Asahi Kasei 2019 Annual Benefits Enrollment Highlights Book - APNA On Boarding
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Asahi Kasei
2019 Annual Benefits Enrollment
Highlights Book
1
Table of Contents
Who to Contact ............................................................................................ 3
Important Notices ......................................................................................... 5
Medical Coverage ........................................................................................ 6
Preferred Provider Organization (PPO 2 & A) ..................................... 7
Consumer Driven Health Plan (CDHP) ............................................... 8
Prescription Drugs .............................................................................. 9
Health Savings Account (HSA) ......................................................... 10
Medical Benefits Summary ............................................................... 12
Preventive Care ................................................................................ 15
Teladoc .............................................................................................. 16
Health Advocate ......................................................................................... 18
Dental Coverage ........................................................................................ 19
Dental Benefits Summary ................................................................. 20
Employee Assistance Program (EAP)......................................................... 22
Vision Coverage........................................................................................... 23
Vision Benefits Summary...................................................................24
Life and Accidental Death & Dismemberment (AD&D) .............................. 26
Disability ..................................................................................................... 28
Legal Shield and Identity Theft Shield ........................................................ 29
Flexible Spending Accounts (FSA) ............................................................. 30
2
Who to Contact
Plan: Administered by: Is there an App for that?
Blue Cross Blue Shield of North Carolina Search for
Medical & (877) 275-9787
BlueConnectNC
Prescription www.bluecrossnc.com or
Drugs www.blueconnectNC.com
Delta Dental of North Carolina Search for Delta
Dental
(800) 662-8856
Dental
www.deltadentalnc.com
United Healthcare (UHC)
Vision
(800) 638-3120 ▪ www.myuhcvision.com
Phone: (866) 695-8622 Search for Health
www.HealthAdvocate.com/members Advocate; enter
Health Advocate Asahi Kasei as the
(enter “Asahi Kasei”) organization
Flores & Associates
Flexible Search for Flores e-
Spending (800) 532-3327
Receipt
Accounts www.flores247.com
Health Equity
Health Savings (866) 346-5800 Search for Health
Account Equity
www.healthequity.com
(800) 654-7757
Legal Shield Search for Legal
www.legalshield.com
Shield
(888) 494-8519
Identity Theft www.idshield.com Search for ID
Shield Shield
Transamerica
(800) 755-5801 Search for
401(k) Transamerica
Retirement Plan asahikasei.trsretire.com (do not put www
before the address)
Lisa: (517) 223-5102
Asahi Kasei Meghan: (517) 223-5191
Benefits Email: asahi-benefits@ak-america.com
Help Net Employee Assistance Program (EAP)
EAP (800) 969-6162 ▪ www.helpneteap.com
3
4

Important Notices
Qualified (Mid-Year) Changes in
Status Please keep in mind:
Your benefit elections will be in effect for the 1. The change you make must be consistent
entire plan year (January 1st through with the event. For example, if you get
December 31st). You may only change your married, you may add your new spouse to
benefit elections during the plan year if you have your coverage.
a qualified change in status as defined by the
Internal Revenue Code and as allowed by the 2. Furthermore, the change must be requested
underlying carrier or vendor. within 30 days of the event. If you do not
notify us within 30 days, you must wait until
the next annual enrollment period to make a
change to your benefits.
3. Lastly, in most cases, the election change
must be made prior to the effective date.
HIPAA Notice of Special Enrollment
Rights
Changes in status include:
If you are declining enrollment for yourself or
Birth, placement for adoption, or your dependents because of other health
adoption of a child, or being subject coverage, you may be able to enroll yourself and
to a Qualified Medical Child Support your dependents in this Plan if you or your
Order which requires you to provide dependents lose eligibility for that other
medical coverage for a child. coverage (or if the employer stops contributing
towards your or your dependents’ other
Marriage, legal separation, coverage).
annulment, or divorce.
In addition, if you have a new dependent as a
Death of a dependent.
result of marriage, birth, adoption, or placement
A change in employment status that for adoption, you may be able to enroll yourself
affects eligibility under the Plan. and your dependents. However, you must
request enrollment within 30 days after you or
A change in election that is on
your dependents’ other coverage ends (or after
account of, and corresponds with, a
the employer stops contributing toward the other
change made under another
coverage), or after the marriage, birth, adoption,
employer Plan.
or placement for adoption.
A dependent ceasing to satisfy
eligibility requirements under the If you or your dependent's Medicaid or CHIP
Plan. (Children's Health Insurance Program) coverage
is terminated as a result of loss of eligibility, or
Electing coverage under your state’s become eligible for a premium assistance
Marketplace during an annual or subsidy under Medicaid or CHIP, you have 60
special enrollment. days to notify the benefits team.
5
Medical Coverage
Who administers our medical Who can I enroll for medical
plan options? coverage?
Blue Cross Blue Shield of North Carolina
(BCBS NC) will administer our medical and You may enroll your:
prescription drug plan options as of Legal spouse
January 1, 2019.
Children by birth, marriage,
adoption, or legal guardianship
until the end of the month they
What are my enrollment reach age 26.
options?
You are required to choose one of Disabled children may be covered past the
the following medical enrollment options: limiting age. Please contact the benefits
1. Enroll in PPO 2, team for more information.
2. Enroll in PPO A (formerly known
as PPO 3),
3. Enroll in the CDHP, or
How do I find a doctor, hospital,
pharmacy or other provider?
4. Waive coverage.
Call the number on the back of your ID
card
Will I receive a new ID card?
Yes. In December, you will receive a new ID Search online at
card from BCBS of NC. www.BlueConnectNC.com or through the
mobile app.
6
PPO (2 & A)
What is a PPO? What is a copay?
“PPO” stands for Preferred Provider A fixed dollar amount you pay for office visits,
Organization. Under a PPO, medical providers urgent care visits and emergency room visits, as
(doctors, hospitals, labs, etc.) join together to well as prescription drugs.
form a network that offers discounted services to
members. Copays do not count toward satisfying your
deductible. Copays do count toward the out-of-
pocket maximum.
What is coinsurance?
Once your deductible is satisfied, the plan will
pay a portion of the cost for most services (other
than those that require a copay) and so will you.
This is called coinsurance. Coinsurance is a pre-
set percentage that you are responsible for
paying, after the deductible has been satisfied.
What is a coinsurance maximum?
It is the total amount of
coinsurance that a plan
participant must pay before
the plan begins to pay 100%
for any services that are
covered at the coinsurance.
What is a deductible?
The PPO plan has an individual and family
deductible. The deductible is a specified dollar
amount a member must pay for covered services Is there a limit to my out-of-pocket
each benefit year before the plan begins to
provide payment for benefits.
costs?
Yes. You will continue to pay a portion of the
The individual deductible must be satisfied by costs until you meet the out-of-pocket maximum.
one person, while the family deductible can be The PPO plan has an individual and family out-of
satisfied by combining expenses for two or more -pocket maximum. If you are a single on a two-
covered family members. person or family contract, you are subject to the
individual out-of-pocket maximum, while the
Office visits, preventive care services and family out-of-pocket maximum can be satisfied by
prescription drugs are not subject to the combining expenses for two or more covered
deductible. family members. Your deductible, copays and
coinsurance all count toward the out-of-pocket
maximum. Once the maximum is met, most
services are covered by the plan at 100%.
7
CDHP
What is a CDHP?
CDHP stands for “Consumer Driven Health
Plan” (CDHP). It is sometimes referred to as a
High Deductible Health Plan (HDHP).
The CDHP option offers you the lowest payroll
contribution and the possibility of saving for
health care expenses in the future (with a Health
Savings Account). See the Health Savings
Account (HSA) pages for additional information.
The CDHP option provides greater control over
how your health care dollars are spent.
The CDHP also works on a PPO platform where
medical providers (doctors, hospitals, labs, etc.)
join together to form a network that offers
discounted services to members.
What is coinsurance?
Once your deductible is satisfied, the plan will
What is a deductible? pay a portion of the cost for most services (and
The CDHP option has a higher annual deductible so will you until you reach the out-of-pocket
than other traditional health plans and you must maximum).
first meet your annual deductible before the
plan will pay any portion of your claims,
including office visits and prescription drugs. What is a coinsurance maximum?
The exception to this is preventive care, which It is the total amount of
includes annual physicals for adults, well-child coinsurance that a plan
exams, well woman exams, etc. participant must pay before
the plan begins to pay 100%
The CDHP option has an individual and family for any services that are
deductible. The entire family deductible must be covered at the coinsurance.
met under a two-person or family contract before
benefits are paid for any person on the contract, Is there a limit to my out-of-pocket
unless that member has met the individual out-of costs?
-pocket maximum. This is true even if one family Yes. You will continue to pay a portion of the
member has satisfied the individual deductible costs until you meet the out-of-pocket maximum.
amount. The entire family out-of-pocket maximum must
be met under a two-person or family contract.
This is true even if one family member has met
Are there copays? the individual out-of-pocket maximum. The
No. All services, including office visits and deductible and coinsurance all count toward the
prescription drugs, are subject to the deductible out-of-pocket maximum. Once the maximum is
and coinsurance. met, most services are covered by the plan at
100%.
8
Prescription Drugs
To be eligible for prescription drug coverage, Are there restrictions on certain
you must elect to participate in one of the
medical plan options.
medications?
Yes. There are limits and restrictions on the
Medications are categorized in a formulary. A plan. Not all prescription drugs will be covered
formulary is a list of prescription medications under the plan. Some drugs are excluded from
selected for coverage under the plan. Drugs the drug benefit. Also, if there is a generic
may be included on the formulary based upon alternative available, you will be required to
their effectiveness, safety and cost. accept the generic. If you elect to receive the
brand when a generic alternative is available,
BCBS NC maintains their own you will be responsible for the difference in cost
formulary. You may notice between the generic and brand, in addition to
changes to the medications the brand copay.
that are covered and/or the
tier they are covered under. Quantity limits
Some medications are subject to quantity limits,
meaning there is a limit of how many pills you
Is there a network of can receive in a month.
pharmacies?
With BCBS NC, you have access to a wide Your doctor will need to tell BCBSNC in writing
network of pharmacies. Nearly every “chain” that you meet our medical necessity criteria to
pharmacy is in the network (CVS, Rite-Aid, receive more than the set amount.
Walgreens and Wal-Mart). Also, you can
search for pharmacies on BCBSN NC’s website
Prior Authorization / Step Therapy
at www.blueconnectNC.com.
Some drugs require that certain clinical criteria
must be met before coverage is provided.
Special Note about Specialty Medications These drugs are typically not covered unless
Specialty Drugs are medications used to treat your physician and BCBSNC agree that the
complex conditions such as multiple sclerosis or drug is medically necessary and that an
rheumatoid arthritis, generally in the form of an alternative medication would be harmful to your
injectable drug. These medications must be health or ineffective. Your doctor will have to
filled at the mail order specialty pharmacy submit a written confirmation BCBSNC that you
AllianceRx Walgreens Prime by calling 1-800- meet medical necessity criteria. Please locate
706-4365 or visiting www.alliancerxwp.com to your medication on the BCBSNC formulary. If
set up your account. You will need your the drug is flagged as needing Prior
Member ID card and information about your Authorization or Step Therapy, you will need to
prescription and the doctor who prescribed it. reach out to your provider to take the necessary
AllianceRx Walgreens Prime will help you steps to have your medication covered by the
schedule your first delivery and ship your Plan.
medication and covered supplies via next-day
delivery anywhere you choose in the United If you have a specific
States. If you are currently taking a specialty question about a
medication, you will be notified by BCBSNC by medication, an upcoming
mail with detailed instructions about how to set procedure or treatment you
up the delivery of your medication. are currently receiving,
please contact the benefits
team.
9
HSA
The HSA is only available to employees who enroll in the CDHP medical plan option.
If you enroll in the “Consumer Driven Health Things change, so your eligibility to contribute
Plan” (CDHP), you have two components to to an HSA is determined on a month-to-month
help pay for medical and prescription drug basis. If you are covered under the CDHP
expenses: option on the first of the month and are HSA-
1. A High Deductible Health Plan (HDHP) eligible, you may contribute 1/12 of the annual
administered by Blue Cross Blue Shield of contribution limit for that month. Essentially,
North Carolina, and you must be enrolled in the CDHP option for the
entire plan year to contribute the maximum
2. A Health Savings Account (HSA) annual limit.
administered by Health Equity.
Who administers the Health
What is a Health Savings Account Savings Accounts?
(HSA)? Health Equity will continue to administer the
An HSA is an investment account that can help Health Savings Accounts. If you have a current
you save money to pay for current or future account with Health Equity it will automatically
qualified medical expenses that are not transfer to our new arrangement with BCBSNC.
reimbursed through health insurance, including If you are already enrolled in the CDHP, your
a Flexible Spending Account. debit card will remain active, and your login and
password with Health Equity will remain the
An HSA allows tax-free contributions and same.
withdrawals, similar to 401(k) retirement
accounts, except it’s for health care expenses.
And, any remaining balance rolls over year-to-
year and is yours to keep, regardless of job
changes or retirement.
Who is eligible to open a Health
Savings Account?
You are eligible to establish an HSA if you are
enrolled in a HSA-compliant health plan, such
as our CDHP.
You are not eligible for an HSA if you:
Are covered by another health care plan
that is not HSA-compliant, including a
Flexible Spending Account, Medicare or Who can contribute to an HSA?
our PPO plan. Anyone (an eligible individual, a family member,
an employer or any other person) may make
Can be claimed as a dependent on
contributions to an HSA on behalf of an eligible
someone else’s tax return.
individual. The total contribution amount,
Are enrolled in a Health FSA with a regardless of source, cannot be greater than
balance greater than $0. the annual limit.
10HSA
How does the HSA work? What happens if I contribute more
You can withdraw money from your account or than the maximum allowed?
use the debit card provided when you have a If you contribute too much money to your HSA,
qualified medical expense. You are responsible a 6% penalty will apply to any amount in your
for deciding if the expense is qualified and, HSA that exceeds the annual contribution limit.
therefore, should understand what health The penalty can be avoided if the excess
expenses are permissible. A good source for contributions are withdrawn before you file your
qualified health expenses is IRS Publication income tax return (the following April 15th).
502. Remember to keep your receipts in case
you need to document your expenditures or It is your responsibility to ensure you do not
decisions during an IRS audit. contribute more than the maximum allowed
amount.
Funds you withdraw from your HSA to pay for
qualified health expenses are tax-free. If you
use your HSA funds to pay for non-qualified
health expenses, the amount will be taxable Can I change my HSA contribution
and you will pay an additional 20% tax penalty. amount during the year?
You may change (or even stop) your HSA
Will the company contribute to my contribution amount by contacting the benefits
HSA? team. The change will be made as soon as
Yes! The company will match your HSA administratively feasible. This is typically by the
contribution dollar for dollar, up to $500 for next pay date.
single coverage or $1,000 for two party or
family coverage. AKBA, APNA, CIS and Sun
Plastech employees who met the prior year’s Do I have to keep any records
wellness requirements will receive an additional regarding my HSA?
$1,000 HSA deposit in January 2019. It is your responsibility to keep track of your
deposits and expenditures and keep all of your
How much can I contribute to my receipts (necessary if you are audited by the
HSA? IRS). It is your responsibility to follow the
For 2019 the IRS will allow contributions of up regulations governing HSAs. The
to $3,500 for an individual or $7,000 for a consequences for not doing so will come from
family. If you and your spouse each have CDHP the IRS.
coverage, the $7,000 annual maximum is a joint
limit between the two of you. Employees age
55 or older can contribute an additional $1,000. What happens to my HSA if I
terminate employment?
You can make contributions to an HSA anytime You own the HSA. You may continue to pay for
during the plan year and up until April 15 of the qualified medical expenses after your employment
following year. The company will allow you to terminates.
contribute to your HSA via payroll deduction.
You will be asked to choose an amount during
annual enrollment. You can also contribute by
personal check.
11Medical Benefits Summary
PPO 2 PPO A (formerly PPO 3) CDHP
Out-of-
In-Network In-Network Out-of-Network In-Network Out-of-Network
Network
Deductibles, Copays & Dollar Maximums
Deductibles $100 for one member, $250 for one mem- $750 for one member, $1,600 for one $1,400 for one $2,800 for one
$200 for family (when ber, $500 for family $2,250 for family member, person contract, person contract,
two or more members (when two or more (when two or more $3,200 for family $2,800 for family (2 $5,600 for family (2
are covered under your members are cov- members are covered (when two or more or more members) or more members)
contract) each calendar ered under your under your contract) members are cov- each calendar year each calendar year
year contract) each cal- each calendar year ered under your
endar year contract) each cal- The full family deductible must be
endar year met under a two-person or family
contract before benefits are paid.
Fixed Dollar $20 copay: office visits After your deducti- $25 copay: office visit After your deducti-
Copays ble is met, the Plan ble is met, the Plan
$20 copay: specialist pays 70% of the $50 copay: specialist pays 70% of the N/A N/A
office visit, urgent care approved amount office visit, urgent care approved amount
for most covered for most covered
$50 copay for emergen- services, you pay services, you pay
cy room visits 30% until the out-of- $150 copay: emergen- 30% until the out-of-
pocket maximum is cy room visits ($300 pocket maximum is
met. per visit after) met.
Coinsurance After your deductible is After your deducti- After your deductible After your deducti- After your deducti- After your deducti-
met, the Plan pays 90% ble is met, the Plan is met, the Plan pays ble is met, the Plan ble is met, the Plan ble is met, the Plan
of the approved amount pays 70% of the 85% of the approved pays 70% of the pays 80% of the pays 60% of the
for most covered ser- approved amount amount for most cov- approved amount approved amount approved amount
vices, you pay 10% until for most covered ered services, you pay for most covered for most covered for most covered
the out-of-pocket maxi- services, you pay 15% until the out-of- services, you pay services, you pay services, you pay
mum is met. 30% until the out-of- pocket maximum is 30% until the out-of- 20% until the out-of 40% until the out-of-
pocket maximum is met. pocket maximum is -pocket maximum pocket maximum is
met. met. is met. met.
Coinsurance N/A N/A $2,250 for one mem- $4,400 for one $1,250 for one $2,500 for one
Maximum ber, $3,750 for family member, $8,800 for member, $2,500 for member, $5,000 for
(when two or more family (when two or family (when two or family (when two or
(total amount members are covered more members are more members are more members are
of coinsurance under your contract) covered under your covered under your covered under your
that a partici- each calendar year contract) each cal- contract) each contract) each cal-
pant could pay) endar year calendar year endar year
Out-of-Pocket $500 for one member, $1,500 for one $3,000 for one mem- $6,000 for one $2,650 for one $5,300 for one
Maximums $1,000 for two or more member, $3,000 for ber, $6,000 for two or member, $12,000 member, $5,300 for member, $10,600
members each two or more mem- more members each for two or more two or more mem- for two or more
calendar year bers each calendar calendar year members each bers each members each
year calendar year calendar year calendar year
Includes de-
ductible, co- Does not include Does not include
pays and coin- copays. copays.
surance.
*Preventive
Covered at 100% Not covered Covered at 100% Not covered Covered at 100% Not covered
Care Services
*See flyer included in this Highlights Book for additional details
12Medical Benefits Summary
PPO 2 PPO A (formerly PPO 3) CDHP
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Diagnostic Services
Laboratory and Pathology 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
Services network network deductible network network deductible deductible network deductible
deductible deductible
Diagnostic Tests and X- 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
rays network network deductible network network deductible deductible network deductible
deductible deductible
Maternity Services Provided by a Physician
Prenatal and Postnatal Covered at 100% 70% after out-of- $25 copay 70% after out-of- 80% after in-network 60% after out-of-
Care network deductible network deductible deductible network deductible
Delivery and Nursery 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
Care network network deductible network network deductible deductible network deductible
deductible deductible
Hospital Care
90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
network network deductible network network deductible deductible network deductible¹
deductible deductible
Inpatient Care*
Note: Non-emergency services must be rendered in a participating hospital
Outpatient Surgery 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
network network deductible network network deductible deductible network deductible
deductible deductible
Mental Health Care and Substance Abuse Treatment
Inpatient Mental Health 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
Care network network deductible network network deductible deductible network deductible
deductible deductible
Inpatient Substance 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
Abuse network network deductible network network deductible deductible network deductible
Treatment deductible deductible
Outpatient Mental Health
Care
90% after in- 70% after in- 85% after in- 70% after out-of- 80% after in-network 80% after in-network
- Facility and clinic (in network network network network deductible deductible deductible, in partici-
participating facilities deductible deductible, in partic- deductible pating facilities only
only) ipating facilities only
$20 copay for $50 copay for
- Physician’s office office visits office visits
Outpatient Substance 90% after in- 70% after in- 85% after in- 70% after out-of- 80% after in-network 60% after out-of-
Abuse Treatment—in network network network network deductible deductible network deductible
approved facilities only deductible deductible deductible
*Some procedures such as certain inpatient surgeries will require precertification when you utilize an out-of-network provider; if you do not obtain precertification (your
doctor should be familiar with this process) your claim will be denied and you will be responsible for 100% of the cost for care. ¹The CDHP has a $250 penalty when a
procedure requires precertification, then services subject to out-of-network deductible and coinsurance.
13Medical Benefits Summary
PPO 2 PPO A (formerly PPO 3) CDHP
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Other Covered Services
Chiropractic Spi- $20 copay per 70% after out-of- 80% after in- 80% after out-of- 80% after in- 60% after out-of-
nal office visit network deductible network network deductible network network deductible
Manipulation and deductible deductible
Osteopathic Ma-
nipulative Therapy
Limited to a combined maximum of 25 visits per member per calendar year.
Outpatient Physi- 90% after in- 70% after out-of- 85% after in- 70% after out-of- 80% after in- 60% after out-of-
cal, Speech and network network deductible network network deductible network network deductible
Occupational deductible deductible deductible
Therapy—
provided for reha-
bilitation Physical and occupational therapy have unlimited visits; Speech therapy is limited to a maximum of 30 visits per
member per calendar year
Durable Medical 90% after in- 90% after in- 85% after in- 80% after in- 80% after in- 60% after in-network
Equipment* network network network network network deductible
deductible deductible deductible deductible deductible
Allergy Testing Testing—Subject 70% after out-of- Testing—Subject 60% after out-of- 80% after in- 60% after out-of-
and Injections to $20 copay network deductible to $25 or $50 network deductible network network deductible
copay deductible
Injections—
covered at $20 Injections—
copay or 100% if covered at $25 or
no office visit $50 copay or
100% if no office
visit
Prescription Drugs
Tier 1 (Usually $10 copay $10 copay plus an $10 copay $10 copay 80% after in- 80% after out-of-
generic) additional 25% of network network
the approved deductible deductible
amount
Tier 2 (Usually $20 copay $20 copay plus an $35 copay $35 copay 80% after in- 80% after out-of-
Preferred Brand) additional 25% of network network
the approved deductible deductible
amount
Tier 3 (Usually $40 copay $40 copay plus an $45 copay $45 copay 80% after in- 80% after out-of-
Non Preferred additional 25% of network network
Brand) the approved deductible deductible
amount
A non-preferred brand medication is one for which there is either a generic alternative or a more cost effective preferred brand
Specialty Medica- $40 Not covered $50 Not covered 80% after in- Not covered
tions¹ network
deductible
90 day supply at Same as retail Not covered 2.5x retail copay Not covered 80% after in- Not covered
retail or mail order above network
deductible
The benefit enrollment communications contain only a brief summary of your benefits. We have tried to ensure the accuracy of these materials, but if there is
any discrepancy between the benefits discussed in these materials and the official plan documents, the official plan documents will rule. Actual benefits will be
paid in accordance with the carrier contracts and any amendments to those contracts in place at the time of the claim. Please refer to the carrier booklets for
details regarding your coverage, including benefit limitations and exclusions. Benefits are provided at the company’s discretion and do not create a contract of
employment. The company reserves the right to amend, modify or terminate any plan at any time and in any manner.
* Durable medical equipment provided as part of an office visit is covered at 100%. ¹Specialty Medications require use of the mail order pharmacy. See page
9 for details.
1415
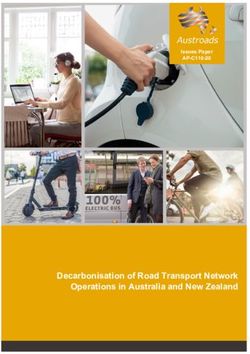
TELEHEALTH
See a doctor from home, at work or on the go 3 ways to activate today
So it’s ready when you need it!
Sunburn at the beach? Stomach bug on Thanksgiving? In a rural area with no
doctors nearby? Think you’ve got the flu but don’t feel up to driving to your doctor’s Download the
office? These are just a few of the reasons people use telehealth. And you can too! Teladoc app on your
Your Blue Cross and Blue Shield of North Carolina (Blue Cross NC) health plan
smartphone or tablet.
includes telehealth services from Teladoc.* It’s a good option for minor health
problems when you can’t see your regular doctor. Plus, it’s often more convenient
and cost effective than urgent care. Go to
www.teladoc.com and
Get started. click “Set Up Account.”
Don’t wait until you’re sick – activate your Teladoc account now so you’re prepared.
There are three ways to activate: mobile app, online or by phone (see graphic).
Once your account is set up, you can see a board-certified doctor via secure online
Call 1-800-835-2362
video from the Teladoc app or your computer. Teladoc’s doctors can diagnose
symptoms, prescribe non-narcotic medication1 and send prescriptions to your
pharmacy.
Skip the waiting room.
Seventy percent of consumers say they’re interested in telehealth – and Why wait?
convenience is the top reason.2 Teladoc offers these time-saving benefits: Average time it takes to see a doctor:
+ Video consults available 24/7 (even on holidays) + Median wait time is just 10
+ Takes just minutes to connect with a Teladoc doctor minutes4
+ No appointment needed (though you can schedule one)
+ 19 minutes at a doctor’s office5
+ Pediatricians available if your child gets sick
(40 minutes for total visit)6
+ If you need a prescription, your Teladoc doctor can electronically send it to the
pharmacy that’s close to you + 30 minutes at an urgent care
+ On the couch, at work, travelling – you can use Teladoc just about anywhere3 (60 minutes for total visit)7
+ 28 minutes at the ER
*Teladoc is an independent company that is solely responsible for the telehealth services it is providing. (153 minutes for total visit)8
1
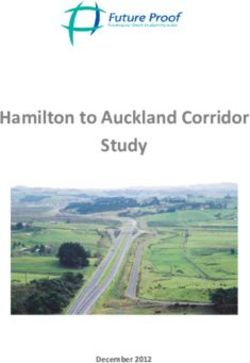
16Save money.
Extra convenience doesn’t mean extra cost. In fact, telehealth runs less than the
typical urgent care visit. And if you go to the ER for a non-emergency? Your cost
can skyrocket more than 1,300%!9 Dollars to dollars
With Teladoc, you’ll pay for a video consult the same as an office visit with your Compare the average member cost for:9
primary care doctor. That means:
$
+ If your health plan has a co-pay: You’ll pay the usual co-pay for a doctor’s visit 667
+ If your health plan has a deductible and co-insurance: You’ll pay no more than $4510 ER
$
Teladoc accepts most major credit and debit cards. It’s also a qualified expense $
45 orless 59
for HSA, HRA and FSA accounts. Urgent Care
Teladoc
Get quality care.
Teladoc doctors are board certified with an average of
20 years’ experience. Specialties range from primary
1 In some states, laws require that a doctor only prescribe medication in
care and internal medicine, to pediatrics and family certain situations and subject to certain limitations.
medicine. So, they can treat a wide range of conditions. 2 “2017 Consumer Survey on Virtual Health.” Accenture. Online: www.
accenture.com/us-en/insight-voting-virtual-health-survey (accessed May
2017).
Trust is also important. Teladoc has a 95% satisfaction 3 Consults not available outside the United States.
4 Source: www.teladoc.com/start (accessed June 2017).
rating – and 92% of issues are resolved after the first 5 Based on national average wait time of 18 minutes and 35 seconds.
visit.4 You’ll see a doctor who is licensed to practice Source: 8th Annual Vitals Index. Online: www.vitals.com/about/posts/
press-center/press-releases/vitals-index-reveals-wait-times-decreasing
in your state. It’s HIPAA-compliant and your personal (accessed May 2017).
6 Shaw, Meredith K., et al. “The duration of office visits in the United
health information is never shared with your employer. States, 1993 to 2010.” The American Journal of Managed Care 20.10
(2014): 820-826.
7 “2016 Benchmarking Report Summary.” Urgent Care
Keep in mind that telehealth isn’t meant to replace your primary care doctor. Association of America. Online: www.ucaoa.org/resource/resmgr/
benchmarking/2016BenchmarkReport.pdf (accessed May 2017).
Instead, think of it as an easy way to get care when common health problems hit. 8 Average times shown are for emergency departments in North Carolina.
Source: https://projects.propublica.org/emergency/ (accessed May 2017).
And of course, you should always call 911 for any life-threatening emergencies. 9 Urgent care and ER figures are the average cost to Blue Cross NC
members across commercial group plans. Based on Blue Cross NC internal
data for 12 months ending December 2016. ER costs include both facility
and professional charges—and combine copayment, deductible and
Teladoc can handle many non-emergency health problems: coinsurance.
10 Until December 31, 2017, the price of a Teladoc visit will be $42. On
+ Acne + Allergies + Constipation January 1, 2018, the cost will be $45. Your health plan may cover these
visits for less.
+ Cough, cold and flu + Diarrhea + Ear problems Teladoc is an independent company that is solely responsible for the
telehealth services it is providing. Teladoc does not offer Blue Cross or Blue
+ Fever + Headache + Insect bites Shield products or services. Availability depends on location at the time of
consultation. Telehealth services are subject to the terms and conditions
+ Joint aches and pains + Nausea and vomiting + Pink eye of the member’s health plan, including benefits, limitations and exclusions.
Telehealth services are not a substitute for emergency care.
+ Rash + Sinus problems + Sore throat Teladoc and the Teladoc logo are registered trademarks of Teladoc, Inc.
and may not be used without written permission. Teladoc does not replace
+ Sunburn + And more the primary care physician. Teladoc does not guarantee that a prescription
will be written. Teladoc operates subject to state regulation and may not
be available in certain states. Teladoc does not prescribe DEA-controlled
substances, non-therapeutic drugs and certain other drugs which may be
harmful because of their potential for abuse. Teladoc physicians reserve the
right to deny care for potential misuse of services. For complete terms of
use, visit https://member.teladoc.com/terms/terms_of_use.
Learn more at www.teladoc.com or by calling 1-800-835-2362. BLUE CROSS®, BLUE SHIELD®, and the Cross and Shield symbols are
marks of the Blue Cross and Blue Shield Association, an association of
independent Blue Cross and Blue Shield Plans. All other marks are the
property of their respective owners. Blue Cross NC is an independent
licensee of the Blue Cross and Blue Shield Association. U13291a, 9/17
2
bcbsnc.com
17Health Advocate
What is Health Advocate? What issues can Health Advocate
Health Advocate offers you access to health assist with?
care experts who provide personalized support
Find the right medical provider
to help you navigate the health care system and
insurance-related issues. Expedite appointments
Research complex medical
conditions, and locate latest
treatment options
Coordinate care and schedule follow
-up visits
Who can contact Health Advocate? Arrange specialized treatments and
You tests
Your spouse / domestic partner Answer questions about results,
Your child(ren) treatments and prescribed
medication
Your parents
Provide procedure cost estimates
Your parents in-law
Identify Gaps In Care
Personal nurse contact
How do I contact Health Advocate? Web-based health information and
Call 1-866-695-8622 decision support
Visit www.healthadvocate.com/ Insurance claims resolution service
members
Locate eldercare
Email answers
@healthadvocate.com
Is there a cost for using Health
Advocate?
No. There is no charge to you or your family
for using this program.
18Dental Coverage
Who administers our Will I receive an ID card?
dental plan? Yes! An ID card will be mailed to your home
Delta Dental of North Carolina will address in December 2018.
administer our dental plan as of
January 1, 2019.
How do I find a dentist?
What are my enrollment Call Delta Dental at 1-800-662-8856, or
options? Search the PPO or Premier networks
There is only one plan option for dental
online at www.deltadentalnc.com/
coverage. If you do not want dental
coverage, simply skip to the next benefit findadentist
selection in ADP.
Who can I enroll for dental Is there a network of dentists?
You can receive services from any dentist you
coverage? choose. However, when you select a dentist
You may enroll your: that participates in one of the Delta Dental
Legal spouse networks, that dentist has agreed to accept
Children by birth, marriage, Delta Dental’s approved amount for services.
adoption, or legal guardianship
until the end of the month they If you visit a dentist that does not participate
reach age 26. in the network, you may be balance billed for
amounts exceeding the approved payment
amount. This can result in significant out-of-
Disabled children may be covered past the pocket costs!
limiting age. Please contact the benefits team
for more information.
19Delta Dental PPO plus Premier
Summary of Dental Plan Benefits
For Group# 0518
This Summary of Dental Plan Benefits should be read along with your Certificate. Your Certificate provides
additional information about your Delta Dental plan, including information about plan exclusions and limitations.
If a statement in this Summary conflicts with a statement in the Certificate, the statement in this Summary applies
to you and you should ignore the conflicting statement in the Certificate. The percentages below are applied to
Delta Dental's allowance for each service and it may vary due to the dentist's network participation.*
Control Plan – Delta Dental of North Carolina
Benefit Year – January 1 through December 31
Covered Services –
Delta Dental Delta Dental Nonparticipatin
PPO Dentist Premier Dentist g Dentist
Plan Pays Plan Pays Plan Pays*
Diagnostic & Preventive
Diagnostic and Preventive Services – exams,
100% 100% 100%
cleanings, fluoride, and space maintainers
Emergency Palliative Treatment – to temporarily
100% 100% 100%
relieve pain
Sealants – to prevent decay of permanent teeth 100% 100% 100%
Radiographs – X-rays 100% 100% 100%
Periodontal Maintenance – cleanings following
100% 100% 100%
periodontal therapy
Basic Services
Minor Restorative Services – fillings and crown repair 80% 80% 80%
Endodontic Services – root canals 80% 80% 80%
Periodontic Services – to treat gum disease 80% 80% 80%
Oral Surgery Services – extractions and dental surgery 80% 80% 80%
Major Restorative Services – crowns 80% 80% 80%
Other Basic Services – misc. services 80% 80% 80%
Relines and Repairs – to bridges and dentures 80% 80% 80%
Occlusal Guards/Adjustments – bite guards and
50% 50% 50%
occlusal adjustments
Major Services
Prosthodontic Services – bridges and dentures 80% 80% 80%
Orthodontic Services
Orthodontic Services – braces 50% 50% 50%
Orthodontic Age Limit – to the end of the to the end of the to the end of the
month of age 19 month of age 19 month of age 19
* When you receive services from a Nonparticipating Dentist, the percentages in this column indicate the portion
of Delta Dental's Nonparticipating Dentist Fee that will be paid for those services. The Nonparticipating Dentist
Fee may be less than what your dentist charges and you are responsible for that difference.
20 Oral exams (including evaluations by a specialist) are payable twice per calendar year.
Prophylaxes (cleanings) are payable twice per calendar year. Full mouth debridement is payable once per
lifetime.
Fluoride treatments are payable twice per calendar year for people up to age 19.
Space maintainers are payable once per area per lifetime for people up to age 19.
Bitewing X-rays are payable twice per calendar year. Full mouth X-rays (which include bitewing X-rays) are
payable once in any three-year period.
Sealants are payable once per tooth per lifetime for the occlusal surface of first and second permanent molars
up to age 16. The surface must be free from decay and restorations.
Composite resin (white) restorations are optional treatment on posterior teeth.
Porcelain and resin facings on crowns are Covered Services on posterior teeth. Veneers and porcelain or resin
facings on onlays are optional treatment.
Vestibuloplasty is a Covered Service.
Full and partial dentures are payable once in any five-year period. Reline and rebase of dentures are payable
once in any two-year period.
Implants and related services are not Covered Services.
Having Delta Dental coverage makes it easy for you to get dental care almost everywhere in the world! You can
now receive expert dental care when you are outside of the United States through our Passport Dental program.
This program gives you access to a worldwide network of dentists and dental clinics. English-speaking operators are
available around the clock to answer questions and help you schedule care. For more information, check our Web
site or contact your benefits representative to get a copy of our Passport Dental information sheet.
Maximum Payment – $1,500 per person total per Benefit Year on all services except orthodontic services. $1,500
per person total per lifetime on orthodontic services.
Deductible – $50 Deductible per person total per Benefit Year limited to a maximum Deductible of $150 per family
per Benefit Year. The Deductible does not apply to diagnostic and preventive services, emergency palliative
treatment, X-rays, sealants, periodontal maintenance and orthodontic services.
If you and your spouse are both eligible for coverage under this Contract, you may be enrolled together on one
application or separately on individual applications, but not both. Your dependent children may only be enrolled
on one application. Delta Dental will not coordinate benefits if you and your spouse are both covered under this
Contract.
21EAP
What is the EAP? contact the EAP for help?
The Employee Assistance Program (EAP) You
provided by HelpNet is a program designed to
assist you and your immediate family members. Your spouse / domestic partner
HelpNet can help you resolve any concerns that Your child(ren)
are affecting your personal or work lives…no
matter what the issue!
Will anyone know I contacted the
What issues can the EAP help EAP?
with? No. The EAP is a confidential benefit. This
means that HelpNet must keep your records,
Mental Health and even the fact that you called them,
Finances confidential from any other party. No one—not
Parenting even your employer—will ever know you used
HelpNet’s services.
Work-Life Balance
Stress Is there a cost for using the EAP?
Aging Parents No. There is no charge to you or your family
for using this confidential program. If you
choose to use any referrals to additional
How does the EAP work? resources, their charges (if any) would be your
Under the program, you can receive: responsibility and may be covered under your
Telephone access to licensed medical plan.
clinicians 24 hours a day, seven
days a week. How do I contact the EAP?
To access this benefit, you can contact HelpNet
Up to 5 face-to-face counseling at 1-800-969-6162 24 hours a day / 365 days a
sessions with EAP network year. You can also log on to their website at
providers. www.helpneteap.com. Click on “Work Life
Referrals to community services. Web”, found at the top of the page.
Online access to an extensive library
of articles and tip sheets on various Username: AKPNA
topics, as well as audio and video
clips. Password: EMPLOYEE
Who can
22Vision Coverage
Who administers our vision Is there a network of vision
plan? providers?
United Healthcare (UHC) will be our Yes. You will receive the highest level of
new vision carrier as of January 1, benefits and lowest out-of-pocket costs when
2019. you seek services from a provider in the
UHC network (sometimes referred to as
What are my enrollment Specter Eyecare Network). The network
includes many well-known chain providers,
options? such as America’s Best, Costco, Eyeglass
Vision will no longer be a “bundled” election World, Visionworks and Warby Parker.
with medical coverage. For 2019, it will be
offered as a stand-alone option for you to If your provider is not in the network and you
elect or waive. You may elect employee only wish to nominate them to join, please contact
or family coverage. If you do not want vision the benefits team for a form.
coverage, simply skip to the next benefit
selection in ADP.
How do I get reimbursed if I visit
a non-network eye care
Who can I enroll for vision provider?
coverage? If you have services performed by a non-
You may enroll your: network provider, you will need to pay out-of-
Legal spouse pocket for those services and file a claim
form for reimbursement, along with providing
Children by birth, marriage, an itemized receipt. You can request a
adoption, or legal guardianship reimbursement form from the benefits team.
until the end of the month they
reach age 26.
How do I find an eye care
Disabled children may be covered past the
limiting age. Please contact the benefits
provider?
Call UHC at or 1-800-638-3120, or
team for more information.
Search online at www.myuhcvision.com
Will I receive an ID card?
Yes! An ID card will be mailed to your home
address in December 2018.
23Asahi KASEI Employees Benefit Plan
Year 1/1/2019 - 12/31/2021 Vision Benefit Summary
Customer Service and Provider Locator: (800) 638-3120
myuhcvision.com
UnitedHealthcare vision has been trusted for more than 50 years to deliver affordable, innovative vision care solutions to the nation’s leading
employers through experienced, customer-focused people and the nation’s most accessible, diversified vision care network.
In-network, covered-in-full benefits (up to the plan allowance and after applicable copay) include a comprehensive exam, eyeglasses with
standard single vision, lined bifocal, lined trifocal, or lenticular lenses, standard scratch-resistant coating and the frame, or contact lenses in lieu
of eyeglasses.
Exam with Materials
Benefit Frequency
Comprehensive Exam(s) Once every Calendar Year(s)
Spectacle Lenses Once every Calendar Year(s)
Frames Once every Calendar Year(s)
Contact Lenses in Lieu of Eyeglasses Once every Calendar Year(s)
In-Network Services
Copays
Exam(s) $ 10.00
Materials $ 30.00
Frame Benefit (for frames that exceed the allowance, an additional 30% discount may be applied to the overage)¹
Private Practice Provider $130.00 retail frame allowance
Retail Chain Provider $130.00 retail frame allowance
Lens Options
Standard Scratch-resistant Coating,Polycarbonate Lenses for Dependent Children (up to age 19) - covered in full.
Other optional lens upgrades may be offered at a discount (discount varies by provider). The Lens Options list can be found at
myuhcvision.com.
Contact Lens Benefit² (Selection contact lenses refers to our formulary contact list. Contact lenses not listed on the formulary are referred to as
non-selection. A copy of the list can be found at myuhcvision.com).
Selection contact lenses If you choose disposable contacts, up to 4
The fitting/evaluation fees, contact lenses, and up to two boxes are included when obtained from
follow-up visits are covered in full after copay (if applicable). an in-network provider.
Non-selection contact lenses
An allowance is applied toward the purchase of contact $105.00
lenses outside the selection. Materials copay (if applicable)
is waived.
{@Bullet} Necessary contact lens 3
Necessary contact lenses Covered in full after copay (if applicable).
Out-of-Network Reimbursements (Copays do not apply)
Exam(s) Up to $42.00
Frames Up to $37.00
Single Vision Lenses Up to $29.00
Lined Bifocal Lenses Up to $39.00
Lined Trifocal Lenses Up to $48.00
Lenticular Lenses Up to $48.00
Elective Contacts in Lieu of Eyeglasses² Up to $73.00
{@Bullet} Necessary conta 3
Necessary Contacts in Lieu of Eyeglasses Up to $73.00
24Discounts
Laser vision
UnitedHealthcare has partnered with the Laser Vision Network of America (LVNA) to provide our members with access to discounted
laser vision correction providers. Members receive 15% off standard or 5% off promotional pricing at more than 550 network provider
locations and even greater discounts through set pricing at LasikPlus® locations. For more information, call 1-888-563-4497 or visit us
at www.uhclasik.com.
Additional Material
At a participating in-network provider you will receive up to a 20% discount on an additional pair of eyeglasses or contact lenses. This
program is available after your vision benefits have been exhausted. Please note that this discount shall not be considered insurance,
and that UnitedHealthcare shall neither pay nor reimburse the provider or member for any funds owed or spent. Additional materials do
not have to be purchased at the time of initial material purchase.
Hearing Aids
As a UnitedHealthcare vision plan member, you can save on high-quality hearing aids when you buy them from hi HealthInnovations™.
To find out more go to hiHealthInnovations.com. When placing your order use promo code myVision to get the special price discount.
¹30% discount available at most participating in-network provider locations. May exclude certain frame manufacturers. Please verify all discounts with your provider.
²Contact lenses are in lieu of eyeglass lenses and/or eyeglass frames. Coverage for Selection contact lenses does not apply at Costco, Walmart or Sam's Club
locations. The allowance for Non-selection contact lenses applies to materials. No portion will be exclusively applied to the fitting and evaluation.
³Necessary contact lenses are determined at the provider's discretion for one or more of the following conditions: Following cataract surgery without intraocular lens
implant; to correct extreme vision problems that cannot be corrected with eyeglass lenses and/or frames; with certain conditions such as anisometropia,
keratoconus, irregular corneal/astigmatism, aphakia, facial deformity; or corneal deformity. If your provider considers your contacts necessary, you should ask your
provider to contact UnitedHealthcare vision confirming the reimbursement that UnitedHealthcare will make before you purchase such contacts.
Important to Remember:
In-Network
• Always identify yourself as a UnitedHealthcare vision member when making your appointment. This will assist the provider in obtaining
your benefit information.
• Your participating provider will help you determine which contact lenses are available in the UnitedHealthcare selection.
• Your $105.00 contact lens allowance applies to materials. No portion will be exclusively applied to the fitting and evaluation. Your material
copay is waived when purchasing non-selection contacts.
• Patient options such as UV coating, progressive lenses, etc., which are not covered-in-full, may be available at a discount at participating
providers. The Lens Options list can be found at myuhcvision.com.
Choice and Access of Vision Care Providers
UnitedHealthcare offers its vision program through a national network including both private practice and retail chain providers. To access the
Provider Locator service or for a printed directory, visit our website myuhcvision.com or call (800) 638-3120, 24 hours a day, seven days a
week. You may also view your benefits, search for a provider or print an ID card online at myuhcvision.com.
Retain this UnitedHealthcare vision benefit summary which includes detailed benefit information and instructions on how to use the program.
Please refer to your Certificate of Coverage for a full explanation of benefits.
In-Network Provider - Copays and non-covered patient options are paid to provider by program participant at the time of service.
Out-of-Network Provider - Participant pays full fee to the provider, and UnitedHealthcare reimburses the participant for services rendered
up to the maximum allowance. Copays do not apply to out-of-network benefits. All receipts must be submitted at the same time to the following
address: UnitedHealthcare Vision, Attn. Claims Department, P.O. Box 30978, Salt Lake City, UT 84130. Written proof of loss should be given
to the Company within 90 days after the date of loss. If it was not reasonably possible to give written proof in the time required, the Company will
not reduce or deny the claim for this reason. However, proof must be filed as soon as reasonably possible, but no later than 1 year after the
date of service unless the Covered Person was legally incapacitated.
Customer Service is available toll-free at (800) 638-3120 from 8:00 a.m. to 11:00 p.m. Eastern Time Monday through Friday,
and 9:00 a.m. to 6:30 p.m. Eastern Time on Saturday.
This Benefit Summary is intended only to highlight your benefits and should not be relied upon to fully determine coverage. This benefit plan
may not cover all of your healthcare expenses. More complete descriptions of benefits and the terms under which they are provided are
contained in the certificate of coverage that you will receive upon enrolling in the plan. If this Benefit Summary conflicts in any way with the
Policy issued to your employer, the Policy shall prevail.
UnitedHealthcare vision coverage provided by or through UnitedHealthcare Insurance Company, located in Hartford, Connecticut, UnitedHealthcare Insurance
Company of New York, located in Islandia, New York, or its affiliates. Administrative services provided by Spectera, Inc., United HealthCare Services, Inc. or their affiliates.
Plans sold in Texas use policy form number VPOL.06.TX or VPOL.13TX and associated COC form number VCOC.INT.06.TX or VCOC.CER.13.TX. Plans sold in
Virginia use policy form number VPOL.06.VA or VPOL.13.VA and associated COC form number VCOC.INT.06.VA or VCOC.CER.13.VA.
25 08/18 © 2018 United HealthCare Services, Inc.
0011400001wWTebAAG
F2790 15329830-7-1-1-R-S 01/01/2019 01/01/2019 - 12/31/2021 NCA-03C (v3.1)Life / AD&D
Who insures our life and Evidence of Insurability (EOI) is required if
you are electing coverage for the first time
accidental death & during annual enrollment or increasing your
dismemberment (AD&D) plans? coverage level. You must complete the EOI
Voya will continue to insure our life and AD&D form and submit it to Voya for their review.
plans. Coverage will not go into effect until approved
by Voya. You can request a form from the
benefits team.
What coverage is provided?
Basic life insurance provides a benefit to your
beneficiary if you die while covered under the
plan. Basic AD&D insurance provides a benefit
in the event of your accidental death or a
percentage of the benefit if you suffer
dismemberment as described by the plan. The
benefit for each is 2.25 times your annual
earnings. There is a maximum benefit of
$750,000.
Who pays for the basic life and Who can I cover under the life
AD&D coverage? and AD&D plans?
The company pays for the basic life and AD&D
coverage. Life insurance in excess of $50,000
will result in non-wage compensation being
added to your W-2, on which you will pay taxes. Your Legal spouse,
This is referred to as imputed income.
Children by
Birth,
Can I purchase additional Marriage,
coverage?
Yes. If you feel that the company-provided Adoption, or
coverage is not enough to protect your family in Legal guardianship
the event of your death, you may choose to
purchase additional coverage for yourself, your until they reach age 26.
spouse or your child(ren). You must elect
coverage for yourself in order to elect Special note: Coverage effective dates and
coverage for your spouse and/or child(ren). increases in coverage may be delayed if you and/
This applies to both the voluntary life and or your dependents are disabled on the date
voluntary AD&D plan. coverage is scheduled to take effect. Life and
AD&D benefits may reduce at specific ages.
Voluntary life and/or AD&D coverage is an after Please review the Voya booklet for specific
-tax deduction. details.
26You can also read