BTS Clinical Statement on Aspiration Pneumonia Draft 11 April 2022 Available for public consultation from 11 April 2022 to 13 June 2022 - British ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BTS Clinical Statement on Aspiration Pneumonia
Draft 11 April 2022
Available for public consultation from
11 April 2022 to 13 June 2022
Contact:
British Thoracic Society,
17 Doughty St, London WC1N 2PL
miguel.souto@brit-thoracic.org.uk
A response form is available on the BTS website.
Please send your responses to Miguel Souto by 5pm on Monday 13th
June 2022
11 BTS CLINICAL STATEMENT ON
2 ASPIRATION PNEUMONIA
3
4 A John Simpson1,2, Jamie-Leigh Allen3, Michelle Chatwin4,5, Hannah Crawford6,7,8, Joanna Elverson2,9,
5 Victoria Ewan1,10, Julian Forton11,12, Ronan McMullan13,14, John Plevris15,16, Kate Renton17,18, Hilary
6 Tedd2, Rhys Thomas1,2, Julian Legg3,19
7
8 1 Newcastle University, Newcastle upon Tyne, UK
9 2 Newcastle upon Tyne NHS Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
10 3 Southampton Children’s Hospital, Southampton, UK
11 4 Clinical and Academic Department of Sleep and Breathing, Royal Brompton Hospital, Guys and St
12 Thomas’ NHS Foundation Trust.
13 5 NMCCC, National Hospital for Neurology and Neurosurgery, University College London NHS
14 Foundation Trust
15 6 Tees, Esk and Wear Valleys NHS Foundation Trust, Darlington, UK
16 7 Teesside University, Middlesbrough, UK
17 8 University of Central Lancashire, Preston, UK
18 9 St Oswald’s Hospice, Newcastle upon Tyne, UK
19 10 South Tees Hospitals NHS Foundation Trust, Middlesbrough, UK
20 11 Noah’s Ark Children’s Hospital for Wales, Cardiff, UK
21 12 Cardiff University, Cardiff, UK
22 13 Queen’s University Belfast, Belfast, UK
23 14 Belfast Health and Social Care Trust, Belfast, UK
24 15 University of Edinburgh, Edinburgh, UK
25 16 Royal Infirmary of Edinburgh, Edinburgh, UK
26 17 University Hospital Southampton, Southampton, UK
27 18 Naomi House & Jacksplace Hospices for Children and Young Adults, Winchester, UK
28 19 University of Southampton, Southampton, UK
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
252
53
54
55
56 Contents Page
57
58 i. Guidance points for clinical practice 4
59 1. Background, definitions, aims and scope of the Clinical Statement 6
60 2. Epidemiology 7
61 AP associated with stroke and chronic neurological conditions
62 Cancers of the head and neck, oesophagus and stomach and their treatment
63 Intubation of the trachea
64 Intubation of the gastrointestinal tract
65 The overlap between AP and CAP/HAP/VAP
66 Mortality
67 3. Pathogenesis 9
68 Normal and abnormal swallowing
69 Normal and abnormal cough
70 Microbiology
71 Pulmonary and systemic immune responses
72 Special considerations in older patients
73 Special considerations in children
74 4. Prevention 15
75 Antibiotics
76 Swallowing difficulties
77 Assessment
78 Physical measures to improve swallowing
79 Pharmacological measures to improve swallowing
80 Cough and muscle strength
81 Oral care
82 Feeding
83 Modifiable risk factors
84 Special considerations in adult patients in intensive care units
85 Special considerations in children
86 Primary aspiration
87 Retrograde aspiration from GOR
88 Aspiration of upper airway secretions
89 Intractable aspiration
90 5. Diagnosis 23
91 Special considerations in children
92 6. Management 26
93 Antibiotics
94 Oxygen
95 Prophylactic anticoagulation
96 Hydration
97 Nutrition
98 Respiratory physiotherapy
99 Initiation of preventive measures
100 Liaison with community teams
101 Advance care planning
102 Special considerations in children
103 7. Palliative and supportive care 30
104 Use of antibiotics at the end of life
105 Clinically assisted nutrition and hydration
106
107 8. Suggested areas for future research 32
108 9. References 33
109 10. Acknowledgements 46
110 11. Disclosures 46
111
112 Appendix 1. Causes of abnormal swallowing 47
113 Appendix 2. Specific additional considerations in palliative care 48
3114 Decisions around eating and drinking with acknowledged risks
115 Symptom management
116 Bereavement support
117 Appendix references 50
118
119
120
121 ABBREVIATIONS
122
123 ACE angiotensin-converting enzyme
124 ACT airway clearance techniques
125 AP aspiration pneumonia
126 BAL bronchoalveolar lavage
127 BiPAP bilevel positive airway pressure
128 BTS British Thoracic Society
129 CAP community-acquired pneumonia
130 COPD chronic obstructive pulmonary disease
131 CPAP continuous positive airway pressure
132 CT computed tomography
133 CXR chest x-ray
134 DMD Duchenne’s muscular dystrophy
135 FEES fibre-optic endoscopic evaluation of swallowing
136 GI gastrointestinal
137 GOR gastro-oesophageal reflux
138 HAP hospital-acquired pneumonia
139 HCAP healthcare-associated pneumonia
140 ICU intensive care unit
141 MCA middle cerebral artery
142 NICE National Institute for Health and Care Excellence
143 PaO2 partial pressure of arterial oxygen
144 PCF peak cough flow
145 PEG percutaneous endoscopic gastrostomy
146 PEJ percutaneous endoscopic jejunostomy
147 PPI proton pump inhibitor
148 SpO2 oxygen saturation assessed by pulse oximetry
149 SAP stroke-associated pneumonia
150 SLT speech and language therapist
151 TRPV1 transient receptor potential vanilloid subtype 1
152 UMN upper motor neurone
153 VAP ventilator-associated pneumonia
154 VFS videofluoroscopy
155
156
157
158
159
160
161
162
163
164
165
4166
167
168
169
170
171
172
173
174
175
176 GUIDANCE POINTS FOR CLINICAL PRACTICE
177
178 The following key points represent an executive summary for clinicians drawn from the sections that
179 follow, in which greater detail is provided.
180
181 General
182
183 Aspiration pneumonia (AP), and risk factors for AP, are common. AP is particularly common in
184 people with a learning disability, in older people and in patients with neurological or upper
185 gastrointestinal conditions.
186
187 Prevention, identification and treatment of AP requires a multidisciplinary team approach.
188
189 Every hospital and care home should have at least one oral health “champion” promoting good oral
190 healthcare.
191
192 Pathogenesis of AP
193
194 AP is usually characterised by micro-aspiration of bacteria-rich secretions from the oropharynx into
195 the lung and is very frequently accompanied by swallowing difficulties.
196
197 Swallowing impairment may be “silent” (not apparent to an observer), so a high index of suspicion is
198 needed for patients at high risk.
199
200 Abnormal swallowing commonly improves/recovers (particularly after a stroke), either
201 spontaneously or with treatment.
202
203 AP is also commonly caused by reflux of material from the gastrointestinal tract.
204
205 Prevention of AP
206
207 Good oral hygiene appears to reduce the rate of AP.
208
209 For patients in hospital or care homes, oral hygiene should include brushing of the teeth, tongue and
210 palate with a soft toothbrush, using non-foaming toothpaste, at least twice a day.
211
212 Oral examination should be performed in all hospitalised patients at risk of AP or with suspected AP,
213 and at least weekly in care home residents, checking for infection (e.g. candidiasis), quality of
214 dentition, food residue, and cleanliness of mucosal surfaces. Any abnormalities should be treated.
215
216 People with swallowing difficulties should be referred to a speech and language therapist (SLT).
5217
218 Whenever feasible, patients with mild swallowing problems who are not considered at high risk of
219 AP after a bedside swallow assessment should be fed orally and observed carefully.
220
221 When consuming food and liquid as normal is felt to present a high risk of AP, cold carbonated
222 drinks may be trialled; alternatively, thickened fluids or feeds may be trialled.
223
224 In patients approaching the end of life and/or with moderate-severe dementia, a best interests
225 discussion should take place prior to a “nil by mouth” instruction.
226
227 When a SLT considers a patient’s swallow presents a high and imminent risk of AP and a “nil by
228 mouth” instruction is issued, a plan should be formulated (a) seeking to restore effective swallow,
229 and (b) arranging further assessment of swallow. A “nil by mouth” instruction should be considered
230 temporary, and steps taken to minimise duration where possible.
231
232 In patients with a newly diagnosed abnormality of swallowing that presents a high risk of AP, who
233 are not felt to be approaching the end of life, early nasogastric feeding (within 3 days of
234 presentation with swallowing difficulties) improves nutritional status and outcomes. Attempts to
235 improve swallow, with a view to restoring eating and discontinuing nasogastric feeding, must be
236 continued.
237
238 Percutaneous endoscopic gastrostomy (PEG) should be considered when abnormal swallow presents
239 a continuing high risk of AP and when nasogastric tubes are either poorly tolerated or fail to provide
240 adequate nutrition.
241
242 PEG tubes should not always be considered permanent. If safe swallow returns PEG tubes can be
243 removed.
244
245 In Chinese and Japanese patients at risk of AP after stroke, and in the absence of contraindications,
246 angiotensin-converting enzyme (ACE) inhibitors should be prescribed to reduce the risk of AP.
247 Insufficient evidence currently exists to support this practice in other ethnic groups.
248
249 Diagnosis of AP
250
251 A careful history is key to increasing the likelihood of an accurate diagnosis of AP. In patients
252 presenting with a likelihood of community-acquired pneumonia (CAP), risk factors and features of
253 the history particularly suggestive of aspiration should be covered.
254
255 Chest x-ray fails to detect AP in up to 25% of cases, when compared with thoracic CT scans.
256
257 Older patients may have a blunted systemic inflammatory response compared to younger patients.
258
259 Management of AP
260
261 For hospitalised patients with AP a broad-spectrum antibiotic regimen should be prescribed (often
262 intravenously at first), guided by local practice and the risk of antibiotic-resistant pathogens.
263
264 A 5-day course of antibiotics is considered adequate for AP unless there is failure to improve, in
265 which case alternative sources of illness and/or an alternative antibiotic regimen should be sought.
266
6267 Hospitalised patients with AP should receive thromboprophylaxis (unless contraindicated), adequate
268 hydration and (if required) supplemental oxygen.
269
270 Patients hospitalised with AP should have early access to physiotherapy (to reduce the risk of
271 sputum retention or atelectasis), with early referral for general, respiratory or neuro-rehabilitation
272 as appropriate.
273
274 Palliative care
275
276 The palliative care needs of patients approaching the end of life, and their families, should be
277 addressed, including advance care planning and referral to specialist palliative care services as
278 appropriate.
279
280
281
282
283
284
285
286
287 1. BACKGROUND, DEFINITIONS, AIMS AND SCOPE OF THE CLINICAL STATEMENT
288
289 This BTS Clinical Statement addresses the risk assessment, prevention and management of
290 aspiration pneumonia (AP). Each section is summarised with key clinical practice points. The
291 recommendations made are based on a review of the published evidence but are predominantly
292 based on expert opinion aimed at providing pragmatic guidance.
293
294 The Statement arose because AP is disproportionately represented in people with a learning
295 disability, in whom it is a major cause of death (1). The management of patients with community-
296 acquired pneumonia (CAP) and learning disability is therefore the focus of a comprehensive parallel
297 BTS Clinical Statement (2). Despite this, however, most AP still occurs in people who do not have a
298 learning disability. The existing literature on AP is of insufficient depth and quality to construct
299 formal, comprehensive guidelines. For these reasons the BTS proposed a Clinical Statement devoted
300 to AP as a stand-alone document, but which specifically cross-references the sister Clinical
301 Statement (2). All of the general preventive, diagnostic and management principles described in this
302 document can be applied to people with a learning disability, and footnotes directing readers to
303 context-specific sections of the sister Statement are provided throughout.
304
305 AP refers to the micro-aspiration of bacteria-rich oropharyngeal or gastrointestinal (GI) secretions
306 into the lung in sufficient amounts to cause alveolar and systemic inflammation. Micro-aspiration
307 sufficient to cause pneumonia is usually associated with abnormal swallowing. To avoid any
308 potential confusion, the terms swallowing impairment, abnormal swallowing or swallowing
309 difficulties are used instead of the term dysphagia, throughout.
310
311 AP is a common condition predominantly affecting older patients, and as the world’s population
312 continues to expand and age, AP will become an increasing concern for healthcare systems globally.
313 Impaired swallowing can lead to malnutrition, dehydration, choking, reduced quality of life, and
314 death (3-5). Because so many people are at risk of developing AP, a significant emphasis of this
315 Statement is on prevention.
316
7317 AP has been the subject of excellent reviews and commentaries in recent years (6-11). However, two
318 broad factors make it harder to generalise findings across studies on AP. Firstly, it is often hard to
319 diagnose AP with certainty, as micro-aspiration is usually clinically “silent” and unwitnessed.
320 Secondly, micro-aspiration due to abnormal swallowing results from a wide range of pathologies,
321 and so heterogeneous patient groups are included in published studies on AP.
322
323 The aim of this Statement is to provide practical, expert-agreed opinion on the epidemiology,
324 pathogenesis, prevention, diagnosis and management of AP, including palliative care for those dying
325 with AP. Summary guidance points for clinical practice are summarised at the end of each section,
326 and are combined on pages 4 and 5. Areas requiring important research to fill key knowledge gaps
327 are also highlighted.
328
329 The Statement focuses on the common clinical setting in which bacteria-rich oropharyngeal
330 secretions are micro-aspirated into the lung. The following are not considered here: aspiration
331 pneumonitis (in which a large volume of vomitus of low pH suddenly enters the lungs, initially
332 causing a chemical insult rather than infection); lipoid pneumonia; inhalation of foreign bodies; and
333 meconium aspiration in the newborn. Similarly, micro-aspiration of infected secretions can cause
334 disease of the airways (e.g., bronchospasm, bronchiectasis, and forms of bronchiolitis). We have
335 focused on AP, but the interested reader is referred to articles describing aspiration-related airways
336 disease (7,8,12).
337
338
339
340
341
342
343 2. EPIDEMIOLOGY
344
345 Micro-aspiration, swallowing difficulties and AP are all common, although high-quality, validated
346 estimates of prevalence at population level are lacking.
347
348 Rough estimates have suggested that as many as 1 in 20 people in the United States may have some
349 degree of swallowing impairment (13), and 0.4% of all hospital admissions in the US may be due to
350 AP (14). Abnormal swallowing is caused by a variety of neurological, muscular or gastrointestinal
351 disorders and is unequivocally associated with increased risk of AP (15-17). The proportion of people
352 with risk factors for AP is increasing (18-21).
353
354 AP is consistently associated with older age (18,22-25). Up to a quarter of care home residents are at
355 risk for AP at any given time (26,27). Older people generally have reduced pharyngeal sensation
356 (28,29). Clinically “silent” micro-aspiration is common in old age and it is likely that abnormal
357 swallowing is greatly underestimated.
358
359 AP associated with stroke and chronic neurological conditions
360
361 Estimates vary according to clinical conditions, but 10-50% of patients with stroke will develop AP
362 (30-33), also known as stroke-associated pneumonia (SAP). Approximately 11% of patients
363 hospitalised with Parkinson’s disease or dementia develop AP over a 3-month period (34), and
364 dementia with Lewy bodies carries a particularly high risk of AP (16). AP also commonly complicates
365 multiple sclerosis, motor neurone disease, Huntington’s disease, Down syndrome and cerebral palsy.
366
367 Cancers of the head and neck, oesophagus and stomach and their treatment
8368
369 Head and neck cancers are associated with a high risk of aspiration, augmented by treatments such
370 as surgery, chemotherapy and radiotherapy, approaching 70% in treated patients in some series
371 (35). The risk accumulates with time in survivors, with around 50% of patients having late AP (36,37),
372 and around 60% describing impaired swallow at 3 years (38). Oesophageal cancer is associated with
373 AP in around 20% of cases (17), and gastric cancer in around 3.5% (39). Major cardiovascular surgery
374 is complicated by AP in 20-45% of cases (40-42), and AP may arise after around 10% of
375 thoracotomies (43).
376
377 Intubation of the trachea
378
379 Intubation of the vocal cords using an endotracheal tube to allow mechanical ventilation creates an
380 ideal environment for micro-aspiration. Ventilator-associated pneumonia (VAP) is therefore a form
381 of AP, developing in approximately 20-30% of patients intubated and mechanically ventilated for
382 more than 3 days (44,45).
383
384 Intubation of the gastrointestinal tract
385
386 Enteral feeding (via nasogastric tubes, post-pyloric feeding tubes, or gastrostomy (e.g. percutaneous
387 endoscopic gastrostomy, PEG) tubes) is often used to feed patients with swallowing difficulties at
388 high imminent risk of developing AP, but paradoxically increases the likelihood of AP, via cephalad
389 movement of feed and aspiration into the lungs.
390
391 The overlap between AP and community-acquired pneumonia (CAP)/hospital-acquired pneumonia
392 (HAP)/VAP
393
394 The commonest classification of pneumonia is based on where the patient was when the pneumonia
395 began. Clearly, however, the process of micro-aspiration may occur regardless of a patient’s
396 location. As such, micro-aspiration contributes to CAP. Between 5 and 15% of all CAP is thought to
397 be AP (22,46), though estimates in Japan have been as high as 60% (47,48). The incidence of
398 admission with community-acquired aspiration pneumonia in persons over 65 years has been
399 estimated at 31 per 10,000 persons, and (for age over 75 years) 35 per 10,000 in different healthcare
400 systems (23,24). Among patients admitted to hospital with pneumonia, 55% have impaired swallow
401 (49), though selected studies report abnormal swallow in up to 80% of patients with CAP (50).
402 Recurrent pneumonia is more common in patients with a history of AP.
403
404 In summary, evidence suggests that a contribution from abnormal swallowing and micro-aspiration
405 is important in a significant proportion of CAP. Micro-aspiration is considered a greater contributing
406 factor for HAP, and to be responsible for all cases of VAP.
407
408 Mortality
409
410 Mortality in patients treated for AP in hospital is approximately 10-15% (51,52), rising with
411 advancing risk factors for swallowing abnormalities (53) and with age (54). VAP carries a mortality of
412 around 33% (44,45,55). AP accounts for about 20% of deaths in head and neck cancer (38).
413
414
415
416
417
418
9419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452 3. PATHOGENESIS
453
454 Micro-aspiration is known to occur in healthy individuals (56-58), and it follows that micro-aspiration
455 does not always lead to AP. Increasing evidence points to micro-aspiration from the oropharynx
456 being the source of the normal bacterial communities in the healthy lung (59,69). The assumption
457 remains that the lung competently deals with microbial loads up to a certain size or bacterial
458 composition, beyond which pneumonia emerges.
459
460 AP therefore arises when sufficient bacteria-rich secretions from the oropharynx or upper GI tract
461 reach the alveolar regions of the lung to drive lung consolidation and an inflammatory immune
462 response. In health, efficient swallow and cough prevent secretions from reaching the lung in
463 sufficient quantities to produce pneumonia. The infective burden of micro-aspirates is determined
464 by the degree of impairment of usual oral, pharyngeal and upper GI clearance mechanisms.
465 Consequently, risk factors for AP generally relate to disrupted neurology, consciousness, muscle
466 function, oropharyngeal integrity, upper GI function or immune function (Table 1).
467
468
469
10470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
Increasing age
Resident in chronic healthcare facility (permanently or in the last 90 days)
Smoking
General Underweight/malnourished
Overweight
Prolonged supine position
Hurried/inattentive feeding by carers
Cardiac arrest
Traumatic brain injury
Reduced conscious level Opiate and non-opiate-based analgesia, anti-psychotic medication, sedatives,
benzodiazepines, anti-seizure medications, antihistamines, anti-spasmodics e.g.
baclofen
Alcohol excess
Stroke
Dementia
Intellectual disability
Neurological disease Parkinson’s disease
11Motor neurone disease
Multiple sclerosis
Cerebral palsy
Delirium
Sarcopenia
Muscle disease Muscular dystrophies and myopathies
Myasthenia gravis
Oesophagogastric cancer
Achalasia
Eosinophilic oesophagitis
Upper GI disease Recurrent vomiting
Benign oesophageal stricture
Gastro-oesophageal reflux (GOR)
Hiatus hernia
Gastroparesis (e.g. via autonomic dysfunction or overuse of opiates)
Laryngopharyngeal disease Pharyngeal or laryngeal cancer
Vocal cord paralysis
Oral cancer
Dry mouth
Sialorrhoea
Dental caries
Oral and dental disease Dental plaque
Dental abscess or decay
Candidiasis
Retained food products
Unclean tongue
Diabetes mellitus
General increased risk of infection Use of antibiotics in the last 90 days
Immunosuppression
Upper GI endoscopy
Nasogastric or nasojejunal tube
Percutaneous endoscopic gastrostomy (PEG) or percutatneous endoscopic
Instrumentation of the airways and digestive jejunostomy (PEJ) tubes
tract Endotracheal tube
Laryngeal mask airway
Nasotracheal tube
508 Table 1. Risk factors for AP. Modifiable risk factors are highlighted in bold text. a
509
510
511
512 Normal and abnormal swallowing
513
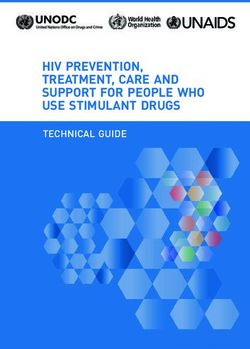
514 Swallowing is divided into oral, pharyngeal, and oesophageal phases (Figure 1). When awake,
515 swallowing is a combination of automatic involuntary and voluntary swallows, and when
516 unconscious a swallow is an upper airway protective reflex.
517
518
519
a
Specific risk factors for pneumonia in learning disability are considered on page 12 of the Learning Disability
Statement, including the opportunity to assess these at a dedicated annual health check (page 16 of the Learning
Disability Statement).
12520
521
522
523
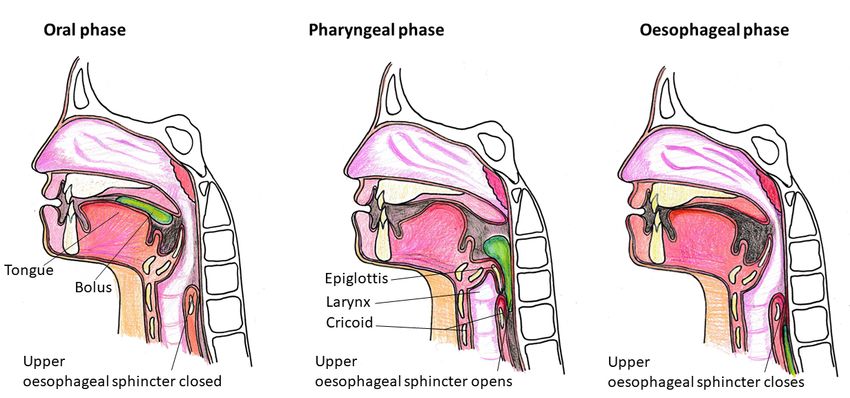
524 Figure 1. Normal swallowing.
525 In the oral phase food is prepared by the lips, tongue and teeth to form a bolus which is propelled backwards
526 by the tongue. Only the oral phase of swallowing is completely under voluntary control. Anticipation of food
527 and mastication stimulate saliva production, which helps effective swallowing. Healthy adults produce around
528 1.5 litres of saliva daily (61).
529 In the pharyngeal phase, the tongue base retracts to push the formed bolus into the pharynx. The anterior
530 upper oesophageal sphincter, the main muscle of which is cricopharyngeus, sits behind the larynx. The upper
531 oesophageal sphincter is a 2-4 cm section under high pressure, which normally stops air entering the
532 oesophagus. The external laryngeal muscles move the anterior cricopharynx and the larynx upwards and
533 forwards, opening the upper oesophageal sphincter. Simultaneously, the epiglottis curves posteriorly and
534 downwards over the larynx to meet the arytenoid cartilage, effectively sealing the larynx and preventing
535 airway penetration. Closure is at the level of the true vocal cords, the false cords, the arytenoids, and the
536 epiglottis. The motion of the hyoid bone and epiglottis also reduces cricopharyngeal pressure, contributing to
537 opening of the upper oesophageal sphincter. The pharynx contracts and moves the food bolus into the
538 oesophagus, closing behind the bolus. As the bolus enters the upper oesophagus apposition of the tongue
539 base and posterior pharyngeal wall propels the tail of the bolus. Successful swallowing also depends on the
540 simultaneous arrest of respiration (deglutition apnoea). This is centrally generated and synchronous with, but
541 not dependent on, laryngeal closure. Typically, exhalation precedes and follows the swallow, to prevent bolus
542 inhalation.
543 During the oesophageal phase of swallowing, the bolus moves towards the stomach by peristalsis, which is
544 regulated entirely by the autonomic nervous system.
545
546
547
548 Sensory receptors and pathways involved in the initiation of effective swallow are complex but have
549 received attention because they may represent therapeutic targets. For example, interest has
550 surrounded thermal and tactile stimuli promoting effective swallowing. Increasing attention has
551 focused on cough regulation by transient receptor potential vanilloid subtype 1 (TRPV1), which is the
552 receptor for the neuropeptide substance P, which in turn can mediate cough. Angiotensin-
553 converting enzyme (ACE) 1 degrades substance P. Local substance P is reduced in patients with
554 swallowing difficulties and AP (62) and restoration of substance P levels, for example by ACE
555 inhibition, has become a therapeutic goal.
556
13557 The multiple interacting mechanisms involved in healthy swallowing can be disrupted by a range of
558 different pathological processes, which are significantly over-represented in conditions associated
559 with a learning disability. These are discussed in more detail in Appendix 1.
560
561 Normal and abnormal cough
562
563 An effective cough requires 3 components to be intact. Firstly, the individual needs to be able to
564 inspire up to 85-90% of total lung capacity. Secondly, intact bulbar function is required to ensure
565 rapid closure of the glottis for approximately 0.2 seconds, with subsequent contraction of abdominal
566 and intercostal (expiratory) muscles to generate intrapleural pressures of >190 cmH20 (63). Thirdly,
567 upon glottic opening, explosive decompression is required to generate transient high peak cough
568 flow (PCF) (64). In patients with swallowing difficulties, those with respiratory inflammation due to
569 aspiration have lower PCF (65). PCF is simple to perform (66). Normal ranges vary with age (67), but
570 values below 270 L/min should generally lead to a more detailed assessment of cough and
571 consideration of teaching cough augmentation techniques. b
572
573 Ineffective cough can be produced by reduced consciousness, brainstem lesions, anti-tussive drugs
574 (e.g. opiates), peripheral nerve lesions (e.g. left recurrent laryngeal nerve palsy), vocal cord
575 pathology (e.g. candidiasis), impaired pharyngolaryngeal sensation, and respiratory muscle
576 weakness.
577
578 Microbiology c
579
580 The healthy oral cavity has a relatively stable population of bacterial communities (57,68). Among
581 patients in residential care, hospital wards or intensive care units (ICUs), the oropharynx becomes
582 colonised with organisms such as Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa
583 and Staphylococcus aureus (69-71). When swallowing is disrupted, oral secretions have a higher
584 chance of being aspirated past the vocal cords and into the lung.
585
586 Poor oral hygiene and reduced salivary flow contribute significantly to altered bacterial species in
587 the mouth (72,73). Several studies have postulated that the development of AP is promoted by
588 gingivitis (74), dental plaque (75-77), or dental caries (37,78). However, results have been
589 inconsistent. One large database study found no association between CAP and chronic periodontitis
590 (79), while another suggested that dental caries predicts pneumonia (80).
591
592 A further source of infected, micro-aspirated secretions is the upper GI tract. Gastro-oesophageal
593 reflux (GOR) is common in patients at risk of AP and increased in the presence of hiatus hernia and
594 enteral feeding (81). Proton pump inhibitors (PPIs) are widely used in older patients. As they
595 increase gastric pH, they may reduce bacterial killing in the upper GI tract and their use is associated
596 with pneumonia in outpatients and hospitalised patients (82,83).
597
598 The organisms responsible for causing AP has been a source of continued debate. Bronchoscopic
599 studies yielding bronchoalveolar lavage (BAL) fluid are scarce. The principal controversy has been
600 around the role of anaerobes in the pathogenesis of AP (84). The emerging consensus is that AP is
601 commonly polymicrobial, and that while aerobic Gram-negative bacilli are over-represented, Gram-
602 positive organisms are also commonly isolated (55,85,86). Anaerobes seem unlikely to make a major
603 difference to outcome except in the most severely ill. The range of bacteria isolated in VAP seems
604 broadly similar to that in AP, but with a wider range of potential pathogens (44,87-99).
b
Assessment of lung function in learning disability is considered in the Learning Disability Statement, page 18
c
Microbiology specifically relevant to CAP in learning disability is considered in the Learning Disability
Statement, page 39
14605
606 Pulmonary and systemic immune responses
607
608 While there are very few specific studies in patients with AP, it is likely that the alveolar and systemic
609 immune responses are similar to those in other forms of pneumonia, with older subjects less likely
610 to generate normal immune responses.
611
612 Special considerations in older patients
613
614 The components of AP pathogenesis described above are exaggerated in older people. Older people
615 have reduced pharyngeal sensory perception for swallowing and cough (28,90). In addition, the
616 commonest pattern of breathing in a normal swallow is exhalation-exhalation, but in some older
617 patients inhalation during swallowing may occur, which may predispose to aspiration (91). Ageing is
618 also associated with loss of muscle mass, decreased saliva production, ineffective dentition, reduced
619 sense of smell and/or taste, and delayed laryngeal closure (25). The upper oesophageal sphincter
620 may decrease in cross sectional area with age, probably driven by weakness in the suprahyoid
621 muscles. This results in smaller boluses being conveyed to the upper oesophagus, leaving larger
622 amounts of pharyngeal residue (92), which in turn can be aspirated (93). Furthermore, pulmonary
623 and systemic immunity becomes impaired with increasing age, increasing susceptibility to infection
624 (94).
625
626 Special considerations in children
627
628 In children abnormal swallowing can lead to failure to thrive, choking, AP and impaired
629 neurodevelopment (95-97). Co-ordinated safe swallowing is established during infancy. Primary
630 aspiration into the airway and retrograde aspiration of refluxate following GOR are relatively
631 common causes of lung disease in children. Healthy infants may aspirate sufficient volumes to cause
632 AP, probably because of immature swallowing reflexes (98,99).
633
634 Silent micro-aspiration is common in children with learning disability and also occurs in healthy
635 infants (100). Chronic aspiration is therefore frequently unrecognised, can result in progressive lung
636 disease, and is a major cause of death in children with severe learning disability. Hypostatic
637 pneumonia (the collection of fluid in the dorsal region of the lungs) occurs especially in those
638 confined to a supine position for extended periods, and is more common in children with learning
639 disability.
640
641 Large-volume aspiration usually occurs because of an underlying predisposition, examples of which
642 are shown in Table 2. Upper airway obstruction increases the risk of aspiration in all infants
643 (101,102).
644
645 GOR is common under 6 months of age. Infants may posset frequently, and some may exhibit
646 discomfort, but for many there are no noticeable consequences. GOR is thought to occur due to
647 immaturity of the gastro-oesophageal junction coupled with a liquid milk diet and the recumbent
648 position of infancy. Acid in the distal oesophagus may trigger bronchospasm. For most children GOR
649 is self-limiting and resolves in the second year of life.
650
651 In infants, small amounts of liquid reaching the larynx can cause laryngospasm. In neonates and
652 preterm infants reflux reaching the larynx can initiate life-threatening reflex apnoea and bradycardia
653 (102). Persistent significant GOR to the level of the larynx may modulate laryngeal sensation and
654 hinder the development of a safe co-ordinated swallow in normal infants (103).
655
15656 Aspiration of oral secretions in the absence of food or refluxate can be a significant problem for
657 children with LD and can contribute to progressive lung disease, even when feeding and GOR are
658 safely managed. This risk may persist into adulthood.
659
660
661
662
Structural abnormalities
Laryngeal cleft
Vocal cord palsy (congenital or acquired)
H-type tracheo-oesophageal fistula
Choanal stenosis
Cleft palate (and Pierre Robin syndrome)
Craniofacial disorders with upper airways obstruction
Vascular ring
Abnormal coordination or weakness of pharyngeal or laryngeal muscles
Cerebral palsy
Neuromuscular weakness (e.g. spinal muscular atrophy, myotonic dystrophy, DMD)
Bulbar palsy (progressive or acquired)
Absence of protective reflexes
Delayed maturation of swallowing reflexes
Cerebral palsy
Sedation, sedative anticonvulsants
Airway adjuncts
Tracheostomy
Nasopharyngeal airway
Endotracheal tube
Non-invasive respiratory support such as continuous positive airway pressure (CPAP) or bilevel
positive airway pressure (BiPAP)
663
664 Table 2. Conditions predisposing to large-volume aspiration in children.
665
666
Clinical Practice Points
• AP is usually characterised by micro-aspiration of bacteria-rich secretions from the
oropharynx into the lung and is very frequently accompanied by swallowing difficulties.
• Swallowing impairment may be “silent” (not apparent to an observer), so a high index of
suspicion is needed for patients at high risk.
• Abnormal swallowing commonly improves/recovers (particularly after a stroke), either
spontaneously or with treatment.
• AP is also commonly caused by reflux of material from the gastrointestinal tract.
667
668
16669
670
671
672
673
674
675
676
677
678 4. PREVENTION
679
680 Pneumonia may develop in any patient with risk factors for AP (Table 1), including all people with
681 learning disability, and preventive measures should be focused on these individuals. In practical
682 terms, many patients will have their first contact with healthcare professionals after already
683 developing risk factors (e.g. stroke with swallowing difficulties), or after already having an episode of
684 AP. The aims should be to promote restoration of effective swallow and cough, to reduce bacterial
685 load in secretions and to ensure adequate hydration and nutrition.
686
687 Effective prevention of AP relies on effective multidisciplinary team working and communication,
688 involving SLTs, physiotherapists, oral hygienists/dentists, dietitians/nutritionists, nurses,
689 pharmacists, radiologists and physicians.
690
691 Antibiotics
692
693 There is currently no evidence to support prophylactic antibiotics in adult patients with swallowing
694 difficulties, though they may be considered in children with recurrent AP, as discussed on page 20). d
695
696 Swallowing difficulties e
697
698 Assessment
699
700 There is no validated screening tool for swallowing in older hospitalised patients at present (104).
701 Cough after eating/drinking, choking episodes witnessed by patients/families/healthcare staff, or
702 episodes of presumed AP are indications that an assessment of swallowing is required.
703
704 Swallowing is best assessed and managed by a SLT using a holistic approach (105-107), as part of a
705 wider, multidisciplinary clinical team. Abnormal swallowing can also impact on psychosocial well-
706 being, including stress around mealtimes, reduced enjoyment of meals, avoidance of eating with
707 others, and reduced quality of life (108). There may also be an adverse impact on carers and families
708 (105,106).
709
710 SLT assessment incorporates a detailed history (109,110), with an oromotor and cranial nerve
711 assessment, focusing on motor and sensory components of eating and drinking. Two or more
712 impaired components of an oromotor exam correlate with a higher risk of aspiration (111). Clinical
713 suspicion of silent aspiration or recurrent pneumonia are indications for SLT assessment.
714
d
Prophylactic antibiotics in the context of recurrent CAP in learning disability is discussed on page 26 of the
Learning Disability Statement.
e
Specific issues relating to swallowing difficulties in learning disability are discussed on page 27 of the
Learning Disability Statement.
17715 Specific preventive advice based on the assessment can be conveyed directly to patients. For people
716 who have difficulties with comprehension or retention of information, ‘compensatory techniques’
717 can be used by carers (112). These may include: changes in posture; physical support methods at
718 mealtimes; changes in food textures; thickening fluids; change to smaller, more regular meals;
719 adapting the environment; or adapting utensils.
720
721 Assessment tools can supplement the standard SLT assessment, including patient-centred quality of
722 life questionnaires (113). In some circumstances effective swallowing assessments can be performed
723 remotely (114). Evidence suggests that effective swallowing assessments can reduce AP (31,15),
724 though others have questioned their value (116).
725
726 Where a clear recommendation cannot be made on the basis of a bedside SLT assessment, and
727 where facilities permit, further investigation of swallowing can be initiated.
728
729 Confirmation of micro-aspiration can be obtained in several ways.
730 • Videofluoroscopy (VFS) involves a modified barium swallow (117). Penetration-aspiration is
731 often measured using the 8-point scale introduced by Rosenbek (118), with aspiration
732 defined as barium visible beneath the true vocal cords. If no throat clearing or coughing is
733 visible, the aspiration is considered “silent”. Since aspiration is episodic in nature, a single
734 VFS may not completely exclude aspiration.
735 • Fibre-optic endoscopic evaluation of swallowing (FEES) involves direct visualisation of food
736 boluses of different textures being swallowed (119). Pharyngeal residue may be visualised in
737 the piriform fossae or in the valleculae at the base of the tongue. FEES also assesses whether
738 upper airway secretions are freely aspirated.
739 • Scintigraphy can be used to image the lungs after the patient has swallowed a radionuclide-
740 labelled food bolus. This technique is largely a research tool at present.
741 • Dual-axis accelerometry appears effective in assessing swallowing in specialist centres (120),
742 but has not yet challenged the place of VFS or FEES in clinical practice.
743
744 VFS and FEES are regarded as gold standards for swallowing assessment.
745
746 Where an upper GI cause is thought to contribute to impairment of swallowing, or where GOR is
747 considered a problem, upper GI endoscopy or oesophageal manometry with oesophageal pH and
748 impedance studies can be considered to assess whether an excess of reflux is reaching the proximal
749 oesophagus.
750
751 Physical measures to improve swallowing
752
753 General strengthening of the pharyngolaryngeal musculature and optimisation of nutrition are
754 anticipated to improve swallowing. A simple physical method used to improve swallowing is the chin
755 down or chin tuck method, which simply involves touching the chin against the chest during
756 swallowing. This appears to benefit about half of patients in whom it is used appropriately (34,121-
757 123). Prevention “bundles” aimed at improving swallowing have also been shown to prevent AP
758 (124).
759
760 Impaired swallowing may also be improved by physical, thermal, transcutaneous electrical, or
761 transcranial magnetic stimulation (125-133). These appear well tolerated and simple electrical
762 techniques can be used by patients at home (134). However, large-scale phase III trials are lacking,
763 and specialist equipment and training are required for electrical stimulation. More evidence is
764 required before these techniques are routinely adopted.
765
18766 Pharmacological measures to improve swallowing
767
768 ACE inhibitors, by preventing breakdown of substance P and preserving cough mechanisms, have
769 been extensively studied as a potential strategy for reducing post-stroke AP. Significant reductions of
770 AP have been demonstrated in large, well-conducted studies, among Chinese and Japanese patients
771 after stroke (135,136), though sub-group analysis has not demonstrated clear benefit in Caucasian
772 patients. A small trial from Hong Kong, comparing low-dose lisinopril and placebo in old patients
773 with neurologic swallowing abnormalities receiving nasogastric feeding (>95% had stroke), was
774 terminated at interim analysis because of increased mortality in the lisinopril group (137).
775
776 Promising results have been demonstrated for drugs targeting similar pathways, mostly in post-
777 stroke studies in Japan. These include amantadine, cabergoline, capsiate, mosapride, nicergoline,
778 cilostazol and (in patients with chronic obstructive pulmonary disease (COPD)) theophylline (138-
779 145). Encouraging results have also been reported for some traditional Chinese medicines (146-148).
780 Metoclopramide, which promotes gastric emptying, has had promising effects in patients fed via a
781 nasogastric tube after a stroke (149), though the Medicines and Healthcare products Regulatory
782 Agency (MHRA) recommends that metoclopramide should only be used for up to 5 days (150).
783
784 At present, ACE inhibition is recommended in Chinese or Japanese patients following stroke, for
785 prevention of AP, but insufficient evidence is currently available in other ethnic groups. Other
786 treatments require further evidence from large clinical trials.
787
788 Cough and muscle strength
789
790 Very few trials have demonstrated beneficial effects of muscle training on aspiration or AP. Cough
791 reflex testing did not alter rates of SAP significantly (151). In Parkinson’s disease, expiratory muscle
792 strength training reduced penetration assessed by VFS (152). Voice exercises in patients with glottal
793 closure insufficiency significantly reduced hospitalisation with AP (153).
794
795 While high-quality evidence is lacking in the specific context of AP, the general proven benefits of
796 early mobilisation, neurorehabilitation and pulmonary rehabilitation on outcomes including mobility,
797 posture, strength and quality of life indicate that rehabilitation should be started as soon as is
798 feasible in all patients at risk of AP.
799
800 Oral care f
801
802 A large literature, containing studies of variable quality, has assessed aspects of oral care and the
803 effects on bacterial colonisation, aspiration or AP. Chorhexidine mouthwash appears to reduce
804 colonisation with potential pathogens (154,155), without improving patient outcomes (27,156).
805
806 Mechanical oral care (usually with toothbrushes) has been associated with reductions in AP and
807 death (157-160) as well as proxy measures such as peak expiratory flow and cough reflex (161,162).
808 Dedicated oral care has been associated with significant healthcare savings (163).
809
810 Given the simplicity and safety, we recommend that the mouths of all patients at risk of AP in
811 hospital or care homes should be examined on admission and regularly thereafter. However,
812 implementation of routine oral care is fraught with challenges around time, equipment, culture and
813 inconsistent policies (164), and oral “champions” should be identified to ensure implementation.
814
f
Specific considerations around oral care in learning disability are discussed on page 34 of the Learning
Disability Statement.
19815 UK National Institute for Health and Care Excellence (NICE) guidelines suggest the teeth of care 816 home residents should be brushed twice daily with fluoride toothpaste and there should be access 817 to mouth rinse (165). A soft toothbrush should be used and the gingiva, tongue and palate should be 818 brushed at the same time. In patients with swallowing difficulties, non-foaming toothpaste should 819 be used to reduce the risk of aspiration of the product (164). Pink foam swabs should not be used, as 820 they are ineffective at cleaning teeth, and the foam can be aspirated (166). Soft, small-headed 821 toothbrushes are preferred to stiffer brushes, and can be used to brush the tongue and palate (164). 822 Mucus secretions can often be removed with a soft toothbrush. 823 824 Moisturising mouth gel is effective at hydrating dried-on secretions that can be brushed off later 825 (164). Useful online guidance on providing oral hygiene is available (167). 826 827 Oral candidiasis is common in patients at risk of AP, especially those with diabetes or malignancy, or 828 in patients taking antibiotics or corticosteroids. Severe candidiasis may cause dysphonia and 829 abnormal swallowing and may require endoscopic assessment. Topical nystatin is effective 830 treatment. 831 832 Sialorrhoea can be managed with glycopyrronium, hyoscine patches, oral atropine, botulinum toxin 833 to the salivary glands, or in severe cases salivary gland surgery. g 834 835 Feeding h 836 837 Whenever feasible, patients with mild swallowing problems in whom the risk of AP is not considered 838 high after a bedside swallow assessment should be fed orally and observed carefully. However, 839 dependence on others for feeding increases the risk of AP (71), possibly due to time pressures on 840 carers/healthcare workers (78). 841 842 Although it is standard practice to modify the thickness of fluids and the texture of food in patients 843 with impaired swallowing, the evidence base for this practice is not strong (25,168,169). In a 844 systematic review considering texture-modified food in patients with dementia, there was evidence 845 of lower energy levels and reduced fluid intake (168). Thickening fluid reduces penetration and 846 aspiration but may increase pharyngeal residue. Serving smaller volumes of thickened fluids, for 847 example using teaspoons, may reduce pharyngeal residue (170). Flavouring thickened feeds with 848 honey/nectar can improve pharyngeal clearance, but this is often unpalatable to patients (121). 849 850 Small studies have suggested that drinking carbonated liquids may reduce aspiration (171-173), 851 suggesting that sensory stimulation of the pharynx may improve swallow, in line with suggestions 852 that cold or hot food promotes better swallow than food at room temperature. 853 854 When an SLT assessment concludes that swallowing is impaired to the extent that there is a 855 significantly high risk of AP, a “nil by mouth” order can be made. The questions of when and whether 856 to commence enteral feeding remain contentious. The detrimental effects of malnutrition need to 857 be balanced against the fact that enteral feeding itself is a risk factor for AP. Expert consensus has 858 suggested that if there is no food intake for more than 3 days, or if
863 It is important to recognise that abnormal swallowing frequently resolves (174), and every effort
864 should be made to carry on with specific and general measures to improve swallowing, with ongoing
865 input from SLTs. Patients who are “nil by mouth” still have to clear saliva (normal production is up to
866 1.5 litres per day), which itself remains an aspiration risk.
867
868 In the context of stroke, a landmark study showed that nasogastric feeding improves survival
869 compared with no feeding (175). Other observational studies have suggested that in patients with
870 pre-existing swallowing impairment, nasogastric feeding may not carry significant additional risk
871 (176,177).
872
873 In general, there is little to suggest a benefit for post-pyloric feeding or PEG feeding over nasogastric
874 feeding, and in the context of stroke there is evidence for a trend toward better outcomes for
875 nasogastric feeding (175). An exception is in patients who reflux and aspirate nasogastric or PEG
876 feeds, when post-pyloric feeding or fundoplication may be beneficial. A further possible exception is
877 in the context of significant pooled oral secretions, for which a recent study suggested PEG feeding
878 may be beneficial (178).
879
880 If abnormal swallowing with high risk of AP persists for weeks, and/or if the patient finds nasogastric
881 tubes uncomfortable/intolerable, a PEG tube is an appropriate alternative. As for nasogastric
882 feeding, PEG feeding should not be regarded as necessarily permanent, and precedent exists for oral
883 feeding re-starting when adequate swallow returns (179).
884
885 The nature of the enteral feed to be given is beyond the remit of this statement, and an enteral
886 nutritionist/pharmacist/dietitian should be consulted. However elemental feeds appear to be
887 associated with less AP and better gastric emptying in gastrostomy-fed patients (180,181).
888
889 Most importantly, “nil by mouth” orders must never stand alone, but instead should be issued with
890 clear statements on the plan for nutrition, the plan for continued measures to improve swallow, and
891 the plan for timing of the next assessment of swallow.
892
893 A shared decision-making approach is required around feeding, especially in older patients with
894 complex comorbidities.
895
896 Hospital pharmacists should be consulted on the best way to administer regular medications when
897 patients are “nil by mouth”, and there are useful examples of publications highlighting general
898 principles (182). Several apps exist to document available liquid formulations and dose calculators.
899
900 Specific considerations relating to eating and drinking in the context of palliative care, and the
901 acknowledged risks, can be found in the Palliative Care section on page 30 and in Appendix 2 on
902 page 48.
903
904 Modifiable risk factors
905
906 Having addressed the issues above, attention should turn to potentially modifiable risk factors in
907 Table 1. In all patients, but particularly those with depressed conscious level, medication review
908 should be undertaken with the aim of reducing doses of sedative medications where possible.
909
910 Special considerations in adult patients in intensive care units
911
21912 The principles described above apply in the ICU setting. Prevention of VAP has been extensively
913 studied, and the evidence base is of higher quality than for AP outside the ICU. Guidance
914 recommendations for prevention of VAP are available (183).
915
916 There is good evidence that nursing critically ill patients at between 30° and 45° reduces the
917 likelihood of VAP (184,185), though maintaining this position in practice is challenging (185).
918
919 In keeping with principles described earlier, sedation breaks are also associated with a reduction in
920 VAP (186,187).
921
922 In the ICU setting, chlorhexidine mouthwash reduces VAP in patients undergoing cardiac surgery
923 (188). In other ICU cohorts, a trend to increased mortality has been described (188,189), although a
924 trial of de-adoption of chlorhexidine mouthwash showed no reduction in mortality (190). On the
925 basis of current evidence, chlorhexidine use in critical care should be confined to patients having
926 cardiac surgery. Small studies have suggested that oral suction prior to position change may
927 positively influence rates of VAP and mortality (191).
928
929 As the endotracheal tube is effectively a conduit for micro-aspiration, interest has focussed on its
930 composition. Infected secretions from the subglottis are thought to access the lung down crevices in
931 the lining of the tube cuff, to cause VAP. This has led to the widespread adoption of subglottic
932 suction drainage (SSD), which significantly reduces the incidence of VAP (193-195). Lubrication of the
933 cuff generally reduces the risk of VAP (196,197). Several studies have sought to determine whether
934 tapered cuffs, or tubes of different composition reduce VAP. While physical leak may be reduced by
935 tapered cuffs, and while modern tubes might reduce bacterial colonisation, these have not
936 convincingly translated into significantly reduced VAP or other important outcomes (198-200).
937 Continuous pneumatic inflation of the cuff does not appear to reduce VAP (201).
938
939 As with patients outside the ICU, no hard evidence has emerged to favour post-pyloric over
940 nasogastric feeding.
941
942 While there is no place for prophylactic antibiotics to prevent micro-aspiration outside the ICU
943 setting, there is some evidence in comatose patients requiring emergency intubation that one or
944 two doses may reduce the incidence of VAP (202-205). A full course of antibiotics is not required in
945 this setting (206).
946
947 Special considerations in children
948
949 A priority is to identify whether any structural abnormality can be repaired (Table 2). In more
950 complex cases, identification of primary, retrograde and salivary aspiration allows bespoke
951 interventions to be considered.
952
953 VFS is the gold standard in assessment of swallow in children and can demonstrate subtle
954 abnormalities (207). A formal clinical feeding assessment by a SLT is essential for planning the VFS,
955 to establish appropriate testing conditions.
956
957 FEES allows real-time direct visualisation of the swallow using different textures. FEES is also well
958 placed to assess whether upper airway secretions are freely aspirated (208).
959
960 Microlaryngobronchoscopy can establish whether the larynx is structurally competent. It can
961 exclude structural causes of aspiration including laryngeal cleft and vocal cord palsy, and the
22962 otolaryngology surgeon will be able to review the dynamics of the oropharynx and larynx during
963 spontaneous breathing.
964
965 Primary aspiration
966
967 SLTs can improve the safety of the swallow by restricting feeding to specific fluid consistencies,
968 optimising positioning, using pacing strategies to prevent fatigue, optimising utensils and beakers,
969 and establishing routine. Healthy infants, with aspiration ascribed to maturational delay of
970 swallowing reflexes, will benefit from exposure to ongoing swallow stimulation.
971
972 Severe swallowing abnormalities, for example in a child with cerebral palsy, may not be amenable to
973 conservative interventions and these children will often need nasogastric feeds (or gastrostomy if
974 the problems are thought to be long-term).
975
976 Retrograde aspiration from GOR
977
978 If medical therapy is ineffective and there is good evidence of retrograde aspiration, then
979 a “super-safe” feeding approach should be considered where both primary and retrograde
980 aspiration are managed. A trial of nasojejunal feeds or, for children with an established gastrostomy,
981 a trial of gastro-jejunal feeds via a gastrojejunostomy tube, may be useful to establish whether GOR
982 is contributing to lung disease before definitive anti-reflux surgery is planned.
983
984 Laparoscopic fundoplication is the most common definitive anti-reflux approach to managing GOR
985 and improves respiratory morbidity in children with LD (209).
986
987 Aspiration of upper airway secretions
988
989 Long-term prophylaxis with azithromycin may be useful in this specific situation in children with
990 recurrent AP. Potentially beneficial effects may relate to pro-motility and anti-inflammatory effects
991 of azithromycin. Attention should be given to positioning so that secretions can drain out of the
992 mouth. Physiotherapy in the morning (to remove retained oropharyngeal secretions accumulating
993 overnight), and in the evening (in preparation for the night ahead) may be beneficial. Anticholinergic
994 therapies such as a hyoscine patch, glycopyrronium liquid or ipratropium nasal spray/nebuliser may
995 help reduce secretion volume, but care should be taken since these medications may thicken
996 secretions and increase the risk of urinary retention and constipation. Anticholinergics may
997 therefore need to be stopped temporarily during intercurrent infections.
998
999 Volume of saliva can be reduced by salivary gland botulinum toxin injection, at 2-3 monthly intervals.
1000 In severe cases, salivary ablation is possible with removal of the submandibular glands and parotid
1001 duct ligation.
1002
1003 Intractable aspiration
1004
1005 Children with recurrent aspiration may be managed with a tracheostomy, particularly if they have
1006 had severe exacerbations leading to respiratory failure and multiple admissions. A cuffed
1007 tracheostomy may enable material above the cuff to be effectively suctioned or aspirated.
1008
1009 Care should be taken when considering a tracheostomy however, since this can increase the risk of
1010 aspiration, increase secretion production and render the child more dependent on regular suction
1011 and physiotherapy, which can be uncomfortable. Intractable aspiration can be managed with radical
1012 surgery such as supraglottic laryngeal closure with tracheostomy, where phonation is preserved, or
23You can also read