Clinical and Experimental Experiences with Intravenous Vitamin C
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical and Experimental Experiences with Intravenous Vitamin C
Clinical and Experimental Experiences
with Intravenous Vitamin C
Neil H. Riordan, PA-C;1 Hugh D. Riordan, M.D.;1 Joseph P. Casciari, Ph.D.1
For the purposes of this paper reference ment. In particular we began testing for
to ascorbic acid or vitamin C refers to so- toxicity of vitamin C toward cultured tumor
dium ascorbate. All in vitro studies de- cell lines using dense monolayers and hol-
scribed herein used sodium ascorbate. All low fiber tumor models to mimic the three
intravenous vitamin C references herein re- dimensionality of tumors. We used human
fer to the use of vitamin C for injection pro- sera as culture media to include the serum
duced by Steris Laboratories, or American inhibitory activity seen in previous assays.
Regent laboratories; both are ascorbic acid Using these new culture conditions we
buffered to a pH range of 5.5 to 7.0 by so- found that the cytotoxic concentration of
dium hydroxide and/or sodium bicarbonate. vitamin C for most human tumor cell lines
was indeed much higher than previously
Background described. (Figure 1, p. 202).
Vitamin C has potential as a chemo-
therapeutic agent. Rather than possessing Human Vitamin C Pharmacokinetics
adverse side effects as most chemotherapeu- Given the information that higher con-
tic drugs do, vitamin C has side benefits such centrations of vitamin C were required to
as increasing collagen production, and en- become cytotoxic to tumor cells, we needed
hancing immune function. to learn more about the pharmacokinetics
We began to study the effects of vita- of vitamin C. There were no data on the
min C on cultured tumor cells in 1991. We concentrations of vitamin C that were
found that vitamin C was preferentially toxic achievable in human beings after high-dose
to tumor cells–it killed tumor cells before intravenous vitamin C. We therefore began
killing normal cells. This phenomenon first a series of experiments to yield data for
came to our attention through the work of modeling pharmacokinetics of high doses
Benade et al in 1969.1 They theorized that of vitamin C.
the preferential toxicity was due to the rela- We gave a series of vitamin C infusions
tive deficiency of catalase in tumor cells. to a 72 year old male who was in excellent
This theory has since been validated by oth- physical condition except for slowly pro-
ers.2 Our early findings on preferential vita- gressing, non-metastatic carcinoma of the
min C toxicity were published in 1994.3 In prostate. Before the infusions, and at in-
that paper we also described a so called “se- tervals thereafter, blood was drawn from a
rum effect;” vitamin C’s toxicity was reduced heparin lock (not the site of infusion). The
by the presence of human serum. Serum’s plasma was separated and analyzed for
inhibitory effects led us to the conclusion plasma vitamin C concentration using a
that the concentrations of vitamin C which microplate-based 2,6-dichlorophenol-indo-
were toxic to tumor cells in our early stud- phenol assay. Some of the results are given
ies (5 to 50 mg/dL) would not necessarily in Figure 2, (p. 202). From this experiment
be toxic in vivo. we observed that a 30 gram infusion was
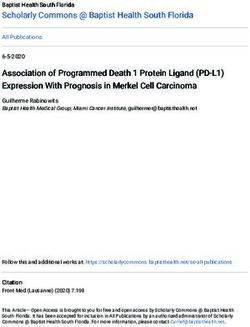
We therefore began a series of experi- not adequate to raise plasma levels of vita-
ments in which we tried more closely to min C to a level that was toxic to tumor
mimic the in vivo tumor micro-environ- cells (>200 mg/dL for dense monolayers
and >400 mg/dL for hollow fiber models).
1. Bio-Communications Research Institute, 3100 N. Hill-
side Ave, Wichita, KS 67219. Infusion of 60 grams resulted in a brief (30
201Journal of Orthomolecular Medicine Vol. 15, No. 4, 2000
Figure 1. Vitamin C toxicity toward human colon cancer cells in different models.
120
100
Percent live cells remaining
80
60 Dense Hollow Fiber
Dense Monolayer
40 Sparse Monolayer
20
0
-20
0 200 400 600 800 1000
Vitamin C (mg/dL)
Figure 2. Effects of 15, 30, 60, and 65 grams of ascorbate infused over various times on
plasma ascorbate concentration in a 72-year-old man.
540
6/4/97 30g in 80 min.
480
6/4/97 60g in 80 min.
420
Plasma Ascorbate (mg/dL)
6/25/97 60g first 60 min
360 20g next 60 min.
300
240
180
120
60
0
-60
-40
-20
20
40
60
80
0
100
120
140
160
180
200
220
240
260
280
300
320
340
360
380
400
IV started Time (min)
202Clinical and Experimental Experiences with Intravenous Vitamin C
min) elevation of plasma levels of vitamin all experiments are shown in Table 2 (p.
C above 400 mg/dL, while 60 grams infused 204) To see if there was any systematic
over 60 minutes immediately followed by variation in Table 2 parameter values over
20 grams infused over the next 60 minutes time, the parameter KX, and the ratio K2/
resulted in a 240 minute period in which K 1 for each experiment were plotted
the vitamin C plasma concentration was against time. The excretion constant, KX,
near or above 400 mg/dL. was remarkably uniform, as was the ratio
K2/K1 (Figure 4, p. 205). The tissue up-
Ascorbate Pharmacokinetics take rate constant, K1, did vary, but not in
Using data from the above experi- a systematic way. We use the ratio K2/K1
ments we designed a two-compartment to point out that while K2 also varies, its
model with four adjustable parameters (VP, variation merely compensates for varia-
KX, K1, K2) to fit the data. The model sche- tions in K1. We conclude from this analy-
matic and the data fit are shown in the sis that the pharmacokinetic parameters
accompanying Figure 3 (below). The pa- of the subject did not change over a one
rameter KX represents the rate of excre- month period of regular ascorbate infu-
tion of ascorbate out of the blood (renal sions.
excretion), while parameter K1 represents
the rate of diffusion of ascorbate from the Other Pharmacokinetic Studies
blood into tissue and K2 represents the dif- We plotted data points from three re-
fusion rate for return of ascorbate to the cent studies (over a three month period)
blood stream from the tissue compart- against the theoretical curve obtained us-
ment. ing the average parameter values given
We used this two compartment above. The results are shown in (Figure 5,
model to obtain kinetic parameters from p. 205). Clearly, there was excellent agree-
each of the in vivo vitamin C experiments ment between the theoretical curve and
where sufficient time-concentration data the recent data, suggesting the ascorbate
were obtained. We first fitted all four pa- pharmacokinetics for this subject were the
rameters, then fixed the blood plasma same over the three month treatment pe-
volume at 30 dL (near the average value riod. This further supports the conclusion
for all experiments) and floated the three that the ascorbate transport parameters
K values. Results are given in Table 1 for a given subject remain relatively con-
(p.204). The average parameter values for stant during the time of treatment.
Figure 3. Two compartment model.
Injection Plasma Injection
G(t) VP, CP(t) Kx
K2 K1
Tissue
QT(t)
203Journal of Orthomolecular Medicine Vol. 15, No. 4, 2000
Table 1. Ascorbate pharmacokinetics in vivo.
Date 5/29/97 6/4/97 6/5/97 6/11/97 6/12/97 6/18/97 6/19/97 6/25/97 6/26/97
Dose (g) 15 30 60 30 60 65 65 65 65
Infusion 45 80 160 40 80 60 60 60 60
min
Kx (min -1) 0.026 0.027 0.024 0.025 0.022 0.025 0.022 0.023 0.027
excretion
K1 (min-1) 0.195 0.214 0.653 0.307 0.124 0.447 0.200 0.150 0.884
tissue adsorb
K2 (min-1) 0.066 0.060 0.165 0.091 0.038 0.141 0.062 0.040 0.235
tissue efflux
K2/K1 0.337 0.279 0.253 0.296 0.302 0.317 0.310 0.265 0.266
efflux/adsorb
Max CP 125.7 186.1 285.3 233.3 417.8 458.4 495.0 472.8 397.2
mg/dL
Ave. (1-8hr) 37.3 70.6 150.1 76.0 165.4 167.6 185.4 221.5 151.9
CP mg/dL
Table 2. Average parameter values.
Parameter Mean SD
Kx 0.025 0.002
K1 0.353 0.261
K2 0.100 0.067
K2/K1 0.292 0.028
Computer Protocol Simulations A) 1 hour at 60 g/hr
A program was then constructed to B) 2 hours at 60 g/hr
predict the plasma ascorbate levels in vari- C) 1 hour at 60 g/hr, then 6 hours at 10 g/hr
ous protocols based on the pharmaco-ki- Predicted plasma ascorbate levels
netic parameters obtained above. Three for these protocols are shown in Figure 6
protocols were simulated: (p.206). Prolonged infusions at higher
204Clinical and Experimental Experiences with Intravenous Vitamin C
Figure 4. Pharmacokinetic variation in parameter values over time.
Figure 5. Plotted data points from three recent studies against the
theoretical curve based on figure four values.
500
450
400 Cp(data)
Plasma Ascorbate (mg/dL)
Cp (calc)
350
300
250
200
150
100
50
0
0 60 120 180 240 300 360 420 480 540
Time (min)
doses obviously give the highest peak val- Effects of Human Serum Obtained from
ues, while a “trickle” infusion can be used Subject Receiving Intravenous Vitamin C
to maintain plasma levels at a desired level. on Tumor Cell Growth
This computer simulation can be a To study more closely the probability
useful tool for examining what plasma of in vivo cytotoxic effects of intravenous
levels we can expect from various vitamin C we planned and performed the
protocols, once the pharmacokinetics for following experiment. Dense monolayers
a given subject are known from an ini- of human prostate tumor cells (PC-3 from
tial experiment. ATCC) were created in microplates. A pa-
205Clinical and Experimental Experiences with Intravenous Vitamin C
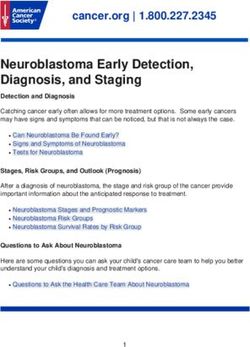
Figure 7. Effects of human serum removed from patient before and at intervals
after intravenous infusion of vitamin C (60 grams) on cultured human
prostate tumor cells.
120.00 700
600
100.00
500
80.00
Survival % (bars)
400
60.00
300
40.00
200
20.00 100
0.00 0
T=0 T=35 T=65 T=95 T=125 T=185 T=245 T=305
Time (min)
tient with carcinoma of the prostate was ter the beginning of the IV vitamin C. Dur-
given 65 grams of intravenous vitamin C ing those periods the serum concentration
(in 500 cc sterile water for injection) over was greater than 400 mg/dL. After that time
65 minutes. Serum separator blood tubes the toxicity decreased. The last sample
were drawn before the infusion and at in- taken (vitamin C concentration 213 mg/dL)
tervals thereafter from a heparin lock sepa- resulted in 64% inhibition compared to the
rate from the infusion site. The final blood controls.
draw was five hours after the infusion be-
gan. Some of the collected serum was then Potentiation of Preferential Toxicity of
tested for vitamin C concentration, and the Vitamin C
rest was heat-inactivated and used as cul- Because plasma concentrations of vita-
ture media for the prostate tumor cells. The min C of greater than 200 mg/dL are prob-
cells were incubated for five days when the lematic to maintain, we began looking for
numbers of viable tumor cells were deter- ways to increase the sensitivity of tumor cells
mined using a previously described to vitamin C. During experimentation we
carboxy-fluorescein diacetate/microplate found that lipoic acid (a water and lipid solu-
fluorometer viable cell determination ble antioxidant that recycles vitamin C) can
method. The results of the experiment are enhance the tumor toxic effects of vitamin
graphed in Figure 7 (p.207). Greater than C. Figure 8 (p.208) illustrates dose response
97% cytotoxicity was observed for the serum of tumor cells in a hollow fiber tumor model
samples taken at 35, 65, and 95 minutes af- exposed to vitamin C with and without lipoic
206Journal of Orthomolecular Medicine Vol. 15, No. 4, 2000
Figure 8. Effect of lipoic acid on ascorbate efficiency: SW620 human colon
carcinoma cells grown as hollow fiber solid in vitro tumors exposed for 48 hours to
sodium ascorbate alone or in combination with lipoic acid sodium (combo 10:1).
1.2
1.0
0.8
Survival Fraction
0.6
0.4 Ascorbate
Combo 10:1
Ascorbate
0.2 LC50 = 700 mg/dL
Combo (10:1)
LC50 = 120 mg/dL
0
10 102 103 104
acid. Lipoic acid decreased the dose of vita- mented cultured tumor cells with vita-
min C required to kill 50% of the tumor cells min C concentrations that are achievable
from 700 mg/dL to 120 mg/dL. with oral supplementation (2 and 4 mg/
dL) and measured the collagen produced
Effects of High-Dose Vitamin C on using a well-known method.5 We found
Tumor Cell Collagen Production that indeed, these concentrations of vi-
It is well known that vitamin C is re- tamin C greatly increased the production
quired for the hydroxylation of proline, and of collagen. Data are summarized in Fig-
that low levels of vitamin C can be a lim- ure 9, p.209. It is interesting to note that
iting factor in the production of colla- when we performed cytotoxicity assays
gen. Because many tumor cells produce of vitamin C against the PC-3 human
collagenase and other proteolytic en- prostate carcinoma cell lines using con-
zymes, we wanted to determine if vita- centrations as high as 300 mg/dL, we
min C supplementation would increase were unable to detach remaining live cells
collagen production by tumor cells, from the tissue culture f lasks using
thereby having a balancing effect on col- trypsin/EDTA. In some cases several
lagenase. In an experiment, we supple- days of treatement with high concentra-
207Journal of Orthomolecular Medicine Vol. 15, No. 4, 2000
Figure 6. Theoretical blood ascorbate levels.
700
A 1 hour at 60 g/hr
600 B 2 hours at 60 g/hr
C 1 hour at 60 g/hr
Plasma Ascorbate (mg/dL)
500 then 6 hours at 10 g/hr
400
300
200
100
0
0 200 400 600
Time (min)
tions of collagenase were required to Patients with Renal Cell Carcinoma
detach the cells. One of us remembers Treated with Intravenous Vitamin C
literally “chipping” cells off the plastic One of us (HDR) reported positive ef-
flasks. Prostate tumor cells are very re- fects of vitamin C therapy in a patient with
sistant to high doses of vitamin C. It may adenocarcinoma of the kidney in 1990.4
be that they are so rapidly using the vita- This report described a 70-year-old white
min C for collagen production that it male diagnosed with adenocarcinoma of
doesn’t have as much residence time as in his right kidney. Shortly after right ne-
other cell lines, and is therefore less toxic. phrectomy, he developed metastatic le-
Of clinical note is that we have several pa- sions in the liver and lung. The patient
tients diagnosed with prostate cancer who elected not to proceed with standard meth-
have taken continuous large oral doses of ods of treatment. Upon his request, he
vitamin C for many years and do not began intravenous vitamin C treatment,
progress to metastatic disease, despite a starting at 30 grams twice per week. Six
relatively large intracapsular tumor bur- weeks after initiation of therapy, reports
den. Perhaps their tumor cells are “gluing indicated that the patient was feeling well,
themselves” in place by high collagen pro- his exam was normal, and his metastases
duction. were shrinking. Fifteen months after ini-
tial therapy, the patient’s oncologist re-
Clinical Experiences ported the patient was feeling well with ab-
We have not observed toxic reactions solutely no signs of progressive cancer. The
to high-dose intravenous vitamin C. All patient remained cancer-free for 14 years.
patients are pre-screened for glucose-5- He died of congestive heart failure at the
phosphate dehydrogenase deficiency. age of 84. A second case study, published
208Clinical and Experimental Experiences with Intravenous Vitamin C
Figure 9. Effects of Vitamin C supplementation on collagen production by
tumor cells.
30
25
Collagen (ug/well)
20 PC-3 pancreatic tumor
cells
15
Ovarian tumor cells
10
5
0
0 2 4
Ascorbic Acid added to Culture Media (mg/dL)
in 1998,5 described another complete remis- nutritional supplement. A radiology report
sion in a patient with metastatic renal cell on a chest x-ray taken January 15, 1998, stated
carcinoma. The patient was a 52-year-old that no significant infiltrate was evident, and
white female from Wisconsin diagnosed there was resolution of the left upper lobe
with non-metastatic disease in September lung metastasis. In February, 1999 a chest x-
1995. In October 1996, eight metastatic ray showed no lung masses, and the patient
lung lesions were found: seven in the right reported being well at that time.
lung and one in the left (measuring be-
tween 1-3 cm). The patient chose not to Combined Intravenous Vitamin C and
undergo chemotherapy or radiation treat- Chemotherapy in a Patient with Stage IV
ments. The patient was started on intra- Colorectal Carcinoma
venous vitamin C and specific oral nutri- In April, 1997, a 51-year-old white male
ent supplements to correct diagnosed de- from Wichita, Kansas was first seen at our
ficiencies and a broad-spectrum oral nu- center. He was well other than having type
tritional supplement in October, 1996. The II diabetes until the previous fall when he
initial dose of intravenous vitamin C was developed painless bright red rectal bleed-
15 grams, subsequently increased to 65 ing. A work-up demonstrated the presence
grams after two weeks. The patient was of a distal colon lesion. On December 31,
given two infusions per week. Intravenous 1997 he underwent an anterior colon re-
vitamin C treatments were continued un- section and appendectomy at a local hos-
til June 6, 1997. An x-ray taken at that time pital. The colon tumor penetrated through
revealed resolution of all but one lung the bowel wall and into the surrounding
metastases. The patient discontinued intra- pericolonic adipose tissue. Two large he-
venous vitamin C infusions at that time and patic metastases were discovered at the
continued taking the broad-spectrum oral time of surgery; one was biopsied. Pathol-
209Journal of Orthomolecular Medicine Vol. 15, No. 4, 2000
Figure 10. Patient with cancer of the pancreas.
8000
7000
6000
CA-19-9 Tumor Marker
5000
4000
3000
2000
1000
0
12/1/96 3/11/97 6/19/97 9/27/97 1/5/98 4/15/98 7/24/98
Date
ogy revealed that the colon lesion was a from the stomach wall and liver. Segments
moderately differentiated adenocarcinoma, three and five both contained multiple nod-
and the liver biopsy was metastatic adeno- ules. His CEA was 9.8 post surgery. The
carcinoma. Following surgery he received Pittsburg University oncologist informed
chemotherapy with weekly 5-FU and leu- him his prognosis was very poor and that
covorin for twelve cycles with a decrease he should go home and begin chemotherapy
in his CEA from 90.2 to 67.7. The patient again. He and his wife asked this oncologist
and his wife, who is an R.N., asked the if he should use intravenous vitamin C. He
chemotherapist about getting intravenous responded, “I know of no studies which
vitamin C along with the chemotherapy. showed that this [vitamin C] would eradi-
The oncologist informed them that vitamin cate or delay progression of cancer.”
C would not be of any value. In spite of the two no-confidence rec-
The patient was then seen at Pittsburg ommendations for the use of intravenous
University hospital on May 13, 1997 where vitamin C, The patient returned to our
he underwent liver resection to segments center for infusions after recovering from
three and five. During surgery, the stom- surgery in June, 1997. He also began re-
ach was mobilized off the inferior surface ceiving weekly 5-FU (1100 mg) and Leu-
of the liver and a frozen section of this area covorin (1300 mg) treatments adminis-
was taken and confirmed metastatic ad- tered by his local oncologist. His first vita-
enocarcinoma. The pathology report min C infusion was 15 grams over one hour.
showed metastatic carcinoma consistent The dose was gradually increased during
with colon primary within the desmoplas- bi-weekly infusions. On September 9, 1997,
tic tissue and adjacent hepatic parenchyma a post-intravenous vitamin C (100 gram in
210Clinical and Experimental Experiences with Intravenous Vitamin C
1000 cc sterile water infused over 2 hours) disappeared upon reinstatement of vitamin
plasma concentration of vitamin C was 355 C infusions; and 4) For this patient intra-
mg/dL. He was then started on intrave- venous vitamin C did not work against the
nous vitamin C, 100 grams, twice weekly. His chemotherapy, as demonstrated by his
wife gave most of these infusions at home. complete remission.
In addition to the vitamin C, he was given Combined Intravenous Vitamin C and
recommendations for oral vitamin and min- Chemotherapy in a Patient with Carcinoma
eral supplementation to increase levels of of the Pancreas
nutrients that he was found to be low in. In October 1997, a 70-year-old white
He kept up his vitamin C infusions until male from Southeastern Kansas was first
February, 1998 when he traveled to Florida seen at our center. After exploratory sur-
for a vacation. While on vacation he con- gery in December 1997 he had been diag-
tinued the 5-FU/Leucovorin injections. Af- nosed with a low-grade mucinous carci-
ter a two weeks hiatus from the vitamin C noma of the pancreas. During surgery there
infusions he began to experience nausea, was found to be widely metastatic disease
diarrhea, stomach pain, and stomatitis; com- affecting all intra-abdominal organs. In
mon side effects of 5-FU. The side effects January 1997 he was started on Gemzar. He
stopped when he restarted intravenous vi- had an allergic reaction to Gemzar and was
tamin C. He continued on chemotherapy placed on weekly 5-FU for 9 weeks. He was
and 100 gm bi-weekly intravenous vitamin placed back on Gemzar in June, 1997 along
C until April 1, 1998. Other than the brief with Decadron to counteract his allergy. In
period of side-effects mentioned above, he spite of chemotherapy his CA-19-9 contin-
had no other side effects during the year of ued to elevate until he was seen at our
chemotherapy. He never experienced center. At that time his CA 19-9 was 7400
leukopenia, thrombocytopenia, or anemia. U/mL (normalJournal of Orthomolecular Medicine Vol. 15, No. 4, 2000
active again. The evidence also suggest hood would have been curative. She also
that intravenous vitamin C was working had a so-called recurrence of her lym-
independently of the chemotherapy given phoma during intravenous vitamin C
the CA-19-9 level continued to decrease therapy months after her radiation
after chemotherapy was discontinued. therapy had ended. The possibility exists
This patient died at home on July 4th, that the lymphoma cells in her lymph
1998. nodes were there at the initial diagnosis
and the adenopathy occurred during im-
Resolution of non-Hodgkin’s Lym- mune recognition of those cells. Also of
phoma with Intravenous Vitamin C-2 note is the fact that this patient received
Cases only 15 grams of vitamin C per infusion.
A 66 year old white female was diag- According to our model, this in not a high
nosed with a large peri-spinal (L4-5) ma- enough dose to achieve cytotoxic concen-
lignant, non-Hodgkin’s lymphoma (diffuse trations of vitamin C in the blood. There-
large cleaved cell of B-cell lineage) in Janu- fore, any effect of vitamin C could only be
ary, 1995. Her Oncologist recommended attributed to its biological response modi-
localized radiation therapy and fication characteristics.
Adriamycin-based chemotherapy. She be- In Fall 1994 a 73-year-old white male
gan localized radiation therapy five days farmer from Western Kansas was diagnosed
per week for five weeks on 1/17/95, but with wide-spread non-Hodgkin’s lym-
refused chemotherapy. On 1/13/95 she phoma. Biopsies and CT-scan revealed bi-
was started on intravenous vitamin C, 15 lateral tumor involvement in his anterior
grams in 250 cc Ringer’s Lactate two times and posterior cervical, inguinal, axillary and
per week which she continued after com- mediastinal lymph node beds. Bone mar-
pleting the radiation therapy. She also row aspirate was negative for malignant
began taking several oral supplements to cells. He was treated with chemotherapy for
replace those found to be deficient by 8 months that resulted in remission. In July,
laboratory testing, and empirical co-en- 1997 he began losing weight (30 lbs). He re-
zyme Q10, 200 mg BID. She was also suc- turned to his oncologist and a CT-scan at
cessfully treated at that time for an intes- that time showed recurrence. He was placed
tinal parasite. On May 6, 1995 she returned on chemotherapy in September, 1997. In De-
to her oncologist with swelling and pain- cember, 1997 he developed leukopenia and
ful supraclavicular lymph nodes. One then extensive left sided Herpes Zoster. As
lymph node was removed and found to a result the chemotherapy was stopped. In
contain malignant lymphoma cells. In March, 1998 he became a patient at our
spite of recommendations for chemo- Center and began receiving intravenous vi-
therapy and more radiation, she refused tamin C and oral nutrient supplements in-
and continued with her intravenous vita- cluding lipoic acid. His vitamin C dose was
min C and oral regimen. Within six weeks escalated until he was receiving 50 grams
the supraclavicular nodes were barely no- in 500 cc sterile water two times per week.
ticeable. She continued intravenous vita- He continued on that dose for 11 months.
min C infusions until December 24, 1996. Three months after beginning vitamin C
She has been followed with regular physi- therapy a CT-scan showed no evidence to
cal exams and has had no recurrence. malignancy. Another CT-scan in February,
During a telephone follow-up on 3/23/99 1999 was also clear and he was declared to
she was well without recurrence. Com- be in complete remission by his oncologist.
ment: This case is rare–the patient re- Also of note is that this patient was ad-
fused chemotherapy, which in all likeli- dicted to sleeping pills when first seen at
212Clinical and Experimental Experiences with Intravenous Vitamin C
our center. After three months of intrave- plasma concentrations of vitamin C using
nous vitamin C therapy he replaced the varied infusion protocols. Lipoic acid en-
sleeping pills with Kava tea. hances vitamin C induced tumor cell tox-
Intravenous Vitamin C in a Patient with icity. Vitamin C in blood concentrations
End-Stage Metastatic Breast Carcinoma achievable through oral supplementation is
In 1995 a hospitalized 68 year old capable of increasing collagen production
women with widely metastatic end-stage by tumor cells. Vitamin C in doses up to 50
breast cancer was seen.6 Her latest bone grams per day, infused slowly, are not toxic
scan showed metastases to “nearly every to cancer patients. Some cancer patients
bone in her skeleton.” She was experienc- have had complete remissions after high-
ing bone pain which was not controlled dose intravenous vitamin C infusions. Con-
with narcotics. At the time of her first con- centrations of vitamin C that kill most
sultation she had blood clots in both sub- tumor cells are not achieved after infusion
clavian veins, and shortly thereafter con- of 30 grams of vitamin C. Therefore, re-
tracted cellulitis in her left arm and hand missions in patients treated with this dose
secondary to an errant arterial blood draw. of vitamin C are likely to have occurred as
After the blood clots were treated with a result of vitamin C induced biological
Activase R, she was placed on intravenous response modification effects rather than
vitamin C, 30 grams per day intially, in- its cytotoxic effects.
creasing to 100 grams per day over five
hours. Within one week, the once bed- References
bound patient began walking the halls of 1. Benade L, Howard T, Burk D: Synergistic kill-
the hospital. Several hospital staff reported ing of Ehrlich ascites carcinoma cells by ascor-
that she looked like a new person. Her cel- bate and 3-amino-1, 2, 4-triazole. Oncology,
1969; 23: 33-43.
lulitis cleared, and she was discharged from 2. Maramag C, Menon M, Balaji KC, Reddy PG,
the hospital. At home she received 100 Laxmanan S: Effect of vitamin C on prostate
grams of intravenous vitamin C three times cancer cells in vitro: effect on cell number, vi-
per week. Three months after starting the ability, and DNA synthesis. Prostate, 1997; 32:
vitamin C therapy a bone scan revealed 188-95.
resolution of several skull metastases. Six 3. Riordan NH, et al: Intravenous ascorbate as a
tumor cytotoxic chemotherapeutic agent. Med
months after starting the vitamin C, she fell Hypoth, 1994; 9: 207-213.
while shopping at a mall, and subsequently 4. Riordan HD, Jackson JA, Schultz M: Case study:
died of complications from pathological High-dose intravenous vitamin C in the treat-
fractures. ment of a patient with adenocarcinoma of the
kidney. J Orthomol Med, 1990; 5: 5-7.
5. Riordan HD, Jackson JA, Riordan NH, Schultz
Conclusion M: High-dose intravenous vitamin C in the
We have presented evidence that vita- treatment of a patient with renal cell carcinoma
min C may be useful in the treatment of of the kidney. J Orthomol Med, 1998; 13: 72-73.
cancer. In particular we have produced the 6. Riordan N, Jackson JA, Riordan HD: Intravenous
following evidence: Vitamin C is toxic to vitamin C in a terminal cancer patient. J
tumor cells. Concentrations of vitamin C Orthomol Med, 1996; 11: 80-82.
that kill tumor cells can be achieved in
humans using intravenous vitamin C infu-
sions. Infusion of a bolus of vitamin C fol-
lowed by slow infusion can result in sus-
tained concentrations of vitamin C in hu-
man plasma. Modeling of vitamin C phar-
macokinetics can accurately predict
213You can also read