A randomised, double-blind, placebo-controlled phase 3 study of lenabasum in diffuse cutaneous systemic sclerosis: RESOLVE-1 design and rationale
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A randomised, double-blind, placebo-controlled
phase 3 study of lenabasum in diffuse cutaneous
systemic sclerosis: RESOLVE-1 design and rationale
R. Spiera1, D. Khanna2, M. Kuwana3, D.E. Furst4, T.M. Frech5,
L. Hummers6, W. Stevens7, M. Matucci-Cerinic8, M. Baron9, O. Distler10,
N. Dgetluck11, B.J. Bloom11, Q. Dinh11, B. White11, C.P. Denton12
Affiliations: page S-131. ABSTRACT Introduction
Robert Spiera, MD Objective. The multi-systemic, heter- Systemic sclerosis (SSc) is a life-threat-
Dinesh Khanna, MD, MSc ogenous nature of diffuse cutaneous ening autoimmune disease character-
Masataka Kuwana, MD, PhD systemic sclerosis (dcSSc) presents ised by thickened skin resulting from
Daniel E. Furst, MD challenges in designing clinical studies vasculopathy, inflammation, and fibro-
Tracy M. Frech, MD
that can demonstrate a treatment effect sis (1-5). Patients with diffuse cutane-
Laura Hummers, MD
Wendy Stevens, MD on overall disease burden. We describe ous systemic sclerosis (dcSSc) experi-
Marco Matucci-Cerinic, MD, PhD the design of the first Phase 3 study ence more widespread disease with the
Murray Baron, MD in dcSSc patients where the Ameri- involvement of multiple organ systems
Oliver Distler, MD can College of Rheumatology (ACR) including gastrointestinal, pulmonary,
Nancy Dgetluck Combined Response Index in diffuse musculoskeletal, cardiovascular, and
Bradley J. Bloom, MD cutaneous Systemic Sclerosis (CRISS) kidney disease (5). Patients with SSc
Quinn Dinh, MD
score was chosen prospectively as the experience markedly impaired health
Barbara White, MD
Christopher P. Denton, FRCP primary outcome. The CRISS measures status compared to the general popula-
Please address correspondence to:
key clinical disease parameters and pa- tion, as well as increased mortality (6,
Robert Spiera, tient-reported outcomes (PROs). 7). Often, SSc patients are treated with
Department of Medicine/Division Methods. RESOLVE-1 is a Phase 3, immunosuppressives. Currently, there
of Rheumatology, randomised, double-blind, placebo- are no approved treatments for overall
The Hospital for Special Surgery, controlled trial of dcSSc patients evalu- disease in SSc specifically targeting
535 East 70 Street, ating the efficacy and safety of lenaba- both inflammation and fibrosis, key
New York City, NY 10021, USA. sum. Patients ≥18 years of age with dc- drivers of SSc pathophysiology (8, 9).
E-mail: spierar@hss.edu
SSc and disease duration ≤6 years were Recently, nintedanib (10) was approved
Received on August 12, 2020; accepted in eligible. Patients could continue stable for slowing the rate of decline in pul-
revised form on October 27, 2020.
background therapy for dcSSc, includ- monary function in patients with SSc-
Clin Exp Rheumatol 2021; 39 (Suppl. 131): ing stable immunosuppressive thera- associated interstitial lung disease (SSc-
S124-S133.
pies. They were randomised to lenaba- ILD), but improvement in other SSc
© Copyright Clinical and
sum 5 or 20 mg twice daily or placebo. disease domains was not demonstrated
Experimental Rheumatology 2021.
The primary efficacy outcome was the (11). Thus, a need exists for pharmaco-
Key words: lenabasum, systemic mean change from baseline to 52 weeks logical treatments that comprehensively
sclerosis, study design, rationale in the ACR CRISS score. address the total disease burden in SSc.
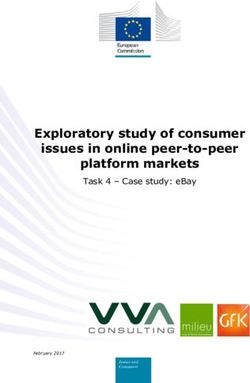
Results. The study enrolled 365 pa- Clinical investigations of pharmacolog-
tients over 1.5 years at 77 sites in 13 ical approaches to SSc have consisted
countries in North America, Europe, mostly of placebo-controlled studies,
Israel, and Asia-Pacific, with the last usually of 6-12 months duration that
patient first visit on May 1, 2019. often fail to include patient-reported
Conclusion. RESOLVE-1 is the first outcomes (PROs) (12). An unmet
Phase 3 interventional study to date need remains for new treatments that
in dcSSc to prospectively use the ACR meaningfully improve overall disease,
CRISS as the primary efficacy outcome. affecting patients’ survival, function,
Eligibility criteria allowed background and/or quality of life. Identifying such
therapy as might occur in clinical prac- therapies is challenging because there is
tice. This approach also facilitated a paucity of patients available for study,
Funding: this work was supported timely patient enrolment. RESOLVE-1 the patient population is highly heterog-
by Corbus Pharmaceutics, Inc., provides a novel study design that may enous, displaying variable disease fea-
Norwood, MA, USA. be used for future Phase 3 dcSSc studies tures, and there had been no validated
Competing interests: page S-131. to assess the holistic efficacy of therapy. outcome measures to assess the overall
S-124 Clinical and Experimental Rheumatology 2021
Rationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
disease (9, 13). Recent publications The study protocol and any amend- Treatment
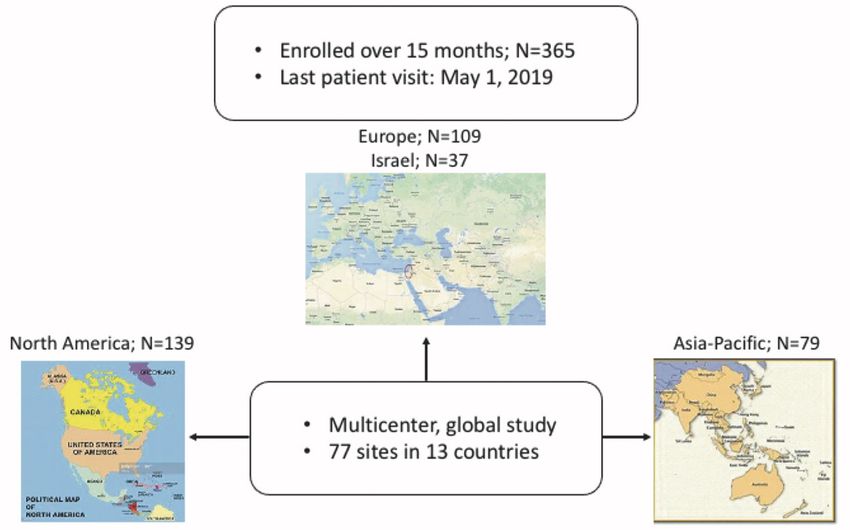
called for study designs of at least 12 ments and informed consent forms Patients were randomised in a 1:1:1 ra-
months duration including broad pa- were reviewed and approved by an In- tio to twice daily treatment with lenaba-
tient selection criteria and both clinical stitutional Review Board/Ethics Com- sum 5 mg, lenabasum 20 mg or match-
and patient focused assessments (14). mittee for each study site. Patients pro- ing placebo, and randomisation was
In a 16-week Phase 2 study in patients vided written informed consent prior to stratified by location (a) United States;
with dcSSc, lenabasum, an oral, selec- participation in any study procedures. b) Canada, Europe, Australia; or c)
tive, cannabinoid receptor type 2 (CB2) An independent, unblinded Data Moni- Asia) and by SSc disease duration (≤24
agonist, was safe and well-tolerated toring Committee (DMC) evaluated or >24 months). An interactive web-
and was associated with improvements safety data to provide recommenda- based response system (IWRS) was
in the American College of Rheumatol- tions on safe continuation of the study. used to assign a unique identification
ogy (ACR) Combined Response Index number to each patient at screening,
in diffuse cutaneous Systemic Sclero- Patient selection and patients were randomised at Visit 1
sis (CRISS) score (15). RESOLVE-1 To be eligible, patients had to be ≥18 (baseline) from a central location.
is a Phase 3 study designed to evaluate years of age, had to fulfil 2013 ACR Lenabasum and placebo capsules had
the efficacy, safety, and tolerability of classification criteria for SSc (17) and identical physical appearance. All pa-
lenabasum versus placebo in patients had have dcSSc (skin thickening on up- tients, the clinical site study staff and
with dcSSc. We describe the rationale per arms proximal to the elbows, upper Corbus remained blinded to treatment
supporting the design, patient selec- legs proximal to the knees, or trunk). In assignment during the entire study.
tion, outcome measures, and statistical addition, patients were required to have Eligibility criteria permitted patients
analysis plan of RESOLVE-1. SSc disease duration ≤6 years from the to receive treatment with stable doses
time of the first non-Raynaud’s symp- of concomitant immunosuppressive
Methods and analysis tom; if the disease duration was >3 medications except oral prednisone
The primary objective of RESOLVE-1 years and ≤6 years, then the modified >10 mg per day (or equivalent) or cy-
was to evaluate the efficacy of lenaba- Rodnan skin score (mRSS) (18) had to clophosphamide. After baseline, doses
sum compared to placebo in the treat- be ≥15 (of 51 maximum score). Enrol- of concomitant immunosuppressive
ment of SSc by assessing the American ment of patients with a disease duration medication(s) could be increased, or
College of Rheumatology (ACR) Pro- >3 years and ≤6 years and mRSS ≥15 new non-investigational immunosup-
visional Combined Response Index in was limited to no more than one-third of pressive medication(s) could be started
diffuse cutaneous Systemic Sclerosis the total study enrolment. At screening, by study investigators 1) if the patient
(CRISS) (16) score at Week 52. The a Patient Global Assessment score 33 or had a documented increase in signs or
study is registered at ClinicalTrials.gov: physician global assessment (MDGA) symptoms of SSc; or 2) if it was consid-
NCT03398837. score ≥3 was required. Patient were re- ered in the best interest of the patient to
quired to be on stable treatment for SSc treat the increase in signs or symptoms
Study design ≥28 days before the first dose of study with a change in dose of concomitant
This 52-week, randomised, double- drug (Visit 1); be willing to remain immunosuppressive medications or the
blind, placebo-controlled study enrolled on their baseline immunosuppressive addition of new non-investigational
patients who satisfied 2013 American treatment for SSc throughout the study; immunosuppressive medications.
College of Rheumatology (ACR) criteria be willing to not use any cannabinoids
for SSc (Fig. 1) (17). The study consist- including recreational marijuana, medi- Efficacy assessments
ed of a screening phase of up to 4 weeks cal marijuana or other prescription can- The primary efficacy variable was the
and a treatment phase of 52 weeks. The nabinoids throughout the study. ACR CRISS score at Week 52 (Table
study included a screening visit and Patients were excluded if they were II). The ACR CRISS score is a con-
11 study visits (Visits 1-11), which oc- medically unstable or had SSc with end- tinuous variable between 0.0 and 1.0.
curred on Day 1 and at the completion stage organ involvement; concomitant A higher score indicates greater likeli-
of Weeks 4, 8, 14, 20, 26, 32, 38, 44, 48, inflammatory myositis, rheumatoid ar- hood of improvement during the study.
and 52. Patients were enrolled at clinical thritis or systemic lupus erythematosus No improvement was defined as ACR
sites located in North America, Europe by ACR criteria; or a positive test for CRISS score = 0, and subjects were au-
(including the UK and Israel), and the anti-centromere antibody, although pa- tomatically assigned a score of zero if
Asia-Pacific region (Fig. 2). tients with a positive test and definite they developed any one or more of the
dcSSc could be enrolled, when agreed following during the trial: 1) new scle-
Ethics and safety monitoring by both investigator and medical moni- roderma renal crisis; 2) decline from
This study was conducted in accord- tor. Full inclusion and exclusion criteria baseline in FVC % predicted (ppFVC)
ance with the principles of the Dec- are provided in Table I. The eligibility by 15%, confirmed after 1 month with
laration of Helsinki and International of each patient had to be reviewed and ppFVCRationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al. Fig. 1. Study design. Fig. 2. Patient enrolment. ejection fraction
Rationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
Table I. Inclusion/exclusion criteria.
Individuals who meet ALL the following criteria at screening were eligible for enrolment:
1. Fulfills the 2013 ACR criteria for systemic sclerosis (van den Hoogen, 2013)
2. Diffuse cutaneous SSc (skin thickening on upper arms proximal to the elbows, upper legs proximal to the knees, or trunk)
3. ≥18 years of age at the time Informed Consent is signed
4. Written informed consent from the subject
5. Disease duration ≤6 years from the first non-Raynaud’s symptom. If disease duration is >3 years and ≤6 years, then mRSS ≥15. Subjects with disease
duration >3 years and ≤6 years and mRSS ≥15 will be limited to no more than 1/3rd of the subjects.
6. Patient Global Assessment ≥3 or MDGA ≥3
7. Stable treatment for SSc ≥28 days before Visit 1
8. Willing to not start or stop any immunosuppressive medications for SSc from Visit 1 through Visit 11, unless a change is considered in the subject’s best
medical interest by the site investigator or another physician who has primary responsibility for treating the subject’s SSc.
9. Willing not to use any cannabinoids including recreational marijuana, medical marijuana and other prescription cannabinoids from Screening through
Visit 11
10. Women of childbearing potential (WOCBP) must not be pregnant or breastfeeding at Screening or Visit 1 and must be using at least one highly effec-
tive method of contraception (failure rate 10 mg per day or equivalent within 28 days before Visit 1. Treatment with intravenous corticosteroids within 28
days before Visit 1 is not allowed, and treatment with intra-articular corticosteroids within 28 days before Visit 1 is allowed (topical corticosteroids
are allowed).
b. New or increase in doses of any non-corticosteroid immunosuppressive medication within 8 weeks before Screening
c. Treatment with cyclophosphamide within 3 months before Visit 1
3. Concomitant inflammatory myositis, rheumatoid arthritis, or systemic lupus erythematosus when definite classification criteria for those diseases are
met (Bohan and Peter criteria for polymyositis and dermatomyositis [Bohan and Peter, 1975a; 1975b]; 2010 rheumatoid arthritis classification criteria
of ACR/EULAR [Aletaha, 2010]; ACR revised criteria for the classification of systemic lupus erythematosus [Hochberg, 1997]).
4. SSc-like illnesses related to exposures or ingestions
5. A positive test for anti-centromere antibody at Screening.
6. Significant diseases or conditions other than SSc that may influence response to the study product or safety, such as:
a. A new bacterial or viral infection that was treated with oral or intravenous antibiotics or anti-viral treatments within 28 days before Visit 1. This does
not include prophylactic antibiotic or anti-viral treatments, or treatment for gastrointestinal bacterial overgrowth.
b. Acute or chronic hepatitis B or C infection
c. Human immunodeficiency virus (HIV) infection
d. History of active tuberculosis or positive tuberculosis test without a completed course of appropriate treatment or already completed at least 1 month
of ongoing appropriate treatment
e. Evidence of required treatment for cancer (except for treated, localised basal or squamous cell carcinoma of the skin or cervical carcinoma in situ)
within 3 years of Visit 1
7. Any of the following values for laboratory tests at Screening:
a. A positive pregnancy test in WOCBP (also at Visit 1)
b. HaemoglobinRationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
all Health; European Quality of Live RESOLVE-1 was expected to enrol correction to degrees of freedom was
Five-domain questionnaire (EQ-5D- approximately 118 patients in each of applied. The assumption of normality
3L) (22); Patient-Reported Outcomes the three treatment arms, for a total for data was tested using the Shapiro-
Measurement Information System-29 of approximately 354 randomised pa- Wilk W test.
item (PROMIS-29) questionnaire (23); tients. To detect a statistically signifi- Sensitivity analyses on the CRISS score
Medical Outcomes Study Short Form- cant difference in the primary efficacy included Van Elteren’s test with stratifi-
36 (SF-36) (24); Scleroderma Skin Pa- endpoint, ACR CRISS at Week 52, cation factors for region, disease dura-
tient Reported Outcome (SSPRO) (25); 107 evaluable patients per treatment tion, and baseline immunosuppressive
The University of California at Los arm (321 patients total) were required use; imputation of missing data using
Angeles Scleroderma Clinical Trials to complete Week 14. This provided multiple imputation methods following
(UCLA SCTC) Consortium Gastroin- >99% power assuming a 2-sided test Markov Chain Monte Carlo techniques;
testinal Tract symptoms questionnaire at alpha = 0.05 and a common standard analysis using completers only; analy-
(GIT 2.0) (26); 5-Dimension Itch Scale deviation (SD) of 0.41 in both treatment sis after imputing missing ACR CRISS
(5-D Itch Scale) (27); and Digital Ulcer arms for the primary efficacy outcome, using last observation carried forward,
Visual Analogue Scale (28). and a difference in the ACR CRISS where data after study product discon-
These efficacy assessments as de- score between lenabasum and placebo tinuation were considered missing; and
scribed are reflected in the study pro- of 0.33. If the resulting treatment effect analysis using tipping point analyses to
tocol for the US and Europe. For the size was smaller (e.g. 0.20), and/or the better understand the impact of data not
study protocol in Japan, mRSS will resulting SD was larger (e.g. 50.0), the missing at random.
be the primary efficacy endpoint with study would maintain ≥83% powered to The modified intent-to-treat (mITT)
ACR CRISS score as the first second- detect a significant treatment difference population was used for efficacy analy-
ary efficacy endpoint. for lenabasum versus placebo for the ses and included all randomised pa-
primary outcome. With 107 evaluable tients who received at least 1 dose of
Safety assessments patients per treatment arm, the power to study drug and had at least one post-
Treatment-emergent adverse events detect a significant treatment difference baseline efficacy evaluation. The safety
(AEs), physical examination, vi- in the first secondary efficacy measure population comprised all patients who
tal signs, 12-lead electrocardiogram (mRSS) was 99% with a corresponding received at least 1 dose of study drug.
(ECG), clinical laboratory results, treatment difference of -5.0, SD of 7.0.
and concomitant medications were as- For primary and secondary efficacy Discussion
sessed. Plasma concentrations and me- outcomes, the overall type I error rate Historically, measurement of skin
tabolites of lenabasum were measured was controlled with independent hi- thickness with mRSS has been the
and punch biopsies of involved skin erarchical assessments of efficacy at primary endpoint in many SSc clini-
were obtained at Visits 1 and 11. Prior each dose of lenabasum. The order of cal studies, particularly in early dcSSc.
to study completion and before entry tests for treatment effect was change mRSS has been used as a clinical sur-
into the open-label extension study, from baseline for mRSS, HAQ-DI, and rogate marker for disease severity and
approximately 90 study patients in the ppFVC for lenabasum 20 mg twice predictor for disease progression and
U.S. will be consented to participate in daily versus placebo, and ACR CRISS, mortality (32). Prior studies suggested
a withdrawal sub-study to assess poten- mRSS, HAQ-DI, and ppFVC for lena- a possible benefit of immunosuppres-
tial withdrawal effects of lenabasum. basum 5 mg twice daily versus pla- sive strategies including methotrex-
Patients will complete withdrawal- cebo. Statistical significance with each ate (33, 34), cyclophosphamide (35)
related PRO questionnaires on depres- endpoint was required to continue with and mycophenolate mofetil (36) for
sion, including suicidality. They will assessment of the next endpoint. mRSS. In more recent trials in which
be instructed that if they experience The primary and key secondary end- the mRSS was used as the primary end-
feelings of depression or suicidality at points are listed in Table III. Analysis point, treatment of patients with early
any time, they need to seek immediate of the primary and secondary efficacy dcSSc with abatacept, riociquat, and to-
medical attention. As part of the with- endpoints was with a mixed-effect cilizumab (37-39), did not demonstrate
drawal study, additional safety assess- model repeated measures (MMRM) a statistically significant improvement
ments included safety outcomes from model that included region, disease comparing active drug versus placebo.
the Beck Depression Inventory (BDI) duration, baseline immunosuppressive Two trials used ACR CRISS score as
(29); Cannabis Withdrawal Scale use, visit, treatment, and treatment-by- a secondary (abatacept) or exploratory
(CWS) (30); and Addiction Research visit as fixed effects and baseline mRSS (tocilizumab) efficacy outcome (40,
Center Inventory – Marijuana (ARCI- as a covariate. Data were presented as 41). In both trials, ACR CRISS was
M) (31) questionnaire (Table II). mean, SD, and 95% confidence in- able to discriminate active drug from
tervals (CI). An unstructured covari- placebo. These results underscore the
Statistical analysis ance structure shared across treatment potential limitation of selecting mRSS
Sample size calculations were based groups was used to model within-pa- as the primary endpoint, since skin
on results from a Phase 2 study (15). tient errors, and the Kenward-Rogers thickness has a relatively high coef-
S-128 Clinical and Experimental Rheumatology 2021Rationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
Table II. Study assessments and definitions.
Assessment Definition
ACR CRISS Continuous variable score between 0.0 and 1.0 (0 – 100%). A higher score indicates greater improvement.
Patients were not considered improved (ACR CRISS score = 0) if they developed new: 1) renal crisis; 2)
decline in FVC% predicted by 15% (relative) to baseline and confirmed after 1 month; 3) left ventricular fail-
ure (systolic ejection fractionRationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
Table III. Study outcomes. The ACR CRISS score was developed
to assess the likelihood of improve-
Primary efficacy outcome Change from baseline to week 52
ment by providing a multiple domain
ACR CRISS Lenabasum 20 mg BID vs. placebo scoring system that includes assess-
ment of skin changes, pulmonary func-
Secondary efficacy outcomes
ACR CRISS Lenabasum 5 mg BID vs. placebo tion, daily function, and patient and
mRSS Lenabasum 20 mg BID vs. placebo physician global assessments (16). In
Lenabasum 5 mg BID vs. placebo an early dcSSc population where there
HAQ-DI Lenabasum 20 mg BID vs. placebo is mRSS regression and improvement,
Lenabasum 5 mg BID vs. placebo
FVC % predicted Lenabasum 20 mg BID vs. placebo
ACR CRISS score can serve as a trial
Lenabasum 5 mg BID vs. placebo endpoint that measures the likelihood
of overall SSc improvement. In trials
Tertiary efficacy outcomes Change from baseline to week 26 (SENCSIS and RISE-SSc) designed
ACR CRISS
for the prevention of worsening for a
mRSS
HAQ-DI specific disease outcome with inclu-
FVC% predicted sion criteria adapted accordingly, ACR
CRISS would likely not be an appro-
Change from baseline to week 26 and 52 priate trial endpoint (11, 39).
MDGA
PtGA In this Phase 3 study with lenabasum,
SSPRO we wanted to select a primary efficacy
5-D Itch outcome that would reflect clinically
PROMIS-29 meaningful treatment benefit-that is
FACIT-fatigue
EQ-5D
how the patient feels and functions. RE-
UCLA SCTC GIT 2.0 SOLVE-1 is the first Phase 3 study in
Digital ulcer VAS dcSSc where the primary efficacy out-
Responders – mRSS, HAQ-DI, FVC % predicted, MDGA, PtGA come is ACR CRISS. The ACR CRISS
is a composite score consisting of test-
ficient of variation and measures one intra-rater variability, although much ing for major organ decrements fol-
aspect of SSc disease which typically of this variability can be minimised lowed by examination of 5 clinical and
peaks and then regresses early in the by study training certification for skin patient-reported outcomes (PROs) de-
disease. Further, it often improves in assessment and the use of experienced veloped to assess the likelihood of over-
both the placebo and treated groups in investigators (44) as was done for RE- all SSc improvement. RESOLVE-1’s
the context of clinical trials. This can SOLVE-1. study design, utilising ACR CRISS as
result in an unpredictable degree of im- Further, the mRSS captures one clinical the primary endpoint and multiple other
provement in the placebo group (42). feature of SSc and may not adequately SSc specific and non-specific PROs as
Despite implementation of various capture the heterogenous features that secondary endpoints, represents an-
cohort enrichment criteria (shorter dis- can contribute to patient quality of life other important path in prospectively
ease duration, defined range of baseline and function in SSc. It therefore is im- evaluating new pharmacological thera-
mRSS, elevated C-reactive protein, and portant to consider the role and value pies for early dcSSc.
evidence of worsening skin in the pre- of PROs in evaluating clinical burden In a Phase 2 study of lenabasum in
vious 6 months prior to screening) to and treatment benefit to patients in SSc 42 patients with dcSSc, where ACR
increase enrolment of patients with ac- studies (32). SSc has a substantial bur- CRISS was used as the primary out-
tive progressive skin disease, the mean den on the health-related quality of life come, improvement was observed in
changes in mRSS from baseline in one (QoL) of affected patients (45). The the lenabasum group starting at Week
year in the placebo group were -4.4 (to- QoL of SSc patients is substantially 8 and increasing over time. The ACR-
cilizumab) and -4.5 (abatacept). In the lower than that in the general popula- CRISS reached a maximum of 0.33
RISE-SSc trial ofriociguat, enrichment tion (7, 45), is worse than in patients probability of improvement compared
for progressors (worsening) of skin with other rheumatic diseases (46), and to 0.00 at Week 16 in the placebo group.
fibrosis using evidence-based criteria is worse in patients with dcSSc than This was consistent with improvement
(43) was successful, but even then, the in patients with limited cutaneous dis- across multiple physician- and patient-
number of progressors was relatively ease (47). Work disability occurs early reported outcomes that spanned overall
low and the regressors still outweighed in the course of the disease and wors- disease, skin involvement, and patient
the progressors (mean change in mRSS ens with the severity of SSc and the function (15). Through 2 years of the
in placebo from baseline -0.8). An- patient’s functional status (47). Both lenabasum Phase 2 open-label exten-
other limitation of the mRSS, which functional disability and anxiety have sion study, additional analyses showed:
is the component most weighed in the a significant impact on QoL in patients ACR CRISS score positively correlated
ACR CRISS score, includes inter- and with SSc (48). with improvements in multiple PROs;
S-130 Clinical and Experimental Rheumatology 2021Rationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
ACR CRISS score correlates more be made to allow background therapy • The use of broad patient selection
strongly with these PROs than change in clinical trials in early dcSSc recog- criteria was designed to reflect the
in mRSS; and improvement in the two nising how devastating the disease can real-world population of patients
PROs [Health Assessment Question- be with the potential for incurring irre- with SSc, including allowance of
naire-Disability Index (HAQ-DI) and versible skin or organ damage which is background therapy with immuno-
Patient Global Assessment (PtGA)] generally most progressive in that early suppressives.
included in the composite ACR CRISS phase (50, 51). Although there are no
score themselves correlate with mul- proven “disease modifying” therapies Acknowledgement
tiple other PROs [Scleroderma Skin for dcSSc or clear definitions as to what The authors would like to acknowl-
Patient Reported Outcome (SSPRO) would constitute disease modifica- edge the editorial assistance of Richard
and Patient-Reported Outcomes Meas- tion, most clinicians and patients opt Perry, PharmD in the preparation of
urement Information System-29 item for therapy in early disease in clinical this manuscript, which was supported
(PROMIS-29) questionnaire] (49). To- practice. Unlike several of the recent by Corbus Pharmaceuticals, Norwood,
gether, these data show that the ACR aforementioned studies, we allowed MA, USA.
CRISS score broadly reflects changes background immunosuppressive thera-
from baseline in how patients feel and py at the risk of blunting a more sub- Affiliations
function in this patient population. In tle treatment effect of lenabasum that 1
Weill Cornell Medical College, New
addition, Step 1 captures survival or dis- might have been seen in a study that did York City, NY, USA;
ease features associated with survival as not allow background immunosuppres- 2
University of Michigan Scleroderma
it assesses clinically meaningful cardio- sives. With this design, we hope to find Program, Ann Arbor, MI, USA;
pulmonary-renal involvement. Since a meaningful incremental advance in 3
Dept. of Allergy and Rheumatol-
the completion of the lenabasum Phase the pharmacological therapy of dcSSc, ogy, Nippon Medical School Graduate
2 randomised, double-blind, placebo- rather than merely demonstrating a School of Medicine, Tokyo, Japan;
controlled trial, ACR CRISS was se- drug-placebo difference in efficacy. By 4
Dept. of Rheumatology, University of
lected as a primary outcome for a num- choosing a 52-week study that allowed California in Los Angeles, CA, USA;
ber of currently active Phase 2 dcSSc background therapy, we also avoided 5
University of Utah and Salt Lake City
clinical trials: MT-7117 (dersimelargon; the ethical dilemma of including a pla- VA Health Care System Salt Lake City,
ClinicalTrials.gov: NCT04440592), cebo-controlled arm for a long-duration UT, USA;
KD025 (belumosudil; ClinicalTrials. study (50). 6
Division of Rheumatology, Johns
gov: NCT03919799), IgPro10 (IVIG; In conclusion, RESOLVE-1 is the first Hopkins University School of Medi-
ClinicalTrials.gov: NCT04137224) and Phase 3 interventional study to date in cine, Baltimore, MD, USA;
belimumab / rituximab (ClinicalTrials. dcSSc to prospectively use the ACR 7
Dept. of Rheumatology, St. Vincent’s
gov: NCT03844061). CRISS as the primary efficacy out- Hospital, Melbourne, Victoria, Australia;
One unique feature of RESOLVE-1 come. The study design incorporated 8
Dept. of Experimental Rheumatology,
was the inclusive eligibility criteria. some unique features including ACR University of Florence and Division of
It allowed background treatment in- CRISS as the primary endpoint, broad Rheumatology AOUC, Florence, Italy;
cluding immunosuppressives and low eligibility criteria, and concomitant 9
Division of Rheumatology, Jewish
dose corticosteroids and even allowed use of stable background immuno- General Hospital, Montreal, Canada;
changes in immunosuppressive dos- suppressive therapy. These features 10
Dept. of Rheumatology, University
ing if needed; this facilitated timely, facilitate rapid recruitment of a large Hospital Zurich, Switzerland;
full enrolment into the study. Conse- placebo-controlled study in 1.5 years. 11
Corbus Pharmaceuticals, Inc. Nor-
quently, the study population would be RESOLVE-1 may provide a template wood, MA, USA;
expected to be more representative of for the design of future Phase 3 dcSSc 12
UCL Centre for Rheumatology and
SSc patients who are managed in clini- studies to demonstrate meaningful im- Connective Tissue Diseases, Royal Free
cal practice. In patients with dcSSc, provement in overall disease activity. Campus, University College London,
this study is evaluating improvement in United Kingdom.
overall disease burden, rather than ef- Take home messages
fects on a single domain of the disease, • An unmet need still exists for phar- Competing interests
which may provide valuable informa- macological therapy of SSc which R. Spiera has received consulting
tion on health outcomes as well as the demonstrates overall clinical benefit fees from Abbvie, Roche-Genentech,
efficacy and tolerability of lenabasum. (i.e. how the patient feels and func- GSK, Sanofi, Janssen, Chemocen-
This study design was chosen to dem- tions). tryx, Formation Biologics; he has re-
onstrate that a new pharmacologic ther- • RESOLVE-1 is the first Phase 3 ceived grants/research support from
apy for dcSSc has incremental benefit study in diffuse cutaneous SSc to Roche-Genentech, GSK, Boehringer
over and beyond what is achieved with prospectively use the ACR CRISS as Ingelheim, Chemocentryx, Corbus,
the traditionally used immunosuppres- the primary efficacy outcome assess- Formation Biologics, Inflarx, Kadmon
sive strategies. A strong argument can ment. and Astra Zeneca. D. Khanna reports
Clinical and Experimental Rheumatology 2021 S-131Rationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
consultancies from Actelion, Bayer, He has received speaker fees on sclero- terstitial lung disease. N Engl J Med 2019;
380: 2518-28.
BMS, Corbus, Genentech, Boehringer, derma and related complications from
12. IUDICI M, BAFETA A, ATAL I, RAVAUD P:
Horizon, Theraly, Talaris, Promethius; Bayer, Boehringer Ingelheim, Med- Ten years of interventional research in sys-
grants from Horizon, BMS, Bayer, scape, Novartis, Roche. In addition, he temic sclerosis: A systematic mapping of
Pfizer; stock ownership in Eicos Sci- has a patent mir-29 for the treatment of trial registries. Arthritis Care Res 2020; 72:
140-8.
ences Inc. M. Kuwana reports personal systemic sclerosis issued (US8247389, 13. DENTON CP: Challenges in systemic sclero-
fees from Corbus Pharmaceuticals dur- EP2331143). N. Dgetluck, B. Bloom, sis trial design. Semin Arthritis Rheum 2019;
ing the conduct of the study; grants and Q. Dinh, and B. White are employ- 49: S3-7.
personal fees from Boehringer Ingel- ees of and may own stock in Corbus 14. DENTON CP, YEE P, ONG VH: News and fail-
ures from recent treatment trials in systemic
heim and Ono Pharmaceuticals; per- Pharmaceuticals. C.P. Denton has had sclerosis. Eur J Rheumatol 2020.
sonal fees from AbbVie, Actelion Phar- consultancies from Corbus Pharmaceu- 15. SPIERA R, HUMMERS L, CHUNG L et al.:
maceuticals, Astellas, Bayer, Chugai, ticals, GSK, Galapagos, Boehringer In- Safety and efficacy of lenabasum in a phase
CSL Behring, Galapagos NV, Glaxo- gelheim, CSL Behring, Acceleron and 2 randomized, placebo-controlled trial in
adults with systemic sclerosis. Arthritis
SmithKline, MBL, Mochida, Reata Arxx Therapeutics. Rheumatol 2020; 72: 1350-60.
Pharmaceuticals, and Kissei. D.E. Furst The other co-authors have declared no 16. KHANNA D, BERROCAL VJ, GIANNINI EH et
has received grant/research support competing interests. al.: The American College of Rheumatology
from Actelion, Amgen, BMS, Corbus, provisional composite response index for clin-
ical trials in early diffuse cutaneous systemic
Galapagos, GSK, NIH, Novartis, Pfiz- References sclerosis. Arthritis Rheum 2016; 68: 299-311.
er, Sanofi, Roche-Genentech. Consul- 1. DENTON CP, KHANNA D: Systemic sclerosis. 17. van den HOOGEN F, KHANNA D, FRANSEN J
Lancet 2017; 390: 1685-99.
tancies from Actelion, Amgen, BMS, 2. KATSUMOTO TR, WHITFIELD ML, CONNOL-
et al.: 2013 classification criteria for systemic
sclerosis: an American College of Rheuma-
Corbus, Galapagos, Novartis, Pfizer. LY MK: The pathogenesis of systemic sclero- tology/European League Against Rheuma-
Speakers Bureau: CME only. L. Hum- sis. Annu Rev Pathol 2011; 6: 509-37. tism collaborative initiative. Arthritis Rheum
mers reports grants from Corbus Phar- 3. ROYLE JG, LANYON PC, GRAINGE MJ, 2013; 65: 2737-47.
ABHISHEK A, PEARCE FA: The incidence,
maceuticals during the conduct of the prevalence, and survival of systemic sclero-
18. KHANNA D, FURST DE, CLEMENTS PJ et al.:
Standardization of the modified Rodnan skin
study; grants from Cytori Therapeutics, sis in the UK Clinical Practice Research Da- score for use in clinical trials of systemic
Inc, Boehringer-Ingelheim, Cumber- talink. Clin Rheumatol 2018; 37: 2103-11. sclerosis. J Scleroderma Relat Disord 2017;
land Pharmaceuticals, Sanofi Aventis, 4. VARGA J, TROJANOWSKA M, MASATAKA 2: 11-8.
KUWANA M: Pathogenesis of systemic scle- 19. COLE JC, KHANNA D, CLEMENTS PJ et al.:
and Glaxo-Smith-Kline; she was site rosis: recent insights of molecular and cel- Single-factor scoring validation for the
PI for this clinical trial and the Uni- lular mechanisms and therapeutic opportu- Health Assessment Questionnaire-Disability
versity received support for this study. nities. J Scleroderma Relat Disord 2017; 2: Index (HAQ-DI) in patients with systemic
137-52.
W. Stevens reports clinical trial fund- sclerosis and comparison with early rheuma-
5. SIERRA-SEPÚLVEDA A, ESQUINCA-GONZÁ- toid arthritis patients. Qual Life Res 2006;
ing from Corbus Pharmaceuticals dur- LEZ A, BENAVIDES-SUÁREZ SA et al.: 15: 1383-94.
ing the conduct of the study; and per- Systemic sclerosis pathogenesis and emerg- 20. HANKINSON JL, KAWUT SM, SHAHAR E,
sonal fees from Janssen, Actelion, and ing therapies, beyond the fibroblast. Biomed SMITH LJ, STUKOVSKY KH, BARR RG: Per-
Res Int 2019; 2019: 4569826.
Boehringer Ingelheim, outside of the formance of American Thoracic Society-
6. ZHOU Z, FAN Y, TANG W et al.: Economic recommended spirometry reference values
submitted work. M. Matucci-Cerinic burden among commercially insured patients in a multiethnic sample of adults: the multi-
has received consulting fees or hono- with systemic sclerosis in the United States. ethnic study of atherosclerosis (MESA) lung
rarium from Actelion, Janssen, Inven- J Rheumatol 2019; 46: 920-7. study. Chest 2010; 137: 138-45.
7. MORRISROE K, HUDSON M, BARON M et al.:
tiva, Bayer, Boehringer, CSL Behring, International Systemic Sclerosis Inception
21. BUTT Z, LAI J-S, RAO D, HEINEMANN AE,
BILL A, CELLA D: Measurement of fatigue in
Corbus, Galapagos, Mitsubishi, Sam- Cohort (INSYNC) collaboration. Determi- cancer, stroke, and HIV using the Functional
sung, Regeneron, Acceleron, MSD, nants of health-related quality of life in a Assessment of Chronic Illness Therapy –
Chemomab, Lilly, Pfizer, Roche. M. multinational systemic sclerosis inception Fatigue (FACIT-F) scale. J Psychosom Res
cohort. Clin Exp Rheumatol 2018; 36 (Suppl. 2013; 74: 64-8.
Baron has received funding from Cor- 113): S53-60. 22. GUALTIEROTTI R, INGEGNOLI F, SCALONE
bus Pharmaceuticals as an investigator. 8. IWAMOTO N, DISTLER O: Molecular targets L et al.: Feasibility, acceptability and con-
O. Distler has/had consultancy rela- for therapy in systemic sclerosis. Fibrogen- struct validity of EQ-5D in systemic sclero-
tionship and/or has received research esis Tissue Repair 2012; 5 (Suppl. 1): S19. sis. Swiss Med Wkly 2016; 146: w14394.
9. KHANNA D, TASHKIN DP, DENTON CP, LU- 23. KHANNA D, KRISHNAN E, DEWITT EM,
funding from Abbvie, Acceleron Phar- BELL MW, VAZQUEZ-MATEO C, WAX S: On- KHANNA PP, SPIEGEL B, HAYS RD: The
ma, Aleimed, Amgen, AnaMar, Arxx, going clinical trials and treatment options for future of measuring patient-reported out-
Baecon, Blade, Bayer, Boehringer In- patients with systemic sclerosis-associated comes in rheumatology: Patient-Reported
gelheim, ChemomAb, Corbus, CSL interstitial lung disease. Rheumatology 2019; Outcomes Measurement Information Sys-
58: 567-79. tem (PROMIS). Arthritis Care Res 2011; 63
Behring, Galapagos, Glenmark, GSK, 10. WOLLIN L, DISTLER JH, DENTON CP, (Suppl. 11): S486-90.
Horizon (Curzion) Pharmaceuticals, In- GAHLEMANN M: Rationale for the evalua- 24. HINCHCLIFF ME, BEAUMONT JL, CARNS
ventiva, iQvia, Kymera, Lupin, Medac, tion of nintedanib as a treatment for systemic MA et al.: Longitudinal evaluation of
Medscape, Mitsubishi Tanabe Pharma, sclerosis-associated interstitial lung disease. PROMIS-29 and FACIT-dyspnea short forms
J Scleroderma Relat Disord 2019. in systemic sclerosis. J Rheumatol 2015; 42:
MSD, Roche, Roivant, Topadur and 11. DISTLER O, HIGHLAND KB, GAHLEMANN 64-72.
UBC in the area of potential treatments M et al.: SENSCIS Trial Investigators. Nin- 25. MAN A, CORREA JK, ZIEMEK J, SIMMS RW,
of scleroderma and its complications. tedanib for systemic sclerosis-associated in- FELSON DT, LAFYATIS R: Development and
S-132 Clinical and Experimental Rheumatology 2021Rationale for phase 3 study of lenabasum in systemic sclerosis / R. Spiera et al.
validation of a patient-reported outcome 35. TASHKIN DP, ELASHOFF R, CLEMENTS PJ 2020; 20: 1-8.
instrument for skin involvement in patients et al.: Cyclophosphamide versus placebo in 43. DOBROTA R, MAURER B, GRAF N et al.:
with systemic sclerosis. Ann Rheum Dis scleroderma lung disease. N Engl J Med 2006; Prediction of improvement in skin fibrosis in
2017; 76: 1374-80. 354: 2655-66. diffuse cutaneous systemic sclerosis: a EU-
26. KHANNA D, HAYS RD, MARANIAN P et al.: 36. TASHKIN DP, ROTH MD, CLEMENTS PJ et STAR analysis. Ann Rheum Dis 2016; 75:
Reliability and validity of UCLA Scleroder- al.: Mycophenolate mofetil versus oral cy- 1743-8.
ma Clinical Trial Consortium Gastrointesti- clophosphamide in scleroderma-related in- 44. KHANNA D, FURST DE, CLEMENTS PJ et al.:
nal Tract (UCLA SCTC GIT 2.0) Instrument. terstitial lung disease (SLS II): a randomised Standardization of the modified Rodnan skin
Arthritis Rheum 2009; 61: 1257-63. controlled, double-blind, parallel group trial. score for use in clinical trials of systemic
27. ELMAN S, HYNAN LS, GABRIEL V, MAYO MJ: Lancet Respir Med 2016; 4: 708-19. sclerosis. J Scleroderma Relat Disord 2017;
The 5-D itch scale: a new measure of pruri- 37. KHANNA D, LIN CJF, KUWANA M et al.: 2: 11-18.
tus. Br J Dermatol 2010; 162: 587-93. Efficacy and safety of tocilizumab for the 45. FISCHER A, ZIMOVETZ E, LING C, ESSER D,
28. STEEN, VD, MEDSGER TA: The value of the treatment of systemic sclerosis: Results from SCHOOF N: Humanistic and cost burden of
health assessment questionnaire and spe- a Phase 3 randomized controlled trial. Lancet systemic sclerosis: A review of the literature.
cial patient-generated scales to demonstrate Respir Med 2020 in press. Autoimmun Rev 2017; 16: 1147-54.
change in systemic sclerosis patients over 38. KHANNA D, SPINO C, JOHNSON S et al.: 46. PARK EH, STRAND V, OH YJ, SONG YW, LEE
time. Arthritis Rheum 1997; 40: 1984-91. Abatacept in early diffuse cutaneous system- EB: Health-related quality of life in systemic
29. BECK AT, WARD CH, MENDELSON M, MOCK ic sclerosis: Results of a Phase II investiga- sclerosis compared with other rheumatic dis-
J, ERBAUGH J: An inventory for measuring tor-initiated, multicenter, double-blind, ran- eases: a cross-sectional study. Arthritis Res
depression. Arch Gen Psychiatry 1961; 4: domized, placebo-controlled trial. Arthritis Ther 2019; 21: 61.
561-71. Rheum 2020; 72: 125-36. 47. FRANTZ C, AVOUAC J, DISTLER O et al.:
30. ALLSOP DJ, NORBERG MM, COPELAND J, 39. KHANNA D, ALLANORE Y, DENTON CP et al.: Impaired quality of life in systemic sclerosis
FU S, BUDNEY AJ: The Cannabis Withdrawal Riociguat in patients with early diffuse cu- and patient perception of the disease: A large
Scale development: Patterns and predictors taneous systemic sclerosis (RISE-SSc): ran- international survey. Semin Arthritis Rheum
of cannabis withdrawal and distress. Drug domised, double-blind, placebo-controlled 2016; 46: 115-23.
Alcohol Depend 2011; 119: 123-9. multicentre trial. Ann Rheum Dis 2020; 79: 48. SIERAKOWSKA M, DOROSZKIEWICZ H,
31. HUESTIS MA, BOYD SJ, HEISHMAN SJ et al.: 618-25. SIERAKOWSKA J et al.: Factors associated
Single and multiple doses of rimonabant an- 40. KHANNA D, SPINO C, BUSH E et al.: Abata- with quality of life in systemic sclerosis: a
tagonize acute effects of smoked cannabis in cept vs. placebo in early diffuse cutaneous cross-sectional study. Qual Life Res 2019; 28:
male cannabis users. Psychopharmacology systemic sclerosis – results of a Phase 2 in- 3347-54.
2007; 194: 505-15. vestigator initiated, double-blind, placebo- 49. SPIERA R, HUMMERS L, CHUNG L et al.:
32. PAULING JD, CAETANO J, CAMPOCHIARO C controlled, multicenter, randomized con- Provisional American College of Rheumatol-
et al.: Patient-reported outcome instruments trolled trial study [abstract]. Arthritis Rheum ogy (ACR) Combined Response Index in Dif-
in clinical trials of systemic sclerosis. J Scle- 2018; 70 (Suppl. 10). fuse Cutaneous Systemic Sclerosis (CRISS)
roderma Relat Disord 2020; 5: 90-102. 41. KHANNA D, LIN CJF, SPOTSWOOD H et al.: Score correlates with changes (Δ) in patient-
33. POPE JE, BELLAMY N, SEIBOLD JR et al.: Evaluation of American College of Rheu- reported outcomes (PROs). J Scleroderma
A randomized, controlled trial of methotrex- matology Provisional Composite Response Relat Disord 2020; 5: 16.
ate versus placebo in early diffuse scleroder- Index in Systemic Sclerosis (ACR CRISS) 50. KHANNA D, FURST DE, ALLANORE Y et al.:
ma. Arthritis Rheum 2001; 44: 1351-8. in a Phase 3 randomized controlled trial [ab- Twenty-two points to consider for clinical
34. van den HOOGEN FH, BOERBOOMS AM, stract]. Arthritis Rheum 2018; 70 (Suppl. 10). trials in systemic sclerosis, based on EULAR
SWAAK AJ et al.: Comparison of methotrex- 42. KUWANA M, HASEGAWA M, FUKUE R et al.: standards. Rheumatology 2015; 54: 144-51.
ate with placebo in the treatment of systemic Initial predictors of skin thickness progres- 51. BARSOTTI S, ORLANDI M, CODULLO V et
sclerosis: a 24-week randomized double- sion in patients with diffuse cutaneous sys- al.: One year in review 2019: systemic scle-
blind trial, followed by a 24-week observa- temic sclerosis: Results from a multicentre rosis. Clin Exp Rheumatol 2019; 37 (Suppl.
tional trial. Br J Rheumatol 1996; 35: 364-72. prospective cohort in Japan. Mod Rheumatol 119): S3-14.
Clinical and Experimental Rheumatology 2021 S-133You can also read