CARE AND PUBLIC HEALTH RESEARCH INSTITUTE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CARE AND PUBLIC HEALTH RESEARCH INSTITUTE
Strategic choices 2018-2022
The attention to care and public health research seems to be on the rise. Last year, the US National Academy of
Medicine launched a policy initiative called ‘Vital Directions for Health & HealthCare’ in which 19 priority focus
areas were defined, many of which are directly relevant for CAPHRI. Also, the Dutch election programs, the
National Science Agenda (NWA) (which puts special emphasis on healthcare research, prevention and treatment),
the taskforce Prevention NWA, the ZonMW initiatives on Personalised Care and the Dutch Health Council Report
on ‘Research that makes you better’ all seem to indicate this renewed interest in care and public health research.
Overall then the zeitgeist is good for CAPHRI research but we need to remain focused on the changing landscapes
in our environment. For example, between now and 2022 we foresee the continued rise of ‘big data’, e-health and
precision medicine, democratisation of professional knowledge, further resource restraints in healthcare,
increasing super-specialisation and counterbalancing need for generalists, complexity and fragmentation of care,
migration and demographic change due to low fertility and ageing populations, more complex extramural and
home care, increased comorbidity among the elderly, increased numbers of people with functional limitations and
chronic disease, growing inequalities, the transformation of the welfare state into a participation state, the rise of
populism and the growing distrust of institutions, including our own academic institution. These developments will
create a new relation between society and health (care). As a School we are, and should be, involved in
researching and shaping this relationship.
In the last 2 years we have also observed changes in the research climate, such as the shift from governmental and
charity funding to public-private funding opportunities, increased competition of researchers due to fewer
available resources, increasing demand for distance PhD programs to build research capacity at local institutes and
a mismatch of current performance indicators to reflect societal relevant research.
CAPHRI is committed to facilitate and stimulate our professional staff and their career span. The current
developments have made us to reflect on our School strategy and we propose new initiatives that can help CAPHRI
researchers to keep excelling in care and public health research during the next 5 years and as such contribute to a
better society.
For the long-term strategy (>10 years), we see that medicine and life sciences are undergoing a conceptual
revolution moving away from healing the sick (20th century) to upgrading the healthy (21st century). These
developments are moving towards an ever-increasing attention to prevention and health, functioning and
wellbeing. For better or worse, we also see medicine and life sciences are moving away from benefiting the masses
to benefiting the individual, of which medicine and data science could be a present-day example. After 2022,
CAPHRI may need to re-focus towards stimulating ‘optimizing health’ instead of only on the integrated care chain,
and towards personal health instead of only public and global health.
Page 1
See appendix A for strategy operations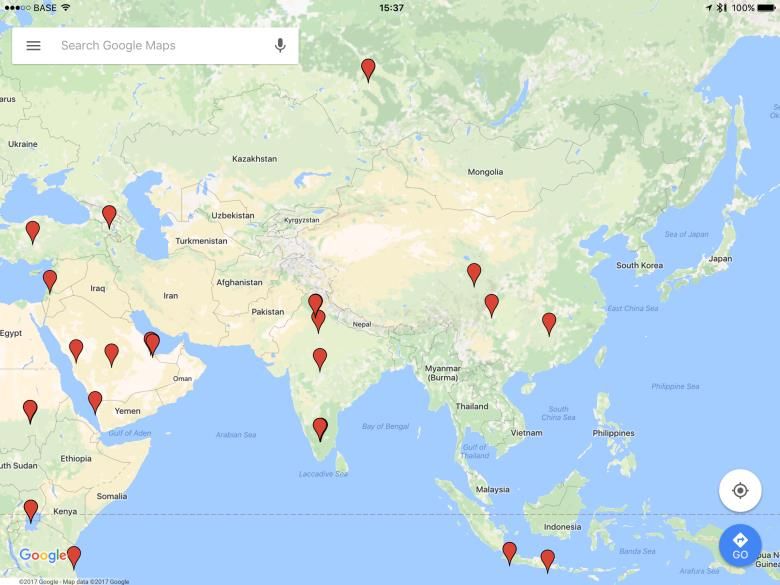
Figure 1: CAPHRI Governance
Maastricht University
Maastricht University (UM) was founded in 1976 and is the youngest university of the Netherlands. UM, the most
international university in the Netherlands, with currently 51% international students and is characterized by its
multidisciplinary and thematic approach to research and learning. It is the best performing young university (under
50 years old) from the Netherlands. In the 2018 ‘QS Top 50 Under 50’ rankings, UM is the 13th best young
university worldwide. In the latest ‘Times Higher Education (THE) 250 under 50’ ranking, (2018) UM is placed
5thworldwide. In the latest THE overall World University Rankings UM scores 103rd place (out of 1102 universities).
In the CWUR by subject (2017), UM ranks world nr. 1 in ‘Education, scientific disciplines’ and nr. 8 in Primary
Health Care (figure 2).
Faculty of Health, Medicine and Life Science
The Faculty of Health, Medicine and Life Sciences (FHML) is UM’s largest faculty, comprising 70% of the total staff
and budget of Maastricht University. The FHML officially exists since January 1st, 2007 after a merger of the former
faculties of Health Sciences and Medicine. In 2008, the FHML has joined a cooperative alliance with Maastricht's
academic hospital under the name Maastricht University Medical Centre+ (Maastricht UMC+). It is a centre for
integrated research and education that covers the entire spectrum of the health sciences, medicine and molecular
life sciences. The ‘+’ added to the name is an expression of its additional focus on health instead of (only)
medicine.
In the FHML Graduate Schools, Masters’ students, PhD candidates and researchers work together. In addition to
research, the Schools are responsible for training PhD candidates. Master-level education is coordinated by the
educational institute. In addition to the Graduate School CAPHRI, the FHML also houses CARIM - School for
Page 2
See appendix A for strategy operations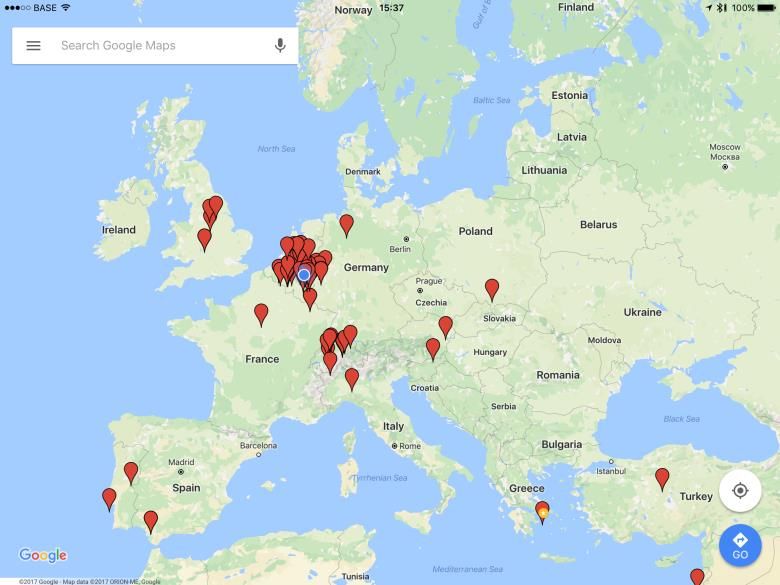
Cardiovascular Diseases, GROW - School for Oncology and Developmental Biology, NUTRIM - School of Nutrition
and Translational Research in Metabolism, MHENS - School for Mental Health and Neuroscience, and SHE - School
of Health Professions Education and the institutes M4I - Maastricht
Care and Public Health Research Institute
The School CAPHRI was formed after a 2003 merger of the School EXTRA that focused on primary care and
extramural care research and the School HEALTH that had a focus on public health research. The more than 300
employees and almost 400 PhD candidates are based at 11 core departments (majority of staff is funded by
CAPHRI) and at the 5 associated departments (figure 2). In 2016, CAPHRI has changed its name from ‘School for
Public Health and Primary Care’ to ‘Care and Public Health Research Institute’ to better reflect its evolution
towards research along the care chain.
CAPHRI Staff # / fte International Reviewed Publications PhD Theses
Scientific staff: 143 / 53,3 FHML: 3.051 (2017) FHML: 236 (2017)
Post-docs: 61 / 35,7 CAPHRI: 881 (2017) CAPHRI: 64 (2017)
Internal PhD-candidates: 76 / 70,3 29% 27%
External PhD-candidates: 320
Support staff: 52 / 32,9
UM: Dutch ranking (2016) UM: UM: CWUR, by subject (2017)
Elsevier: 3rd THE World University Ranking (2018) Education, scientific disciplines: 1st
Overall: 103th Primary Health Care: 8th
THE ‘250 under 50’ ranking (2018)
5th best young university
Figure 2: At a glance
Vision
A healthy society for everyone.
Mission
To conduct high-quality research in care and public health with societal relevance.
Values
We Care 4 Health and wellbeing
(Public) Health, care and wellbeing are crucial elements of resilient individuals and successful societies.
We value cooperation and inclusion
It is our conviction that innovations take place when people from different backgrounds, perspectives and
capabilities meet and converge.
Our research has societal relevance
Although generating new knowledge is important in its own right, we foster dissemination to society through
publications, public education and applications. Research that has no societal relevance does not belong to
CAPHRI.
Page 3
See appendix A for strategy operations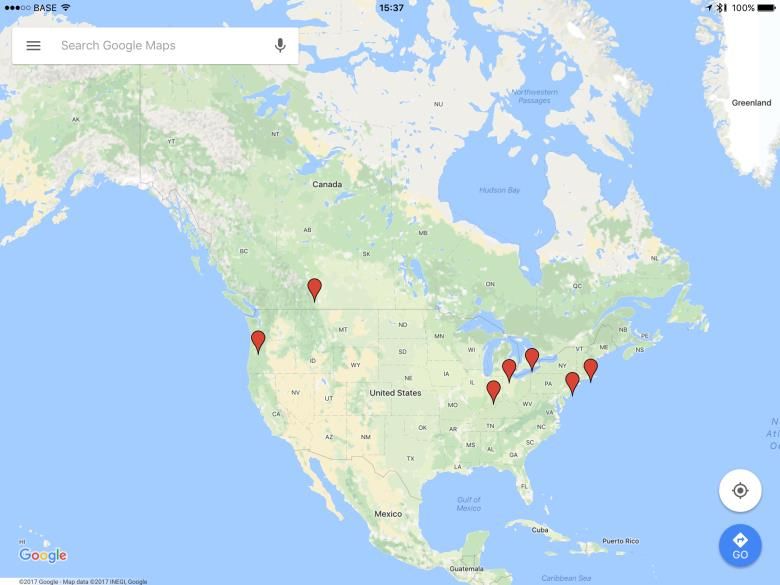
Strategy
We help scientists to reach their highest ambition in care and public health research
We are the natural academic partner for care and public health challenges in our region and beyond
Table 1. Our Strategy
Aspiration 1
We help our scientists to reach their highest ambition in care and public health research
1.1 Our research is interdisciplinary and focused
1.2 Our infrastructure facilitates high quality research
1.3 Our research is driven by society
1.4 We take care of our staff
1.5 We provide high quality training for our researchers.
Aspiration 2
We are the natural academic partner for care and public health challenges in our region and beyond
2.1 We connect to other groups within MUMC+ and Maastricht University
2.2 We contribute to a healthy society in Limburg and the Netherlands
2.3 We are a globally connected European School that is anchored in the EU-region
2.4 We are visible and attractive
Page 4
See appendix A for strategy operations
Aspiration 1
We help our scientists to reach their highest ambition in care and public health research
1.1 Our research is interdisciplinary and focused
CAPHRI is organised along six thematic oriented research lines (RL) in which researchers from different
departments operate together in multidisciplinary teams. Each RL contributes to both public health and health
care innovation albeit in different proportions. Each RL consist on average 36 (13 fte) senior research employees
and 64 PhD candidates. They have subsequently developed their own vision, mission and strategic plans that
contribute to the overall School direction. Their mission statements are summarized below. The research lines are
expected to further prioritise future appointments to develop into unique, albeit strongly connected, research
units . Only in identity new connections can be made.
Inequity, Participation and Globalisation (IPG)
Keywords: Inequity, Participation, Globalization
Take home message: We are dedicated to unravel the dynamics between health capabilities, inequity,
participation and globalization in local and regional settings and across the globe
Mission: To unravel the historically shaped entanglements of inequities, participation and globalisation in various
public health practices, geographic regions and cultural settings, including those related to (re)emerging health
threats like infectious diseases and antibiotics resistance. As such, we will contribute to the identification of
effective, legitimate, and just solutions and policies.
Creating Value-based Health Care (VHC)
Keywords: Organization, Policy and Economics
Take home message: We focus on the organization, economics, policy and governance of health care innovation in
the whole continuum of care from a regional, national and international perspective
Mission To contribute to the improvement of population health and wellbeing through better health systems,
services and products in all areas of the health care chain. We conduct research in order to innovate and create
value at a macro, meso and micro level, balancing societal, organizational and personal values in a reality of
scarcity.
Promoting Health and Personalised Care (PHPC)
Keywords: Promoting Healthy Choices
Take home message: Our research concerns prevention and care in public health, clinical and policy settings from
a motivational, behavioural and participatory perspective
Mission: To develop new theories, interventions and research methods to promote health and personalised care
involving shared decision making principles and to recognise that personalisation and tailoring of prevention and
care involves active participation and normative reflections of all stakeholders, such as healthy persons, patients,
health care professionals, scientists, and health care policy makers.
Optimizing Patient Care (OPC)
Keywords: Primary Care and Integrated Care
Take home message: We use epidemiologic methods to improve diagnostic and prognostic evaluation and
interventions in patients in primary and integrated care
Mission: To develop optimal evidence-based and knowledge-informed patient care ranging from prevention and
lifestyle and early diagnosis to management/prognosis. Our approach is based on the translational concept,
meaning exploitation of basic research leading to patient-oriented clinical science. Our mission is to investigate the
incremental value of prevention and lifestyle, including nutrition, early diagnosis and management and the
underlying molecular mechanisms in a patient-centred approach.
Page 5
See appendix A for strategy operationsFunctioning and Rehabilitation (FR)
Keywords: Functioning, Participation, Context
Take home message: We cover the continuum of research into functioning and participation of individuals in
society, and herein the role of the personal and environmental context
Mission: To optimize and foster functioning and participation of individuals in society throughout the lifespan of
individuals by developing and evaluating strategies for prevention, diagnosis, prognosis and treatment of persons’
health impairments and societal/labor participation restrictions.
Ageing and Long-Term Care (Alt-C)
Keywords: Ageing and Long-term Care
Take home message: We are focused on the development, evaluation and implementation of innovative health
care programs for older people in long-term care
Mission: The mission in this RL is twofold. Firstly, to develop and disseminate knowledge and expertise on
psychosocial, clinical and environmental determinants of health care problems including its prevalence, need of
care, societal participation, independency and quality of life among older persons. And secondly, to develop and
evaluate innovative health care programs, research methods and interventions for and with older persons to slow
down processes of disablement and to improve the quality of particularly long-term care.
1.2 Our infrastructure facilitates high quality research
CAPHRI has a consistently high quality research output (figure 2), no matter whether it is measured in earning
power (appr. 18M per year), the number of international refereed publications (appr. 800 per year) or the number
of PhD graduates (appr. 50 per year). We aim to have systems in place to facilitate and support high quality
research and help researchers to bring out the best in themselves. This includes increasing our support staff
appointments to a 1 to 3 ratio compared to academic appointments , we provide a suitable infrastructure for
methodology support and by providing researchers automated tools to monitor progress on their publication
output (PURE) or the quality of their PhD Supervision (TRACK). We have initiated a life feedback loop system
(DASHBOARD), where researchers can compare their own output against the average of others at different levels
of the organisation. This is being adopted on the Faculty level. To counteract possible inverse incentives due to the
use of only quantitative research metrics, the DASHBOARD will also include qualitative parameters such as marks
of recognition, use of research products, societal impact, portfolio input and will use field normalization .
The RLs have been given a high level of responsibility to give strategic advice regarding staff or investments. The
School will provide a guideline on how to make these strategic advices
CAPHRI has established a management office that provides support to individual researchers, departments and
research lines on practical, administrative, legal and financial matters regarding all aspects of the research
enterprise. This includes staff management (tenure, non-tenure & support staff), accounting, project acquisition
and financial project management.
CAPHRI provides a 13k euro bonus system per graduated PhD for the supervisory team , with an extra 5k euro
provided by the FHML faculty if the PhD project is finished within 4 years. CAPHRI’s Committee for Scientific
Grants and Fellowships’ (figure 1) provides researchers with feedback on grant applications and scans for grant and
award opportunities for the CAPHRI staff. Although CAPHRI staff is currently well represented in the national and
international funding and advisory committees, the participation in such committees will become a standard item
in annual review meetings and planning and control cycles .
CAPHRI hosts a variety of academic partnership agreements with institutes in the region and beyond (see 2.3) that
creates opportunities for PhD candidates and staff from both partner institutes. We would like to build further on
these infrastructures and expand partnerships from trusted relationships and increase our number of ‘preferred
partners’ . Future academic partnerships will further strengthen CAPHRI’s influence, reach and reputation in care
and public health research.
Page 6
See appendix A for strategy operationsIn addition to research output, we pay equal attention to the quality of our products and processes. CAPHRI has
therefore established a new quality system, will appoint a quality officer and will develop a quality handbook for
research conduct and auditing . This includes reducing research that does not generate new knowledge (research
waste), establishing procedures to ensure that CAPHRI adheres to the institutional, national and European codes of
Research Integrity and involving CAPHRI staff in UM data security initiatives CAPHRI will quickly adopt all
University- and Faculty-level data privacy and data infrastructure initiatives.
A substantial part of research within CAPHRI makes use of large scale follow-up research studies, such as cohort
studies (e.g. the Maastricht Cohort Study on Fatigue, the Koala Birth Cohort Study, the Maastricht Study etc.).
CAPHRI will lead an cohort working group, which will develop a policy aimed at fostering and facilitating these
unique cohorts and stimulate new data infrastructure initiatives. All other Schools of FHML are represented in this
working group.
To ensure CAPHRI’s financial sustainability in an ever-increasing resource constraint environment, the School will
invest in becoming less dependent on government and Faculty funding by creating new opportunities for income.
The School will therefore stimulate commercial innovation such as contract research, monetisation of existing
datasets and entrepreneurship (start-up, scale-up). This is realistic (given that UM has joint a partnership with
Brightlands) but it is also an unexplored ambition of our School. In 2017, CAPHRI has appointed an EiT Health
Officer that will act as a liaison between researchers and industry and from 2018 we investigate an incentive
system for intrapreneurial initiatives, that are innovative, have some risk of failure but could develop a new
revenue stream for the School .
1.3 Our research is driven by society
CAPHRI purposefully tries to build a bridge between our research and society. Our work is used as a basis for
clinical or policy guidelines; our research facilities are being used by many societal groups, including healthcare
institutes in our region (figure 1); we not only publish in scientific journals but also in professional journals, books
or via the press, which is monitored and valued by the School and we stimulate the co-creation of inventions.
As from 2019 CAPHRI will incorporate societal impact as one of the key performance indicators in the evaluation of
research lines based on which, among others, staff allocation will be decided . The purpose of the next period is
to involve more stakeholders and to increase the visibility of research across all research lines. National funding for
research has stagnated and varies stakeholders are lobbying for 1billion extra government investment in R&D.
Community support for a knowledge economy essential for this. This is especially important in our province where
the health status of the population is among the nation lowest and the local economy depends largely on the
existence of the university. In the next period, we therefore aim to make a next step and will change our focus to
‘anchoring’ and ‘co-creation’ with our community through practical applications, publications and public
education. As from 2020 CAPHRI will participate in Mosae Vita, a large-scale citizen participation initiative and
public-access building with a focus on healthy living . Our societal responsibility also includes duties towards our
employees (paragraph 1.4) and ethical considerations, e.g. to protect research integrity also if this reduces output
(paragraph 1.2)
1.4 We take care of our staff
CAPHRI’s reason for existence is to provide a stimulating environment where talent can grow and flourish. Where
possible, we prefer to use lean methodology and place accountability, responsibility and authority at the lowest
level (individual, team, research line, School, Faculty). Employees work smarter and better when they believe they
have more decision-making authority and when they believe their colleagues are committed to their success. The
research lines are responsible (but not accountable) for financing staff appointments for research tasks. In 2018,
we will explore on mandating principle investigators financial management accountability, responsibility and
Page 7
See appendix A for strategy operationsauthority of the decentral reserves .
CAPHRI’s passion for health, also translates to employee’s health and a healthy work/life balance. This includes
having lifelong learning opportunities that offer courses for internal and external professionals and career
prospects within and outside the organisation . In 2016, the School has introduced an ‘euro formation model’
instead of an fte-model to appoint permanent staff. This has removed the incentive to only hire expensive staff,
creates opportunities to build career trajectories for young staff and strategic investment for research lines. In
order to stimulate more permanent contracts, CAPHRI absorbs the risk of permanent contracts from PI’s when de-
central financial reserves are available for at least 6 years (upon annual re-evaluation) . In collaboration with
Human Resources, we will facilitate (project) staff to find career opportunities elsewhere . This is also to the
benefit of the School as good scientists may decide to return to CAPHRI or build a new collaboration with us.
1.5 We provide high quality training for our researchers
We train highly employable and skilled PhDs for independent research positions in the academic, industrial and
governmental labour market and to contribute to workforce capacity building of professionals pursuing their PhD
at CAPHRI at a later stage in their career. A strong feature of CAPHRI PhD’s and postdocs entering the labour
market are their strong generic and practice-related skills combined with their usually high societal and economic
impact. A PhD alumni from CAPHRI is therefore likely to find a good career. Our alumni analysis shows that About
all (100%) of CAPHRI PhD graduates have found a new job at the time of their PhD defense (or earlier!) and in case
of external PhDs, continue working at their current employer. A high number in comparison with national figures,
namely up to 41%, stay in research-related fields in and outside academia, often combined with teaching activities
(16%). About a quarter works in the health care sector and 15% in consultancy or policy advice. CAPHRI has built a
strong support system for PhD candidates. This includes a PhD Panel with a PhD representative per department
and per research line, confidentiality advisors, bimonthly PhD/Postdoc committee meetings, a spring and fall
meeting for all PhD candidates and postdocs, a PhD/Postdoc parallel session and poster session at the CAPHRI
annual meeting, a 1st years meeting, e-assessment support for supervisors for the selection of internal PhD
candidates , training and supervision plans for PhD candidates, a training course for PhD supervisors and an
online system (TRACK) to monitor PhD progress and the quality of supervision of supervisors.
Aspiration 2
We are the natural academic partner for care and public health challenges in our region and beyond.
It is our conviction that innovations take place when people from different backgrounds, perspectives and
capabilities meet and converge. CAPHRI’s competitive strength can be found in our inter-disciplinary connections
in care and public health research that CAPHRI continues to feed in institutional, regional and international
collaborations. This makes us unique.
2.1 We connect to other groups within MUMC+ and Maastricht University.
CAPHRI’s passion for care and public health research with its focus on PhD education and on the region, Europe
and beyond aligns seamlessly with Maastricht University’s mission that focusses on the (1) Health-Related Quality
of Life, (2) Europe and a Globalizing World and (3) Learning and Innovation. Also, CAPHRI’s focus on inter-
disciplinary partnership and societal impact is right at the heart of Maastricht University’s strategy ‘community at
the CORE’. As Maastricht University has historically been initiated as a ‘Health Research University’ collaboration
with other faculties on a health topic is more natural, acceptable and current practice.
Internal connection is indeed already strong as can be shown by our joint staff appointments, joint PhD projects
large interfaculty projects, and the CAPHRI initiated UM Centre for Global Health. CAPHRI will investigate if
facilitating cross-faculty collaboration by ensuring the PhD incentive of 13k for promotors for a CAPHRI graduation,
also when sharing projects with other faculties, will lead to more cross-faculty projects and enough benefits to
Page 8
See appendix A for strategy operationsbalance the additional costs . About 50 of CAPHRI’s PhD projects (12.5%) are already in collaboration with other
Schools, which is substantial more than the other Schools. However, CAPHRI will investigate the possibility to
further intensify cross-School collaboration within its Faculty of Health, Medicine and Life Sciences .
Maastricht University’s Faculty of Health, Medicine and Life Sciences has joined a cooperative alliance with
Maastricht's academic hospital (azM) under the name Maastricht University Medical Centre+ (MUMC+). CAPHRI’s
mission also aligns with MUMC+’s strategy for 2020 ‘Healthy living’ and its need to also matter for citizens in the
region. We both wish to address societal and economic deliverables and milestones in our province. Our wish is to
demonstrate to the world how a hospital can become – in joint coalition with a knowledge institute – truly
embedded and (partly) responsible for the health of its citizens in their region. As a natural partner, CAPHRI acts as
a non-obtrusive ‘societal impact’ reflector for hospital policies. CAPHRI’s researchers also directly contribute to
hospital care as they investigate the effectiveness of novel medical interventions, their societal or economic value,
and future challenges in hospital care, including towards having a more public health responsibility and the
substitution of hospital care with primary care. MUMC+ collaboration further brings efficiencies and
professionalism due to economies of scale.
2.2 We contribute to a healthy society in Limburg and the Netherlands.
The School is traditionally very well connected in the region. CAPHRI functions as a dedicated and innovative
interface between regional stakeholders, such as care organisations, knowledge institutes, governments and local
health councils, citizen representatives and researchers who work with CAPHRI. This network function brings
responsibility. Together with our regional partners we are co-responsible for the health and economy of the
citizens in Limburg and deploy initiatives to stimulate this. Examples are our ‘kennis-as’ large-scale projects on
healthy schools (Movare project), healthy work places (4Limburg project) and health measurements (Lime-
project); and our Academic Collaborative centres (figure 1) on public health, general practice, sustainable health,
rehabilitation, ageing and in the future possible on infectious disease control . During the next years CAPHRI will
explore how to build on these existing relationships and expand them for the benefit of other researchers within
the School .
CAPHRI cooperates with the partner knowledge institutes Nivel, Amsterdam Public Health research institute and
the Radboud Institute for Health Sciences that together form the national School CARE that is accredited by the
Dutch Royal Society of Sciences. It is our aim to enlarge this cooperation to involve more research institutes that
focus on care and public health in the Netherlands . This will give us more leeway to influence national policies
regarding care and public health research.
2.3. We are a globally connected European School that is anchored in the EU-region.
Successful research in care and public health often has an international perspective. Considering concepts and
results of international research is essential, also for research focusing on the national level. Most of our CAPHRI
research already stems from or is related to internationally oriented research projects and connections and our
PhD candidates are of more than 40 nationalities (figure 5). Also, the new strategic program of Maastricht
University “Community at the CORE” (2017-2021) emphasizes internationalization under the theme that UM is a
“globally linked European university” that is anchored in the EU-region Maas-Rhine (figure 4). The profile of
CAPHRI fits well to this reality and further ambitions of the university to establishing and maintaining strong
research connections in the EU-region, Europe and globally.
Page 9
See appendix A for strategy operationsFigure 4. CAPHRI’s alliances in the EU-Region Maas-Rhine
Being internationally positioned is important for CAPHRI and its research in many ways: (1) Diversity: With
international staff, PhD candidates and research collaborations, we increase in critical mass and add different
perspectives. (2) Attractiveness: Staff, including young and promising researchers, finds it attractive to work and be
creative in an international environment and to contextualize current research in an international perspective. (3)
Funding chances: large funding organizations often require collaborations between countries and within
international networks to capitalize on expertise and excellence. (4) Societal responsibility: Collaborations with e.g.
middle income countries can support their capacity development and strengthen their health (care) research and
health (care) systems.
To build sustainable, effective and efficient international research collaborations, CAPHRI formulates the following
strategy: CAPHRI wants to explore and support further collaboration and strengthen existing promising
collaborations with other research organizations, such as universities, universities of applied sciences and public
health institutes, according to the principle of “growing in mutual trust”: Existing research collaborations of
CAPHRI researchers with EU (regional) and international research organizations that are successful with regard to
research output and have the potential to be of interest to CAPHRI researchers beyond the own team, will be
extended, pruned and consolidated (figure 5).
The research collaboration shall be materialized in common grant applications, research projects, staff mobility,
mutual part-time appointments and collaborative PhD supervision – the latter could be carried out in joint or
double PhD programs or in accepting external PhD candidates who work (also) at our international partner
universities.
Page 10
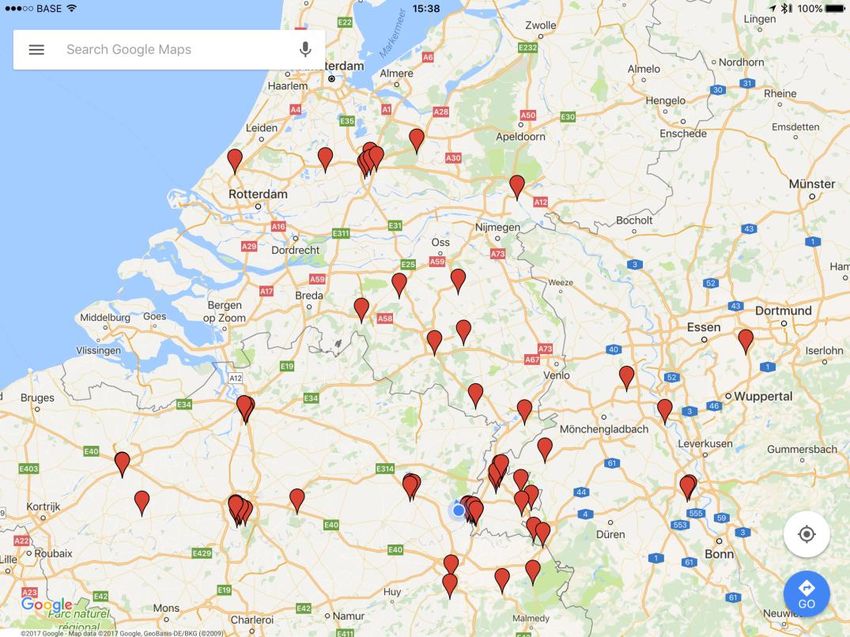
See appendix A for strategy operationsFigure 5. CAPHRI’s international Alliances in the USA, Europe, Africa and Asia
We will actively establish sustainable institutional research and PhD collaborations in our neighboring countries
Belgium, Germany, Luxembourg, the UK and in countries where special opportunities appear, e.g. stimulated by
FHML or individually established research collaborations. Institutionalized international collaborations are open to
all CAPHRI researchers to participate.
2.4 We are visible and attractive
To achieve our aspirations and to keep building towards a community at the CORE culture internal and external
communication is essential. We want our PhD candidates, researchers and support-staff to identify with different
organisational groups: their project team, their department (for disciplinary cohesion) and their research line (for
thematic cohesion). Our international communication is organised via digital updates (monthly newsletters and ad
hoc social media) and via frequent person-to-person contact. This includes an open-door policy with the
directorate, weekly meetings of the directorate, monthly meetings with the board of RL chairs (consisting of
representatives of the 6 research lines), quarterly meetings with the school council and our annual away day. It is
CAPHRI’s ambition to be housed in one building instead of four. Our external communication is also based on
digital communication such as via website updates, twitter and LinkedIn) and via site-visits. To facilitate the
latter meetings in 2018 a CAPHRI brochure and business gifts will be developed and shared with our PI’s to be
used with new prospects.
Page 11
See appendix A for strategy operationsYou can also read

















































