Changes in Televisit Modalities Due to the Covid-Pandemic in Chile: A Comparison of Patient Satisfaction.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Changes in Televisit Modalities Due to the Covid-Pandemic in Chile: A
Comparison of Patient Satisfaction.
Freddy Constanzo ( teleneurologiahht@gmail.com )
Hospital Las Higueras
Paula Aracena-Sherck
Universidad San Sebastián
Luis Benavides
Universidad Católica de la Santísima Concepción
Jorge Garcés
Universidad Católica de la Santísima Concepción
Rodrigo Villalobos
Universidad Católica de la Santísima Concepción
Mery Marrugo
Hospital Las Higueras
Katia Kuzmanic
Hospital Las Higueras
Ramón Caamaño
Hospital Las Higueras
Lorena Peña
Hospital Las Higueras
César Silva
Hospital Las Higueras
Cristobal Alvarado
Hospital Las Higueras
Research Article
Keywords: Assisted televisit, televisit, COVID-19 pandemic, Telemedicine.
Posted Date: September 3rd, 2021
DOI: https://doi.org/10.21203/rs.3.rs-806460/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Page 1/13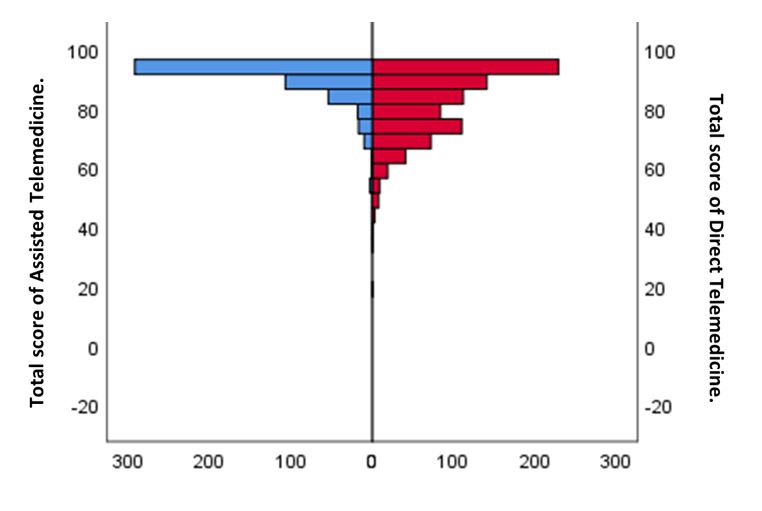
Abstract BACKROUND: The corona virus 2019 (COVID-19) pandemic has impacted healthcare guidelines and modalities of patient consultation worldwide. The frequent cycles of quarantine confinement in Chile has caused mobility restrictions for both patients and physicians, which forced the Hospital Las Higueras de Talcahuano (HHT) to replace the assisted televisit modality with a more classic televisit program. This change may have impacted the satisfaction of patients. METHODS: Patient’s perception of satisfaction was evaluated through self-administered survey questionnaires, previously validated in the Spanish language. Cohorts were grouped according to two relational models:i) Assisted televisit, 503 neurology patients during the years 2018-2019; and ii) Televisit, 831 patients from different specialtiestreated during 2020. Perception of satisfaction was compared by gender, age, and type of televisit, and internal consistency (Cronbach alpha) and reliability (factorial analysis of main components) were assessed. RESULTS: Assisted televisit and televisit cohortswere composed by 64.2% and 67.6% women, respectively; patients under 65 years of age were 62.2% and 75%, respectively. Assisted televisit patients showed very high 94.4% (n=475) and high 5.2% (n=26) satisfaction levels, while televisit patients showed very high 22.3% (n=185), high 63.9% (n=531), and moderate 13.1% (n=109) satisfaction levels; this difference is statistically significant at p
an electronic device such as smartphone or computer (usually at their home). The televisit modality has been previously shown to be successful in highly
developed regions (14); this modality, however, appears to be less accepted by communities in underdeveloped or developing regions (15, 16). Although
most likely multifactorial, causes for community acceptance of the televisit or assisted televisit modalities have yet to be elucidated. The modality change
in the HHT teleneurology program, from an assisted televisit consultation to a televisit one during the COVID-19 pandemic, provides an opportunity to
evaluate potential differences in patient satisfaction between these two televisit modalities. The present study shows results of a patient satisfaction
survey, previously validated for the HHT teleneurology program (9), with outpatients from different medical specialties, that consulted through the televisit
modality in 2020, and their comparison with the assisted televisit modality implemented in 2019 (9). Data are discussed in the context of factors allowing
populations to prefer one or another modality in televisit.
2. Methods
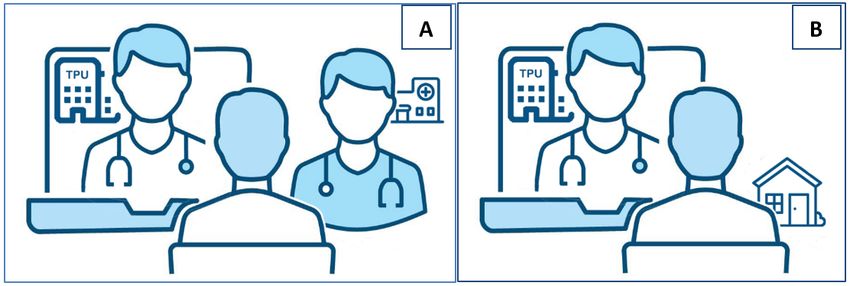
Telemedicine care modalities: Here we define two relational models, i) Assisted televisit and ii) televisit. Assisted televisit is a relational model already
published by Contanzo et al. (9): it consists of the connection of the specialist doctor who is located in the hospital with the patient who is located in a
local primary health service, both assisted by the TPU (Fig. 1A). The patient in this modality is accompanied by a general medical practitioner who works in
the local primary care service. The second model, televisit, was implemented in the HHT by the TPU, due to the COVID-19 pandemic-derived confinement of
patients in their homes. In this model, the specialist contacts the patient directly through electronic devices without the assistance of another health
professional from the primary care service (Fig. 1B).
Patient Cohorts: Patient cohorts were divided according to the televisit model: i) Assisted televisit, corresponding to a cross-sectional study of 503 patients
of the HHT Teleneurology program, treated in the assisted televisit modality during the years 2018–2019; and ii) Televisit, corresponding to a cross-
sectional study of a cohort of 831 patients treated during 2020 in the HHT Telemedicine program (assisted by the TPU) from different medical specialties:
Bronchopulmonary, Cardiosurgical, Cardiology, Endocrinology, Gastroenterology, Geriatric, Hematology, Internal Medicine, Physical medicine, Nephrology,
Neurology, Oncology, Otorhinolaryngology, Rheumatology, and Others.
Inclusion Criteria: Participants of the Assisted televisit cohort had to meet the inclusion criteria described in Constanzo et al (9). Participants of the Televisit
cohort had to meet the following inclusion criteria: i) to consent for remote care, included new appointments and controls; ii) to have internet connection
and at least a computer, a tablet, or a smartphone with camera; iii) to present a pathology not requiring emergency care and are stable; iv) to be of legal
age and mentally competent, according to the Chilean Law (Bill 28584, article 28). The research protocol was approved by the Scientific Ethics Committee
of the SST of the Ministry of Health. All participants signed a written informed consent.
Survey design assisted televisit and televisit: To evaluate the patient’s perception of satisfaction, two essentially identical surveys were employed. The
assisted televisit survey evaluated patient perception of satisfaction using the questionnaire designed and constructed in Spanish, consisting of a total of
23 questions with closed responses on a single Likert scale (totally disagree, disagree, neither agree nor disagree, agree, totally agree), which was
previously validated by Constanzo et al (9). The survey questionnaire, with a maximum score of 115 points, was graded in terms of satisfaction: very low
(under or equal to 23 points), low (24 to 46 points), moderate (47 to 69 points), high (70 to 92 points), and very high (93 to 115 points). The televisit survey
was identical to the previous one, except for the exclusion of questions related to the general medical practitioner from the primary health center (questions
13, 17, 22 and 23), as this professional is absent from this model. Following this adaptation, the survey consisted in a total of 19 questions with closed
responses on a single Likert scale (totally disagree, disagree, neither agree nor disagree, agree, totally agree). The survey questionnaire, with a maximum
score of 95 points, was graded in terms of satisfaction: very low (under or equal to 19 points), low (20 to 38 points), moderate (39 to 57 points), high (58 to
76 points), and very high (77 to 95 points). Both questionnaires were self-administered to safeguard the anonymity of the study participant.
Survey evaluation and statistical analysis. A descriptive analysis of normality of the sample (Kolmogorov-Smirnov) was conducted. The internal
consistency was evaluated by Cronbach's alpha test, which suggests the following scale for alpha coefficients: excellent (> 0.9), good (> 0.8), acceptable (>
0.7), questionable (> 0.6), poor (> 0.5), and unacceptable (< 0.5) (9). Difficulty and discrimination of the instrument were evaluated by index of difficulty and
specific biserial correlation, respectively. To compare the means of both surveys with a not normal distribution, we used The Mann-Whitley U test for
independent samples. All analyses were carried out in SPSS, version 25.0. Statistical significance was established at p < 0.05.
Ethics approval and consent to participate: This project was approved by Scientific Ethics Committee of the SST of the Ministry of Health (Acta N°97 from
12.12.2017). I confirm that all research was performed in accordance with relevant guidelines/regulations, and theinformed consent was obtained from all
participants and/or their legal guardians. Consent obtained from study participants was written (assisted televisit)and verbal (televisit) and both ways
were approved by the ethics committee.
Page 3/13Table 1
Patients of assisted televisit (n = 503) and
televisit (n = 803) modality categorized by gender
and age.
Assisted Televisit Televisit
GENDER n % n %
Male 180 35,8 269 32,4
Female 323 64,2 562 67,6
Total 503 100,0 831 100,0
AGE n % n %
Under 65 313 62,2 623 75,0
Over 65 190 37,8 208 25,0
Total 503 100,0 831 100,0
Table 2
Televisit patients categorized by medical specialty (n = 831). All
patients of assisted televisit were neurology patients.
Medical Specialty Frequency Percentage
Endocrinology 165 20%
Otorhinolaryngology 126 15%
Bronchopulmonary 122 15%
Internal Medicine 91 11%
Neurology 68 8%
Gastroenterology 56 7%
Cardiology 46 6%
Hematology 39 5%
Cardiosurgery 26 3%
Others 23 3%
Rheumatology 21 3%
Physical Medicine & Rehabilitation 19 2%
Geriatrics 11 1%
Oncology 10 1%
Nephrology 8 1%
Total 831 100%
Table 3
User satisfaction of assisted televisit (n = 503).
Variables Total
n %
User Satisfaction
Very low satisfaction (≤ 23 points on satisfaction scale) - -
Low satisfaction (24–46 points on satisfaction scale) - -
Moderate satisfaction (47–69 points on satisfaction scale) 2 0,4%
High satisfaction (70–92 points on satisfaction scale) 26 5,2%
Very high satisfaction (93–115 points on satisfaction scale) 475 94,4%
Total 503 100%
Page 4/13Table 4: User satisfaction of televisit (n=831).
Variables Total
n %
User satisfaction
Very low satisfaction (≤19 points on satisfaction scale) 1 0,1%
Low satisfaction (20-38 points on satisfaction scale) 5 0,6%
Moderate satisfaction (39-57 points on satisfaction scale) 109 13,1%
High satisfaction (58-76 points on satisfaction scale) 531 63,9%
Very high satisfaction (77-95 points on satisfaction scale) 185 22,3%
Total 831 100%
Table 5. Descriptive data of the total population by mean per question, difficulty, mean when the question is deleted, reliability analysis (a-Cronbach), and
biserial correlation of the patient satisfaction survey, used in assisted televisit (n=503) and televisit (831).
Page 5/13Assisted Televisit (n=503) Televisit (n=831)
N° Variables Mean Difficulty Biserial Mean α when Mean Difficulty Biserial Mean α when
per Correlation when the per Correlation when the
question the question question the question
question is question is
is deleted is deleted
deleted deleted
0,90 0,94
1 I am satisfied 4,83 0,97 0,63 104,22 0,90 4,47 0,89 0,70 77,39 0,93
with the care
received in
Telemedicine.
2 My family is 4,44 0,89 0,40 104,62 0,90 4,28 0,86 0,66 77,57 0,93
satisfied with the
care received in
Telemedicine.
3 Telemedicine 4,75 0,95 0,54 104,30 0,90 4,16 0,83 0,71 77,70 0,93
helps me to know
my state of
health.
4 Telemedicine 4,71 0,94 0,55 104,34 0,90 4,18 0,84 0,69 77,67 0,93
helps me know
how to improve
my health status.
5 Telemedicine 4,79 0,96 0,58 104,27 0,90 4,28 0,86 0,70 77,57 0,93
allows me to
better follow the
recommendations
and indications of
my specialist
doctor.
6 I felt comfortable 4,71 0,94 0,54 104,34 0,90 4,49 0,90 0,68 77,36 0,93
talking to my
specialist doctor
through a camera
and a
microphone.
7 Talking to my 4,58 0,92 0,69 104,48 0,89 3,89 0,78 0,74 77,97 0,93
specialist doctor.
through a camera
and a
microphone. was
as effective as in
person.
8 During my 4,67 0,93 0,61 104,38 0,90 4,40 0,88 0,71 77,45 0,93
Telemedicine care
it was easy for
me to explain my
health problem to
my specialist
doctor.
9 My specialist 4,70 0,94 0,53 104,36 0,90 4,22 0,84 0,67 77,64 0,93
doctor has
identified my
health problem
through
Telemedicine.
10 I have been 4,68 0,94 0,22 104,37 0,91 4,05 0,81 0,38 77,80 0,94
informed of my
right to privacy of
my personal and
medical
information
included in
Telemedicine.
11 I trust that my 4,81 0,96 0,54 104,24 0,90 4,39 0,88 0,62 77,47 0,93
personal
information and
privacy will be
protected after
my attention by
Telemedicine.
12 The quality of the 4,76 0,95 0,36 104,30 0,90 4,50 0,90 0,58 77,35 0,93
Page 6/13image and sound
were adequate to
talk to my
specialist doctor.
13* The general 4,88 0,98 0,50 104,17 0,90
doctor who
accompanied me
in person helped
me during my
Telemedicine
consultation. *
14 My attention by 4,84 0,97 0,74 104,21 0,89 4,45 0,89 0,82 77,41 0,93
Telemedicine was
helpful to me.
15 The time with a 4,74 0,95 0,49 104,31 0,90 4,21 0,84 0,54 77,65 0,94
specialist is faster
by Telemedicine.
16 I prefer 4,71 0,94 0,61 104,34 0,90 4,25 0,85 0,57 77,60 0,93
Telemedicine
because it is
easier to go to the
doctor's office
than to go to the
hospital.
17* I prefer 4,56 0,91 0,49 104,50 0,90
Telemedicine
because it is
cheaper to go to
the office than to
go to the hospital.
18 For my future 4,56 0,91 0,49 104,50 0,90 3,95 0,79 0,60 77,90 0,93
controls I will
prefer to continue
using
Telemedicine.
19 My specialist 4,87 0,97 0,63 104,19 0,90 4,53 0,91 0,71 77,33 0,93
doctor was able
to answer my
questions through
Telemedicine
20 My specialist 4,84 0,97 0,52 104,21 0,90 4,57 0,91 0,70 77,29 0,93
doctor showed
concern in solving
my health
problem during
Telemedicine
care.
21 I trust the 4,87 0,97 0,66 104,18 0,90 4,60 0,92 0,72 77,25 0,93
instructions of my
specialist doctor
during my
Telemedicine
care.
22* The general 4,86 0,97 0,55 104,19 0,90
practitioner who
accompanied me
in person during
the Telemedicine
service was able
to answer my
questions.*
23* The general 4,89 0,98 0,54 104,16 0,90
practitioner who
accompanied me
in person during
the Telemedicine
care could answer
the questions of
my specialist
doctor. *
3. Results
Page 7/13Patient cohort description assisted televisit and televisit: The Assisted televisit cohort consisted of64.2% women and 35.8% men; 62,2% of patients were under 65 years old, and 37.8% were older. On the other hand, the Televisit cohort consisted of 67.6% women and 32.4% men; 75% of patients were under 65 years old, and 25% were older (Table 1). While allparticipants of the Assisted televisit cohort were neurological patients, those of theTelevisit cohortconsulted different medical specialties: Endocrinology 20% (n=165),Otorhinolaryngology 15% (n=126),Bronchopulmonary 15% (n=122),Internal Medicine 11% (n=91),Neurology 8% (n=68),Gastroenterology 7% (n=56),Cardiology 6% (n=46),Hematology 5% (n=39),Cardiosurgery 3% (n=26),Others 3% (n=23),Rheumatology 3% (n=21),Physical Medicine & Rehabilitation 2% (n=19),Geriatrics 1% (n=11),Oncology 1% (n=10),and Nephrology 1% (n=8) (Table 2). In terms of the perception of satisfaction with each model,different patterns of satisfaction arose: Assisted televisit patients showed very high 94.4% (n=475) and high 5.2% (n=26) satisfaction (Table 3), whileTelevisit patients showed very high 22.3% (n=185), high 63.9% (n=531) and moderate 13.1% (n=109) satisfaction (Table 4). Comparison of participant satisfaction in both cohorts by gender andage did not result in significant differences (p
through reinforcement and managing by the general practitioner who accompanies the patient in situ during the televisit. This modality allows for several
advantages for the patient, including: i) the patient is better appraised of his or her diagnosis and treatment by two physicians instead of one, reinforcing
the clinical messages; ii) in most cases, there is an already ongoing rapportbetween the patient and the general practitioner, which in turn, facilitates and
strengthens the one of the patient with the specialist; and iii) since the general practitioner works in a healthcare institution that covers the geographical
area where the patient lives in, this professional can better perceive the patient’s livelihood reality,facilitating the specialist-patient dialogue. (10,11,20).
Furthermore, the assisted televisit model generates a space for continuous collaboration between tertiary and primary healthcare, highlighting the
importance of a team work that contributes to overcomingthe fragmentation evidenced in the Chilean health system and other latitudes, through an
integrative solution that reinforces a patient-centered praxis, instead of a institutional-centered one(24).
The HHT TPU has pioneered the assisted televisit modality in the region, and the hurdles imposed by the COVID-19 pandemic has allowed for the widening
of the specialty spectrum of telemedicine programs. We expect that once this pandemic is managed, the TPU not only will be able to restore assisted
televisit modality but also implement this model to more specialties in the HHT. In addition, there are still several landmarks to be accomplished in this area
of healthcare: i) to further widen the spectrum of specialties covered by the TPU, ii) to educate the health community and patients in remote care, and iii) to
create a new digital hospital with new facilities.Overall, high satisfaction scores shown in the present study indicate that patients in both the public and
private healthcare systems would be benefited by implementing telemedicine programs, in particular, under the assisted model.
5. Abbreviations
Hospital Las Higueras of Talcahuano (HHT)
Teleprocess Unit (TPU)
Health Service of Talcahuano (SST) of the Ministry of Health.
6. Declarations
Ethics approval and consent to participate. The research protocol was approved by Scientific Ethics Committee of the SST of the Ministry of Health (Acta
N°97 from 12.12.2017). All participants signed a written informed consent.
Documento de Formulario de Información para el estudio “VALIDATION OF A PATIENT SATISFACTION SURVEY OF THE TELENEUROLOGY PROGRAMME IN
CHILE”
Este formulario de Consentimiento Informado se dirige a hombres y mujeres que son atendidos en el programa de Teleneurología del Hospital Higueras de
Talcahuano, y a los que se les invita a participar en una investigación cuyo objetivo es validar un instrumento de recolección de datos que permita medir la
satisfacción usuaria de los pacientes respecto de la atención neurológica recibida mediante el programa de Teleneurología del HHT.
El investigador principal de esta investigación es el Dr. Freddy Constanzo Parra, la cual se encuentra patrocinada por la Universidad Católica de la
Santísima Concepción.
Introducción
Yo soy (nombre del médico tratante encargado de solicitar el consentimiento informado), trabajo para el Servicio de Salud de Talcahuano y formo parte del
equipo de investigación del Dr. Constanzo. Actualmente, queremos validar una encuesta que permita conocer el nivel de satisfacción de la población con
respecto a la atención recibida en el programa de Teleneurología, por lo que vengo a invitarlo a participar de esta investigación. No tiene que decidir hoy si
participa o no en el estudio. Antes de decidirse, puede hablar con alguien que se sienta cómodo y en confianza sobre la investigación.
Puede que haya algunas palabras que no comprenda, por ello cuando lo estime necesario puede pararme para recibir la explicación que necesite. Si tiene
alguna pregunta puede preguntarme a mí o a cualquier miembro del equipo de investigación cuando lo estime necesario.
Propósito
Validar un instrumento que permita conocer la satisfacción de los usuarios de un programa, lo cual en un futuro permitirá identificar errores y mejorar
falencias, prestando así una atención de mayor calidad a los usuarios.
Tipo de Intervención de Investigación
Esta investigación sólo incluye la contestación de una encuesta, la cual será anónima y completada por usted en un ambiente de tranquilidad y respeto.
En caso de no saber leer o presentar un problema que le impida completar la encuesta, personalmente me haré cargo de ayudarlo para responder,
asegurándole un ambiente de seguridad y anonimato.
El tiempo para completar esta encuesta no será superior a los 30 minutos.
Selección de participantes
Estamos invitando a adultos que han formado parte del programa de Teleneurología a responder esta encuesta.
Page 9/13Participación Voluntaria
Su participación en esta investigación es totalmente voluntaria. Usted puede elegir participar o no hacerlo. Tanto si elige participar o no, continuarán todos
los servicios que recibía en este programa y nada cambiará. Usted puede cambiar de idea más tarde y dejar de participar aun cuando lo haya aceptado
antes.
Riesgos
Esta investigación no implica ningún riesgo para su salud.
Beneficios
Esta investigación no implica ningún beneficio económico.
Confidencialidad
Nosotros no compartiremos la identidad de las personas que participen de esta investigación. Las respuestas que se obtengan a través de esta encuesta
se mantendrán en absoluta confidencialidad.
Compartiendo los Resultados
Los hallazgos encontrados en esta investigación podrán ser utilizados para realizar publicaciones científicas, obviamente sin revelar la identidad de los
participantes.
A Quién Contactar
Si tiene cualquier pregunta puede hacerla ahora o más tarde, incluso después de haber respondido la encuesta.
Si desea realizar preguntas más tarde puede contactar al Dr. Freddy Constanzo Parra, Jefe del Servicio de Neurología del Hospital las Higueras de
Talcahuano. Dirección Alto Horno 777. Talcahuano. Fono: 41-2687345. Email: neurologia.higueras@redsalud.gov.cl.
También pude consultar al Comité Ético Científico del Servicio de Salud de Talcahuano, que es un comité cuya tarea es asegurarse de que se protege de
daños a los participantes en la investigación. Nombre presidente de comité: Dra. Marcela Cortés, fono 41-2722150. Email: etica.sst@redsalud.gov.cl.
Encuestas Online.
Las encuestas online fueron realizadas vía telemática y todos los pacientes consintieron contestar la encuesta remota.
Consent for publication: Not applicable.
Availability of data and material. The dataset supporting the conclusions of this article is included within the article and its additional file.
Competing interests. I declare that me (Dr. Freddy Constanzo) and all the authors included in this manuscript have no conflict of interest.
Funding. Not applicable.
Authors' contributions: All authors have read and approved the manuscript
FC: Study conception and design, supervision of informed consent signing and survey application, and manuscript elaboration.
PA-S: Manuscript elaboration and English editing.
LB: Clinician and survey application.
JG: Clinician and survey application.
RV: Clinician and survey application.
MM: Clinician and survey application.
KK: Clinician and survey application.
RC: Clinician and survey application.
LP: Clinician and survey application.
CS: Supervision of Teleprocesses Unit.
CA: Statistical analysis, research coordinator, and manuscript elaboration.
Page 10/13Acknowledgements. We thank all the staff personnel of the Teleprocess Unit at the HHT, for their invaluable contributions to this work.
7. References
1. Instituto Nacional de Estadísticas (INE). Instituto Nacional de Estadísticas (INE). [Internet]. 2021 [cited 2021 Apr 8]. Availablefrom: https://www.ine.cl/
2. Gobierno de Chile. Gob.cl - Cifras Oficiales [Internet]. 2021 [cited 2021 Apr 8]. Available from:
https://www.gob.cl/coronavirus/cifrasoficiales/#resumen
3. Coronavirus Resource Center. COVID-19 Map - Johns Hopkins Coronavirus Resource Center [Internet]. 2021 [cited 2021 Apr 8]. Available from:
https://coronavirus.jhu.edu/map.html
4. Wang WW. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J Med Virol. 2021 Apr 1;92(4):441–7.
5. Gobierno de Chile. Gob.cl - Cifras Oficiales [Internet]. 2021 [cited 2021 Apr 10]. Available from: https://www.gob.cl/coronavirus/cifrasoficiales/
6. Ministerio de Salud G de C. 4to informe trimestral de garantías de oportunidad respecto a los retrasos en regimen GES. [Internet]. 2019 [cited 2021 Apr
10]. Available from: https://www.minsal.cl/wp-content/uploads/2020/05/Ord-251-Glosa-06.pdf
7. Ministerio de Salud. Glosa 06, Lista de Espera No GES y Garantías de oportunidad GES retrasadas [Internet]. Santiago; 2021 Apr [cited 2021 Jun 30].
Available from: https://www.minsal.cl/wp-content/uploads/2021/05/ORD-1204-DIGERA-Glosa-06.pdf
8. Constanzo F, Aracena-Sherck P, Hidalgo JP, Peña L, Marrugo M, Gonzalez J, et al. Contribution of a synchronic teleneurology program to decrease the
patient number waiting for a first consultation and their waiting time in Chile. BMC Med Inform DecisMak. 2020 Feb 5;20(1).
9. CENS. Telemedicina durante la epidemia de COVID-19 en Chile: Guía de Buenas Prácticas y Recomendaciones. 2020.
10. Constanzo F, Aracena-Sherck P, Hidalgo JP, Muñoz M, Vergara G, Alvarado C. Validation of a patient satisfaction survey of the Teleneurology program
in Chile. BMC Res Notes. 2019;12(1).
11. Constanzo F, Aracena-Sherck P, Hidalgo JP, Peña L, Marrugo M, Gonzalez J, et al. Contribution of a synchronic teleneurology program to decrease the
patient number waiting for a first consultation and their waiting time in Chile. BMC Med Inform DecisMak. 2020;20(1).
12. Constanzo FM, Aracena-Sherck P, Peña L, Marrugo M, Gonzalez J, Vergara G, et al. Characterization of the Teleneurology patients at the Hospital Las
Higueras de Talcahuano-Chile. Front Neurol. 2020;11:1438.
13. Klein BCNAB. Author response: COVID-19 is catalyzing the adoption of teleneurology | Neurology [Internet]. Neurology. 2020 [cited 2020 May 20].
Available from: https://n.neurology.org/content/author-response-covid-19-catalyzing-adoption-teleneurology
14. Camila Meza Sparza. Teleconsultas: la tecnología a favor del paciente en tiempos de pandemia - Universidad Católica de la Santísima Concepción.
Noticias UCSC [Internet]. 2020 [cited 2020 May 20]; Available from: https://www.ucsc.cl/noticias/teleconsultas-la-tecnologia-a-favor-del-paciente-en-
tiempos-de-pandemia/
15. Judd E. Hollander MD. and BGCMD. Virtually Perfect? Telemedicine for Covid-19. N Engl J Med. 2020 Apr 30;382:1679–81.
16. Roy B, Nowak RJ, Roda R, Khokhar B, Patwa HS, Lloyd T, et al. Teleneurology during the COVID-19 pandemic: A step forward in modernizing medical
care. J Neurol Sci. 2020 Jul 15;414.
17. Craig J, Russell C, Patterson V, Wootton R. User satisfaction with realtime teleneurology. J Telemed Telecare [Internet]. 1999 Dec 23 [cited 2018 Dec
20];5(4):237–41. Available from: http://journals.sagepub.com/doi/10.1258/1357633991933774
18. Ford JA, Pereira A. Does teledermatology reduces secondary care referrals and is it acceptable to patients and doctors?: A service evaluation. J Eval
Clin Pract. 2015 Aug 1;21(4):710–6.
19. Dorsey ER, Glidden AM, Holloway MR, Birbeck GL, Schwamm LH. Teleneurology and mobile technologies: the future of neurological care. Nat Rev
Neurol [Internet]. 2018 May 6 [cited 2018 Dec 20];14(5):285–97. Available from: http://www.nature.com/doifinder/10.1038/nrneurol.2018.31
20. Mair F, Whitten P. Systematic review of studies of patient satisfaction with telemedicine. BMJ [Internet]. 2000 Jun 3 [cited 2018 Dec
20];320(7248):1517–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10834899
21. Powell RE, Henstenburg JM, Cooper G, Hollander JE, Rising KL. Patient Perceptions of Telehealth Primary Care Video Visits. Ann Fam Med [Internet].
2017 May 8 [cited 2019 Mar 7];15(3):225–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28483887
22. Reed ME, Parikh R, Huang J, Ballard DW, Barr I, Wargon C. Real-Time Patient-Provider Video Telemedicine Integrated with Clinical Care. N Engl J Med
[Internet]. 2018 Oct 11 [cited 2019 Mar 7];379(15):1478–9. Available from: http://www.nejm.org/doi/10.1056/NEJMc1805746
23. Channer D. Telemedicine Technology. In: Teleneurology in Practice [Internet]. New York, NY: Springer New York; 2015 [cited 2019 Jan 17]. p. 39–46.
Available from: http://link.springer.com/10.1007/978-1-4939-2349-6_4
24. Tsao JW, Demaerschalk BM, editors. Teleneurology in Practice [Internet]. New York, NY: Springer New York; 2015 [cited 2019 Jan 17]. Available from:
http://link.springer.com/10.1007/978-1-4939-2349-6
25. Weinstein RS, Lian F, Bhattacharyya AK. Teleneuropathology. In: Teleneurology in Practice [Internet]. New York, NY: Springer New York; 2015 [cited
2019 Jan 17]. p. 113–29. Available from: http://link.springer.com/10.1007/978-1-4939-2349-6_11
26. Alexandre de la Court. Principio de suficiencia y prestaciones mínimas de Seguridad Social: una revisión desde el derecho al mínimo de existencia
alemán. Rev Derecho. 2019;32(2):165–84.
27. Bakken S, Holzemer WL, Brown M-A, Powell-Cope GM, Turner JG, Inouye J, et al. Relationships Between Perception of Engagement with Health Care
Provider and Demographic Characteristics, Health Status, and Adherence to Therapeutic Regimen in Persons with HIV/AIDS. AIDS Patient Care STDS
[Internet]. 2000 Apr [cited 2017 Jul 5];14(4):189–97. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10806637
Page 11/1328. Dick PT, Filler R, Pavan A. Participant satisfaction and comfort with multidisciplinary pediatric telemedicine consultations. J Pediatr Surg [Internet].
1999 Jan [cited 2018 Dec 20];34(1):137–41; discussion 141-2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10022159
29. Demiris G, Speedie SM, Hicks LL. Assessment of Patients’ Acceptance of and Satisfaction with Teledermatology. J Med Syst [Internet]. 2004 Dec [cited
2017 Jul 5];28(6):575–9. Available from: http://link.springer.com/10.1023/B:JOMS.0000044959.71456.df
30. Demiris G, Speedie SM, Finkelstein S. Change of Patients’ Perceptions of TeleHomeCare. Telemed J e-Health [Internet]. 2001 Sep [cited 2017 Jul
5];7(3):241–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11564360
31. Demiris G, Speedie S, Finkelstein S. A questionnaire for the assessment of patients’ impressions of the risks and benefits of home telecare. J Telemed
Telecare [Internet]. 2000 Oct [cited 2017 Jul 5];6(5):278–84. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11070589
32. Bakken S, Grullon-Figueroa L, Izquierdo R, Lee N-J, Morin P, Palmas W, et al. Development, Validation, and Use of English and Spanish Versions of the
Telemedicine Satisfaction and Usefulness Questionnaire. J Am Med Informatics Assoc [Internet]. 2006 Nov 1 [cited 2017 Jul 5];13(6):660–7. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/16929036
33. Telemedicine Forms - The Source [Internet]. [cited 2017 Jul 5]. Available from: http://hub.americantelemed.org/thesource/resources/telemedicine-
forms
Figures
Figure 1
Representation of the assisted televisit (A) and televisit (B) used before and during COVI-19 pandemic, provided by Teleprocess Unit (TPU). ORIGINAL
PICTURE.
Page 12/13Figure 2
We compare the user satisfaction between assisted televisit (left-blue, N=503) and televisit (right-red, N=831). The Mann-Whitley U test for independent
samples showed a significant difference between the two populations distribution (p=0.000). ORIGINAL PICTURE.
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
DATABASE2021.xlsx
Page 13/13You can also read

















































