support a
meaningful life.
A decent care package for families of children with complex
disabilities. Virtually every family I know is on their knees trying
Reasonable workload for doctors, nurses, therapy to get care & support. Disabled children are forgotten in this
staff. Good colleagues are leaving at a rate I have conversation & their families too exhausted to speak up.
never seen. I share every 'recipients' frustrations
with the system but adding more policy / work /
expectations on pressurised staff wont work We all want to live in the place we call home with the
people and things that we love, in communities
where we look out for one another, doing things that
matter to us. That’s the future we seek.
We need to tell a better story: People
Pathway for patients that they
assume care work happens primarily in
know what to do, what to expect
institutions, not homes. - Just as people
and what that standard should be We hope the system will have made the sorts
associate care work with healthcare, their
on a national level. Services of holistic, community-based care options
first assumption is that care work occurs
designed for people by people. much more prominent and raised awareness
in institutions, in particular hospitals .
of them amongst people who deliver services
and those who could receive them.NHS Youth Forum (aged 14 - 24 including both users and trainees)
…What key message would you like us to take away and hold in our hearts and
minds as we take this work forward?
XXXX’s (great) point about the
necessity to ensure there is a bright
-more staff
Community, personalised care is the way "beacon of hope" within an NHS
-better training (flexibility)
forward as it will help reduce pressure career that would cut through the
-better working conditions and staff
on primary and secondary services. negativity / downsides and
benefits
encourage more young people to
-better work/life balance
consider a career pathway....What
-better idea sharing between CCGs
would the beacon be?
Changing the idea of children (some have really great ideas)
and young people being grouped -more info on the how the system
into one. Making sure that young works (esp for patients from Make the career more appealing.
people are considered from the abroad) Why should someone go into
ages of 18-25 and children are healthcare and pay £500/mo to
below 18 park at work when they can go
into tech with less years of
Trans healthcare needs to become a education and get catered
bigger focus within the NHS in the lunches every day?
future and be made more accessible
We need to remove the stigma overall. Healthcare settings also need
surrounding mental health illnesses to be made safer and more inclusive for Promote NHS as a
and instead provide support. LGBTQ+ people. career for all kinds of
people, from all
backgroundsConclusion
The big message from the call for evidence was
We have big ambitions for the health and
social care system but we need more of the
same to get us there
Our perspective is shifting through the first deliberative event and the roundtables
We need new and different thinking. We
have to change our paradigm about what
care and support is, how it is delivered and
who delivers it in future
Paradigm: A set of assumptions, concepts, values, and
practices that constitutes a way of viewing reality for the
community that shares themIN YOUR FORESIGHT GROUP Breakout one: reflecting on the collective ambition in our foresight groups 1. Does the collective ambition resonate? 2. Is there anything missing or shouldn’t be there?
Getting into your foresight group breakout room Three ways to join your foresight group breakout group: 1. Everyone should have received a foresight group list which encompasses your foresight group’s members and the link to your foresight group. Click on the link attached to the list, for example it will look like this: Click here for Foresight Group 8 2. The link for each foresight group (and associated participants) will also be posted to the meeting chat box. Click on the link for your foresight group in the chat box. Please be patient it will take time to post 25 links into the chat box. 3. After step 2 above has been completed and you do not know which foresight group you have been allocated to, simply pick a group to join and click the link – you will be welcome!! Notes: • When you reach a breakout room, please be a little patient, it can take a minute or two for others to join • If your convenor or facilitator hasn’t arrived, please start the conversation anyway • if you cannot get into a foresight group even after clicking on a link, stay in the main meeting room and one of the tech team will look to help you
Future workforce – counterfactual scenarios Rob Smith Strategic Framework – Deliberative event 2
Future workforce scenarios – a health (and care) warning
• RISK - A focus on workforce numbers may constrain thinking and
move us from foresight to forecast
• A ‘strawman’ scenario → counterfactual that allows us to compare to
our imagined changes
• Existing work in the public domain
• A rational framework – ensure all levers are considered and
assumptions understood
• Purpose of diagnostic models is to drive action – scenarios should
not come true!Demand Perspectives • Demographic drivers • Income effects • Other cost pressures (including differential productivity and effect of technology)
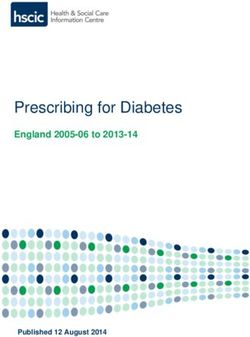
Skills for Care: future demand projection
• A 15 year
projection
• Population growth
only
• 490,000 additional
jobs by 2035
• 1.9% demand
growth per
annum
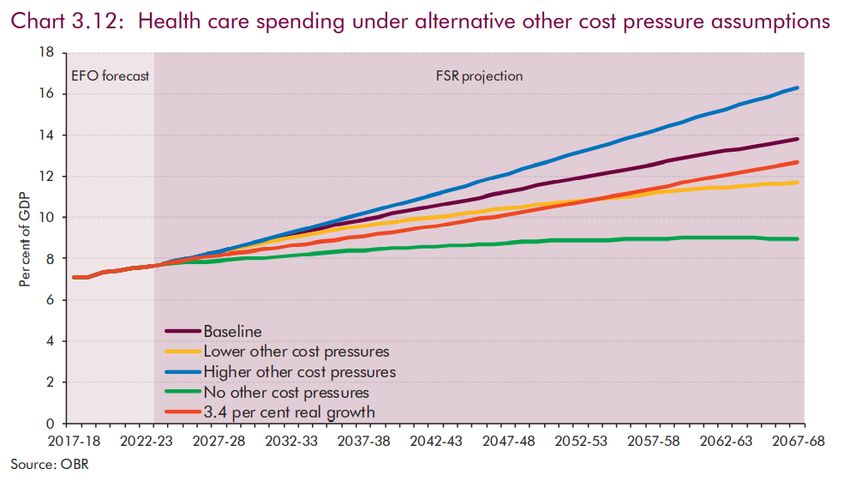
The size and structure of the adult social care sector and workforce in England (skillsforcare.org.uk)Office for Budget Responsibility (OBR) – Health care spending
• A 50 year projection exercise
• Biannual Fiscal Sustainability
Report
• Particular focus on health and
care as largest variable in
public spending assumptions
• Expressed as a % of GDP
• Growth on top of anticipated
GDP increases
• Baseline projection = approx.
3.5% real terms increase per
annum
• ‘No other cost pressures’
(demography only) = approx.
Fiscal sustainability report - July 2018 - Office for Budget Responsibility (obr.uk)
2.4% per annum
• NOT a forecast – diagnosis to
highlight government choices
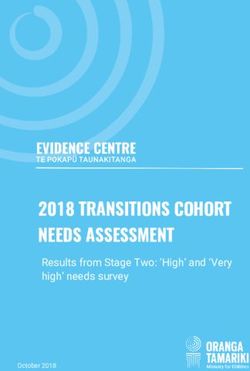
to maintain fiscal sustainability.Historic trend on UK health spending
• Highly variable in
shorter term even
on 5 year rolling
average
• Long term
average 3.7%
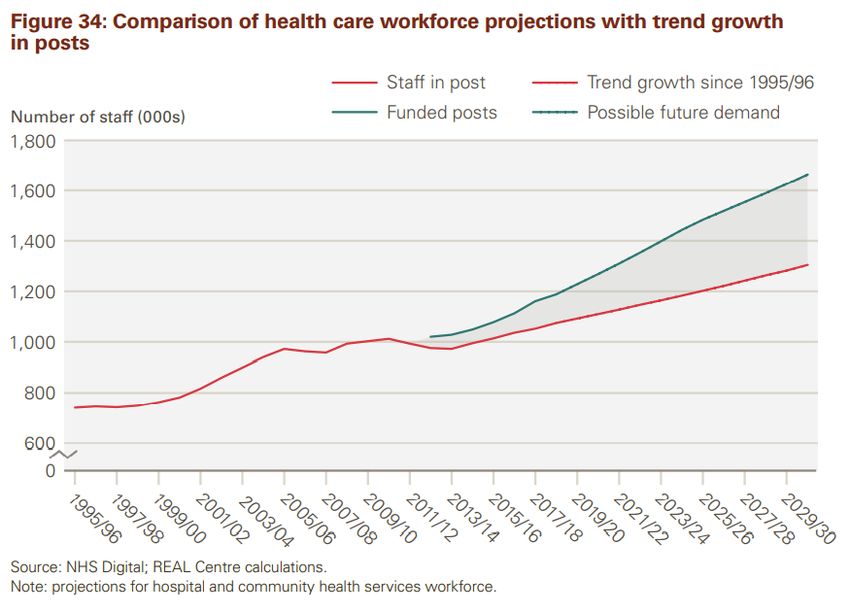
per annumFacing the facts: Shaping the future – an OBR based projection 2017
• A 10 year future
scenario, for NHS
• 4 year under SR2015
• 6 years beyond
• Period from 2021
based on OBR
(FSR2015)
• 190,000 health posts
• 2.7% annual
increase in demand
• 72,000 additional
supply
• 1.3% annual
increase in supply
Facing the Facts, Shaping the Future – a draft health and care workforce strategy for England to 2027.pdf (hee.nhs.uk) (with no additional
actions)Health Foundation REAL centre
– Health and Social Care Funding Projections 2021 • A 10 year future scenario, for
health and care
• 488,000 health posts
• 2.8% annual increase (health)
• 627,000 social care posts
• 3.7% annual increase (social
care)
REALCentreFundingProjections_WEB.pdf
Rocks S, Boccarini G, Charlesworth A, Idriss O, McConkey R, Rachet-Jacquet L. Health and social care funding projections 2021. The Health
Foundation; 2021 (https://doi.org/10.37829/HF-2021-RC18).Supply Perspectives • Domestic supply (including from education for vocational roles) • International migration • Long term joiner / leaver rates
Trends in the health and care workforce
EMP13: Employment by industry - Office for National Statistics (ons.gov.uk) • A 43 year time series
• 2.0% annual growth (health and care)
• 1978 1:14 work in health and care
• 2021 1:7 work in health and careVery long-term NHS supply growth – selected professions
• 450% over 70 years
• 2.2% per annum increaseA finite (domestic) labour market
Are there absolute limits to the number of people who could work in health and care?
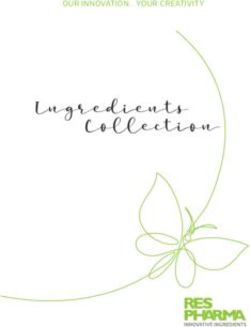
Total ‘working age’ population Proportion by industrySummary of Demand and Supply trends and projections
Service Workforce Workforce
Projection / historic time series Sector Period Funding Demand Supply
• Social care workforce
Historic Trends demand between 2%
ONS Jobs Health & Care 1978-2021 2.0%
ONS Jobs & public expenditure Health 1978-2021 3.7% 2.1%
and 4%
ONS Jobs Social Care 1978-2021 1.7% • Trend supply 1.7%
Topol review - various sources NHS (selected) 1949 to 2021 2.2%
• Health care workforce
Projections
demand between 2%
OBR - principle projection Health 2017 to 2067 3.5%
OBR - demography only Health 2017 to 2067 2.4% and 3% depending on
assumptions (but higher
Skills for Care - demography only Social Care 2020 to 2035 1.9% trend spend)
• Trend supply 2.1%
HEE - Facing the facts (per OBR2015) NHS (HCHS) 2021 to 2027 2.7% 1.3%
What might happen if we
Health Foundation REAL centre Adult Social Care 2019 to 2031 4.3%/5.8% 3.7%
NHS (HCHS) 2018 to 2031 3.1%/3.5% 2.8%
do nothing different……
HEE flow tool NHS (HCHS) 2021 to 2031 1.7%Demand for what?
The future system goals and associated service model
• Counterfactuals extrapolate the current model +/- marginal changes – This is a
MAJOR limitation
• Does a new model mean less of the current (or less extra) or is it in addition
to?
• What are the supply requirements of the new model? What scale? What make
up? And does this open opportunities about supply source?
• Modelling for ‘foresight’ would need a new approach.A new paradigm for health and social care
What we heard through all of these events, conversations and literature reviews is that
people don’t just want ‘faster horses’ (more of the same), they want a completely
different approach to health and social care, both for those who provide the care and
those who receive it (indeed, challenging the current boundaries between the two).
The traditional approach to workforce planning is unlikely to deliver this, because it
is based upon ‘forecasting’ based upon historic trends.
Just as Henry Ford moved from ‘faster horses’ to cars, or the leap from the landline, to
mobiles, to iPhones, we need to acknowledge and challenge the current paradigm
within which we think about health and social care and the workforce required to
deliver it.
Paradigm: A set of assumptions, concepts,
values, and practices that constitutes a way of
viewing reality for the community that shares themThree paradigms for thinking about health & social care
not mutually exclusive, but thinking about where the centre of gravity
is/might be And their journey to
sustain a healthy life
Network
“Relational” needs:
Met by addressing the unique needs of an individual as a
member of a wider family/community, with holistic support,
and asset-based approach
Examples: Lucy (eating disorder) Antonio (looked after care)
and Brenda (complex community care)
Pathway
“Process” needs:
Met by going through a process or pathway of care
Example: a standardised care pathway for someone
undergoing a hip replacement or Charlotte (on a
breast cancer treatment pathway)
Two of the service paradigms can fit within the overarching third:
They aren’t separate
Source: based on a paradigm model by Steve Schefer: https://squiretothegiants.com/2021/12/03/part-1-autonomy-autonomy-support-autonomy-enabling/Paradigms influence how we frame both the problem and the workforce response
(but of course, they overlap in reality)
Network
Winsome, 35 years old
‘Repair Winsome is the mother of two daughters, 7 and 4 She is an active Problem typically framed as:
mother who considered herself healthy before her diagnosis. She
shop’ exercises regularly though perhaps enjoyed more units of alcohol a
What about the children?
week then recommended, exacerbated by an increase in her intake How can we support the family and
Problem typically framed as: over lockdown. prevent MH and other problems? What
How can we diagnose earlier? Her breast cancer was diagnosed at stage 2 despite limited matters to Winsome, and what support
Treat faster with better health symptoms thanks to a blood test as part of a national trial screening can the wider
outcomes for Winsome? programme. When she initially presents to her GP she is offered family/community/health/social care
rapid diagnostic testing which has recently been introduced locally. system provide not just when she is
Genomics creating more
She is offered genomic testing and genetic counseling as it appears
possibility for there might be a genetic component to her cancer. She is very
acutely ill, but for recovery, prevent
predictive/preventative worried about how her cancer diagnosis might impact her children recurrence & if she & her family needs it,
approach, but within a care She did not have to have a mastectomy due to receiving advanced high quality palliative care?
system based on ‘reacting’ precision radiotherapy
Response typically focused on building
Response typically focused on Pathway capacity in informal and formal
how many more ‘workforce’, with science/ technology as
professions/skills we need in Problem typically framed as: how can we improve the an enabler in the network, (if supported
the formal workforce & how pathway of care for people, from prevention, diagnosis, to be digital and data literate) not just an
can science/technology treatment and rehab or palliative care? accelerant in the hospital, to co-create
accelerate & assist with the Response typically focused on: ensuring we have enough health. Considerations of equity, power &
diagnosis and treatment of the people/skills/technology along each part of the pathway to culture key, to support genuine health
individual improve equality of access and outcomes – but what of creation rather than care substitution.
equality of expectations?The balance between paradigms may shift over time and for different individuals - but the overarching paradigm will determine the answer to some fundamental questions What do we mean by What do we value? How would we train/equip people? How would we ‘workforce’? The most By expecting people to sacrifice any employ people? Do our supply models just academically able, personal life in favour of a specialist Does it make sense include the formal workforce, or reach into more career that they need to choose and for people to be or do we recognise (and diverse devote themselves to very early on, or employees of educate and train) the backgrounds and in in a more flexible, caring providers or ‘informal’ workforce life experiences? environment, that provides more systems? And what (individuals/family/community) What values are we general as well as specialist skills, would good work and factor that into our looking for? including the ability to work with families look like? What demand modelling (if and other non-professional roles as co- values and culture? ‘upstream investment’ producers of health? reduces need for formal care etc.) These questions need to be addressed before any meaningful modelling can take place, otherwise we are just recycling current assumptions back into the future workforce, meaning that history, rather than ambitions and actual needs will shape our future.
Learning from
other systems:
the 15 year case
study of
Canterbury
District Health
Board,
New ZealandThe Canterbury District Health Board
(CDHB) transformed its delivery system for
health and care
The CDHB Board worked out
Serves a population
of 565,000; that if they didn’t move to a
18,000 people in different care model by 2020,
total work in health Canterbury would need a
and social care hospital twice the current size,
20% more GPs and 2,000 more
residential care beds: a 40%
Devastating increase
earthquakes
struck in 2010
and 2011The DHB set out three goals for
transformation
Goal 1: Services should enable The system transformation that followed
people to take more responsibility comprised multiple programmes around
for their own health and three themes:
wellbeing.
• integrating across organisational
Goal 2: People should stay well in boundaries
their own homes and communities
• increasing investment in community-based
as far as possible.
services
Goal 3: When complex care is
required it should be timely and • strengthening primary care
appropriate
Source: Developing accountable care systems Lessons from Canterbury, New Zealand, The King’s FundPositive measurable impacts of the
integrated care system
As a result of the transformations:
• the health system is supporting more people in their homes and
communities and has moderated demand for hospital care
• Canterbury has lower:
• acute medical admission rates;
• acute readmission rates;
• length of stay;
• emergency department attendances;
• spending on emergency hospital care
And higher spending on community services
• The changes in Canterbury required considerable investment –
i.e., in implementing new technologies, training people and
developing new models of provision – and took several years.
Source: Developing accountable care systems Lessons from Canterbury, New Zealand, The King’s FundWhat were the conditions that made this
transformation possible?
• An ongoing process of transformation • Sustained investment in giving staff skills to support
that had begun long before the them to innovate & giving them permission to do so;
earthquake; • Consistent use of well-validated improvement,
• Strong, visionary leaders in the DHB; innovation and design methods; investing in them at
• Developing new models of integrated an expert level and building these skills in all their
working people;
• Strong trusting relationships between • An explicit theory of change;
primary and secondary care; • Innovation and investment in IT, and partnership
with the local IT industry
• Probably the most mature, networked
• A national health system which at that time gave a
primary care system in New Zealand;
lot of autonomy to DHBs;
• A unified funding system for health and • The earthquake created a “burning platform” for
social care; change
Source: review of all the literature on the CDHB transformationRepair shop, pathway and network at Canterbury
DHB
A significant
shift to the network
model with a drive
towards community based,
integrated care models, with
services based around the
person in their own Move to standardised The repair shop approach
community access routes and applies largely to those
However, the model pathways of care, across people with complex,
adopted was less about primary and secondary unpredictable, higher risk
community assets and settings through the needs
more about how HealthPathways model
professional roles are (more than 900 currently)
organised
Network Pathway Repair shopIn 2020, most of the executive
leaders that had led the system
transformation at Canterbury
DHB resigned in conflict with
the DHB board over its
approach to financial deficitsWhat is relevant for our context?
• “More of the same” is not a viable option
• Significant opportunities to move to a more networked approach (and
to take it further, with a bigger role for community assets)
• Repair shop, pathway and network all have a role but segmentation is
clear
• There are a series of inherent tensions or paradoxes in this case study:
• Realism vs. optimism (the Stockdale paradox played out)
• Doing new and radical things in a system at the same as meeting the
transactional requirements
• The urgent need for change and the timescale it takes
• Meeting the needs of the local population vs. a national approach to
providing health and careBreakout 2: Does the collective ambition resonate? Is there anything missing / shouldn’t be there? Breakout 3: What are the opportunities and implications of future service models, based on different paradigms, in how we develop our workforce? Looking backward and learning from the past, what barriers might we need to overcome to develop this future workforce? What strengths and assets can we build on to create this future?
Co-production Language and identities
At level of patients and populations • How we build and/or create engagement
AND with people who work in health and care
NHS with other actors within the wider health and care system AND
• How we ensure that we co-create the
Differing perspectives: Doing this with wider society? Leading future as partners (equitable) with others
from the front AND being responsive? and right across our society (citizens AND
populations)
• Ownership, responsibility, agency …
Vision, direction, Reconstituting identities of workforce,
destination Forecast citizens and populations - develop shared
How can we understand this well understanding of challenges and 'passing
enough to move towards it? back' responsibility
Foresight • Structural inhibitors e.g. vertical
Outward mindset – seeking analogies
and comparators globally professional progression
Trust, equity and power Repair shops, pathways, networks
• Multiple layers of ‘disconnect’ within our • System shifting from where we are now…
system(s) – social; adult/children’s; NHS • Imbalance in the “three paradigms” now – we
and health more widely understood need to reflect more on the balance and the
• Disconnect between current service connections between them
models and our imperative towards • Society, social determinants of health…?
preventionOpportunities, barriers, strengths…
Nuanced thinking
Barriers
• Constant crisis management mode
• Resource to make change
Connections between
• Whole system reluctance to make change
• Owning our part Light and shade
(weakness/asset link)
Opportunities
Leading for complexity:
Strengths a collective endeavour
• Increasing confidence to collaborate across
boundaries
• Space for new and different coalitions
• Formal and informal workforce(s)
• Experimentation with non-traditional modelsIN YOUR FORESIGHT GROUP Breakout four: Working from the future backwards • What do we need to start doing NOW to deliver the future workforce? • How do we define “workforce”? • Who do we need to recruit to do what? • How should the workforce be trained, employed and organized? • What are the potential implications for regulation and registration? • What environmental factors - culture, OD and CPD and other support is needed for workforce to be successful and retained beyond recruitment? • What key questions must we address in deliberative event 3?
Getting into your foresight group breakout room Three ways to join your foresight group breakout group: 1. Everyone should have received a foresight group list which encompasses your foresight group’s members and the link to your foresight group. Click on the link attached to the list, for example it will look like this: Click here for Foresight Group 8 2. The link for each foresight group (and associated participants) will also be posted to the meeting chat box. Click on the link for your foresight group in the chat box. Please be patient it will take time to post 25 links into the chat box. 3. After step 2 above has been completed and you do not know which foresight group you have been allocated to, simply pick a group to join and click the link – you will be welcome!! Notes: • When you reach a breakout room, please be a little patient, it can take a minute or two for others to join • If your convenor or facilitator hasn’t arrived, please start the conversation anyway • if you cannot get into a foresight group even after clicking on a link, stay in the main meeting room and one of the tech team will look to help you
• What do we need to start doing NOW to deliver the future workforce? • How do we define “workforce”? • Who do we need to recruit to do what? • How should the workforce be trained, employed and organized? • What are the potential implications for regulation and registration? • What environmental factors - culture, OD and CPD and other support is needed for workforce to be successful and retained beyond recruitment? • What key questions must we address in deliberative event 3?
Recurrent themes…
• How do we adopt a co-productive mindset (to process and
content) from the outset?
• Acknowledge whom the current paradigms work for (power)
• Parity of esteem (sectors; professions; entities e.g. Local
Government / NHS)
• “Workforce” as a whole (remunerated or not)
• Widen out entry into the workforce: foundation years,
apprenticeships, ‘tester’ experiences
• Expand fluidity – more versatile career paths across boundaries
(with interoperable systems and approaches to enable it); from
“roles” to “skills”; changing expectations re life/work/health
Continuing our work • More time to deep-dive on each element – an asynchronous
after today… process in-between?
Our next Deliberative • Implementation to move in parallel with deliberation
Event… • Leverage points for change: ICS (what AND how)
• Theory/concept AND grounded/reality: linking paradigms into the
current system realities
• Diversify our leadership participationReflections and next steps Leading into deliberative event 3 (February 10th) Sir David Behan
The next steps • Preparing for deliberative event number three: • February 10th 10am to 3pm • We will send the slides • Report of the outputs of today within two weeks • We will check in with you before the next event • Tweet about the event #OurFutureWorkforce
You can also read