BEYOND THE CLINIC: Remote Spirometry Data Collection in Respiratory Diseases - A WHITEPAPER FROM KONEKSA - Koneksa Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BEYOND THE CLINIC: Remote Spirometry Data Collection in Respiratory Diseases A W H I T E PA P E R F R O M KO N E K S A

E X EC U T I V E S U M M A RY
Spirometry is a key technology to assess lung function; it provides important data
for the diagnosis and monitoring of disease and for the measurement of treatment
efficacy. However, its deployment in clinical practice and research presents both
unique challenges and opportunities.
One of these is remote data collection. Moving spirometry out of the clinic can offer
opportunities for collecting more data in settings reflective of patients’ day-to-day
activities, while also improving the patient experience.
Valid questions about ensuring patient compliance and the quality of the data
in mobile spirometry have historically existed, but recent studies (Kerwin et al.,
Rodriguez-Roisin et al.,) have demonstrated that the data collected by means of
mobile spirometry is comparable to clinic spirometry, and that the mobile spirometry
technique itself offers additional advantages. These advantages include gathering
dense data points (enabling researchers to adjust for the hours of the day and the
seasons of the year), engaging patients to be active participants, and offering greater
convenience to patients.
This whitepaper will discuss the evolution of mobile spirometry techniques and its
current potential in respiratory disease clinical trials. It also offers considerations
for the implementation of best practices and presents results from a recent study
supporting mobile spirometry’s use in clinical research (Huang et al.,).
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 2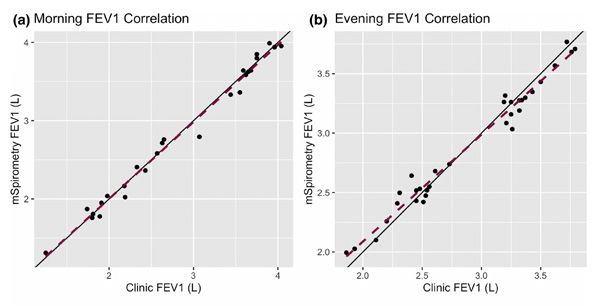
S P I R O M E T RY B E YO N D T H E C L I N I C
Spirometry is a foundational tool for the evaluation of the health of the pulmonary system
and is used routinely for diagnosis and treatment monitoring. Conventionally, spirometry
assessments are completed during a visit to the doctor’s office. These measures have been
in use since the 19th century and are instrumental in respiratory disease clinical practice.
The major drawback of a clinical spirometry assessment is the need for a patient to go to a
doctor’s office. The symptoms of airway diseases vary in a number of parameters over time.
These include diurnal variability, as well as seasonal and environmental changes due to factors
like air pollution or pollen counts. To get a more robust picture of disease fluctuations over
time, more frequent assessments are needed.
PERFORMING MOBILE SPIROMETRY TESTS OUTSIDE OF THE CLINIC PRESENTS
AN OPPORTUNITY TO ADDRESS THESE CONCERNS.
The development of reliable hand-held spirometers (used in combination with mobile
applications) facilitates the performance of the test procedure without direct supervision
by a healthcare professional, along with data collection and transmission, and provides an
opportunity to move spirometry from the clinic into a patient’s daily life.
While the advantages of mobile spirometry are evident (patient convenience, better
engagement, and more frequent, dense data), concerns have existed related to the data
quality. Some factors may impact the quality of mobile data collection.
• Did the person engage in any physical activity immediately before taking a test?
• Did the person sit or stand while taking the test?
• Did the person move while taking the test?
Moreover, performing a pulmonary function test takes effort on the part of the patient.
Will people put their best effort into performing a test unsupervised?
All of these questions were raised before the COVID-19 pandemic and became more pressing
as quarantine restrictions were put into effect, with the American Thoracic Society (ATS)
urging healthcare professionals to keep clinic visits to an absolute minimum to reduce the
risk of infection to patients (who are among the most vulnerable). Fortunately, answers
to these concerns are becoming clearer, pointing to the potential for mobile spirometry to
be a solution for both care delivery and clinical trials.
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 3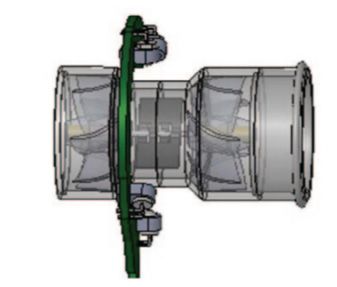
T H E P OW E R O F M O B I L E S P I RO M E T RY I N
CLINICAL TRIALS
Mobile spirometry moves this pulmonary function test out of the clinic by means of small,
handheld, Bluetooth-enabled spirometry devices working in conjunction with an application
on the patient’s smartphone. The mobile spirometer electronically records the data. Later,
the data is transmitted to the cloud via a phone application, which also documents patient
compliance and confirms for the patient whether the data-collection maneuver has been
performed satisfactorily.
WHAT DOES MOBILE SPIROMETRY BRING TO THE TABLE, IN ADDITION TO
ADDRESSING COVID-19–RELATED SAFETY CONCERNS?
SAMPLE SIZE REDUCTION
The repeated measures and dense data of mobile spirometry increase statistical degrees
of freedom, allowing researchers to control for factors that drive variation in spirometry
measures, such as FEV1. Having a higher number of measures means that the statistical
models assessing the effect of a treatment can be adjusted for parameters such as time of
the day, weather factors, or pollen counts. This also means that the same conclusions can
be drawn from studies with fewer participants as compared to larger studies that use only
infrequent clinic spirometry measures.
Figure 1
Huang, C., Izmailova, E.S., Jackson, N., Ellis, R., Bhatia, G., Ruddy, M. and Singh, D. Remote FEV1 monitoring in
asthma patients: a pilot study. Clin Transl Sci. (2020). https://doi.org/10.1111/cts.12901
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 4PROOF OF CONCEPT (POC) STUDIES
Mobile spirometry can have an impact on POC study design. Instead of doing a POC study in
a broad population (a concept often criticized for being underpowered and not representing a
population of patients recruited in pivotal studies (Patel et al.,), the study can be done in well-
defined patient populations, drawing conclusions that may enable a Phase 3 study design and
increase the probability of technical success. Doing a POC study in subpopulations can enable
personalized medicine approaches, increasing the benefit of giving treatment to the right
patients and minimizing the occurrence of side effects with no added benefit.
ADDITIONAL BENEFITS
Dense data collection through mobile spirometry can ascertain the trajectory of disease
change with greater confidence than sparse data collected in the clinic. The conventional way
of drawing conclusions in airway diseases is to compare the results of an FEV1 test taken at
baseline, with the same test taken at the end of the study. This approach introduces the risk
of a random anomalous test impacting the results, which drives up the number of subjects to
be recruited and the cost of clinical studies.
Frequently collected data eliminates this risk, with the added benefit of gathering the data
in a natural patient environment, doing so more conveniently for patients, and allowing
compliance monitoring in near real time.
SAMPLE MEASURES
• FEV1, FVC & Flow-Volume Loop
• Expiratory & Tidal Volume
• Inspiratory & Expiratory Reserve Volume
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 5B E S T P R AC T I C E S I N M O B I L E S P I RO M E T RY
DEVELOP TRIAL DESIGNS THOUGHTFULLY. While mobile spirometry offers many benefits in
terms of the data it provides, caution and careful consideration are still needed. Studies must be
designed thoughtfully with adequate endpoints and fit-for-purpose measures. Reduced sample
size does diminish generalizability of the results; a larger patient population with more variable
demographics and disease features may produce somewhat different results. The mitigation
strategy to address this concern can include utilizing adaptive study designs or conducting studies
in several well-defined populations (see above).
While mobile spirometry mitigates some of the data variability issues inherent to in-clinic measures
requiring a large number of participants, it can introduce other points of variability as the patient
conducts the measures, such as a suboptimal effort on the patient’s behalf.
ENSURE APPROPRIATE PROCEDURES FOR MOBILE DATA COLLECTION IN CONJUNCTION
WITH SPIROMETER CHOICE AND PATIENT INSTRUCTION. When considering or choosing a
mobile spirometer, it is important to ensure that the device can perform in the following ways to
obtain useful, trustworthy data (McCarthy):
• Meet the standards of the American Thoracic Society (ATS) and European Thoracic Society
(ERS) for low airflow measurement
• Inform the patient whether they performed the test according to ATS/ERS requirements
• Measure full flow volume loops
• Maintain ATS/ERS standards without requiring daily calibration
OFFER STUDY PARTICIPANTS THOROUGH TECHNICAL SUPPORT. Make sure that patients have
the tools and encouragement they need to be as compliant and successful as possible in their data
capture. For instance, they can be offered:
• A manual with clear, step-by-step, illustrated instructions
• Easy ways to contact their site if they need technical support
• Monitoring data collection compliance for fast support and issue mitigation
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 6PAT I E N T E N G A G E M E N T & E M P O W E R M E N T
With mobile spirometry, patients may feel increasingly empowered as they become active
participants, rather than passive recipients, in their own care. This may be true whether they
are using mobile spirometry tools as part of their standard care or in a clinical trial.
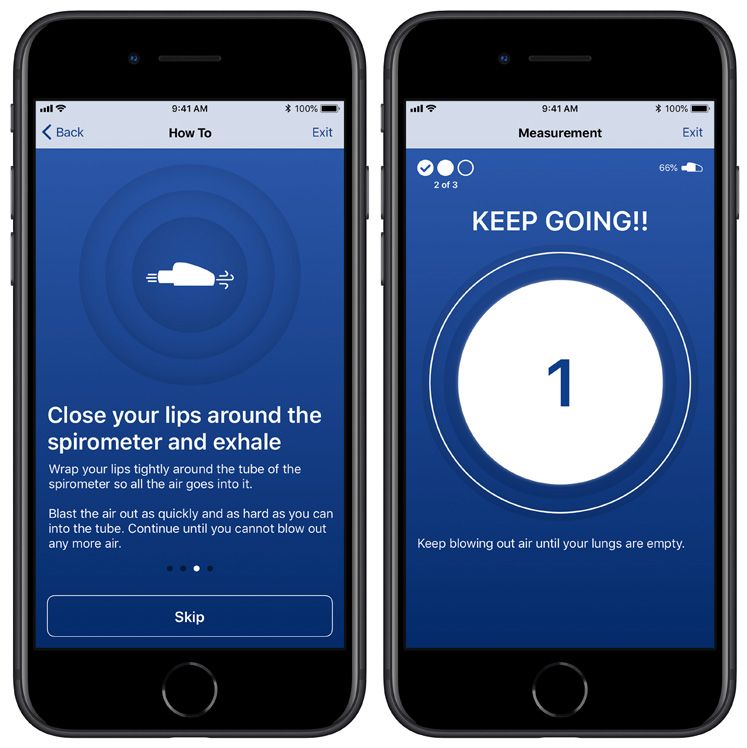
A well-designed patient application deployed with a mobile spirometer will be easy and
pleasant to use. This technology provides instructions, audio coaching through the procedure,
immediate feedback, and helpful alerts and reminders.
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 7LOOKING AHEAD
Mobile spirometry has been found to offer patients and researchers a portable, connected tool
that is more cost-efficient per data point to improve clinical trials in respiratory conditions.
Following the success of a recent pilot study, Koneksa seeks to conduct a larger study with
approved medications, such as montelukast or tiotropium, to achieve two key aims:
• Confirm results that the treatment effect can be observed with a smaller number
of study participants
• Extend findings to a broader disease population, such as patients in
different stages of asthma or COPD
Pilot Study in Clinical and Translational Science
Researchers from Koneksa, Regeneron Pharmaceuticals, and the University of
Manchester sought to investigate patient compliance in performing mobile spirometry
daily, establish concordance between mobile and in-clinic spirometry, and assess the
reliability of both measures in a recent publication in Clinical and Translational Science
(CTS). The pilot study results demonstrated good patient compliance, high correlation,
tight limits of agreement between mobile and clinic counterparts, and excellent test-
retest reliability for both measures. Moreover, mobile spirometry provided increased
statistical power, suggesting a potential for use in asthma clinical research.
Huang, C., Izmailova, E.S., Jackson, N., Ellis, R., Bhatia, G., Ruddy, M. and Singh, D. Remote FEV1
monitoring in asthma patients: a pilot study. Clin Transl Sci. (2020). https://doi.org/10.1111/cts.12901
Figure 2
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 8TERMINOLOGY
FEV1 – Forced expiratory volume in one second measurement inaccuracy if not replaced according
(FEV) is a measurement of the amount of air that a to manufacturer specifications. Disposable turbines
patient can exhale in the first second of the FVC test may incur significantly higher overall lifetime costs.
(see below).
Figure 3
FVC – Forced vital capacity (FVC) is a test that uses
a spirometer to measure the maximum amount of air
that a patient can forcefully exhale after inhaling as
much as possible.
Lung function tests – Lung function tests, or
pulmonary function tests (PFTs), are measurements
of how well a patient’s lungs function. The simplest
PFT is spirometry.
SVC – Slow vital capacity (SVC) is a test that uses McCarthy, K. Selecting spirometers for home testing.
a spirometer to measure the maximum amount of Respiratory Therapy. 12, 4 (2017). http://monitoredrx.
air that a patient can slowly exhale after inhaling as com/wp-content/uploads/2019/07/RT-McCarthy_
much as possible. The difference between FVC and testing_article.pdf
SVC has been found to be greater in overweight or
obese patients, and researchers have suggested that Ultrasonic spirometer – An ultrasonic spirometer
it can help to more accurately diagnose respiratory measures airflow using two ultrasonic transducers that
disease in these patients. emit sound pulses and measure their changes. It has
no moving parts, which permits increased accuracy,
Spirometer – A spirometer is a device that measures repeatability, and calibration stability. Its measurement
how much air a patient is able to inhale or exhale is independent of temperature, humidity, air pressure,
through their mouth. and other potential sources of error.
Spirometry – Spirometry is an assessment of how Figure 4
much air a patient’s lungs inhale, and how much, and
how quickly, their lungs exhale. The data gathered
from this activity is used to diagnose conditions
that affect the lungs, monitor lung condition, and
measure the efficacy of treatments.
Turbine spirometer – A turbine spirometer measures
airflow by directing it, using swirl plates, past a
vane, the spin of which is monitored and counted
by infrared beams that pass over it. The spin of the
McCarthy, K. Selecting spirometers for home testing.
turbine can sometimes cause a vibrating feeling in
Respiratory Therapy. 12, 4 (2017). http://monitoredrx.
the patient’s airway. Turbine spirometers may have
com/wp-content/uploads/2019/07/RT-McCarthy_
difficulty measuring extremely low airflow. Wear and
testing_article.pdf
tear on the moving parts of the turbine may induce
Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 9REFERENCES Remote FEV1 Monitoring in Asthma Patients: A Pilot Study. Huang, C., Izmailova, E.S., Jackson, N., Ellis, R., Bhatia, G., Ruddy, M., & Singh, D. Clin Transl Sci. (2020). https://ascpt.onlinelibrary.wiley.com/doi/abs/10.1111/cts.12901 Relationship Between Handheld and Clinic-Based Spirometry Measurements in Asthma Patients Receiving Beclomethasone. Kerwin, E.M., Hickey, L. & Small, C.J. Respir Med. 151, 35-42 (2019). https://doi.org/10.1016/j. rmed.2019.03.010 Selecting Spirometers for Home Testing. McCarthy, K. Respiratory Therapy. 12, 4 (2017). http://monitoredrx.com/ wp-content/uploads/2019/07/RT-McCarthy_testing_article.pdf Phase 2 to Phase 3 Clinical Trial Transitions: Reasons for Success and Failure in Immunologic Diseases. Patel, D.D., Antoni, C., Freedman, S.J., Levesque, M.C., Sundy, J.S. Paradigms and perspectives. 140, 3, 685-687 (2017). https://doi.org/10.1016/j.jaci.2017.04.029 Daily Home-Based Spirometry During Withdrawal of Inhaled Corticosteroid in Severe to Very Severe Chronic Obstructive Pulmonary Disease. Rodriguez-Roisin, R., et al. Int J Chron Obstruct Pulmon Dis. 11, 1973-1981 (2016). https://doi.org/10.2147/COPD.S106142 Beyond the Clinic: Remote Spirometry Data Collection in Respiratory Diseases PAGE 10
We’d love to talk. Contact us today to discuss how Koneksa can help you introduce mobile spirometry in your respiratory disease clinical research. hello@koneksahealth.com www.koneksahealth.com
You can also read