ADULT CONGENITAL HEART DISEASE - NEW GUIDELINES AND CLINICAL CARE PERSPECTIVE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DOI: 10.5644/PI2021.199.04
ACHD - New Guidelines and Clinical Care Perspective
Professional paper
ADULT CONGENITAL HEART DISEASE – NEW
GUIDELINES AND CLINICAL CARE PERSPECTIVE
Nabil Naser, Zumreta Kušljugić
Association of Cardiologists in Bosnia and Herzegovina, Štrosmajerova 6, 71000 Sarajevo, Bosnia
and Herzegovina
Corresponding author:
Nabil Naser
Association of Cardiologists in Bosnia and Herzegovina
Štrosmajerova 6, 71000 Sarajevo
Bosnia and Herzegovina
nabil@bih.net.ba
ORCID ID: http://www.orcid. org/0000-0002-278-8574
Submitted: 2021, accepted: 2021, published: 2021
Abstract
To date, the prevalence of CHD worldwide is ∼9 per 1000 newborns, with substantial geo-
graphic variation. The latest knowledge in the world for the last 50 years about their origin,
diagnosis and therapy has contributed to their care. Since adult patients with CHD now pre-
sent increasing numbers at advanced ages, including the elderly, the term grown-up CHD no
longer appears appropriate and was therefore replaced with adult CHD (ACHD) according
to the ESC guidelines published in 2020 year. Due to medical, surgical, and technological
evolutions over the past decades, >90% of individuals who are born with CHD now survive
into adulthood. ACHD represent a challenge for clinicians. Despite optimal medical and
surgical treatment, many will experience a progressive decline in cardiopulmonary function
leading to advanced heart failure. Severe ventricular dysfunction and/or pulmonary hyper-
tension may not be amenable to corrective repair. Their early recognition and follow-up in
adolescence will contribute to better care for these patients. Importantly, the care for ACHD
patients is a lifelong process and requires advance care planning strategies.
Key words: Adult congenital heart disease, heart failure, pulmonary hypertension, infective
endocarditis, sudden cardiac death.
International Scientific Symposium
52 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”
Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
Introduction
To date, the prevalence of CHD worldwide is ∼9 per 1000 newborns, with
substantial geographic variation. Congenital heart defects (CHD) are more
common than those found in all age groups, including the fetus. The latest
knowledge in the world for the last 50 years about their origin, diagnosis and
therapy has contributed to their care. However, in underdeveloped countries,
millions of children born with CHD do not have adequate diagnosis, therapy,
or prevention.
Since 2006, The World Society for Pediatric and Congenital Heart
Surgery has been promoting the care of children with CHD from fetus to
adulthood, regardless of the economic status of patients, with recommenda-
tions for education, diagnostic and therapeutic care for all. Since 1970, more
than 70 population epidemiological studies have been published worldwide
with a questionnaire on genetics, sociodemographic, medical-obstetric data,
exposure to environmental risks and drugs, risk assessment and prevention of
heart defects. Since adult patients with CHD now present increasing numbers
at advanced ages, including the elderly, the term grown-up CHD no longer
appears appropriate and was therefore replaced with adult CHD (ACHD) ac-
cording to the ESC guidelines published in 2020 year.
Methods and materials
A. Aetiology
Congenital heart defects are disorders of the anatomical structure or function
of the heart and blood vessels, which are most often the result of impaired or
stopped development of certain structures at the level of the embryonic or fe-
tal phase. The exact cause of most congenital heart defects remains unknown.
They are the result of the complex action of genetic and environmental fac-
tors. Knowing the aetiology is important for their prevention.
Chromosomal aberrations and gene mutations have been detected in less
than 10% of congenital heart defects, whether they are isolated or associated
with other genetic abnormalities in syndromes such as Down, Turner, Marfan,
Noonan, Loeys-Dietz and others. There has been remarkable progress in un-
derstanding the genetic basis of cardiovascular malformations. Chromosome
microarray analysis has provided a new tool to understand the genetic ba-
sis of syndromic cardiovascular malformations resulting from microdeletion
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 53
Special Editions ANUBiH CXCIX, OMN 60, p. 52-67
or microduplication of genetic material, allowing the delineation of new
syndromes.
Enzyme deficiencies in fetal cells obtained by amniocentesis or biopsy
of chorionic villi contribute to the prediction of defects, and fetal echocardi-
ography can directly detect cardiovascular malformations during the so-called
risk factors (family burden, mother’s age, etc.). Teratogenic agents, which act
especially during the embryonic development of the heart, have a role in the de-
velopment of congenital heart defects in the first 3 months of pregnancy. They
are divided into infectious, chemical and physical, and the most famous are
rubella and maternal viral infections in general; drugs the mother takes, as well
as heroin, cocaine, smoking, alcohol; then hypoxia, radiation, trauma, etc.
B. Classification of ACHD
The classification of congenital heart defects can be based on anatomical,
functional (hemodynamic), radiological or other characteristics of defects
that are often combined or complex. CHD can be classified as mild, moder-
ate, or severe according to complexity. (Table No. 1)
Table No. 1. Classification of congenital heart disease complexity
MILD:
Isolated congenital aortic valve disease and bicuspid aortic disease
Isolated congenital mitral valve disease (except parachute valve, cleft leaflet)
Mild isolated pulmonary stenosis (infundibular, valvular, supravalvular)
Isolated small ASD, VSD, or PDA
Repaired secundum ASD, sinus venosus defect, VSD, or PDA without residuae or sequellae, such as chamber
enlargement, ventricular dysfunction, or elevated PAP.
MODERATE: (Repaired or unrepaired where not specified; alphabetical order)
Anomalous pulmonary venous connection (partial or total)
Anomalous coronary artery arising from the PA
Anomalous coronary artery arising from the opposite sinus
Aortic stenosis - subvalvular or supravalvular
AVSD, partial or complete, including primum ASD (excluding pulmonary vascular disease)
ASD secundum, moderate or large unrepaired (excluding pulmonary vascular disease)
Coarctation of the aorta
Double chambered right ventricle
Ebstein anomaly
Marfan syndrome and related HTAD, Turner Syndrome
International Scientific Symposium
54 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”
Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
PDA, moderate or large unrepaired (excluding pulmonary vascular disease)
Peripheral pulmonary stenosis
Pulmonary stenosis (infundibular, valvular, supravalvular), moderate or severe
Sinus of Valsalva aneurysm/fistula
Sinus venosus defect
Tetralogy of Fallot – repaired
Transposition of the great arteries after arterial switch operation
VSD with associated abnormalities (excluding pulmonary vascular disease) and/or moderate or greater shunt
SEVERE: (Repaired or unrepaired where not specified; alphabetical order)
Any CHD (repaired or unrepaired) associated with pulmonary vascular disease (including Eisenmenger syndrome)
Any cyanotic CHD (unoperated or palliated)
Double-outlet ventricle
Fontan circulation
Interrupted aortic arch
Pulmonary atresia (all forms)
Transposition of the great arteries (except for patients with arterial switch operation)
Univentricular heart (including double inlet left/right ventricle, tricuspid/mitral atresia, hypoplastic left heart
syndrome, any other anatomic abnormality with a functionally single ventricle)
Truncus arteriosus
Other complex abnormalities of AV and ventriculoarterial connection (i.e., crisscross heart, heterotaxy syndromes,
ventricular inversion).
ASD = atrial septal defect; AV = atrioventricular; AVSD = atrioventricular septal defect; CHD = congenital heart disease; HTAD =
heritable thoracic aortic disease; LV = left ventricle/ventricular; PA = pulmonary artery; PAP = pulmonary artery pressure; PDA =
patent ductus arteriosus; VSD = ventricular septal defect. Source: 2020 ESC Guidelines for the management of adult congenital heart
disease. European Heart Journal, Volume 42, Issue 6, 7 February 2021, Pages 563-645,
The classification into defects without cyanosis and with cyanosis is com-
mon. Cyanosis is divided into defects with left-right shunt and without shunt.
Defects with a shunt are further divided according to the level of communication
between the systemic and pulmonary circulation, and defects without a shunt
depending on whether they refer to the structures of the inflow or outflow trough
the left or right heart. Cyanotic defects are divided into those with increased and
reduced pulmonary flow, based on which the cause of cyanosis (mixing of arte-
rial and venous blood or reduction of pulmonary flow) is clarified.
Congenital heart defects in adults include: atrial septal defect (ASD),
atrial septal defect and anomalous pulmonary venous connection, ventricular
septal defect (VSD), atrioventricular septal defect (AVSD), patent ductus ar-
teriosus (PDA), left ventricular outflow tract obstruction (LVOTO), valvular
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 55
Special Editions ANUBiH CXCIX, OMN 60, p. 52-67
aortic stenosis, supravalvular aortic stenosis, subaortic stenosis, coarctation of
the aorta (CoA), Aortopathies including Marfan syndrome, right ventricular
outflow tract obstruction (RVOTO), Ebstein’s anomaly, Tetralogy of Fallot,
Pulmonary atresia with ventricular septal defect, transposition of the great
arteries, congenitally corrected transposition of the great arteries (ccTGA),
univentricular heart, patients after Fontan operation and coronary anomalies.
To date, ∼90% of patients with mild, 75% with moderate, and 40% with com-
plex heart defects reach the age of 60 years.
The frequency of individual defects is different. Although over a hundred
anomalies have been described, 85% are due to 8 congenital heart defects
that also occur in adults: atrial septal defect, ventricular septal defect, patent
ductus arteriosus, congenital aortic stenosis, aortic coarctation, pulmonary
stenosis, tetralogy of Fallot, transposition of great arteries.
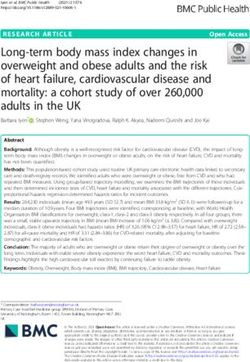
Figure 1. A secundum atrial septal defect (ASD) in 46 years old female patient with
left-to-right shunt was confirmed by 2-dimensional transthoracic echocardiogram
(TTE) (Panel A), 2-dimensional TTE color Doppler (Panel B). Transesophageal
bicaval view with color Doppler (TEE) (Panel C) and TTE echocardiography of
the final result after transcatheter closure with Amplatzer occluder (Panel D).
International Scientific Symposium
56 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”
Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
Secundum ASD (80% of ASDs; located in the region of the fossa ovalis
and its surrounding). The ASD type secundum is the communication between
the left and right atria placed lower towards the mitral valves. It is often as-
sociated with anterior mitral valve fissure and consequent mitral regurgita-
tion (MR). Device closure has become the first choice for secundum defect
closure, when feasible, based on the morphology (includes stretched diameter
≤38 mm and sufficient rim of 5 mm except towards the aorta).
Primum ASD [15%; synonyms: partial AV septal defect [atrioventricular
septal defect (AVSD) with communication on the atrial level only], partial
AV canal; located near the crux, AV valves are typically malformed, result-
ing in various degrees of regurgitation. The shunt volume depends on RV/LV
compliance, defect size, and LA/RA pressure. If the defect is large, it burdens
the pulmonary circulation and gives symptoms. It can be treated by surgical
or catheter interventional treatment.
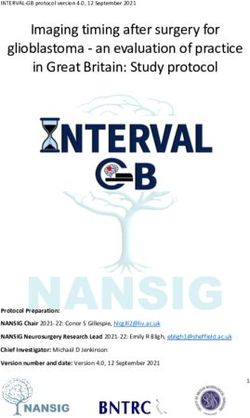
Figure 2. A perimembranous ventricular septal defect with small muscular VSD
in 34 years old male with left - right shunt was confirmed by 2-dimensional
transthoracic echocardiogram (TTE) (Panel A) and 2-dimensional TTE color
Doppler (Panel B, C and D).
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 57Special Editions ANUBiH CXCIX, OMN 60, p. 52-67
VSD is mostly diagnosed and, when indicated, treated before adulthood.
Spontaneous closure is frequent in childhood. Several locations of the defect
within the interventricular septum are possible, and these can be divided into
four groups according to their location within the RV: perimembranous /para-
membranous/subaortic/conoventricular (most common, ∼80% of VSDs),
muscular/trabecular (up to 15-20%), Outlet (with or without malalignment of
the outlet septum) and Inlet/AV canal/AVSD type. Due to the increased blood
flow on the left side, the pulmonary circulation is burdened. Surgical closure
can be performed with low operative mortality (1–2%) and good long-term
results. Transcatheter closure has become an alternative, particularly in re-
sidual VSDs, in VSDs that are poorly accessible for surgical closure, and in
muscular VSDs that are located centrally in the interventricular septum.
Patent ductus arteriosus (PDA) is the persistent communication between
the proximal left PA and the descending aorta just distal to the left subclavian
artery. It can be associated with a variety of CHD lesions, however, in adults,
it is usually an isolated finding. PDA originally results in L–R shunt and LV
and LA volume overload. In adults, calcification of the PDA may cause a
problem for surgical closure. Device closure is the method of choice, even if
cardiac operations are indicated due to other concomitant cardiac lesions and
can be successfully performed in the vast majority of adults with a very low
complication rate.
Figure 3. Ebstein’s Anomaly with atrialization of the right ventricle in 56 years
old female patient with history of supraventricular paroxysmal tachycardia and
ischemic cerebrovascular insult.
Ebstein’s anomaly is characterized by abnormally formed and apically
displaced leaflets of the tricuspid valve. The anterior leaflet usually originates
International Scientific Symposium
58 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
at the annular level but is enlarged and sail-like, while the septal and posterior
leaflets are displaced towards the RV apex and often tethered to the endocar-
dium. Clinical symptoms determine the treatment. Conservative therapy can
alleviate symptoms temporarily and create a beneficial basis for the following
operation. Surgical repair remains challenging and should only be performed
by surgeons with specific experience in this lesion.
CoA is considered as part of a generalized arteriopathy, and not only as
narrowing of the aorta. It occurs as a discrete stenosis or as a long, hypo-
plastic aortic (arch) segment. Typically, CoA is located in the area where the
ductus arteriosus inserts, and only in rare cases occurs ectopically (ascend-
ing, descending, or abdominal aorta). Associated lesions include bicuspid
aortic valve (up to 85%), ascending aortic aneurysm, subaortic stenosis or
supraoptic stenosis and (supra)mitral valve stenosis. Patients with CoA who
reach adolescence demonstrate particularly good long-term survival up to age
60 years. The natural course may be complicated by left heart failure, in-
tracranial haemorrhage (from berry aneurysm), infective endocarditis, aortic
rupture/dissection, premature coronary and cerebral artery disease, and asso-
ciated heart defects. (1,2,3.4.5.6)
C. Clinical signs
Due to medical, surgical, and technological evolutions over the past decades,
>90% of individuals who are born with CHD, now survive into adulthood. As
a result, the prevalence of CHD in the community has increased and now by
far exceeds the number of children with CHD.
In congenital heart defects, anatomical changes cause functional changes
in the heart and circulation, which further cause new anatomical changes and
vice versa. They are interdependent, dynamic and constantly progressing,
from the beginning to the end of life. Depending on the severity of the hemo-
dynamic disorders, a number of defects are fatal before birth or immediately
after birth. A significantly higher number of anomalies allow the development
of the child, but with disorders (developmental delay, feeding dyspnoea, heart
failure, etc.) that require correction in the earliest childhood or during adoles-
cence. There are also defects with mild hemodynamic disorders and without
them, which remain undiagnosed in childhood, and for quite a long time in
adults until the appearance of problems due to complications of the defect,
e.g., pulmonary hypertension and heart failure in the IV or V decade of life of
a patient with a moderately large left-right shunt.
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 59Special Editions ANUBiH CXCIX, OMN 60, p. 52-67
ACHD have an anamnestic long asymptomatic period, followed by a feel-
ing of fatigue, shortness of breath on exertion, palpitations, arrhythmias, res-
piratory infections, and bacterial endocarditis.
Thanks to advances in early detection, medical and/or surgical treatment
of defects and interventional cardiology, palliative/total correction of even
complex congenital heart defects is performed at an earlier age, which allows
the patient to live with fewer symptoms or without them. In the population
of adults with congenital heart defects, more and more patients are operat-
ed on instead of patients with advanced functional and/or pathoanatomical
disorders that prevent surgical intervention (except for transplantation). The
condition of the pulmonary vascular bed and pulmonary hypertension play a
decisive role in determining the operability of the defect, on which the clini-
cal manifestations, course and prognosis of many defects also depend.
Pulmonary hypertension occurs due to increased blood flow and/or re-
sistance in the pulmonary circulation. Increased pulmonary flow is given by
defects with the left-right shunt. Increased pulmonary vascular resistance is
most often the result of histopathological, obstructive changes in the small
muscular arteries and pulmonary arterioles that occur in patients with pul-
monary hypertension and/or increased pulmonary blood flow. Assessment of
pulmonary hypertension and the condition of the pulmonary vascular bed is
most often performed by catheterization of the heart. In addition to pressures,
the magnitudes of blood flow and vascular resistance in the pulmonary and
systemic bloodstream are determined and their relative ratios are calculated.
In advanced cases, pulmonary angiography and lung biopsy are required.
Cyanosis: Central-type cyanosis in adults with congenital heart defect is
a symptom and sign of hypoxemia due to the right-left shunt. Congenital cy-
anotic heart defects are less common, and cyanosis occurs much more often
due to left-right shunt reversal in unoperated patients with initially cyanotic
defect (Eisenmenger’s syndrome due to a large interventricular septal defect,
atrioventricular septal defect or open arterial canal).
Erythrocytosis is a physiological response to hypoxemia. Increased eryth-
rocyte mass (haematocrit) and total blood volume are features of polycythae-
mia in patients with right-left shunt. Polycythaemia itself has side effects:
thrombosis, embolism, bleeding. Thromboembolic complications and symp-
toms such as headache, dizziness, fatigue, numbness of the fingers, are caused
by increased blood viscosity due to high haematocrit (Hct> 60%). Bleeding
International Scientific Symposium
60 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
is a consequence of haemostasis disorders, due to impaired platelet function
and abnormalities in the coagulation and fibrinotic system.
Infective endocarditis is a common complication in patients with congeni-
tal heart defects, and routine antibiotic prevention is mandatory in all non-
operated patients, as well as in most patients after defect correction. Patients
are especially at risk after the implantation of valves (artificial, heterograft
or homograft) and “conduit”, so in these cases, parenteral administration of a
combination of antibiotics is recommended. (1,2,9,11,12,13,14,15,17)
D. Diagnostic tools
The diagnosis is made by clinical examination, ECG, X-ray of the lungs and
heart, biomarkers, echocardiography, Cardiac magnetic resonance imaging
(CMRI), Computed tomography (CT), cardiopulmonary exercise testing
(CPET) and cardiac catheterization. Echocardiography remains the first-
line investigation and continues to evolve, with improved functional assess-
ment using 3D echocardiography. Cardiovascular Magnetic Resonance
Imaging (CMRI) has become an essential facility in the specialist unit. It
enables 3D anatomical reconstruction, which is not restricted by body size or
acoustic windows and has rapidly improving spatial and temporal resolution.
Cardiovascular CT has high spatial resolution and rapid acquisition time; it
is particularly relevant for imaging the great vessels, coronary arteries, and
collateral arteries, and for parenchymal lung disease. Cardiopulmonary ex-
ercise testing has an important role in the CHD population, in which quality
of life and functional capacity are key measures of the success of interven-
tion. Cardiac catheterization is mainly reserved for resolution of specific ana-
tomical and physiological questions, or for intervention. Different classes of
biomarkers have been reported to be associated with adverse events in the
CHD population, including: neurohormones peptides [B-type natriuretic pep-
tide (BNP) and N-terminal-pro-BNP (NT-pro-BNP)], markers of myocardial
injury (high-sensitivity troponins) or inflammation marker (high-sensitivity
C-reactive protein). (1,2,6,7,10,17)
D. Therapeutic consideration
Heart Failure: The development of heart failure is a common problem af-
fecting 20 to 50% of the ACHD population and is a main cause of death.
Arrhythmias: The entire spectrum of arrhythmias may be encountered in
ACHD patients. Supraventricular arrhythmias: atrioventricular reentrant
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 61Special Editions ANUBiH CXCIX, OMN 60, p. 52-67 tachycardia (AVRT), intraatrial reentrant tachycardia (IART), ectopic atri- al tachycardia (EAT) and atrial fibrillation (AF). Ventricular arrhythmias: sustained ventricular tachycardia (SVT) & sudden cardiac death (SCD). Bradycardia: sinus node dysfunction (SND) and AV block. Sudden cardiac death (SCD) related to ventricular arrhythmia is of concern (7–26% of all deaths in adults). Although the incidence in the CHD population at large is relatively low (
Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective Future directions The main unmet needs in adult congenital heart disease are: 1. Increase in the number of randomized controlled trials. 2. Advanced care of heart failure in ACHD (Mechanical assist devices, transplant in complex CHD). 3. Cardiac resynchronization therapy in complex ACHD. 4. Leadless pacing. 5. Primary prevention of sudden cardiac death in patients with systemic right ventricle or single ventricular physiology. 6. Targeted therapies for pulmonary hyperten- sion in Fontan patients. 7. RCTs for novel therapeutic agents in pulmonary hypertension associated with CHD. 8. Drug therapies in patients with failing systemic right ventricle or single ventricle. 9. Direct oral anticoagulants in ACHD patients. 10. Implementation of AI for better assessing systemic right ventricular or singe ventricle failure. 11. Development of validated prognostic models. 12. Omics-based personalized healthcare. There is a need for special- ist ACHD centres worldwide. Staff requirements for specialist ACHD centres include adult/paediatric cardiologist with ACHD certification, ACHD imag- ing specialist (certified in TTE/TOE, CMR, CCT), congenital interventional cardiologist, CHD surgeon, anaesthesiologist with CHD experience and ex- pertise, specialist nurse, invasive electrophysiologist with ACHD experience, pulmonary vascular disease expert, clinical geneticists, psychologist, social worker and palliative care team. (3,1,2) Conclusion ACHD represent a challenge for clinicians. Their early recognition and fol- low-up in adolescence will contribute to better care of these patients. The vast majority of patients survive into adulthood and their profile in terms of comorbidities has changed. Organization of tertiary and nontertiary care, collaboration at national and international level, randomized controlled trials and implementation of novelties, such as research based biobanking, e-health and artificial intelligence should all be employed to meet their healthcare needs. Importantly, the care for ACHD patients is a lifelong process and also requires advance care planning strategies. References 1. Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Lung B et al. 2020 ESC Guidelines for the management of adult congenital heart disease. European Heart Journal, Volume 42, Issue 6, 7 February 2021, Pages 563–645, https:// doi.org/10.1093/eurheartj/ehaa554. International Scientific Symposium “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 63
Special Editions ANUBiH CXCIX, OMN 60, p. 52-67
2. Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS et al. 2018 AHA/ACC
Guideline for the Management of Adults With Congenital Heart Disease: Executive
Summary: A Report of the American College of Cardiology/American Heart Association
Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019 Apr 2;73(12):1494-
1563. doi: 10.1016/j.jacc.2018.08.1028. Epub 2018 Aug 16. Erratum in: J Am Coll
Cardiol. 2019 May 14;73(18):2361. PMID: 30121240.
3. Ntiloudi D, Gatzoulis MA, Arvanitaki A, Karvounis H, Giannakoulas G. Adult congenital
heart disease: Looking back, moving forward. International Journal of Cardiology
Congenital Heart Disease, Volume 2, February 2021, 100076.
4. van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ,
Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic
review and meta-analysis. J Am Coll Cardiol 2011;58:2241–2247.
5. Michelena HI, Della Corte A, Prakash SK, Milewicz DM, Evangelista A, Enriquez-
Sarano M. Bicuspid aortic valve aortopathy in adults: incidence, etiology, and clinical
significance. Int J Cardiol 2015;201:400–407.
6. Nabil Naser, Nura Hadžiomerović, Sevleta Avdić. Transcatheter device closure of
secundum septal defect in adult patient. Acta Inform Med 2021, 29(1):65-70. doi:
10.5455/aim.202129 .65-70.
7. Cohen MS, Eidem BW, Cetta F, et al.. Multimodality imaging guidelines of patients with
transposition of the great arteries: a report from the American Society of Echocardiography.
Developed in collaboration with the Society for Cardiovascular Magnetic Resonance and
the Society of Cardiovascular Computed Tomography.J Am Soc Echocardiogr. 2016;
29:571–621.
8. Thomet C, Moons P, Budts W, De Backer J, Chessa M, Diller G, Eicken A et al. ESC
Working Group on Grown-up Congenital Heart Disease. Staffing, activities, and
infrastructure in 96 specialised adult congenital heart disease clinics in Europe. Int J
Cardiol 2019;292:100–105.
9. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F et al. ESC
Scientific Document Group. 2015 ESC Guidelines for the management of infective
endocarditis: The Task Force for the Management of Infective Endocarditis of the
European Society of Cardiology (ESC). Eur Heart J 2015;36:3075–3128.
10. Baggen VJ, van den Bosch AE, Eindhoven JA, Schut AW, Cuypers JA,, Witsenburg M et
al. Prognostic value of N-terminal pro-B-type natriuretic peptide, troponin-T, and growth-
differentiation factor 15 in adult congenital heart disease. Circulation 2017;135:264–279.
11. Van De Bruaene A, Hickey EJ, Kovacs AH, Crean AM, Wald RM, Silversides CK et al.
Phenotype, management and predictors of outcome in a large cohort of adult congenital
heart disease patients with heart failure. Int J Cardiol 2018;252:80–87.
12. Van De Bruaene A, Meier L, Droogne W, De Meester P, Troost E, Gewillig M, Budts W.
Management of acute heart failure in adult patients with congenital heart disease. Heart
Fail Rev 2018;23:1–14.
13. Priori SG, Blomstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J et al.
2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the
prevention of sudden cardiac death: The Task Force for the Management of Patients with
Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European
Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and
Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867.
International Scientific Symposium
64 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
14. Simonneau G, Montani D, Celermajer DS, Denton CP,, Gatzoulis MA, Krowka M,
Williams PG, Souza R. Haemodynamic definitions and updated clinical classification of
pulmonary hypertension. Eur Respir J 2019;53:1801913.
15. Diller GP, Korten MA, Bauer UM, Miera O, Tutarel O, Kaemmerer H, Berger F,
Baumgartner H, German Competence Network for Congenital Heart Defects Investigators.
Current therapy and outcome of Eisenmenger syndrome: data of the German National
Register for congenital heart defects. Eur Heart J 2016;37:1449–1455.
16. Chessa M, Baumgartner H, Michel-Behnke I, Berger F, Budts W, Eicken A, Sondergaard
L, Stein J, Wiztsemburg M, Thomson J. ESC Working Group Position Paper: transcatheter
adult congenital heart disease interventions: organization of care - recommendations
from a Joint Working Group of the European Society of Cardiology (ESC), European
Association of Pediatric and Congenital Cardiology (AEPC), and the European
Association of Percutaneous Cardiac Intervention (EAPCI). Eur Heart J 2019;40:1042–
1048.
17. Oliver JM, Gallego P, Gonzalez AE, Garcia-Hamilton D, Avila P, Alonso A, Ruiz-Cantador
J, Peinado R, Yotti R, Fernandez-Aviles F. Impact of age and sex on survival and causes
of death in adults with congenital heart disease. Int J Cardiol 2017;245:119–124.
18. Sluman MA, Apers S, Sluiter JK, Nieuwenhuijsen K, Moons P, Luyckx K, Kovacs AH et
al. Education as important predictor for successful employment in adults with congenital
heart disease worldwide. Congenit Heart Dis 2019;14:362–371.
19. Butera G, Carminati M, Chessa M, Youssef R, Drago M, Giamberti A, Pome G, Bossone
E, Frigiola A. Percutaneous versus surgical closure of secundum atrial septal defect:
comparison of early results and complications. Am Heart J 2006;151:228–234.
20. Hager A, Kanz S, Kaemmerer H, Schreiber C, Hess J. Coarctation Long-term Assessment
(COALA): significance of arterial hypertension in a cohort of 404 patients up to 27 years
after surgical repair of isolated coarctation of the aorta, even in the absence of restenosis
and prosthetic material. J Thorac Cardiovasc Surg 2007;134:738–745.
21. von Kodolitsch Y, Rybczynski M, Vogler M, Mir TS, Schuler H, Kutsche K, Rosenberger
G et al. The role of the multidisciplinary health care team in the management of patients
with Marfan syndrome. J Multidiscip Healthc 2016;9:587–614.
22. Rydman R, Shiina Y, Diller GP, Niwa K, Li W, Uemura H, Uebing A, Barbero U, Bouzas
B, Ernst S, Wong T, Pennell DJ, Gatzoulis MA, Babu-Narayan SV. Major adverse
events and atrial tachycardia in Ebstein’s anomaly predicted by cardiovascular magnetic
resonance. Heart 2018;104:37–44.
23. McElhinney DB, Sondergaard L, Armstrong AK, Bergersen L, Padera RF, Balzer DT,
Lung TH, Berger F, Zahn EM, Gray RG, Hellenbrand WE, Kreutzer J, Eicken A, Jones
TK, Ewert P. Endocarditis After transcatheter pulmonary valve replacement. J Am Coll
Cardiol 2018;72:2717–2728.
24. Zaragoza-Macias E, Zaidi AN, Dendukuri N, Marelli A. Medical therapy for systemic
right ventricles: a systematic review (part 1) for the 2018 AHA/ACC Guideline for the
management of adults with congenital heart disease: a report of the American College of
Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J
Am Coll Cardiol 2019;73:1564–1578.
25. Khairy P, Fernandes SM, Mayer JEJr., Triedman JK, Walsh EP, Lock JE, Landzberg MJ.
Long-term survival, modes of death, and predictors of mortality in patients with Fontan
surgery. Circulation 2008;117:85–92.
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 65Special Editions ANUBiH CXCIX, OMN 60, p. 52-67
26. Naser Nabil, Bukša Marko, Lozo Vesna, Brđanović Snježana. Ebstein’s Anomaly with
ASD,VSD & paradoxical cerebral emboli. Third congress of cardiology and angiology of
Bosnia and Herzegovina, Med Arch 2004; 58(2, suppl.1):53.
27. Al-Tawil Dj, Talirević M, Naser Nabil, Arslanagić A, Talirević E. Ebstein’s Anomaly
with PFO and paroxismal supraventricular tachycardia. Med Arch 2000; 54(3):163-164.
28. Naser Nabil, Talirević M , Al-Tawil Dj , Bukša Marko, Talirević Emir. Single ventricle
with pulmonary valve stenosis and laposition of great arteries. Med Arch 2000; 54(2):
89-91.
International Scientific Symposium
66 “Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)”Nabil Naser, Zumreta Kušljugić: Adult Congenital Heart Disease – New Guidelines and Clinical Care Perspective
UROĐENE SRČANE BOLESTI ODRASLIH - NOVE
SMJERNICE I PERSPEKTIVE KLINIČKE NJEGE
Apstrakt
Trenutna prevalencija urođenih srčanih mana (USM, eng. CHD) u svijetu je ∼9 na 1000
novorođenčadi, sa značajnim geografskim varijacijama. Najnovija svjetska saznanja u po-
sljednjih 50 godina o njihovom porijeklu, dijagnozi i terapiji doprinijela su njezi. Budući
da danas ima sve više odraslih pacijenata s urođenim srčanim manama čak i u poodmakloj
dobi, uključujući duboku starost, pojam “grown-up CHD” više se ne čini prikladnim i stoga
je zamijenjen pojmom “adult CHD” (ACHD) prema smjernicama ESC-a objavljenim 2020.
godine. Zbog medicinskog, hirurškog i tehnološkog napretka u posljednjim decenijama,
>90% pojedinaca koji su rođeni s USM sada preživljavaju i u odraslu dob. ACHD predstav-
ljaju izazov za kliničare. Uprkos optimalnom medicinskom i hirurškom liječenju, mnogi će
doživjeti progresivno smanjenje kardiopulmonalne funkcije što dovodi do uznapredovale
srčane insuficijencije. Teška ventrikularna disfunkcija i/ili plućna hipertenzija možda neće
biti podložne korektivnim intervencijama. Njihovo rano prepoznavanje i praćenje u adoles-
cenciji doprinijet će boljoj skrbi za ove pacijente. Važno je istaknuti da je briga o pacijentima
s ACHD-om doživotni proces i zahtijeva unaprijed planirane strategije njege.
Ključne riječi: urođena srčana mana kod odraslih, zatajenje srca, plućna hipertenzija, infek-
tivni endokarditis, iznenadna srčana smrt
International Scientific Symposium
“Diagnostics in Cardiology and Grown-Up Congenital Heart Disease (GUCH)” 67You can also read