Retinal Vascular Changes in Pre-Diabetes and Prehypertension
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Reviews/Commentaries/ADA Statements
R E V I E W A R T I C L E
Retinal Vascular Changes in Pre-Diabetes
and Prehypertension
New findings and their research and clinical implications
THANH TAN NGUYEN, MBBS1 therapy may also reduce retinopathy re-
JIE JIN WANG, MMED, PHD1,2 quiring laser treatment (7).
TIEN YIN WONG, MD, PHD1,3
Hypertensive retinopathy
Like diabetic retinopathy, classic hyper-
CLASSIC RETINAL
T
he retinal vasculature can be tensive retinopathy is well characterized.
viewed directly and noninvasively, VASCULAR CHANGES The clinical signs include generalized and
offering a unique and easily acces- focal arteriolar narrowing, arterio-venous
sible “window” to study the health and Diabetic retinopathy nicking, increased retinal arteriolar light
disease of the human microcirculation In individuals with diabetes, the classic reflex (copper or silver wiring), flame-
in vivo. In the last decade, advances in primary retinal vascular complication— and blot-shaped retinal hemorrhages,
digital retinal photography and imaging diabetic retinopathy—is well described cotton wool spots, and, in severe cases,
techniques have allowed precise charac- (1). Diabetic retinopathy signs are optic disc swelling (8,9). The association
terization of subtle retinal vascular broadly divided into nonproliferative and of these retinal signs with blood pressure
changes in large populations. These ret- proliferative retinopathy. The prevalence is consistent and seen in both adults (10 –
inal changes can be broadly divided into of diabetic retinopathy increases with 20) and children (21), even in individuals
four groups: 1) classic retinal vascular duration of diabetes. The Australian Dia- without clinical hypertension (13–15,
changes in diabetes and hypertension betes, Obesity and Lifestyle Study (Aus- 22–24).
(i.e., diabetic and hypertensive retinop- Diab) showed that the prevalence of
athy), 2) isolated retinopathy signs in diabetic retinopathy is less than 10% in ADVANCES IN ASSESSING
individuals with diabetes or hyperten- those with diabetes duration of less than 5 RETINAL VASCULAR
sion (e.g., microaneurysm, retinal hem- years but more than 50% in those with 20 CHANGES — Digital retinal photog-
orrhage, or cotton wool spot), 3) years or longer diabetes (2). The two ma- raphy and new imaging technology have
changes in retinal vascular caliber, and jor risk factors of diabetic retinopathy are now allowed more precise assessment of
4) changes in retinal vascular architec- hyperglycemia and hypertension, with the subtle changes seen in the retinal
ture (e.g., retinal tortuosity). hyperlipidemia as a possible third major microvasculature (22,25–28). One key
New studies in large populations now risk factor. The importance of hypergly- development has been methods to objec-
show that retinal vascular changes are cemia has been confirmed in epidemio- tively quantify retinal vascular caliber.
common in the general population and logical studies (3), as well as two pivotal Historically, narrowed retinal arteriolar
may precede the subsequent develop- clinical trials: the DCCT (Diabetes Con- caliber, an early hypertensive retinopathy
ment of overt diabetes and hypertension. A trol and Complications Trial) in patients sign, has been difficult to measure using
consistent pattern of associations is also with type 1 diabetes (4) and the UKPDS the clinical ophthalmoscope (29). Parr,
Hubbard, and colleagues (22,30,31) de-
emerging, showing that specific retinal vas- (UK Prospective Diabetes Study) in pa-
veloped techniques to measure retinal
cular changes may be related differently to tients with type 2 diabetes (5). The UK-
vascular caliber from photographs and
hyperglycemia and blood pressure. PDS also showed that blood pressure summarized these as the arterio-venous
In this review, we summarize recent control reduces the risk of retinopathy in- ratio (AVR). These techniques are now
studies on the retinal vascular changes dependent of glycemia levels (6). New used in large epidemiological studies
seen in diabetes and hypertension and data from the FIELD (Fenofibrate Inter- (20,22,25,27,28) and have substantial re-
speculate on potential research and clini- vention and Event Lowering in Diabetes) producibility.
cal implications. Study now suggest that lipid-lowering Recent studies suggest the interpreta-
tion of the AVR may be overly simplistic.
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● A smaller AVR was thought to reflect gen-
From the 1Centre for Eye Research Australia, University of Melbourne, Victoria, Australia; the 2Centre for eralized retinal arteriolar narrowing, since
Vision Research, University of Sydney, New South Wales, Australia; and the 3Singapore Eye Research venular caliber was assumed to be rela-
Institute, National University of Singapore, Singapore.
Address correspondence and reprint requests to Tien Yin Wong, MD, PhD, Centre for Eye Research
tively constant (22). Thus, when a low
Australia, University of Melbourne, 32 Gisborne St., Victoria 3002, Australia. E-mail: twong@ AVR was associated with elevated blood
unimelb.edu.au. pressure (18,32) and cardiovascular out-
Received for publication 15 April 2007 and accepted in revised form 20 June 2007. comes such as stroke (33,34) and coro-
Published ahead of print at http://care.diabetesjournals.org on 26 June 2007. DOI: 10.2337/dc07-0732. nary heart disease (35), the associations
Abbreviations: ARIC, Atherosclerosis Risk In Communities; AVR, arterio-venous ratio.
A table elsewhere in this issue shows conventional and Système International (SI) units and conversion were initially thought to reflect general-
factors for many substances. ized arteriolar narrowing. Newer analy-
© 2007 by the American Diabetes Association. ses, however, suggest a smaller AVR may
2708 DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007Nguyen, Wang, and Wong
not only reflect narrower arterioles but
also wider venules (36,37). Furthermore,
arteriolar and venular calibers appear to
reflect different pathophysiological pro-
cesses (37,38).
Liew et al. (38,39) have suggested the
need to control for venular caliber in sta-
tistical models of arteriolar caliber, and
vice versa, as venular caliber explains
⬃30% of the variability in arteriolar cali-
ber (38)—presumably from shared ge-
netic and ocular factors (22).
Improvements in imaging software
have also led to quantification of other
architectural changes in the retinal vascu-
lar network (36,37), as well as “batch pro-
cessing” of retinal images (20,22,
25,27,28). There remain technical chal-
lenges. For example, the impact of mag-
nification error (i.e., eyes of different re-
fraction) requires further study (40).
ISOLATED RETINOPATHY
SIGNS
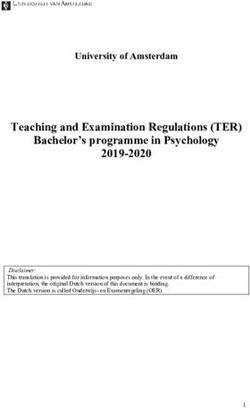
Figure 1—Prevalence of retinopathy in nondiabetic populations (A) and nondiabetic and non-
Epidemiology hypertensive populations (B). AusDiab: Australian Diabetes, Obesity and Lifestyle Study (year
There is increasing evidence that typical began: 1999 –2000, n ⫽ 2,177, aged ⱖ25 years) (2); ARIC (year began: 1987–1990, n ⫽ 10,954,
lesions of diabetic retinopathy (microan- aged 48 –73 years) (22); BDES: Beaver Dam Eye Study (year began: 1988 –1990, n ⫽ 4,926, aged
eurysms, hemorrhages, and cotton wool 43– 84 years) (15); BMES: Blue Mountain Eye Study (year began: 1992–1994, n ⫽ 3,654, aged
spots), termed isolated retinopathy signs, 49 –97 years) (13); CHS: Cardiovascular Health Study (year began: 1989 –1990, n ⫽ 2,050, aged
are now recognized to be more common 67–97 years) (14), Hoorn (year began: 1989 –1992, n ⫽ 626, aged 50 –74 years) (23), Rotterdam
than previously thought in people with- (year began: 1990 –1993, n ⫽ 6,191, aged 55–99 years) (44), and Funagata (year began: 2000 –
out diabetes and hypertension (41– 43). 2002, n ⫽ 1,481, aged ⱖ35 years) (24).
Recent studies using retinal photography
to document these signs suggest preva- Risk factors and pathophysiology isolated retinopathy in people without di-
lence rates in the general population of The underlying risk factors and patho- abetes (50) supports the hypothesis that
5–10% (2,13–15,22–24,44) (Fig. 1A) physiology of isolated retinopathy signs inflammatory processes may also be a
and 2.6 – 8.6% among those without dia- in nondiabetic and normotensive individ- possible pathway that underlies early sub-
betes or hypertension (13–15,22–24) uals are poorly understood. Associations clinical microvascular disease in the pre-
(Fig. 1B). Prospective study data have fur- of these retinopathy signs with increasing diabetes or prehypertension state.
ther shown that up to 10% of individuals age (15,45), elevated blood pressure
aged ⱖ40 years without diabetes may de- (8,13–15,44,47– 49), and hyperglycemia Associations with risk of diabetes,
velop these isolated retinopathy signs (24,44,47,48) have been found. Other hypertension, and cardiovascular
within 5 years (16,45). possible risk factors include hyperlipid- diseases
Two studies have reported on the emia (17,23,48), higher BMI (23,24), and A clinically relevant question is whether
prevalence of retinopathy in individuals systemic inflammation (48,50). We can signs of isolated retinopathy in individu-
with pre-diabetes. In the AusDiab Study, speculate that isolated retinopathy signs als without diabetes are markers of the
retinopathy signs were seen in 6.7% of in normotensive and nondiabetic individ- future risk of diabetes (i.e., do these pa-
individuals with impaired glucose toler- uals may represent early microvascular tients require monitoring for the develop-
ance or impaired fasting glucose (46), damage from a combination of risk fac- ment of diabetes). The evidence here is
whereas in the Diabetes Prevention Pro- tors, including blood pressure and abnor- not consistent. While previous studies
gram this was seen in 7.9% of individuals mal glucose metabolism, which may suggest that detectable retinopathy pre-
with impaired fasting glucose (5.3– 6.9 reflect an underlying process of develop- cedes the onset of type 2 diabetes by 4 –7
mmol/l) or impaired glucose tolerance, ing clinical diabetes or hypertension. years (54), new prospective data from the
who had no history of diabetes (47). Animal models and human studies Blue Mountains (45,55), the Atheroscle-
These isolated retinopathy signs may suggest that chronic inflammation and rosis Risk In Communities (ARIC) (56),
be transient. Population studies show that glucose-induced arteriolar endothelial and Beaver Dam (57) studies reported no
between 40 and 70% of these isolated ret- dysfunction are related to development of increased risk of diabetes in nondiabetic
inopathy signs seen at baseline are not classic diabetic retinopathy (51–53). The individuals with signs of retinopathy.
present 3–5 years later (45,48). association of inflammation and signs of However, there are two notable excep-
DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007 2709Retinal vascular changes
Table 1—Associations of retinal vascular changes with diabetes, hypertension, and cardiovascular diseases
Retinal vascular signs Associations Populations References
Retinopathy Impaired fasting glucose ARIC (67)
Obesity Hoorn (23)
Blood pressure ARIC, AusDiab, BDES, BMES, CHS, (2,13–15,22–24,44)
Funagata, Hoorn, Rotterdam
Incident hypertension BDES (57)
Incident diabetes ARIC, BDES (56,57)
Heart disease BDES, CHS, ARIC (14,59,114)
Nephropathy ARIC, CHS (60,61)
Cerebrovascular disease ARIC, CHS, BDES (14,33,34,114–117)
Retinal arteriolar narrowing Blood pressure Funagata, BDES, BMES, Rotterdam, (10,22,24,32,37,87)
ARIC, CHS
Blood pressure in children SCES, SCORM (21)
Measures of atherosclerosis Rotterdam (37)
Waist-to-hip ratio ARIC (67)
Incident hypertension ARIC, BMES, BDES, Rotterdam (58,88–90)
Incident diabetes ARIC, BDES (64,65)
Coronary heart disease CHS (98)
Retinal venular dilatation Impaired fasting glucose ARIC, MESA (20,67)
Measures of atherosclerosis Rotterdam (37)
Obesity in children SCORM (69)
Waist-to-hip ratio ARIC (67)
Hypertriglyceridemia ARIC (67)
Incident obesity BMES (118)
Incident hypertension BMES (39)
Incident impaired fasting glucose Rotterdam (66)
Cerebrovascular diseases Rotterdam, CHS (96–98)
Carotid artery disease Rotterdam (37)
AusDiab, Australian Diabetes, Obesity and Lifestyle Study; BDES, Beaver Dam Eye Study; BMES, Blue Mountain Eye Study; CHS, Cardiovascular Health Study;
MESA, Multi-Ethnic Study of Atherosclerosis; SCES, Sydney Childhood Eye Study; SCORM, Singapore Cohort Study of Risk Factors for Myopia.
tions. First, in the Beaver Dam Study, that isolated microaneurysms, hemor- sion and prehypertension, are sum-
among individuals aged ⬍65 years at rhages, and cotton wool spots predict the marized in Table 1.
baseline, signs of retinopathy were asso- development of clinical cardiovascular
ciated with an increased 15-year inci- and cerebrovascular events independent Associations with diabetes and pre-
dence of diabetes (odds ratio [OR] 3.68 of traditional risk factors (Table 1). Vari- diabetes
[95% CI 1.23–10.96]) (57). Second, in ous population-based studies have shown Consistent associations of retinal venular
the ARIC Study, among participants with associations of isolated signs of retinopa- caliber with hyperglycemia, diabetes, and
a family history of diabetes, signs of reti- thy with the risk of stroke (33), congestive its complications are now emerging (20).
nopathy were also associated with an in- heart failure (59), renal dysfunction Prospective data from three population-
creased 3-year risk of diabetes (2.3 [1.0 – (60,61), and measures of atherosclerosis based cohorts have shown that changes in
5.3]) (56). Thus, the literature suggests (14,62,63). In the ARIC Study, the pres- retinal vascular caliber may predict the
that isolated signs of retinopathy in indi- ence of retinopathy was associated with a development of type 2 diabetes (64,65)
viduals without diabetes are not necessar- threefold higher risk of congestive heart and impaired fasting glucose (66). In two
ily markers of future diabetes risk, except failure in those without previous coro- early analyses, an association between
possibly in younger individuals and in nary heart disease (relative risk 2.98 [95% smaller retinal AVR and incident diabetes
those with a family history of diabetes. CI 1.50 –5.92]) (59). This later associa- was found in the ARIC Study (OR 1.71
Similarly, there is conflicting evi- tion suggests that microvascular disease [95% CI 1.13–2.57]; comparing smallest
dence that isolated signs of retinopathy may be important in the development of to largest AVR quintile) and the Beaver
are markers of future hypertension risk. diabetic cardiomyopathy in the absence Dam Study (1.53 [1.03–2.27]; comparing
Data from the Beaver Dam Study showed of established coronary artery disease. smallest to largest AVR quartile) (64,65).
that among nonhypertensive individuals, Subsequently, the Rotterdam Study dem-
those with signs of retinopathy had a onstrated that these associations reflected
higher incidence of hypertension (OR RETINAL VASCULAR wider retinal venular caliber rather than
1.48 [95% CI 1.05–2.07]) (57), but these CALIBER — The associations and clin- narrower arteriolar caliber (1.23 [1.02–
findings are not supported by other stud- ical significance of early retinal vascular 1.47]; per SD increase in venular caliber)
ies (15,45,58). caliber changes in individuals with diabe- (66). Reanalysis of the ARIC and Beaver
There is now substantial evidence tes and pre-diabetes, as well as hyperten- Dam studies confirms this finding
2710 DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007Nguyen, Wang, and Wong
(T.Y.W., unpublished data). Thus, it ap- ber, there is now substantial evidence that Associations with cardiovascular
pears that wider retinal venular caliber is a hypertension preferentially affects retinal diseases
marker of chronic hyperglycemia and the arteriolar caliber (83) (Table 1). It has In addition to their associations with dia-
pre-diabetes state and reflects the early long been known that generalized retinal betes and hypertension, changes in retinal
microvascular changes that occur in the arteriolar narrowing is an early character- vascular caliber have also been linked to a
development of diabetes. istic sign of hypertensive retinopathy range of cardiovascular diseases (Table 1).
Wider retinal venular caliber has also (8,84,85). More recent studies using Wider retinal venular caliber has been as-
been linked to the metabolic syndrome quantitative measurements of retinal vas- sociated with carotid artery disease (37),
and its components (20,37,67). In the cular caliber have now demonstrated a magnetic resonance imaging– detected la-
Blue Mountains Study, wider retinal graded association of narrowed retinal ar- cunar infarcts and white matter lesions
venular caliber was associated with the terioles with increasing blood pressure in (96), and clinical stroke events (97,98). In
5-year incidence of obesity among indi- different populations of various racial/ the Cardiovascular Health Study, wider
viduals of normal weight at baseline (OR ethnic groups and age-groups (10,20, retinal venular caliber was predictive of
1.8 [95% CI 1.0 –3.1]; comparing largest 22,24,32,37,86,87). incident coronary heart disease (rate ratio
to lowest venular caliber quintile) (68). 3.0 [95% CI 1.6 –5.7]; comparing largest
Of greater significance are prospec-
Similarly, in children aged 6 – 8 years, to smallest venular caliber quartile) and
tive findings from four populations that
wider retinal venular caliber was also as- incident stroke (2.2 [1.1– 4.3]), whereas
sociated with higher BMI (69), suggesting show retinal arteriolar narrowing is a pre-
narrower arteriolar caliber was predictive
that retinal venular caliber may be influ- clinical marker of hypertension risk. The of incident coronary heart disease (2.0
enced by metabolic disorders early in life. ARIC Study (OR 1.62 [95% CI 1.21– [1.1–3.7]; comparing smallest to largest
There is also evidence that wider venular 2.18]; comparing smallest to largest AVR arteriolar caliber quartile) (98). These
caliber is associated with various micro- quintile) (58), the Beaver Dam Study findings suggest that both wider venular
vascular complications of diabetes, not (1.82 [1.39 –2.40]; comparing smallest to caliber and narrower arteriolar caliber
only diabetic retinopathy (70,71) but also largest AVR quartile) (88), the Blue may be markers of early subclinical car-
diabetic nephropathy (72). Mountains Study (2.6 [1.7–3.9]; compar- diovascular disease.
Despite these observations, the ing smallest to largest arteriolar caliber
pathophysiological processes underlying quintile) (89), and the Rotterdam Study CHANGES IN RETINAL
the association of wider retinal venular (1.38 [1.23–1.55]; per SD decrease in ar- VASCULAR ARCHITECTURE —
caliber with hyperglycemia, diabetes, and teriolar caliber) (90) all reported that New imaging methods have allowed the
its complications are unclear. It has been among individuals without hypertension measurement of other architectural
speculated that retinal venular widening at baseline, those with narrowed retinal changes in the retinal microvasculature.
may be the result of increased blood flow arterioles had a higher risk of hyperten- Hypertension, for example, has been as-
associated with hyperglycemia (73) and sion in the subsequent 3–10 years, inde- sociated with an increase in the retinal
retinal hypoxia (74). Alternatively, it may pendent of baseline blood pressure levels, arteriolar length-to-diameter ratio
also reflect inflammatory processes impli- BMI, and other known hypertension risk (99,100), increased retinal venular tortu-
cated in the pathogenesis of impaired glu- factors. osity (99), reduced branching angle at ar-
cose metabolism (75), supported by These observations support the hy- teriole bifurcations (101), and reduced
epidemiological findings of wider retinal pothesis that peripheral vascular resis- microvascular density (99,101,102).
venules with elevated systemic inflamma- tance, reflected by retinal arteriolar Some of these retinal changes have
tory markers (17,20,37,76). Experiments narrowing, is an important contributing also been shown to be associated with in-
have demonstrated that local inflamma- factor for hypertension development creased cardiovascular risk. For example,
tory processes lead to wider retinal venu- (91). Added support to this hypothesis the Beaver Dam Study demonstrated that
lar calibers. For example, administration comes from a recent genome-wide link- suboptimal arteriolar bifurcation and de-
of lipid hydroperoxide in the vitreous of age analysis from the Beaver Dam Study, creased arteriolar tortuosity are associated
rats leads to an increase in the retinal with coronary heart mortality (103).
which demonstrated that associations of
venular diameter (77). Similarly, admin-
retinal arteriolar diameter to multiple ge-
istration of Escherichia coli endotoxin in IMPLICATIONS FOR
netic loci are linked to regulation of blood
human eyes has been reported to increase RESEARCH AND CLINICAL
retinal venular diameter (78). Finally, ret- pressure, endothelial function, and vas- MANAGEMENT — It is now well
inal venular dilation may be related to en- culogenesis (92). Thus, retinal arteriolar recognized that individuals with impaired
dothelial dysfunction, reflecting an narrowing may be considered a surrogate glucose metabolism or pre-diabetes have
increased production of nitric oxide (79) marker of an individual’s genetic predis- higher mortality from cardiovascular dis-
secondary to higher levels of cytokines position to hypertension development ease (104 –106). Similarly, individuals
(80), seen often in association with im- (93). with high to normal blood pressure or
paired glucose metabolism (81,82) and Finally, a recent study has shown that prehypertension (107) are more likely to
diabetes (81). the association between higher blood develop cardiovascular events (108,109).
pressure and retinal arteriolar narrowing To permit appropriate preventative strat-
is detectable in healthy children aged 6 – 8 egies, there is therefore great interest in
Associations with hypertension and years (21), reinforcing the concept that early detection of individuals with pre-
prehypertension the effects of higher childhood blood diabetes and prehypertension.
In distinct contrast to the association of pressure may have an adverse effect on This review suggests that retinal im-
hyperglycemia with retinal venular cali- the microcirculation (94,95). age analysis offers a novel noninvasive
DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007 2711Retinal vascular changes
measurement of early changes in the vas- nal vascular changes using new imaging on cardiovascular events in 9795 people
culature—not detectable on routine clin- techniques offers great potential to ad- with type 2 diabetes mellitus (the FIELD
ical examination—that may allow the vance our understanding of the early study): randomised controlled trial. Lan-
identification of individuals at risk of di- pathophysiological pathways of diabetes cet 366:1849 –1861, 2005
8. Wong TY, Mitchell P: Hypertensive ret-
abetes and hypertension and their subse- and hypertension development. Recent
inopathy. N Engl J Med 351:2310 –2317,
quent complications. Retinal vascular studies support the concept that the reti- 2004
imaging might also permit physicians to nal vasculature provides a summary mea- 9. Wong T, Mitchell P: The eye in hyper-
optimize management of individuals with sure of lifetime exposure to various tension. Lancet 369:425– 435, 2007
established diabetes and/or hypertension. processes involved in the development of 10. Leung H, Wang JJ, Rochtchina E, Tan
For example, retinal vascular imaging diabetes and hypertension. Furthermore, AG, Wong TY, Klein R, Hubbard LD,
may allow monitoring of chronic varia- these studies suggest that the effects of Mitchell P: Relationships between age,
tions in glucose and blood pressure, as glucose and blood pressure on the retinal blood pressure, and retinal vessel diam-
well as the presence and severity of sub- microvasculature are graded and contin- eters in an older population. Invest Oph-
clinical microvascular damage. However, uous, and our current definitions of dia- thalmol Vis Sci 44:2900 –2904, 2003
a number of issues should be resolved be- betic and hypertensive retinopathy are 11. Sharp PS, Chaturvedi N, Wormald R,
McKeigue PM, Marmot MG, Young SM:
fore retinal vascular imaging can be uti- arbitrary and do not capture early disease. Hypertensive retinopathy in Afro-Carib-
lized in clinical practice. Future research is clearly needed to assess beans and Europeans: prevalence and
First, despite a large body of data on the ability of retinal vascular imaging to risk factor relationships. Hypertension
the associations and risk prediction of ret- provide clinically useful information that 25:1322–1325, 1995
inal vascular caliber measurement in dif- adds to existing risk prediction models of 12. Wang JJ, Mitchell P, Leung H, Roch-
ferent population-based studies, there is diabetes and hypertension. tchina E, Wong TY, Klein R: Hyperten-
no accepted standardized classification of sive retinal vessel wall signs in a general
retinal vascular changes, and a lack of older population: the Blue Mountains
age-, sex-, body size–, and blood pres- References Eye Study. Hypertension 42:534 –541,
sure–specific normative data. New stud- 1. Ciulla TA, Amador AG, Zinman B: Dia- 2003
betic retinopathy and diabetic macular 13. Yu T, Mitchell P, Berry G, Li W, Wang JJ:
ies of retinal vascular changes in children, Retinopathy in older persons without di-
edema: pathophysiology, screening, and
who are generally free of many systemic novel therapies. Diabetes Care 26:2653– abetes and its relationship to hyperten-
conditions, may provide these reference 2664, 2003 sion. Arch Ophthalmol 116:83– 89, 1998
data (21,110). 2. Tapp RJ, Shaw JE, Harper CA, de Cour- 14. Wong TY, Klein R, Sharrett AR, Manolio
Second, for retinal vascular imaging ten MP, Balkau B, McCarty DJ, Taylor TA, Hubbard LD, Marino EK, Kuller L,
to be useful for risk stratification, there HR, Welborn TA, Zimmet PZ: The prev- Burke G, Tracy RP, Polak JF, Gottdiener
must be a demonstration of independent alence of and factors associated with di- JS, Siscovick DS: The prevalence and
predictive value that substantially adds to abetic retinopathy in the Australian risk factors of retinal microvascular ab-
traditional methods. This has not been population. Diabetes Care 26:1731– normalities in older persons: the Cardio-
conclusively demonstrated. Different an- 1737, 2003 vascular Health Study. Ophthalmology
3. Klein R, Klein BE, Moss SE, Davis MD, 110:658 – 666, 2003
alytical methods have hampered the com-
DeMets DL: Glycosylated hemoglobin 15. Klein R, Klein BE, Moss SE, Wang Q:
parison of results between studies, and predicts the incidence and progression Hypertension and retinopathy, arterio-
application-common methods in differ- of diabetic retinopathy. JAMA 260: lar narrowing, and arteriovenous nick-
ent studies will allow data pooling to 2864 –2871, 1988 ing in a population. Arch Ophthalmol
generate more valid risk estimates. Addi- 4. The effect of intensive treatment of dia- 112:92–98, 1994
tionally, the role of novel measures of ret- betes on the development and progres- 16. Klein R, Klein BE, Moss SE: The relation
inal vascular structure (99,103,111–113) sion of long-term complications in of systemic hypertension to changes in
in predicting diseases remains to be deter- insulin-dependent diabetes mellitus: the the retinal vasculature: the Beaver Dam
mined. Diabetes Control and Complications Eye Study. Trans Am Ophthalmol Soc 95:
Third, the predictive value of retinal Trial Research Group. N Engl J Med 329: 329 –348, 1997
vascular imaging is currently based on as- 977–986, 1993 17. Klein R, Sharrett AR, Klein BE, Chamb-
5. The UK Propsective Diabetes Study less LE, Cooper LS, Hubbard LD, Evans
sociations seen in large population-based Group: Intensive blood-glucose control G: Are retinal arteriolar abnormalities
samples (114 –117). It is unclear whether with sulphonylureas or insulin com- related to atherosclerosis? The Athero-
the retinal measurements are sufficiently pared with conventional treatment and sclerosis Risk in Communities Study.
precise to differentiate risk at an individ- risk of complications in patients with Arterioscler Thromb Vasc Biol 20:1644 –
ual level. type 2 diabetes (UKPDS 33). Lancet 352: 1650, 2000
Finally, it is unknown whether mod- 837– 853, 1998 18. Sharrett AR, Hubbard LD, Cooper LS,
ification of risk factors (e.g., increased 6. The UK Propsective Diabetes Study Sorlie PD, Brothers RJ, Nieto FJ, Pinsky
physical activity, reduction in weight) or Group: Tight blood pressure control and JL, Klein R: Retinal arteriolar diameters
institution of treatment (e.g., diabetes and risk of macrovascular and microvascular and elevated blood pressure: the Athero-
antihypertensive medications) may im- complications in type 2 diabetes: sclerosis Risk in Communities Study.
UKPDS 38. BMJ 317:703–713, 1998 Am J Epidemiol 150:263–270, 1999
prove retinal vascular measures and 7. Keech A, Simes RJ, Barter P, Best J, Scott 19. Duncan BB, Wong TY, Tyroler HA,
whether this is associated with lowered R, Taskinen MR, Forder P, Pillai A, Davis Davis CE, Fuchs FD: Hypertensive reti-
risks of diabetes, hypertension, and their T, Glasziou P, Drury P, Kesaniemi YA, nopathy and incident coronary heart
complications. This remains an important Sullivan D, Hunt D, Colman P, d’Emden disease in high risk men. Br J Ophthalmol
area of future research. M, Whiting M, Ehnholm C, Laakso M: 86:1002–1006, 2002
In conclusion, measurement of reti- Effects of long-term fenofibrate therapy 20. Wong TY, Islam FM, Klein R, Klein BE,
2712 DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007Nguyen, Wang, and Wong
Cotch MF, Castro C, Sharrett AR, Shahar Am J Ophthalmol 77:472– 477, 1974 42. Svardsudd K, Wedel H, Aurell E, Tibblin
E: Retinal vascular caliber, cardiovascu- 31. Parr JC, Spears GF: Mathematic relation- G: Hypertensive eye ground changes:
lar risk factors, and inflammation: the ships between the width of a retinal ar- prevalence, relation to blood pressure
multi-ethnic study of atherosclerosis tery and the widths of its branches. Am J and prognostic importance: the study of
(MESA). Invest Ophthalmol Vis Sci 47: Ophthalmol 77:478 – 483, 1974 men born in 1913. Acta Med Scand 204:
2341–2350, 2006 32. Wong TY, Klein R, Klein BE, Meuer SM, 159 –167, 1978
21. Mitchell P, Cheung N, de Haseth K, Tay- Hubbard LD: Retinal vessel diameters 43. McDonough JR, Garrison GE, Hames
lor B, Rochtchina E, Islam FMA, Wang and their associations with age and CG: Blood pressure and hypertensive
JJ, Saw SM, Wong TY: Blood pressure blood pressure. Invest Ophthalmol Vis Sci disease among negroes and whites: a
and retinal arteriolar narrowing in chil- 44:4644 – 4650, 2003 study in Evans County, Georgia. Ann In-
dren. Hypertension 49:1156 –1162, 2007 33. Wong TY, Klein R, Couper DJ, Cooper tern Med 61:208 –228, 1964
22. Hubbard LD, Brothers RJ, King WN, LS, Shahar E, Hubbard LD, Wofford MR, 44. Stolk RP, Vingerling JR, de Jong PT,
Clegg LX, Klein R, Cooper LS, Sharrett Sharrett AR: Retinal microvascular ab- Dielemans I, Hofman A, Lamberts SW,
AR, Davis MD, Cai J: Methods for evalu- normalities and incident stroke: the Ath- Pols HA, Grobbee DE: Retinopathy, glu-
ation of retinal microvascular abnormal- erosclerosis Risk in Communities Study. cose, and insulin in an elderly popula-
ities associated with hypertension/ Lancet 358:1134 –1140, 2001 tion: the Rotterdam Study. Diabetes 44:
sclerosis in the Atherosclerosis Risk in 34. Mitchell P, Wang JJ, Wong TY, Smith W, 11–15, 1995
Communities Study. Ophthalmology Klein R, Leeder SR: Retinal microvascu- 45. Cugati S, Cikamatana L, Wang JJ, Kifley
106:2269 –2280, 1999 lar signs and risk of stroke and stroke A, Liew G, Mitchell P: Five-year inci-
23. van Leiden HA, Dekker JM, Moll AC, mortality. Neurology 65:1005–1009, dence and progression of vascular reti-
Nijpels G, Heine RJ, Bouter LM, Stehou- 2005 nopathy in persons without diabetes: the
wer CD, Polak BC: Blood pressure, lip- 35. Wong TY, Klein R, Sharrett AR, Duncan Blue Mountains Eye Study. Eye 20:
ids, and obesity are associated with BB, Couper DJ, Tielsch JM, Klein BE, 1239 –1245, 2006
retinopathy: the Hoorn Study. Diabetes Hubbard LD: Retinal arteriolar narrow- 46. Wong TY, Barr EL, Tapp RJ, Harper CA,
Care 25:1320 –1325, 2002 ing and risk of coronary heart disease in Taylor HR, Zimmet PZ, Shaw JE: Reti-
24. Kawasaki R, Wang JJ, Rochtchina E, men and women: the Atherosclerosis nopathy in persons with impaired
Taylor B, Wong TY, Tominaga M, Kato Risk in Communities Study. JAMA 287: glucose metabolism: the Australian Dia-
T, Daimon M, Oizumi T, Kawata S, 1153–1159, 2002 betes Obesity and Lifestyle (AusDiab)
Kayama T, Yamashita H, Mitchell P: Car- 36. Patton N, Aslam T, Macgillivray T, Dhil- study. Am J Ophthalmol 140:1157–1159,
diovascular risk factors and retinal mi- lon B, Constable I: Asymmetry of retinal 2005
crovascular signs in an adult Japanese arteriolar branch widths at junctions af- 47. The prevalence of retinopathy in im-
population: the Funagata Study. Oph- fects ability of formulae to predict trunk paired glucose tolerance and recent-on-
thalmology 113:1378 –1384, 2006 arteriolar widths. Invest Ophthalmol Vis set diabetes in the Diabetes Prevention
25. Couper DJ, Klein R, Hubbard LD, Wong Sci 47:1329 –1333, 2006 Program. Diabet Med 24:137–144, 2007
TY, Sorlie PD, Cooper LS, Brothers RJ, 37. Ikram MK, de Jong FJ, Vingerling JR, 48. Wong TY, Klein R, Islam FM, Cotch MF,
Nieto FJ: Reliability of retinal photogra- Witteman JC, Hofman A, Breteler MM, Couper DJ, Klein BE, Hubbard L, Shar-
phy in the assessment of retinal micro- de Jong PT: Are retinal arteriolar or rett AR: Three-year incidence and cumu-
vascular characteristics: the Athero- venular diameters associated with mark- lative prevalence of retinopathy: the
sclerosis Risk in Communities Study. ers for cardiovascular disorders? The Atherosclerosis Risk in Communities
Am J Ophthalmol 133:78 – 88, 2002 Rotterdam Study. Invest Ophthalmol Vis Study. Am J Ophthalmol 143:970 –976,
26. Sherry LM, Wang JJ, Rochtchina E, Sci 45:2129 –2134, 2004 2007
Wong T, Klein R, Hubbard L, Mitchell P: 38. Liew G, Sharrett AR, Kronmal R, Klein R, 49. Wong TY, Klein R, Duncan BB, Nieto FJ,
Reliability of computer-assisted retinal Wong TY, Mitchell P, Kifley A, Wang JJ: Klein BE, Couper DJ, Hubbard LD, Shar-
vessel measurement in a population. Measurement of retinal vascular caliber: rett AR: Racial differences in the preva-
Clin Experiment Ophthalmol 30:179 – issues and alternatives to using the arte- lence of hypertensive retinopathy.
182, 2002 riole to venule ratio. Invest Ophthalmol Hypertension 41:1086 –1091, 2003
27. Li H, Hsu W, Lee ML, Wong TY: Auto- Vis Sci 48:52–57, 2007 50. van Hecke MV, Dekker JM, Nijpels G,
matic grading of retinal vessel caliber. 39. Liew G, Wong TY, Mitchell P, Wang JJ: Moll AC, Heine RJ, Bouter LM, Polak BC,
IEEE Trans Biomed Eng 52:1352–1355, Are narrower or wider retinal venules as- Stehouwer CD: Inflammation and endo-
2005 sociated with incident hypertension? thelial dysfunction are associated with
28. Wong TY, Knudtson MD, Klein R, Klein Hypertension 48:e10, 2006 retinopathy: the Hoorn Study. Diabeto-
BE, Meuer SM, Hubbard LD: Computer- 40. Patton N, Aslam TM, MacGillivray T, logia 48:1300 –1306, 2005
assisted measurement of retinal vessel Deary IJ, Dhillon B, Eikelboom RH, Yo- 51. Miyamoto K, Khosrof S, Bursell SE, Ro-
diameters in the Beaver Dam Eye Study: gesan K, Constable IJ: Retinal image han R, Murata T, Clermont AC, Aiello
methodology, correlation between eyes, analysis: concepts, applications and po- LP, Ogura Y, Adamis AP: Prevention of
and effect of refractive errors. Ophthal- tential. Prog Retin Eye Res 25:99 –127, leukostasis and vascular leakage in
mology 111:1183–1190, 2004 2006 streptozotocin-induced diabetic reti-
29. Wagener HP, Clay GE, Gipner JF: Clas- 41. Leibowitz HM, Krueger DE, Maunder nopathy via intercellular adhesion mol-
sification of retinal lesions in the pres- LR, Milton RC, Kini MM, Kahn HA, ecule-1 inhibition. Proc Natl Acad Sci U S
ence of vascular hypertension: report Nickerson RJ, Pool J, Colton TL, Ganley A 96:10836 –10841, 1999
submitted to the American Ophthalmo- JP, Loewenstein JI, Dawber TR: The Fra- 52. Izuora KE, Chase HP, Jackson WE, Coll
logical Society by the committee on mingham Eye Study monograph: an JR, Osberg IM, Gottlieb PA, Rewers MJ,
Classification of Hypertensive Disease of ophthalmological and epidemiological Garg SK: Inflammatory markers and di-
the Retina. Trans Am Ophthalmol Soc 45: study of cataract, glaucoma, diabetic ret- abetic retinopathy in type 1 diabetes. Di-
57–73, 1947 inopathy, macular degeneration, and vi- abetes Care 28:714 –715, 2005
30. Parr JC, Spears GF: General caliber of the sual acuity in a general population of 53. Joussen AM, Poulaki V, Le ML, Koizumi
retinal arteries expressed as the equiva- 2631 adults, 1973–1975. Surv Ophthal- K, Esser C, Janicki H, Schraermeyer U,
lent width of the central retinal artery. mol 24:335– 610, 1980 Kociok N, Fauser S, Kirchhof B, Kern TS,
DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007 2713Retinal vascular changes
Adamis AP: A central role for inflamma- of diabetes mellitus. Arch Intern Med Y: Lipid hydroperoxide stimulates leu-
tion in the pathogenesis of diabetic reti- 165:1060 –1065, 2005 kocyte-endothelium interaction in the
nopathy. FASEB J 18:1450 –1452, 2004 66. Ikram MK, Janssen JA, Roos AM, Ri- retinal microcirculation. Exp Eye Res 75:
54. Harris MI, Klein R, Welborn TA, etveld I, Witteman JC, Breteler MM, 69 –75, 2002
Knuiman MW: Onset of NIDDM occurs Hofman A, van Duijn CM, de Jong PT: 78. Kolodjaschna J, Berisha F, Lung S,
at least 4 –7 yr before clinical diagnosis. Retinal vessel diameters and risk of im- Schaller G, Polska E, Jilma B, Wolzt M,
Diabetes Care 15:815– 819, 1992 paired fasting glucose or diabetes: the Schmetterer L: LPS-induced microvas-
55. Cugati S, Mitchell P, Wang JJ: Do reti- Rotterdam Study. Diabetes 55:506 –510, cular leukocytosis can be assessed by
nopathy signs in non-diabetic individu- 2006 blue-field entoptic phenomenon. Am J
als predict the subsequent risk of 67. Wong TY, Duncan BB, Golden SH, Klein Physiol Heart Circ Physiol 287:H691–
diabetes? Br J Ophthalmol 90:928 –929, R, Couper DJ, Klein BE, Hubbard LD, H694, 2004
2006 Sharrett AR, Schmidt MI: Associations 79. Wilkinson-Berka JL: Vasoactive factors
56. Wong TY, Mohamed Q, Klein R, Couper between the metabolic syndrome and and diabetic retinopathy: vascular endo-
DJ: Do retinopathy signs in non-diabetic retinal microvascular signs: the Athero- thelial growth factor, cycoloxygenase-2
individuals predict the subsequent risk sclerosis Risk In Communities study. In- and nitric oxide. Curr Pharm Des
of diabetes? Br J Ophthalmol 90:301– vest Ophthalmol Vis Sci 45:2949 –2954, 10:3331–3348, 2004
303, 2006 2004 80. Chester AH, Borland JA, Buttery LD,
57. Klein R, Klein BEK, Mos SE, Wong TY: 68. Wang JJ, Taylor B, Wong TY, Chua B, Mitchell JA, Cunningham DA, Hafizi S,
The relationship of retinopathy in per- Rochtchina E, Klein R, Mitchell P: Reti- Hoare GS, Springall DR, Polak JM, Ya-
sons without diabetes to the 15-year in- nal vessel diameters and obesity: a pop- coub MH: Induction of nitric oxide syn-
cidence of diabetes and hypertension: ulation-based study in older persons. thase in human vascular smooth muscle:
Beaver Dam Eye Study. Trans Am Oph- Obesity (Silver Spring) 14:206 –214, interactions between proinflammatory
thalmol Soc 104:98 –107, 2006 2006 cytokines. Cardiovasc Res 38:814 – 821,
58. Wong TY, Klein R, Sharrett AR, Duncan 69. Cheung N, Saw SM, Islam FM, Rogers 1998
BB, Couper DJ, Klein BE, Hubbard LD, SL, Shankar A, de Haseth K, Mitchell P, 81. de Rekeneire N, Peila R, Ding J, Colbert
Nieto FJ: Retinal arteriolar diameter and Wong TY: BMI and retinal vascular cali- LH, Visser M, Shorr RI, Kritchevsky SB,
risk for hypertension. Ann Intern Med ber in children. Obesity (Silver Spring) Kuller LH, Strotmeyer ES, Schwartz AV,
140:248 –255, 2004 15:209 –215, 2007 Vellas B, Harris TB: Diabetes, hypergly-
59. Wong TY, Rosamond W, Chang PP, 70. Klein R, Klein BE, Moss SE, Wong TY, cemia, and inflammation in older indi-
Couper DJ, Sharrett AR, Hubbard LD, Sharrett AR: Retinal vascular caliber in viduals: the health, aging and body
Folsom AR, Klein R: Retinopathy and persons with type 2 diabetes: the Wis- composition study. Diabetes Care 29:
risk of congestive heart failure. JAMA consin Epidemiological Study of Dia- 1902–1908, 2006
293:63– 69, 2005 betic Retinopathy: XX. Ophthalmology 82. Ling PR, Mueller C, Smith RJ, Bistrian
60. Wong TY, Coresh J, Klein R, Muntner P, 113:1488 –1498, 2006 BR: Hyperglycemia induced by glucose
Couper DJ, Sharrett AR, Klein BE, Heiss 71. Klein R, Klein BE, Moss SE, Wong TY, infusion causes hepatic oxidative stress
G, Hubbard LD, Duncan BB: Retinal mi- Hubbard L, Cruickshanks KJ, Palta M: and systemic inflammation, but not
crovascular abnormalities and renal dys- Retinal vascular abnormalities in per- STAT3 or MAP kinase activation in liver
function: the atherosclerosis risk in sons with type 1 diabetes: the Wisconsin in rats. Metabolism 52:868 – 874, 2003
communities study. J Am Soc Nephrol 15: Epidemiologic Study of Diabetic Reti- 83. Nguyen TT, Wong TY: Retinal vascular
2469 –2476, 2004 nopathy: XVIII. Ophthalmology 110: manifestations of metabolic disorders.
61. Edwards MS, Wilson DB, Craven TE, 2118 –2125, 2003 Trends Endocrinol Metab 17:262–268,
Stafford J, Fried LF, Wong TY, Klein R, 72. Wong TY, Shankar A, Klein R, Klein BE: 2006
Burke GL, Hansen KJ: Associations be- Retinal vessel diameters and the inci- 84. Tso MO, Jampol LM: Pathophysiology of
tween retinal microvascular abnormali- dence of gross proteinuria and renal in- hypertensive retinopathy. Ophthalmol-
ties and declining renal function in the sufficiency in people with type 1 ogy 89:1132–1145, 1982
elderly population: the Cardiovascular diabetes. Diabetes 53:179 –184, 2004 85. Walsh JB: Hypertensive retinopathy: de-
Health Study. Am J Kidney Dis 46:214 – 73. Grunwald JE, Riva CE, Baine J, Brucker scription, classification, and prognosis.
224, 2005 AJ: Total retinal volumetric blood flow Ophthalmology 89:1127–1131, 1982
62. Rema M, Mohan V, Deepa R, Ravikumar rate in diabetic patients with poor glyce- 86. Leung H, Wang JJ, Rochtchina E, Wong
R: Association of carotid intima-media mic control. Invest Ophthalmol Vis Sci 33: TY, Klein R, Mitchell P: Impact of cur-
thickness and arterial stiffness with dia- 356 –363, 1992 rent and past blood pressure on retinal
betic retinopathy: the Chennai Urban 74. Saldivar E, Cabrales P, Tsai AG, Intagli- arteriolar diameter in an older popula-
Rural Epidemiology Study (CURES-2). etta M: Microcirculatory changes during tion. J Hypertens 22:1543–1549, 2004
Diabetes Care 27:1962–1967, 2004 chronic adaptation to hypoxia. Am J 87. Wong TY, Hubbard LD, Klein R, Marino
63. Wong TY, Klein R, Islam FM, Cotch MF, Physiol Heart Circ Physiol 285:H2064 – EK, Kronmal R, Sharrett AR, Siscovick
Folsom AR, Klein BE, Sharrett AR, Shea H2071, 2003 DS, Burke G, Tielsch JM: Retinal micro-
S: Diabetic retinopathy in a multi-ethnic 75. Caballero AE: Metabolic and vascular vascular abnormalities and blood pres-
cohort in the United States. Am J Oph- abnormalities in subjects at risk for type sure in older people: the Cardiovascular
thalmol 141:446 – 455, 2006 2 diabetes: the early start of a dangerous Health Study. Br J Ophthalmol 86:1007–
64. Wong TY, Klein R, Sharrett AR, Schmidt situation. Arch Med Res 36:241–249, 1013, 2002
MI, Pankow JS, Couper DJ, Klein BE, 2005 88. Wong TY, Shankar A, Klein R, Klein BE,
Hubbard LD, Duncan BB: Retinal arte- 76. Klein R, Klein BE, Knudtson MD, Wong Hubbard LD: Prospective cohort study
riolar narrowing and risk of diabetes TY, Tsai MY: Are inflammatory factors of retinal vessel diameters and risk of hy-
mellitus in middle-aged persons. JAMA related to retinal vessel caliber? The Bea- pertension. BMJ 329:79, 2004
287:2528 –2533, 2002 ver Dam Eye Study. Arch Ophthalmol 89. Smith W, Wang JJ, Wong TY, Roch-
65. Wong TY, Shankar A, Klein R, Klein BE, 124:87–94, 2006 tchina E, Klein R, Leeder SR, Mitchell P:
Hubbard LD: Retinal arteriolar narrow- 77. Tamai K, Matsubara A, Tomida K, Mat- Retinal arteriolar narrowing is associated
ing, hypertension, and subsequent risk suda Y, Morita H, Armstrong D, Ogura with 5-year incident severe hyperten-
2714 DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007Nguyen, Wang, and Wong
sion: the Blue Mountains Eye Study. Hy- SA, Hughes AD: Arteriolar length-diam- the JNC 7 report. JAMA 289:2560 –
pertension 44:442– 447, 2004 eter (L:D) ratio: a geometric parameter of 2572, 2003
90. Ikram MK, Witteman JC, Vingerling JR, the retinal vasculature diagnostic of hy- 109. Hsia J, Margolis KL, Eaton CB, Wenger
Breteler MM, Hofman A, de Jong PT: pertension. J Hum Hypertens 10:417– NK, Allison M, Wu L, LaCroix AZ, Black
Retinal vessel diameters and risk of hy- 418,1996 HR: Prehypertension and cardiovascular
pertension: the Rotterdam Study. Hyper- 101. Stanton AV, Wasan B, Cerutti A, Ford S, disease risk in the Women’s Health Ini-
tension 47:189 –194, 2006 Marsh R, Sever PP, Thom SA, Hughes tiative. Circulation 115:855– 860, 2007
91. Mulvany MJ: Are vascular abnormalities AD: Vascular network changes in the 110. Cheung N, Islam FM, Saw SM, Shankar
a primary cause or secondary conse- retina with age and hypertension. J Hy- A, de Haseth K, Mitchell P, Wong TY:
quence of hypertension? Hypertension pertens 13:1724 –1728, 1995 Distribution and associations of retinal
18:I52–I57, 1991 102. Kutschbach P, Wolf S, Sieveking M, Ittel vascular caliber with ethnicity, gender,
92. Xing C, Klein BE, Klein R, Jun G, Lee KE, TH, Schulte K, Reim M: Retinal capillary and birth parameters in young children.
Iyengar SK: Genome-wide linkage study density in patients with arterial hyper- Invest Ophthalmol Vis Sci 48:1018 –1024,
of retinal vessel diameters in the Beaver tension: 2-year follow-up. Graefes Arch 2007
Dam Eye Study. Hypertension 47:797– Clin Exp Ophthalmol 236:410 – 414, 111. Gould DB, Phalan FC, van Mil SE, Sund-
802, 2006 1998 berg JP, Vahedi K, Massin P, Bousser
93. Wang JJ, Wong TY: Genetic determi- 103. Witt N, Wong TY, Hughes AD, Chatur- MG, Heutink P, Miner JH, Tournier-
nants of retinal vascular caliber: addi- vedi N, Klein BE, Evans R, McNamara Lasserve E, John SW: Role of COL4A1 in
tional insights into hypertension patho- M, Thom SA, Klein R: Abnormalities of small-vessel disease and hemorrhagic
genesis. Hypertension 47:644 – 645,2006 retinal microvascular structure and risk stroke. N Engl J Med 354:1489 –1496,
94. Ingelfinger JR: Pediatric antecedents of of mortality from ischemic heart disease 2006
adult cardiovascular disease–awareness and stroke. Hypertension 47:975–981, 112. Gekeler F, Shinoda K, Junger M, Bartz-
and intervention. N Engl J Med 350: 2006 Schmidt KU, Gelisken F: Familial retinal
2123–2126, 2004 104. Sorkin JD, Muller DC, Fleg JL, Andres R: arterial tortuosity associated with tortu-
95. Barker DJ, Osmond C, Golding J, Kuh D, The relation of fasting and 2-h postchal- osity in nail bed capillaries. Arch Oph-
Wadsworth ME: Growth in utero, blood lenge plasma glucose concentrations to thalmol 124:1492–1494, 2006
pressure in childhood and adult life, and mortality: data from the Baltimore Lon- 113. Muiesan ML, Grassi G: Assessment of
mortality from cardiovascular disease. gitudinal Study of Aging with a critical retinal vascular changes in hyperten-
BMJ 298:564 –567, 1989 review of the literature. Diabetes Care 28: sion: new perspectives. J Hypertens 24:
96. Ikram MK, De Jong FJ, Van Dijk EJ, Prins 2626 –2632, 2005 813– 814, 2006
ND, Hofman A, Breteler MM, De Jong 105. Brunner EJ, Shipley MJ, Witte DR, Fuller 114. Wong TY, Klein R, Nieto FJ, Klein BE,
PT: Retinal vessel diameters and cerebral JH, Marmot MG: Relation between Sharrett AR, Meuer SM, Hubbard LD,
small vessel disease: the Rotterdam Scan blood glucose and coronary mortality Tielsch JM: Retinal microvascular ab-
Study. Brain 129:182–188, 2006 over 33 years in the Whitehall Study. normalities and 10-year cardiovascular
97. Ikram MK, de Jong FJ, Bos MJ, Vinger- Diabetes Care 29:26 –31, 2006 mortality: a population-based case-con-
ling JR, Hofman A, Koudstaal PJ, de Jong 106. Glucose tolerance and mortality: com- trol study. Ophthalmology 110:933–940,
PT, Breteler MM: Retinal vessel diame- parison of WHO and American Diabetes 2003
ters and risk of stroke: the Rotterdam Association diagnostic criteria: the DE- 115. Wong TY, Klein R, Sharrett AR, Couper
Study. Neurology 66:1339 –1343, 2006 CODE study group: European Diabetes DJ, Klein BE, Liao DP, Hubbard LD,
98. Wong TY, Kamineni A, Klein R, Sharrett Epidemiology Group: Diabetes Epide- Mosley TH: Cerebral white matter le-
AR, Klein BE, Siscovick DS, Cushman miology: Collaborative analysis Of Diag- sions, retinopathy, and incident clinical
M, Duncan BB: Quantitative retinal nostic criteria in Europe. Lancet 354: stroke. JAMA 288:67–74, 2002
venular caliber and risk of cardiovascu- 617– 621, 1999 116. Wong TY, Mosley TH Jr, Klein R, Klein
lar disease in older persons: the cardio- 107. Gu D, Wildman RP, Wu X, Reynolds K, BE, Sharrett AR, Couper DJ, Hubbard
vascular health study. Arch Intern Med Huang J, Chen CS, He J: Incidence and LD: Retinal microvascular changes and
166:2388 –2394, 2006 predictors of hypertension over 8 years MRI signs of cerebral atrophy in healthy,
99. Hughes AD, Martinez-Perez E, Jabbar among Chinese men and women. J Hy- middle-aged people. Neurology 61:806 –
AS, Hassan A, Witt NW, Mistry PD, pertens 25:517–523, 2007 811, 2003
Chapman N, Stanton AV, Beevers G, 108. Chobanian AV, Bakris GL, Black HR, 117. Wong TY, Klein R, Sharrett AR, Nieto FJ,
Pedrinelli R, Parker KH, Thom SA: Cushman WC, Green LA, Izzo JL Jr, Boland LL, Couper DJ, Mosley TH, Klein
Quantification of topological changes in Jones DW, Materson BJ, Oparil S, BE, Hubbard LD, Szklo M: Retinal mi-
retinal vascular architecture in essential Wright JT Jr, Roccella EJ: The Seventh crovascular abnormalities and cognitive
and malignant hypertension. J Hypertens Report of the Joint National Committee impairment in middle-aged persons: the
24:889 – 894, 2006 on Prevention, Detection, Evaluation, Atherosclerosis Risk in Communities
100. King LA, Stanton AV, Sever PS, Thom and Treatment of High Blood Pressure: Study. Stroke 33:1487–1492, 2002
DIABETES CARE, VOLUME 30, NUMBER 10, OCTOBER 2007 2715You can also read