Analgesia & WHO Pain Ladder - DR PRIYA ABRAHAM - Study Hub
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Analgesia & WHO Pain Ladder. DR PRIYA ABRAHAM
OUTLINE
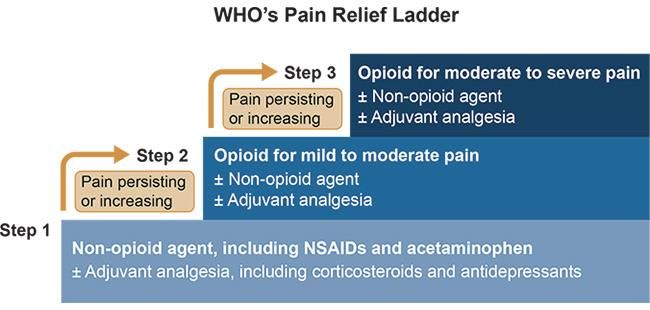
Pain Ladder
Different Analgesia
CasesPain Ladder
▪ Strong from weak to strong
▪ At each step reassess:
▪ Where
▪ Which
▪ How
▪ When
▪ Oral when possible
▪ Fixed interval to give continuous
relief
▪ Stepwise approachParacetamol ▪MOA: Weak inhibiter of cyclooxygenase (COX). Antipyretic and Analgesic ▪Side Effects: well tolerated not very many SE. In OVERDOSE → NAPQI → Hepatocellular necrosis ▪N-acetylecysteine and Treatment Curve: ▪ Most effective within 8hrs, can be given up to 24hrs post digestion ▪ Give Treatment if: ▪ Staggered OD ▪ Doubt over the time of paracetamol ingestion ▪ Plasma paracetamol concentration on or above treatment line at joining points ▪ When prescribing always consider ▪ Weight
NSAIDs ▪ MOA: inhibits cyclooxygenase and prevents the production of prostaglandins ▪ Side Effects: GI toxicity, renal impairment and increased risk of cardiovascular events (e.g. myocardial infarction and stroke). ▪ When prescribing always consider: ▪ AKI ▪ PPI especially for MSK problems ▪ Duration of analgesia ▪ Important interactions: ▪ ⬆️ Peptic Ulcer when prescribed along side Aspirin + Corticosteriods ▪ ⬆️ GI bleeding when prescribed along side anticoagulant, SSRIs, Venlafaxine ▪ ⬆️ Bleeding with warfarin
Opioids
▪ MOA: Activation of opioid μ (mu) receptors in the central nervous system. It reduces neuronal
excitability and pain transmission.
▪ Side effects: Respiratory depression, neurological depression (euphoria and detachment),
nausea and vomiting, pupillary constriction, constipation, itching, urticaria, vasodilatation and
sweating. Continued use can lead to tolerance and dependence.
▪ Opioids are split into weak (2nd rung) and strong (3rd rung).
Weak Strong
Codeine Morphine
Dihydrocodeine Oxycodone
Tramadol
▪ You start with a short acting opioid, assess the patient’s response before considering to a
switch to modified twice daily preparation + PRN for break through pain.Opioids ▪ Overdose: ▪ Respiratory Depression ▪ Pin point pupil ▪ Drowsy ▪ Naloxone: competitive antagonist to opioid μ-receptors and displaces the opioid and restores consciousness and respiratory rate. ▪ 400 micrograms → 800 micrograms for up to 2 doses at 1 minute intervals → 2 mg for 1 dose → up to 4mg ▪ When Prescribing always consider: ▪ Anti-emetic: Metoclopramide/ Domperidone ▪ Laxatives: stimulant e.g. Senna, Docusate ▪ CKD: Alfentanil ▪ Route: Oral, IM, SC, IV
Control Drugs
Legal requirements:
1. Legible capital letters, indelible ink, Black
2. Patient details
3. Prescriber details
4. Drug details: formulation, strength (if applicable), dose and frequency, total quantity
supplied in words and figures
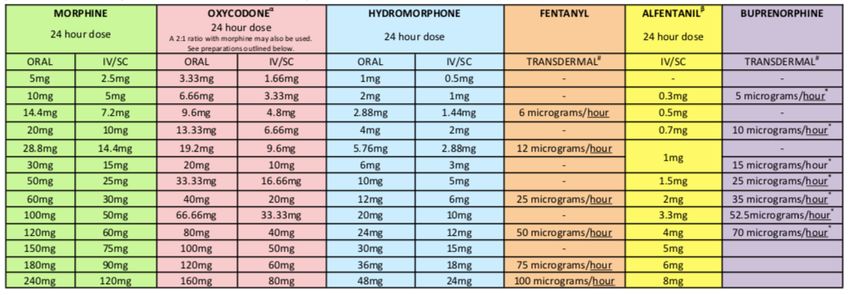
5. Eliminate space for additionsConversions
Palliative Prescribing ▪ More common ▪ Dependence less problematic when taken therapeutically, shouldn’t deter you from offering opioids for severe or chronic pain, especially in end-of-life care. ▪ Modified release or continuous infusion through sub cut/syringe driver ▪ Break through: 1/6th of the total 24hr dose ▪ Anticipatory Meds: ▪ Anti secretary ▪ Anti-emetic ▪ Agitation
Adjuvant Therapy ▪ Pharmacological ▪ Non-Pharmacological ▪ Anti-convulsants e.g. Gabapentin, Pregabalin ▪ Trans-cutaneous electrical nerve stimulation ▪ Antidepressants e.g. Amitriptyline (TENS) ▪ Bisphosphonates ▪ Complementary therapy e.g. massage ▪ Steroids ▪ Counselling ▪ Benzodiazepines ▪ Relaxation techniques ▪ Other treatments e.g. nerve blocks, radiotherapy ▪ Spiritual support ▪ Nefopam
Case 1 27 year-old female has presented to A+E with abdominal pain, nausea and vomiting. She rates her pain 5/10. She has no known drug allergies, no significant PMHx. Please prescribe appropriate analgesia: Paracetamol 1g IV/PO QDS, regularly. Patient tells you she weighs 48.5kg and has been taking co-codamol 30/500 from her GP. Does this change your prescription? Yes, Paracetamol 500mg IV/PO QDS, regularly and omit co-codamol.
Case 2 36 year-old male has presented to the GP with a painful, swollen great toe. After examination you suspect he has gout. He has no known drug allergies. Please prescribe appropriate analgesia: Stat does of Naproxen 750mg PO Then 250mg every 8hrs/TDS PO You anticipate the patient will take the analgesia for at least 4 weeks. Is there any other medication you should co-prescribe? Omeprazole 20mg OD whilst taking Naproxen You review that patients drug history and he is taking 75mg of Aspirin and 50mg of Sertraline. What is he at risk of? Peptic ulceration and GI bleed. You weigh the risk vs benefits
Case 3 85 year old female presented to A+E after a fall. X-ray of the R hip shows she has a NOF#. She is in a lot of pain. She has no NKDA, DHx 75micrograms of Levothyroxine, 1g of Metformin BD, Paracetamol 1g QDS. Please prescribe appropriate analgesia: Morphine 2-10mg IV every 8-6hrs Senna 7.5mg ON Metoclopramide 10mg TDS/every 8 hours She is still in pain. She has a total of 30mg of IV morphine in the last 24hrs. You decide to adjust her prescription for analgesia: Zomorph 15mg PO BD/12hourly PRN Oramorph 5mg PO every 8-6 hourly
Case 4 89yo male patient has metastatic prostate cancer and is prescribed Oramorph 10mg 4 hourly. His pain is well controlled, but develops severe nausea and is struggling to take oral medications. You decide to start a syringe driver. What dose of Morphine will you put into the syringe driver? What will be the PRN SC Morphine dose? Oramorph 10mg x 6 = 60mg PO Morphine in 24 hours. 60mg divided by 2 = 30mg/24 hours via CSCI. The SC PRN dose will be 30mg divided by 6 = 5mg PRN. Every 4 hours, max total dose 30mg in 24 hours.
Tips ▪ Top 100 → the questions at the back ▪ Prescribing Scenarios at a glance ▪ PassMed ▪ Practice as much as you can
Questions? Email: Priya.Abraham1@nhs.net
You can also read

















































