Break the flu cycle: Regional meeting - Chaired by Dr George Kassianos - Cogora
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

London
Break the flu cycle:
Regional meeting
Chaired by Dr George Kassianos
30 October 2017
10:00–12:30
CPD accredited
This meeting has been organised and funded by Seqirus UK Ltd.
Prescribing Information for surface antigen, inactivated, influenza vaccine adjuvanted with MF59C.1 can
1 be found at the end of this presentation. UK/FLUD/0817/0016ap | October 2017
Meeting objectives
Discuss how to raise awareness and address the burden of influenza for
adults aged 65 years and over with key decision makers in primary healthcare
Share knowledge on the influenza environment: discussing how to implement
a best-practice local influenza vaccination programme to improve outcomes
Introduction copy
Explore the use and effectiveness of current vaccines when considering
the guidance and recommendations from appropriate professional bodies
Support the professional development of attendees through engaging plenary
sessions and interactive workshops
2
Agenda
Time Session Speaker
10:00–10:15 Starting the cycle Dr George Kassianos
10:15–10:30 The burden of flu Pauline MacDonald
10:30–10:45 Personalising vaccination care Dr Roger Henderson
Dr George Kassianos
10:45–11:15 How do we break the cycle? Dr Roger Henderson
Pauline MacDonald
11:15–11:30 copy
Introduction Break
Workshop sessions
11:30–12:10 1. Best practice: Interactive case study Dr Roger Henderson
2. Practical guidance on adult influenza vaccination Dr George Kassianos
Dr George Kassianos
12:10–12:20 Summary of key learnings and faculty questions Dr Roger Henderson
Pauline MacDonald
12:20–12:30 Closing remarks Dr George Kassianos
12:30 Lunch
3
Questions
During the course of the meeting,
questions can be submitted in
two ways:
• Raise your hand and a microphone
Introduction copy
will be brought to you
• Fill in one of the question cards
provided and hand it to one of
the meeting organisers
4
Before we start
Mobile phones
Please make sure your mobile is switched off
Fire alarms and location of emergency exits
No tests are planned today
Introduction Evaluation
copy forms
Please complete your evaluation forms provided via an email link
Certificate of attendance/CPD
Will be provided after the meeting via an email link, please use this to obtain
3 CPD credits from the Federation of the Royal Colleges of Physicians
Reasonable travel expenses
An email link will be provided after the meeting
5
Public Health England:
Leading causes of death in England, 2015
Males (% of all male deaths) Females (% of all female deaths)
Dementia and Alzheimer’s
1 Heart disease 14% 15%
disease
2 Dementia and Alzheimer’s disease 8% Heart disease 9%
3 Lung cancer 7% Stroke 8%
4 Chronic lower respiratory disease 6% Influenza and pneumonia 6%
Introduction
5 Stroke copy 6% Chronic lower respiratory disease 6%
6 Influenza and pneumonia 5% Lung cancer 5%
7 Prostate cancer 4% Breast cancer 4%
8 Colorectal cancer 3% Colorectal cancer 2%
Kidney disease and other
9 Leukaemia and lymphomas 3% 2%
diseases of the urinary system
10 Cirrhosis and other liver disease 2% Leukaemia and lymphomas 2%
6 Public Health England. Chapter 2: major causes of death and how they have changed. Accessed from: https://www.gov.uk/government/publications/health-profile-for-england/chapter-2-major-causes-
of-death-and-how-they-have-changed. Accessed October 2017.
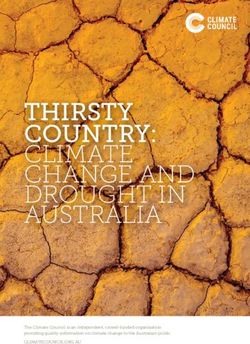
Pathogens detected in patients with radiographic
community-acquired pneumonia
EPIC study, Centers for Disease Control
Human rhinovirus
Influenza
Streptococcus
Streptococcus pneumoniae
pneumoniae
Human metapneumovirus
Respiratory syncytial virus
Parainfluenza viruses
Introduction copy
Other Gram negatives
Coronaviruses
Mycoplasma
Mycoplasma pneumoniae
pneumoniae
Staphylococcus
Staphylococcusaureus
aureus
Adenovirus
Legionella
Streptococcus spp
Other
0 20 40 60 80 100 120 140 160 180 200
7
Wunderink RG, Waterer G. BMJ 2017;358:bmj.j2471.
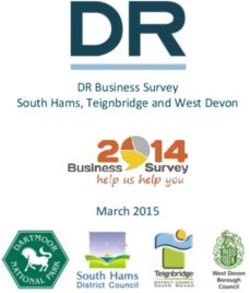
Seasonal influenza activity summary in different
climate areas
Travel medicine
NORTHERN
HEMISPHERE
Influenza peak:
November–March
Introduction copy TROPICS
Year-round activity
SOUTHERN
HEMISPHERE
Influenza peak:
April–September
8
Cox NJ, Subbarao K. Annu Rev Med. 2000;51:407-421.
Starting the cycle
Dr George Kassianos
MD (Hons), FRCGP, FESC, FBGTHA, FFTM RCPS (Glasg),
FBHS, FHEA, FAcadMEd, DRCOG, LRCP (Edin.), LRCS (Edin.),
LRCP&S (Glas.), DMedAcup., DMedHypn., DFP.
9
Disclosures
• Dr George Kassianos is BGTHA President and RCGP National Immunisation Lead
• He has participated in advisory boards or lectured at meetings organised by Sanofi
Pasteur, MSD, Seqirus, Pfizer, AZ and Valneva
Introduction copy
• Chair of RAISE Pan-European influenza committee
10All adults and the elderly population get the same
vaccine…
However, vaccine effectiveness has been observed to differ considerably among
ages and is lowest in the elderly!
How do we break the current flu cycle?
Autumn
Practice orders
TIV or QIV
Introduction copy
Autumn/Winter Spring
Pharmacists and PHE issues
Practices vaccinate the Flu Plan
September Spring/Summer
Influenza JCVI/PHE reports
vaccines arrive vaccine effectiveness
11
CI, confidence interval; PHE, Public Health England; TIV, trivalent influenza vaccine; QLAIV, quadrivalent live attenuated influenza vaccine.Lower effectiveness of the 2014–2015 influenza
vaccine due to A(H3N2) drift
Circulating A(H3N2) and B strains genetically and antigenically drifted against
the 2014–2015 seasonal flu vaccine for the northern hemisphere
Vaccine effectiveness (VE)
Adjusted VE 95% CI
Any influenza 34% 18–48
Influenza A(H3N2)
Introduction copy 29% 9–45
Influenza due to B strain 46% 14–67
VE forQLAIV overall effectiveness among children
2–17 years in 2015–2016 influenza season
Vaccine effectiveness
Adjusted QLAIV
Against: 95% CI
effectiveness
Any influenza 58% 25–76
Influenza A (H1N1) pdm09* 42% 9–69
Introduction copy
Influenza due to B strains* 81% 40–94
*The 2015–2016 season in the UK was initially dominated by influenza A(H1N1)pdm09 and then influenza of B/Victoria lineage.
13 CI, confidence interval; QLAIV, quadrivalent live attenuated influenza vaccine.
Pebody R et al. Euro Surveill. 2016;21:pii=30348.UK vaccine effectiveness in 65 years and over age group
Adjusted influenza vaccine effectiveness (VE) against medically-attended
laboratory-confirmed influenza by age group and influenza type in 2016/17, UK1,2
A(H3N2) adjusted* VE Flu B adjusted VE Flu A and B
Population
(95% CI) (95% CI) adjusted VE (95% CI)
2 – 17 years† 57 (8, 80) 79 (-86, 98) 66 (30, 83)
18 – 64 years 37 (10, 55) 52 (-20, 81) 41 (19, 56)
Introduction copy
≥65+ years -68 (-249, 19) 17(-250, 80) -6 (-95, 42)
All ages 32 (10, 48) 55 (11, 77) 40 (23, 53)
*Adjusted for age-group, sex, month, pilot area and surveillance scheme; † LAIV only.
CI, confidence interval, ICU, intensive care unit; JCVI, Joint Committee on Vaccination and Immunisation LAVI, live attenuated influenza vaccine; VE, vaccine effectiveness.
1. JCVI minute of the meeting on 7 June 2017. Draft minute. Available at: https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/198733240440. Accessed September 2017.
14 2. Public Health England. Influenza vaccine effectiveness. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/641162/Influenza_vaccine_effectiveness_in_primary_care_1617_final.pdf Accessed October 2017.JCVI opinion is that the current influenza vaccine
effectiveness for adults ≥65 years is disappointing1
• A downward trend in vaccine efficacy against influenza A(H3N2) has been observed
over recent years1–4
- Immunosenescence could be an important factor in the reduced effectiveness
being seen
•Introduction
This contrasted
copywith higher A(H3N2) effectiveness in younger adults
• Additional benefit for vaccine effectiveness was however, seen from the use
of the QIV vaccine for the childhood influenza vaccination programme
• The over 65 year old population component of the influenza programme will
be considered during the October 2017 JCVI meeting
JCVI, Joint Committee on Vaccination and Immunisation; TIV, trivalent influenza vaccine; QIV, inactivated quadrivalent influenza vaccine.
1. JCVI minute of the meeting on 7 June 2017. Draft minute. Available at: https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/198733240440. Accessed October 2017; 2. Belongia EA, et al. Lancet Infect
Dis 2016;16:942–51; 3. Kissling E, et al. Euro Surveill. 2017;22:pii=30464; 4. Public Health England. Influenza vaccine effectiveness in adults and children in primary care in the UK: provisional end-of-
15 season results 2016–17. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/641162/Influenza_vaccine_effectiveness_in_primary_care_1617_final.pdf.
Accessed October 2017.National uptake of free influenza vaccine
in eligible UK population
Flu season ≥ 65sThe burden of flu
Pauline MacDonald
Independent Nurse Consultant – Infection Matters Ltd
17Disclosures
• Pauline MacDonald has received an honorarium from Seqirus for her time spent
preparing this presentation
• She has received honoraria in the past from pharmaceutical companies including
Sanofi Pasteur and MSD
• Thanks to Public Health England for some of the data and figures included in this
Introduction copy
presentation
18What this talk will cover:
Objectives
• Revision of flu the disease and virus
• Challenges for flu immunisation and control
• Epidemiology and burden of influenza
- Particularly in the 65 years and over age-group
Introduction copy
19Influenza – Features
• Transmission:1
– Airborne droplets
– Articles such as handkerchiefs contaminated
by nasopharyngeal secretions
• Incubation: ~2 days2
• Virus shed: 5–10 days
Introduction copy
• Symptoms: Fever, headache, myalgia, fatigue, cough,
sore throat, stuffy nose, diarrhoea and vomiting3, no
symptoms4
• Complications: Bronchitis, otitis media, pneumonia,
meningitis, organ failure, death2,3
1. Centers for Disease Control and Prevention. Clinical signs and symptoms of influenza.
Available at: https://www.cdc.gov/flu/professionals/acip/clinical.htm. Accessed October 2017; 2. World Health Organization. Biologicals, Influenza. Available at:
20 http://www.who.int/biologicals/vaccines/influenza/en/. Accessed October 2017; 3. Dasaraju PV, Liu C. Chapter 93 Infections of the Respiratory System. Medical Microbiology 4th edition.
1996; 4. Hayward AC, et al Lancet Respir Med 2014;2:430-431.Influenza is a single-stranded, helical RNA virus
of the orthomyxovirus family
What causes influenza?
• There are four basic antigen types:1
– A – Multiple strains
– B – Two lineages: Victoria and Yamagata
– C and D – Not clinically relevant in humans
•Introduction
Influenza Acopy
virus subtypes are determined by their surface antigens in
human cells:2–4
– Haemagglutinin (HA):
Virus attachment
– Neuraminidase (NA):
Virus release Hemagglutinin Neuraminidase
• 18 “H” subtypes and 11 “N” subtypes
1. World Health Organization. Influenza (Seasonal). Fact sheet. Available at: http://www.who.int/mediacentre/factsheets/fs211/en/. Accessed October 2017; 2. World Health Organization. Biologicals,
21 Influenza. Available at: http://www.who.int/biologicals/vaccines/influenza/en/. Accessed October 2017; 3. Centers for Disease Control and Prevention. Available at:
https://www.cdc.gov/flu/avianflu/influenza-a-virus-subtypes.htm. Accessed October 2017; 4. World Health Organization memorandum Bulletin of the World Health Organization 1980;58:585-591.Influenza is a single-stranded, helical RNA virus
of the orthomyxovirus family
Type of Hemagglutinin Neuraminidase
nuclear material
Introduction copy
A/Fujian/411/2002 (H3N2)
Virus Geographic Strain Year of Virus
type location number isolation subtype
Standard nomenclature for isolated influenza viruses1
22
1. World Health Organization memorandum Bulletin of the World Health Organization 1980;58:585-591.Since 1977 influenza A (H1N1 and H3N2),
and influenza B have been in circulation
Influenza A is the most common circulating virus, however influenza
can be unstable and can undergo changes via antigenic drift/shift
• Flu A strains are more prone to drift/shift
than ‘more stable’ B strains
• New influenza virus subtypes due to Human
antigenic drift and shift (re-assortment) influenza virus
•Introduction
New influenza copy
subtypes increase potential
of epidemics or pandemics – people have
little or no protective immunity
New virus that
• Even minor changes can present Pig infected
with both has evolved by
genetic re-
a challenge for vaccine matching viruses
assortment
Avian
(antigenic shift)
influenza virus
• So why is all this important?....
23
World Health Organization. Biologicals, Influenza. Available at: http://www.who.int/biologicals/vaccines/influenza/en/. Accessed October 2017.Challenges for flu immunisation and control
Growing concern of low vaccine efficacy (VE) against influenza A(H3N2)1–3
• Influenza A(H3N2) disproportionately affects the elderly1
• 2016–17 (provisional) end-of-season vaccine effectiveness estimates
showed no significant effectiveness in ≥65 year olds3,4
- Thesecopy
Introduction results highlight the importance of effective vaccination
interventions to protect the elderly population
• It is important to consider immunosenescence as a factor when
vaccinating ≥65 year olds
*Provisional data.
1. Belongia EA, et al. Lancet Infect Dis 2016;16:942–51; 2. Kissling E, et al. Euro Surveill. 2017;22:pii=30464; 3. JCVI minute of the meeting on 7 June 2017. Draft minute. Available at:
24 https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/198733240440. Accessed October 2017; 4. Public Health England. Provisional end-of-season results 2016-17. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/641162/Influenza_vaccine_effectiveness_in_primary_care_1617_final.pdf. Accessed October 2017.Immune response is lower in elderly due to
immunosenescence
Immunosenescence: The effects of ageing on the immune system
Waning immunity with age (immunosenescence)1
and comorbidities (chronic diseases)
Reduced immune
Increased susceptibility to
response to infection and
and severity of infection1
Introduction copy vaccination1
Increased risk of hospitalisation2
Greater risk of disability3
Reduced quality of life3
Increased mortality rate3,4
25 1. Gavazzi G, Krause K-H. Lancet Infect Dis 2002;2:659–66; 2. Thompson WW, et al. JAMA 2004;292:1333–40; 3. McElhaney JE. Vaccine 2005;23:S10–S25; 4. Thompson WW, et al. JAMA
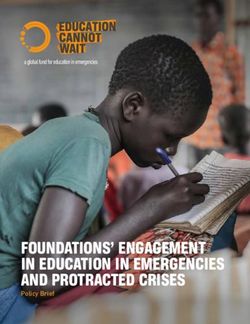
2003;289:179–86.Influenza epidemiology: 2016–2017
Weekly all age GP influenza-like illness rates
for 2016–2017 and past seasons, England (RCGP)
140 • Influenza activity usually between
130 September to March
120
110 • Impact of influenza varies from
100
90
year to year
80
70
• Biggest impact in 2016/17 in older
Introduction
60
copy adults:
50
40 • Increased care homes
30 outbreaks, and excess mortality
20 seen in ≥65 year olds
10
0
40 42 44 46 48 50 52 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 • High number of admissions to
Week number hospital and ICU/HDU admissions*
2010-11 2014-15 2015-16 2016-17
Baseline threshold Low Medium High Very high
*although lower than in past two seasons.
HDU, high dependency; IDU, intensive care unit; ILI, influenza-like illness; RCGP, Royal College of General Practitioners.
26 Public Health England (PHE) Surveillance of influenza and other respiratory viruses in the UK: Winter 2016 to 2017 [Online]. PHE, London.
Available at: https://www.gov.uk/government/statistics/annual-flu-reports. Accessed October 2017.Complications associated with influenza in the elderly
Influenza-like illness can increase Influenza-like illness can
the risk for other diseases exacerbate underlying conditions
Stroke1 and
Myocardial Heart Disease4
infarction2
Introduction copy
COPD5 and
Pneumonia3
Asthma6
Image: Tsyhun/Shutterstock.com.
COPD, chronic obstructive pulmonary disease.
*In patients vaccinated with trivalent influenza virus vaccine with or without intranasal live-attenuated, cold-adapted influenza vaccine.
1. Field TS, et al. Neuroepidemiology 2004;23:228–35; 2. Warren-Gash C, et al. Lancet Infect Dis 2009;9:601–10; 3. Rothberg MB, et al. Am J Med 2008;121:258–64; 4. Madjid M, et al.
27 Tex Heart Inst J 2004;31:4‒13; 5. Neuzil KM, et al. Clin Infect Dis 2003;36:169‒74; 6 Centers for Disease Control and Prevention. Flu and people with asthma. Available at:
http://www.cdc.gov/flu/asthma/. Accessed October 2017.Immunisation recommendations for the elderly
In 2000, the JCVI recommended influenza vaccination for over 65 year olds1
• The over 65 population are more vulnerable to morbidity and mortality caused by
influenza due to immunosenescence2,3
• In October 2017 JCVI have reviewed the influenza vaccination programme for the
over 65 population1
- Review needed due to poor vaccine effectiveness, recent dominance of A(H3N2)
Introduction copy
with high morbidity and mortality in the elderly, new vaccines entering the market
- Minutes of the meeting will be available mid-November
28 1. JCVI minute of the meeting on 7 June 2017. Draft minute. Available at: https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/198733240440. Accessed September 2017. 2. Baguelin M, et al. PLoS
Medicine 2013;10:e1001527; 3. Silva DAA, Palmer DB. Immunology 2007;120:435–46.Summary:
Think about your adults aged 65 and over1–5
Many factors contribute to increased risk of flu in adults aged 65 years and over:
Sub-optimal
Increased Age-related
effectiveness
incidence of IMMUNO
of current
co-morbidity SENESCENCE
Introduction copy vaccines
In adults aged 65 years and over:
there are much higher rates of preventable influenza-related complications,
including GP consultations, hospitalisations and death.
29 1. Gavazzi G, et al. Lancet Infect Dis 2002;2:659–66; 2. Ansaldi F, et al. Vaccine 2008;26:1525–9; 3. Thompson WW, et al. JAMA 2004;292:1333–40;
4. Thompson WW, et al. JAMA 2003;289:179–86; 5. Rivetti D, et al. Cochrane Database System Rev 2006(2):CD004876.Questions
Refrigerated transport – maintaining the cold chain!
30Personalising vaccination care
Dr Roger Henderson
Senior Partner in General Practice, and Media Medic
31Declarations
• Dr Roger Henderson has received an honorarium from Seqirus for his time spent
preparing this presentation
• He has received honoraria in the past from pharmaceutical companies including
Pfizer, GSK, Takeda and Novartis
Introduction copy
32What this talk will cover:
Objectives
• The downward trend in vaccine efficacy against influenza A(H3N2)
• Review of the current the influenza programme
• Strategies which could increase protection among the elderly
• Introduction to adjuvanted vaccines
Introduction copy
33A downward trend in vaccine efficacy against influenza
A(H3N2) has been observed in recent years1–3
In 2016/17 the vaccination rate in adults aged 65 years and over was 70.5%4
2016/17 cumulative influenza confirmed hospital
admissions by age group and influenza type
Number of admissions by influenza
900
• However, there was only 40% Influenza A(H3N2)
800
Influenza A (H1N1) pdm09
effectiveness in the adjusted 700 Influenza A (unknown subtype)
all-age vaccine effectiveness5
600 Influenza B
Introduction copy 500
• Vaccine effectiveness against
A(H3N2) was lowest in the over 400
65 years age group1 300
200
100
0Influenza A(H3N2) disproportionately affects the elderly1
A higher rate of ICU/HDU influenza-confirmed admissions were observed in adults
aged 65 years and over2
2016/17 cumulative influenza confirmed ICU/HDU
admissions by age group and influenza type
500
• ICU lab-confirmed admission Influenza A(H3N2)
450
Influenza A (H1N1) pdm09
rates*, with the largest numbers 400
Influenza A (unknown subtype)
of admissions in the over 65 350
Influenza B
years age group2 300
250
• Excess mortality reached 200
moderate levels, mostly seen in 150
the over 65 years age group2 100
50
0What is the solution?
What strategies could increase protection among the elderly?
1. Increase uptake among eligible groups to reduce transmission in communities
- Children, families, healthcare workers (in practices, hospitals and nursing homes etc.)
2. Achieve a higher vaccination rate among the elderly
3. Alternative route to IM/SC intradermal
Introduction copy vaccines…
4. More effective
36
IM, intramuscular; SC, subcutaneous.There are multiple factors influencing vaccine
effectiveness and disease burden in the ≥65 age group
Population Influenza strain Vaccine type Coverage
Matching of
Age-related
vaccine strain Vaccine type/
immunosenescence Flu campaigns
vs. circulating technology
and comorbidities
flu strain
Antigenic mismatch
Less effective
resulting in reduced Not all elderly
Insufficient immune vaccine resulting
Introduction copy
response 1
cross-reactive
in limited seek healthcare
antibodies2 provision4
protection1‒3
Strategies to reduce the disease burden include:
Accessing vaccines capable of eliciting better immune response
and improving clinical outcomes
to protect against influenza infection
TIV, trivalent influenza vaccine.
37 1. McElhaney JE. Aging Health 2008;4:603–13; 2. Ansaldi F, et al. Vaccine 2008;26:1525–9; 3. Jefferson T, et al. Cochrane Database System Rev 2010(2):CD004876; 4. Molinari NAM, et al. Vaccine
2007;25:5086–96.What influenza vaccines are currently available
for the UK 2017/2018 influenza season?
A trivalent or quadrivalent vaccine composition
• Trivalent vaccine comprising of:
- an A/Michigan/45/2015 (H1N1)pdm09-like virus
- an A/Hong Kong/4801/2014 (H3N2)-like virus
- a B/Brisbane/60/2008-like virus
• Introduction
Quadrivalentcopy
vaccine comprising of:
- The three viruses present in
the TIV vaccination
- a B/Phuket/3073/2013-like virus
BMI, body mass index; LIAV, live attenuated influenza vaccine; TIV, trivalent influenza vaccine; QIV, quadrivalent influenza vaccine.
*At-risk group now includes coeliac patients and morbidly obese patients (BMI >40).
38 Public Health England. National flu immunisation programme 2017/18. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600880/annual_flu__letter_2017to2018.pdf. Accessed October 2017.Licensed influenza vaccines available in the UK
influenza season 2017/181
Strain Route of Indicated UK
Vaccine type Product name
coverage administration age group
Influenza vaccine, surface antigen,
Inactivated;
inactivated (Mylan Products);
surface antigen; Trivalent Intramuscular ≥ six months old
Influenza vaccine surface antigen,
non-adjuvanted
inactivated (Seqirus UK)
Inactivated;
≥ six months old Inactivated influenza vaccine BP
split virion; Trivalent Intramuscular
(Sanofi Pasteur)
non-adjuvanted
Influenza vaccine, pre-filled
Introduction
Inactivated; copy syringe (Pfizer Vaccines);
split virion; Trivalent Intramuscular ≥ five years old
Influenza vaccine split virion,
non-adjuvanted
inactivated (Pfizer Vaccines)
Live attenuated; 24 months old to Influenza vaccine live attenuated,
Quadrivalent Intranasal
non-adjuvanted < 18 years old nasal (AstraZeneca)
Influenza vaccine split virion,
Inactivated;
inactivated (GlaxoSmithKline);
split virion; Quadrivalent Intramuscular ≥ three years old
Quadrivalent influenza vaccine
non-adjuvanted
(Sanofi Pasteur)
39 1. Public Health England. National flu immunisation programme 2017/18. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600880/annual_flu__letter_2017to2018.pdf. Accessed October 2017.Licensed influenza vaccines predicted to be available
in the UK influenza season 2018/191,2
Strain Route of Indicated UK
Vaccine type Product name
coverage administration age group
Influenza vaccine, surface antigen,
Inactivated;
inactivated (Mylan Products);
surface antigen; Trivalent Intramuscular ≥ six months old
Influenza vaccine surface antigen,
non-adjuvanted
inactivated (Seqirus UK)
Inactivated;
Trivalent Inactivated influenza vaccine BP (Sanofi
split virion; Intramuscular ≥ six months old
Pasteur)
non-adjuvanted
Influenza vaccine, pre-filled syringe (Pfizer
Inactivated;
Vaccines);
≥ five years old
Introduction copy
split virion;
non-adjuvanted
Trivalent Intramuscular
Influenza vaccine split virion, inactivated
(Pfizer Vaccines)
Inactivated; surface Surface antigen, inactivated, influenza
antigen; MF59C.1- Trivalent Intramuscular ≥ 65 years old vaccine adjuvanted with MF59C.1
adjuvanted (Seqirus UK)
Live attenuated; 24 months old to Influenza vaccine live attenuated, nasal
Quadrivalent Intranasal
nonadjuvanted < 18 years old (AstraZeneca)
Inactivated; Influenza vaccine split virion, inactivated
split virion; Quadrivalent Intramuscular ≥ three years old (GlaxoSmithKline); Quadrivalent influenza
non-adjuvanted vaccine (Sanofi Pasteur)
40 1. Public Health England. National flu immunisation programme 2017/18. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600880/annual_flu__letter_2017to2018.pdf. Accessed October 2017. 2. Seqirus Press Release. New influenza vaccine
offers improved protection for older adults. Available at: http://www.seqirus.com/newsroom/New-influenza-vaccine-offers-improved-protection-for-older-adults. Accessed October 2017.JCVI suggested that an adjuvanted trivalent influenza
vaccine may provide vaccine effectiveness in ≥65 years1,2
An adjuvanted trivalent influenza vaccine for those aged over 65 years could
potentially be used in the 2018/19 season
• Published studies indicated higher vaccine immunogenicity
and effectiveness for the adjuvanted vaccine in comparison
with non-adjuvanted vaccines
• In October 2017, the JCVI is considering the over 65 year
Introduction copy
olds component of the influenza immunisation programme
- These considerations may well generate advice
specifically with regard to protecting the elderly against
influenza
41 1. JCVI minute of the meeting on 7 June 2017. Draft minute. Available at: https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/198733240440. Accessed October 2017; 2. Seqirus Press Release. New
influenza vaccine offers improved protection for older adults. Available at: http://www.seqirus.com/newsroom/New-influenza-vaccine-offers-improved-protection-for-older-adults. Accessed October 2017.What are adjuvanted vaccines?
Adjuvants enhance the magnitude and breadth of the immune response1
Vaccines based on purified
Individuals with a naïve
or recombinant antigens
or weakened immune
may induce a suboptimal
system respond less
immune response in older
well to vaccines
adults
Introduction copy Why enhance the immune response?
Vaccine antigen
Vaccine-induced immunity
may not exactly match
may not be long-lasting in
the circulating
older adults
influenza virus strain
42
42 1. O’Hagan DT, et al. Drug Discov Today 2009;14:541–51.What adjuvanted influenza vaccines are available?
• Adjuvanted inactivated, surface antigen or aTIV contains an oil-in-water emulsion of
the adjuvant squalene – MF59C.1®1
• The adjuvant can potentially enhance antigen-specific immune response to vaccine
antigens resulting in:
- Higher antibody levels against all strains within the vaccine, when compared
against copy
Introduction conventional non-adjuvanted TIV
- Production of cross-protective antibodies against unmatched strains when they are
similar to those included in the vaccine2,3
- Longer persistence of antibodies, when compared to conventional non-adjuvanted
TIV3
43 1. O’Hagan DT, et al. Expert Rev Vaccines 2013;12:13-30; 2. Surface antigen, inactivated, influenza vaccine adjuvanted with MF59C.1 Summary of Product Characteristics October 2017; 3. Frey SE, et
al. Vaccine 2014;32:5027–34..LIVE study
Adjuvanted TIV: Real-world data
In peak influenza season, influenza-related or pneumonia-related hospitalisation was
significantly reduced when adults were vaccinated with aTIV compared with non-
adjuvanted TIV1
2
Reduction in risk of hospitalisation due to
(95%CI: 0.57, 0.98)
1.6
25% reduction in risk of hospitalisation
influenza or pneumonia
1.2
Vaccination with adjuvanted TIV significantly
Introduction
0.8 copy reduced risk of influenza-related or pneumonia-related
hospitalisations compared with non-adjuvanted TIV
0.4 during peak influenza season*†
0
TIV Adjuvanted TIV
Category 1
There was a greater risk in the adjuvanted TIV group of influenza-related hospitalisations
occurring before the influenza season.
This was due to age, functional limitations and higher rate of comorbidities.†
*Residual bias indicates that this value is likely to be an underestimate; †RRs were adjusted to address important confounding factors that contributed to the imbalance between aTIV and TIV groups
such as age, sex, influenza season, comorbidities, vaccine provider and functional status, Risk ratio: 1.17 (95% CI: 0.96–1.43).
44 aTIV, adjuvanted trivalent influenza vaccine; CI, confidence interval; RR, risk ratio; TIV, trivalent influenza vaccine.
1. Mannino S, et al. Am J Epidemiol. 2012;176:527–33.Canadian study
Adjuvanted TIV: Real-world data
Adjuvanted TIV had an absolute vaccine effectiveness of 58%*, whereas
conventional non-adjuvanted TIV was just as effective in the elderly population
when compared with unvaccinated subjects†1
2
(95%CI: 4.86, P=0.04)
Relative vaccine effectiveness as
compared to non-adjuvanted TIV
1.6
Introduction copy 63% higher relative vaccine effectiveness1
1.2
Adjuvanted TIV was 63% more effective
than non-adjuvanted TIV
0.8
0.4
0
TIV Adjuvanted TIV
Category 1
*(95% CI: 5–82, PPivotal Study: Solicited local adverse events
Pivotal clinical trial data adjuvanted TIV vs. conventional TIV1
100 aTIV (n=3505) TIV (n=3495)
80
Subjects (%)
1–7 days following vaccination
60
Introduction
40
copy
25
21
20 12 11
1 1 1 1 1Pivotal Study: Solicited systemic adverse events
Pivotal clinical trial data adjuvanted TIV vs. conventional TIV1
100 aTIV (n=3505) TIV (n=3495)
80
Subjects (%)
1–7 days following vaccination
60
Introduction
40
copy
20 15 13 10 13
9 9 8 7 7 5 5 5 4 3 3 3 2
1
0
Systemic adverse events
47 TIV, trivalent influenza vaccine. aTIV, adjuvanted trivalent influenza vaccine
1. Frey SE, et al. Vaccine 2014;32:5027–34.Summary:
Is it time to personalise vaccination care?
There is a growing concern of low vaccine efficacy against
influenza A(H3N2) in ≥65 year olds1,2
IntroductionThe provisional end-of-season vaccine effectiveness for 2016–
copy
17 estimates showed no significant effectiveness in ≥65 year
olds3
JCVI suggested that an adjuvanted trivalent influenza vaccine
may provide vaccine effectiveness in adults aged ≥65 years4
1. Belongia EA, et al. Lancet Infect Dis 2016;16:942–51; 2. Kissling E, et al. Euro Surveill. 2017;22:pii=30464; 3. Public Health England. Provisional end-of-season results 2016-17. Available at:
48 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/641162/Influenza_vaccine_effectiveness_in_primary_care_1617_final.pdf. Accessed October 2017; 4. JCVI minute of the
meeting on 7 June 2017. Draft minute. Available at: https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/198733240440. Accessed October 2017.How do we break the cycle?
Dr George Kassianos, Dr Roger Henderson
and Pauline MacDonald
49Pooled seasonal vaccine effectiveness
by influenza strain1
Vaccine improvements are needed to generate greater protection against influenza
A(H3N2) than with current vaccines
Older adults >60 years Working adults 20–60 years
90
80
Pooled Vaccine Effectiveness (%)
70
60
Introduction 50copy
40
30
20
10
0
-10
A(H3N2) A(H1N1) B
50
1. Belongia EA, et al. Lancet Infect Dis 2016;16:942–51.Persistence of influenza vaccine protection
Single season studies
• EU, UK, Australia
• Amount of ‘waning’ inconsistent across studies age group and flu-type1
• Decline in vaccine effectiveness within flu season most evident in influenza A(H3N2)1
• For influenza A(H3N2), vaccine effectiveness declined toPooled season adjusted vaccine effectiveness
(Five seasons)
Influenza A(H3N2)
• “…while there appears to be waning of vaccine effect over time, we cannot disentangle to what
extent this is due to virus change and subsequent non-matching of the vaccine, or loss of
vaccine-induced immunity within the individual”1
Overall season (all ages) Early season (all ages) Overall season (60 years and older)
Introduction copy
52 Figures from: Kissling E, et al. Euro Surveill. 2016;21:pii=30201.
1. Kissling E, et al. Euro Surveill. 2016;21:pii=30201.
52So what are the strategies that could increase
protection among adults ≥65 years?
The current need
Higher immune response:
1 Influenza vaccines are less effective in older adults due to immunosenescence
Breadth of protection:
2 Influenza
Introduction copy vaccines are even less effective in older adults during seasons
when drift and strain mismatch occur
Persistence:
3 Influenza vaccine effectiveness wanes significantly during the season
53Break
15 minutes
54Workshop sessions
Dr Roger Henderson:
Best Practice – interactive case study
Dr George Kassianos:
Practical guidance on adult influenza vaccination
55Workshop session
Dr Roger Henderson:
Best Practice – interactive case study
Senior Partner in General Practice, and Media Medic
56Best Practice –
Interactive case study
How do we achieve high influenza
vaccination uptake?
57Why can similar practices vary so much in their
influenza vaccination uptake?
Practice A Practice B
Semi-rural and in same town
Average of 15,000 patients each
Mainly social classes 1–3, relatively low social deprivation
Introduction copy Good literacy population
Practice A Practice B 27%
38%
Total uptake 62% Total uptake 73%
62%
73%
What factors could affect this? ?
58What are the top five key ways
for a practice to optimise
influenza vaccination uptake?
59Top five ways to optimise influenza
vaccination update in your practice
Have a lead member of staff with tenacity in overall charge of the
1 vaccination campaign
2 Set aspirational uptake targets
3 copy
Introduction Develop and use additional flu vaccination prompts in your IT system
4 Have GPs and practice nurses who opportunistically vaccinate
5 Use phone calls and text reminders (mJog) to invite patients
60What are the simple steps
required to change behaviour in
your practice in order to optimise
uptake?
61Plan/Invite/Provide/Review principles
Plan:
By identifying lead member - running campaign and another who will identify
all eligible patients. Modify practice IT searches to achieve this if needed
Invite:
Send a personal invitation to all eligible patients, and collaborate with community
midwives too
Introduction copy
Provide:
Allocate appointments as well as walk-in sessions in order to increase attendance.
Continue when QOF targets reached
Review:
Document uptake rates in a written report to all staff, especially those leading
the campaign
62How can we optimise
influenza vaccination uptake
without patient hesitancy?
63Improving vaccination uptake without
causing patient hesitancy
Use a separate Read code for
Start vaccinating as soon vaccination bookings to facilitate
as vaccine arrives follow-up of non-attenders
Send prompt reminders to Ensure all patients receive
Introduction copy
patients who do not respond accurate information about
to invitation vaccination benefits
Review vaccine uptake Aim to complete vaccinations
fortnightly to allow targeting by end of Oct/early Nov, although
of shortfall areas continue vaccinations after this
64How can we measure the impact
of our initiatives to build in a
solutions-driven feedback loop?
65Workshop session
Dr George Kassianos:
Practical guidance on adult influenza vaccination
MD (Hons), FRCGP, FESC, FBGTHA, FFTM RCPS (Glasg), FBHS, FHEA,
FAcadMEd, DRCOG, LRCP (Edin.), LRCS (Edin.), LRCP&S (Glas.),
DMedAcup., DMedHypn., DFP.
66Annual flu programme 2017/18 flu season1
Introduction copy
67
1. Public Health England. 2017 to 2018 flu season. Available at: https://www.gov.uk/government/collections/annual-flu-programme#2017-to-2018-flu-season. Accessed October 2017.Immunisation training resources
for healthcare professionals1,2
• Immunology for immunisers animation
• e-Learning immunisation resources
- Influenza Knowledge Transfer Series
Specific on the burden of seasonal
influenza in an older adult population
- Accredited by the Royal College of
General copy
Introduction Practitioners (RCGP)
• Immunisation knowledge and skills
competence assessment tool
• Slide sets for core curriculum teaching
• Quality framework to support the
implementation of national standards
and guidelines on immunisation training
1. Public Health England. Immunisation. Immunisation training resources for healthcare professionals. Available at: https://www.gov.uk/government/collections/immunisation#infographics. Accessed
October 2017; 2.. mdBriefCase™. Influenza Knowledge Transfer series. Available at:
68 http://www.mdbriefcase.net/uk/influenza?regionID=16&utm_source=RCGP&utm_medium=Referral&utm_campaign=FLU%20KTS&utm_content=UK%20EN%20FLU%20RCGP%20Social%201.
Accessed October 2017Patient Group Directions (PGDs)1
Introduction copy
69
1. Immunisation patient group direction (PGD) templates. Available at: https://www.gov.uk/government/collections/immunisation-patient-group-direction-pgd. Accessed October 2017.GP vaccination of children aged between
two and three years old1,2
Children who are not yet four on 31 August 2017*
• All children: One dose of influenza vaccine live attenuated, nasal
• If first ever flu vaccination and in ‘at risk groups’: Two doses at least four weeks apart
• If influenza vaccine live attenuated, nasal contraindicated AND child in a ‘group at risk’:
- TIV children 6 months toGP vaccination of children 4 to 8 years of age1,2
• Local NHS England teams will commission
this service:
- Local providers
- Predominantly in primary school settings
• GPs can immunise children of this age in
the ‘at risk groups’*
Introduction copy particularly if not
vaccinated at school
* At risk children include those who have a long-term health
condition, such as: asthma and other respiratory diseases,
liver, kidney, neurological conditions including learning
disabilities (even if well managed)
1. Public Health England. The national flu immunisation programme 2017/18. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600880/annual_flu__letter_2017to2018.pdf. Accessed October 2017.
71 2. Public Health England. Which flu vaccine should children have?. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/619722/Children_flu_vaccine_graphic.pdf.
Accessed October 2017.PGD for QLAIV1
Introduction copy
72 1. Public Health England. Live attenuated influenza vaccine (Fluenz Tetra®): Patient group direction (PGD) template. Available at: https://www.gov.uk/government/publications/influenza-vaccine-
fluenz-tetra-patient-group-direction-pgd-template. Accessed October 2017.The 2017/18 GP programme1,2
Introduction copy
1. Public Health England. Flu vaccine for children: best practice guide for GPs. Available at: https://www.gov.uk/government/publications/flu-vaccine-best-practice-guide-for-gps. Accessed October
73 2017; 2. Public Health England. Flu vaccination: Who should have it this winter and why. Available at: https://www.gov.uk/government/publications/flu-vaccination-who-should-have-it-this-winter-and-
why. Accessed October 2017.Annual influenza vaccination 2017/18 campaign1
Introduction copy
74 1. Public Health England. The national flu immunisation programme 2017/18. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600880/annual_flu__letter_2017to2018.pdf.. Accessed October 2017.Which groups are to be vaccinated?1,2
Influenza vaccination groups
• All children aged two and three years old • Children in former primary school ‘pilot areas’
(by GPs)
• People in long-stay Residential Homes
• Children aged four to eight years old – not prisons, young offenders institutions,
(vaccinated at schools) university halls
• All patients aged ≥65 years on 31/03/2018 • Carers – those on carer’s allowance, main
carer of elderly, child or disabled persons
•Introduction
All pregnantcopy
women – at any stage of
pregnancy • Health and Social Care Staff - in direct
contact with patients: Employers finance
• ‘At risk’ groups – aged between six months
vaccination
to 64 years old
• Locums (via their registered GP)
• Other only at GP’s discretion
1. NHS England. Directed Enhanced Service Specification. Available at: https://www.england.nhs.uk/wp-content/uploads/2017/03/sfl-pneumococcal-2017-18-service-specification.pdf . Accessed
75 October 2017. 2. NHS England. Flu Plan Winter 2017/18. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600532/annual_flu_plan_2017to2018.pdf.
Accessed October 2017.Who are patients in the ‘at risk’ groups?1
Influenza vaccination for at risk groups in those aged six months to 64 years old
• Chronic respiratory disease: • Chronic kidney disease:
Asthma on inhaled or oral steroids, COPD, Stage 3–5, nephrotic syndrome, transplant
interstitial lung disease, cystic fibrosis,
• Chronic neurological disease:
Pneumoconiosis, bronchopulmonary
Stroke, TIA, Polio, MS, cerebral palsy,
dysplasia, children with LRT disease
learning disorders, Parkinson’s, MND
• Chronic heart disease:
Introduction copy • Diabetes
Congenital, HF, coronary heart disease,
hypertension with cardiac complications • Asplenia, splenic dysfunction:
Homozygous sickle cell disease, coeliac
• Chronic liver disease:
disease-may lead to hyposplenism
Cirrhosis, biliary atresia, chronic hepatitis
• Immunosuppression:
• Morbidly obese:
Active disease or treatment, oral
BMI ≥40
prednisolone ≥20mg for >1 month or child
≥1mg per kg body weight per day
COPD, chronic obstructive pulmonary disease; HF, heart failure; LRT, lower respiratory tract infection; MND, motor neurone disease.
76 1. NHS England. Flu Plan Winter 2017/18. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600532/annual_flu_plan_2017to2018.pdf. Accessed October
2017.GPs Enhanced Service (ES)1,2
Fee: ES £9.80 per dose
• Age ≥65 years on 31 March 2018
• Pregnant women
• Children aged 2 and 3 years old
• Patients in the ‘at risk’ groups aged 6 months toPharmacists influenza vaccination service1
Fee: £9.14 per dose
(Fee: £7.64 plus additional fee in recognition of providing the service in the community £1.50)
• Age ≥65 years old
• Pregnant women
• Patients ‘at risk’ aged 18 toQuality and Outcomes Framework (QOF) for GPs1
Payment
Indicator Points
stages (%)
CHD 004: % of patients with CHD who have a record of flu
vaccination in the preceding 1 September – 31 March 7 56–96
STROKE 006: % of patients with TIA or Stroke who have had flu
vaccination in the preceding 1 September – 31 March 2 55–95
Introduction copy
COPD 006: % of patients with COPD who have a record of flu
vaccination in the preceding 1 September – 31 March 6 57–97
Diabetes Mellitus 10: % of patients with DM who have had
influenza vaccination in preceding 1 September to 31 March 3 55–95
Total 18 points x £171.20 = £3,082 [For 7,460 patients – England]
CHD, coronary heart disease; COPD; chronic obstructive pulmonary disease; DM, diabetes mellitus; TIA, transient ischaemic attack.
79 1. Summary of changes of QOF 2017/18 – England. Available at: http://www.nhsemployers.org/~/media/Employers/Documents/Primary%20care%20contracts/QOF/2017-
18/201718%20Quality%20and%20outcomes%20framework%20summary%20of%20changes.pdf. Accessed October 2017.PGD for intramuscular inactivated influenza vaccine1
Inactivated influenza vaccine
Introduction copy
80 1. Intramuscular inactivated influenza vaccine: patient group direction (PGD) template. Available at: https://www.gov.uk/government/publications/intramuscular-inactivated-influenza-vaccine-patient-
group-direction-pgd-template. Accessed October 2017.I had my flu vaccine
Have you?
Introduction copy
81General Medical Council:
UK’s regulating body for doctors
Good medical practice1 – issued February 2013
Getting an annual
influenza vaccination:
A professional responsibility
Introduction copy
82
1. General Medical Council. Good medical practice 2013. Available at: http://www.gmc-uk.org/guidance/good_medical_practice.asp. Accessed October 2017.What about other HCPs?
Nurses, Midwives and Health Visitors as per the NMC Code1
“Take all reasonable personal precautions necessary to avoid any
potential health risks to colleagues, people receiving care and the public”
Others such as Physiotherapists, Radiographers, Paramedics registered
Introduction copy
with the Health and Care Professionals Council:2
“You must take all reasonable steps to reduce the risk of harm
to service users, carers and colleagues as far as possible”
83 1. Nursing and Midwifery Council. The code for nurses and midwives. Available at: https://www.nmc.org.uk/standards/code/. Accessed October 2017; 2. Health and Care Professionals Council.
Standards of conduct, performance and ethics. Available at: http://www.hcpc-uk.org/assets/documents/10004EDFStandardsofconduct,performanceandethics.pdf. Accessed October 2017.Summary of key learnings
and faculty questions
Dr George Kassianos, Dr Roger Henderson
and Pauline MacDonald
84Closing remarks
Dr George Kassianos
85Please complete
your evaluation form,
which will be provided via an
email link
86A certificate of attendance will be provided via an
email link
You can apply for 3 continuing professional
development (CPD) credits from the Federation of the
Royal Colleges of Physicians
87Please switch
your mobile
phone back on!
88Thank you! 89
Fluad® Prescribing information:
Fluad® suspension for injection in pre-filled syringe (CTAB), barium sulphate, or in anyone who has had an following have been reported post-marketing:
Influenza Vaccine (surface antigen, inactivated, anaphylactic reaction to previous influenza thrombocytopenia, lymphadenopathy, asthenia,
adjuvanted with MF59C.1) Presentation: Each 0.5ml vaccination. Immunisation shall be postponed in influenza-like illness, extensive swelling of injected
of Fluad® contains 15 micrograms of each of three patients with febrile illness or acute infection. limb, injection-site cellulitis-like reaction, allergic
purified influenza virus antigens prepared from the Warnings and Precautions: Appropriate medical reactions including anaphylactic shock (in rare cases),
strains of influenza virus that comply with the WHO treatment and supervision should be readily available anaphylaxis, angioedema, vasculitis with transient
recommendations (Northern Hemisphere) and EU in case of an anaphylactic event following renal involvement, and neurological disorders such as
decision for the 2016/17 season: A/California/7/2009 administration. Do not inject intravascularly or encephalomyelitis, Guillain-Barré syndrome,
(H1N1) pdm09-like strain (A/California/7/2009, NYMC subcutaneously. Endogenous or iatrogenic convulsions, neuritis, neuralgia, paraesthesia,
X-181) 15 micrograms haemagglutinin, A/Hong immunosuppression may result in insufficient antibody syncope, and presyncope. Overdose: Overdosage is
Kong/4801/2014 (H3N2)-like strain (A/Hong response. Latex-sensitive individuals: Although no unlikely to have any untoward effect. Legal Category:
Kong/4801/2014, NYMC X-263B) 15 micrograms natural rubber latex is detected in the syringe tip cap, POM. Package Quantities: Packs of 1 or 10 pre-filled
haemagglutinin, B/Brisbane/60/2008-like strain the safe use of Fluad® in latex-sensitive individuals syringes. Marketing Authorisation Number: UK: PL
Introduction copy
(B/Brisbane/60/2008, wild type) 15 micrograms has not been established. Interactions: No clinical 46752/0001. Basic NHS Cost: £9.79 per 0.5ml pre-
haemagglutinin, with adjuvant MF59C.1 (9.75mg data on concomitant administration with other vaccines filled syringe, £97.90 per 10 pack. Marketing
squalene, 1.175mg polysorbate 80, 1.175mg sorbitan are available. If Fluad® needs to be used at the same Authorisation Holder: Seqirus S.r. l., Via Fiorentina 1,
trioleate, 0.66mg sodium citrate, 0.04mg citric acid, time as another vaccine, immunisation should be 53100 Siena, Italy
water). Indications: Active immunisation against carried out on separate limbs. It should be noted that For full prescribing information and details of other
influenza in the elderly (65 years of age and over), the adverse reactions may be intensified. Pregnancy side effects see the Summary of Product
especially for those with an increased risk of and Lactation: Not applicable. Effects on ability to Characteristics at www.gov.uk/pil-spc
associated complications. Dosage and drive and use machines: Fluad® has Date of preparation: August 2017 UK/FLUD/0717/0015
Administration: Intramuscular injection into the deltoid no or negligible influence on the ability to drive and use ®Registered trade mark Seqirus S.r.l, Italy
muscle using a 1-inch needle. Adults aged 65 years machines. Side Effects: The most common reactions
Adverse events should be reported. Reporting forms
and over: Single dose 0.5ml. Contra-indications: are headache, myalgia, injection site pain and
and information can be found at
Hypersensitivity to the active substances, components tenderness, fatigue, nausea, diarrhoea, vomiting, www.mhra.gov.uk/yellowcard. Adverse events relating
of the adjuvant, excipients, to chicken or egg proteins sweating, arthralgia, fever, malaise, and shivering; to Seqirus products should also be reported to Seqirus
(such as ovalbumin), kanamycin, neomycin sulphate, local reactions include redness, swelling, ecchymosis, Vaccines on 01748 828816
formaldehyde, cetyltrimethylammonium bromide and induration. Uncommon reactions include rash. The
90Lunch is
now available
91You can also read