Cholecystitis Information for patients - North Tees and Hartlepool NHS Foundation Trust
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

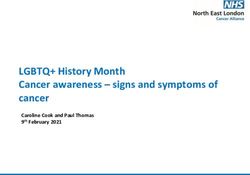
Cholecystitis Information for patients This leaflet can be made available in other formats including large print, CD and Braille and in languages other than English, upon request. This leaflet tells you about cholecystitis. What is cholecystitis? Cholecystitis is the medical term for inflammation (swelling and redness) of the gallbladder. The gallbladder is a small sac, 3 - 4 inches, (7.5 - 10 cm) long. It lies under your ribs at the front on your right hand side, below your liver and above your small bowel. The gallbladder is connected to the liver by the bile duct (small tube). See diagram below. What does the gallbladder do? The gallbladder stores bile (a yellow / green fluid) which is produced by the liver. Bile helps digest the food you eat, especially fatty food. After eating a meal, your gallbladder contracts (squeezes) and pushes bile into your bile duct (see diagram) and then into your duodenum (small bowel) to help the digestion of your food. It is not a vital organ and it can be surgically removed if it causes problems. Surg/107.4 (2017) Page 1 of 6 For Review Spring 2020
Cholecystitis
What causes cholecystitis?
Inflammation of the gallbladder is often caused when gallstones irritate the
gallbladder and sometimes cause an infection. Gallstones are formed in the
gallbladder or bile duct and develop when bile forms crystals. Over time these
crystals become hardened and eventually grow into stones but they do not always
cause problems.
However, gallstones can cause:
jaundice. If the stones move from your gallbladder and block your bile duct
jaundice can occur. If this happens you may notice your skin develops a
yellowish colour, you may have pale stools (poo) and dark urine (wee).
pancreatitis. This is an inflammation of the pancreas. The pancreas lies
behind your stomach and produces digestive enzymes (your body’s natural
chemicals) which pass into the upper part of your small bowel through a tube
called the pancreatic duct. Enzymes help to digest the fat in your food.
A gallstone can block the pancreatic duct, trapping digestive enzymes in the
pancreas and causing pancreatitis. Pancreatitis can be a life threatening
illness if left untreated.
cancer of the gallbladder. This is a rare cancer. Signs and symptoms can
be similar to those of gallstones. If cancer of the gallbladder is suspected
your consultant will discuss this with you.
Why do some people develop gallstones and others do not?
It is not known why some people develop gallbladder disease and others do not.
There are some reasons which can make people more likely to develop gallstones
and these include:
heredity. Gallstones tend to run in families.
gender. Women are twice as likely as men to have gallstones.
pregnancy. Pregnancy causes oestrogen (female hormone) levels to rise
which can increase the risk of gallstones developing.
body weight. Being overweight increases the amount of cholesterol in your
bile. This extra cholesterol may form into crystals and eventually into
gallstones.
lifestyle. What you eat and drink can make it more likely for gallstones to
develop, for example, high fat, high sugar food and drinks or low calorie diets.
Rapid weight loss can also make you more at risk.
Surg/107.4 (2017) Page 2 of 6 For Review Spring 2020Cholecystitis
age. The chance of developing gallstones increases with age.
previous bowel surgery. Some operations to the bowel can increase the risk
of developing gallstones.
How will I know if I have gallstones?
Most people with gallstones do not know they have them as they do not have any
problems. If gallstones start to cause problems you may notice signs and symptoms
such as:
chronic indigestion. This includes a feeling of bloating and heartburn,
especially after a fatty meal.
nausea (feeling sick) and vomiting (being sick).
biliary colic (gallbladder pain). Biliary colic can be caused by muscular
spasm when your gallbladder tries to expel (get rid of) the stones. This usually
starts in the upper right part of your abdomen (tummy). The pain may shift to
your right shoulder and into the centre of your back. If a gallstone becomes
lodged (stuck) in your common bile duct, bile may back up and cause your
gallbladder to become infected, causing you to feel feverish.
jaundice. If the stones move from your gallbladder and block your bile duct
jaundice can occur. If this happens you may notice your skin develops a
yellowish colour, you may have pale stools and dark urine.
What tests will I need?
To help find the cause of your symptoms your doctor or nurse practitioner will ask
you about your medical history, examine you, and take a sample of your blood for
testing in the laboratory.
He or she may also request you have the following tests:
abdominal x-ray. This is an x-ray of your abdomen.
ultrasound scan. This is a painless examination using sound waves to make
pictures of the inside of your body.
Magnetic Resonance Cholangiopancreatography (MRCP). This is a painless
examination which needs you to lie still on an x-ray couch whilst a scanning
machine passes over your body. It then produces detailed pictures of the
inside of your body.
Surg/107.4 (2017) Page 3 of 6 For Review Spring 2020Cholecystitis
What treatments are available for cholecystitis?
There is no one single treatment best suited for all patients. Your doctor will discuss
all treatment choices with you and advise what he or she feels is best for you.
These can include:
cholecystectomy. If your doctor advises cholecystectomy (surgical removal
of your gallbladder). This can be performed in 2 different ways:
Laparoscopic cholecystectomy (keyhole surgery)
This means you will have a number of small incisions (cuts) in your abdomen.
Your gallstones and gallbladder are removed by your surgeon. You will
usually be discharged the same day or if needed, an overnight stay in
hospital.
You may need to take about 2 - 3 weeks off work, depending on your job.
Open cholecystectomy
This means you will have an incision (about 4 inches or 10 centimetres) in
your upper abdomen. Your gallstones and gallbladder are removed by your
surgeon. You will usually be discharged within
1 – 2 days.
You may need to take about 4 - 6 weeks off work, depending on your job.
Endoscopic Retrograde Cholangiopancreatography (ERCP)
An ERCP is an examination of your pancreatic and bile ducts through an
endoscope (viewing instrument) and x-ray. A special dye is injected down the
endoscope to help your pancreatic and bile ducts show up on x-ray.
If the tests show gallstones, or any narrowing of your pancreatic or bile ducts,
these can usually be treated during your ERCP examination.
no treatment. You and your doctor may decide that no treatment is needed
at this time. If you feel your symptoms are getting worse you should contact
your GP for advice.
medical treatment. If your general health is poor and you are unable to
undergo an operation, medication can treat some gallstones by dissolving
them. These drugs work slowly over the course of several months and are
only useful if your symptoms are not severe. Your doctor will advice if this
treatment could help you.
Surg/107.4 (2017) Page 4 of 6 For Review Spring 2020Cholecystitis If you need treatment your doctor will discuss this with you during your outpatient appointment. He or she will be able to answer any questions or concerns you may have. If you are going to have surgery or an ERCP you will be given a more detailed information leaflet. Further information is available from: NHS Choices telephone: 111 (when it is less urgent than 999) calls to this number are free from landlines and mobile phones or via the website at www.nhs.uk Surg/107.4 (2017) Page 5 of 6 For Review Spring 2020
Cholecystitis
This leaflet has been produced in partnership with patients and carers. All patient
leaflets are regularly reviewed, and any suggestions you have as to how it may be
improved are extremely valuable. Please write to the Quality Assurance Team,
University Hospital of North Tees or email: patientinformation@nth.nhs.uk
Comments, Concerns, Compliments or Complaints
We are continually trying to improve the services we provide.
We want to know what we’re doing well or if there’s anything which we can
improve, that’s why the Patient Experience Team is here to help.
Our Patient Experience Team is here to try to resolve your concerns as quickly as
possible. If you would like to contact or request a copy of our PET leaflet, please
contact:
telephone: 01642 624719
Monday – Friday, 9.00 am – 4.00 pm
Messages can be left on the answering machine and will be picked up throughout
the day.
freephone: 0800 092 0084
Mobile: (can use text): 0779 506 1883
Email: patientexperience@nth.nhs.uk
Out of hours if you wish to speak to a senior member of Trust staff, please contact
the hospital switchboard who will bleep the appropriate person.
telephone: 01642 617617
24 hours a day, 7 days a week
The Patient Experience Team is available to discuss your concerns in person
Monday – Friday, 1.30 pm – 4.30 pm. The office is based on the ground floor at
the University Hospital of North Tees.
Data Protection and use of patient information
The Trust has developed a Data Protection Policy in accordance with the Data
Protection Act 1988 and the Freedom of Information Act 2000. All of our staff
respect this policy and confidentiality is adhered to at all times. If you require
further information please contact the Information Governance Team.
telephone: 01642 833551 or email: information.governance@nth.nhs.uk
University Hospital of North Tees, Hardwick, Stockton-on-Tees. TS19 8PE
University Hospital of Hartlepool, Holdforth Road, Hartlepool. TS24 9AH
Telephone: 01642 617617 Fax: 01642 624089
Surg/107.4 (2017) Page 6 of 6 For Review Spring 2020You can also read