100 Top Hospitals, 2019 - Competitor Report Client Hospital Date of Delivery - IBM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
100 Top Hospitals, 2019 Competitor Report Client Hospital Date of Delivery
Contents –Background and Approach
–Profiled Competitors
–Executive Summary
–2017 Performance and 5-Year Rate of
Improvement Graphs
–Methodology Overview
Watson Health © IBM Corporation 2019 2Background In this analysis, Sample Hospital’s performance and rate of
improvement are compared to that of seven client-selected
and Approach competitors, using the 100 Top Hospitals® measures and
methodologies
Measures included in the analysis:
OVERALL performance score
Inpatient mortality Average length of stay
Complications Emergency department throughput
Healthcare-associated infections* Inpatient expense per discharge
Mean 30-day mortality Operating profit margin
Mean 30-day readmissions HCAHPS score (Overall rating question)
Results are displayed as the rank percentile of each
hospital’s performance and rate of improvement compared to
all U.S. hospitals within each hospital’s 100 Top peer group
– Conversion to percentiles allows direct comparison of all
selected hospitals, without regard to peer group
*Healthcare-Associated Infections composite index was included in the Overall Score but is not reported on the matrix graph because there
are insufficient data years to trend. We have shown HAI as a separate bar graph.
Watson Health © IBM Corporation 2019Profiled
Competitors –Client Hospital
–Competitor 1
–Competitor 2
–Competitor 3
–Competitor 4
–Competitor 5
–Competitor 6
–Competitor 7
Watson Health © IBM Corporation 2019 4Executive Overall National Performance
– Sample Hospital falls into the ____ Percentile nationally for
Summary both 2017 performance and 2013-2017 rate of improvement
– Competitor ______ and ______ facilities lead this group
based on performance on all 100 Top Hospitals measures
Where Sample Hospital is strong among peers, and
improving
– Curabitur pulvinar dui a erat placerat gravida. Nunc non felis
eu ante vestibulum posuere ultricies at neque.
– Donec vehicula lorem feugiat enim congue, quis blandit
metus suscipit. Mauris vel elementum velit. In at dictum arcu.
Where Sample Hospital might have significant opportunity to
improve nationally, and compared to these competitors
– Phasellus vitae egestas felis. Sed libero ante, dignissim id
massa commodo, iaculis tincidunt neque.
– Pellentesque volutpat, sapien eget bibendum lobortis, sem
leo feugiat odio, nec ornare neque sapien at leo.
Watson Health © IBM Corporation 2019 5100 Top Hospitals, 2019
Overall Performance Comparison
2017 Performance and 2013-2017 Rate of Improvement
100
Hospital Key
3 1 Client Hospital
80 4 2 Competitor 1
7
3 Competitor 2
2013 - 2017 Rate of Improvement
1 4 Competitor 3
5 Competitor 4
6 6 Competitor 5
60
7 Competitor 6
8 Competitor 7
40
2 Quintile Key
> 80 to 100
8 > 60 to 80
20
> 40 to 60
> 20 to 40
5 > 0 to 20
0
0 20 40 60 80 100
2017 Performance
Watson Health © IBM Corporation 2019 6100 Top Hospitals, 2019
Risk-Adjusted Inpatient Mortality
2017 Performance and 2013-2017 Rate of Improvement
100
4 Hospital Key
6
3 7 1 Client Hospital
80 2 Competitor 1
2013 - 2017 Rate of Improvement
3 Competitor 2
4 Competitor 3
5 Competitor 4
60 6 Competitor 5
7 Competitor 6
8 Competitor 7
8
40
2 Quintile Key
> 80 to 100
> 60 to 80
20 5
> 40 to 60
1
> 20 to 40
> 0 to 20
0
0 20 40 60 80 100
2017 Performance
Watson Health © IBM Corporation 2019 7100 Top Hospitals, 2019
Risk-Adjusted Complications
2017 Performance and 2013-2017 Rate of Improvement
100
6 Hospital Key
3 1
7 1 Client Hospital
8
80 5 2 Competitor 1
2013 - 2017 Rate of Improvement
3 Competitor 2
2 4 Competitor 3
5 Competitor 4
60 6 Competitor 5
7 Competitor 6
8 Competitor 7
4
40
Quintile Key
> 80 to 100
20 > 60 to 80
> 40 to 60
> 20 to 40
> 0 to 20
0
0 20 40 60 80 100
2017 Performance
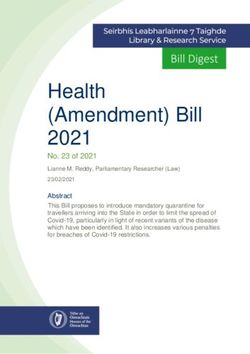
Watson Health © IBM Corporation 2019 8100 Top Hospitals, 2019
Healthcare-Associated Infections
(HAI) Composite Performance
Higher percentile denotes better relative performance in
peer comparison group.
100 Client Hospital
93.6
88.4
90 Competitor 1
80 Competitor 2
72.9
65.5
2017 Rank Percentile
70 Competitor 3
61.0
60 Competitor 4
50 Competitor 5
Competitor 6
40
Competitor 7
30
25.2
20
11.9
6.7
10
0
Watson Health © IBM Corporation 2019 9100 Top Hospitals, 2019
Mean 30-Day Mortality*
2017 Performance and 2013-2017 Rate of Improvement
100
8 Hospital Key
6
1 Client Hospital
1
80 2 Competitor 1
2013 - 2017 Rate of Improvement
3 Competitor 2
4 Competitor 3
5 Competitor 4
60 6 Competitor 5
3
7 Competitor 6
8 Competitor 7
40 5
2
4 Quintile Key
> 80 to 100
20 > 60 to 80
> 40 to 60
> 20 to 40
7 > 0 to 20
0
0 20 40 60 80 100
2017 Performance
*Includes AMI, HF, PN, COPD, STK
Watson Health © IBM Corporation 2019 10100 Top Hospitals, 2019
30-Day Readmissions
2017 Performance and 2013-2017 Rate of Improvement
100
4
Hospital Key
3 1 Client Hospital
80 2 Competitor 1
2013 - 2017 Rate of Improvement
3 Competitor 2
4 Competitor 3
5 Competitor 4
60
7
6 Competitor 5
7 Competitor 6
8 Competitor 7
40 2
Quintile Key
> 80 to 100
20
> 60 to 80
6 > 40 to 60
5 > 20 to 40
8 1
> 0 to 20
0
0 20 40 60 80 100
2017 Performance
*Includes AMI, HF, PN, THA/TKA, COPD, STK
Watson Health © IBM Corporation 2019 11100 Top Hospitals, 2019
Severity-Adjusted Average Length of Stay
2017 Performance and 2013-2017 Rate of Improvement
100
7
Hospital Key
1 Client Hospital
2 Competitor 1
80 4 3 Competitor 2
2013 - 2017 Rate of Improvement
4 Competitor 3
5 Competitor 4
60 6 Competitor 5
6 7 Competitor 6
8 Competitor 7
40
8 Quintile Key
> 80 to 100
> 60 to 80
20
> 40 to 60
1
3 > 20 to 40
2
5 > 0 to 20
0
0 20 40 60 80 100
2017 Performance
Watson Health © IBM Corporation 2019 12100 Top Hospitals, 2019
Mean Emergency Department Throughput*
2017 Performance and 2013-2017 Rate of Improvement
100 2
Hospital Key
3
4 1 1 Client Hospital
80 2 Competitor 1
3 Competitor 2
2013 - 2017 Rate of Improvement
4 Competitor 3
5 Competitor 4
60 6 Competitor 5
7
5 7 Competitor 6
8 Competitor 7
40
Quintile Key
> 80 to 100
20 > 60 to 80
6 > 40 to 60
> 20 to 40
8 > 0 to 20
0
0 20 40 60 80 100
2017 Performance *Includes median time to admission; median time
to discharge for non-admitted patients
Watson Health © IBM Corporation 2019 13100 Top Hospitals, 2019
Inpatient Expense per Discharge*
2017 Performance and 2013-2017 Rate of Improvement
100 8
Hospital Key
1 1 Client Hospital
6 2 Competitor 1
80
2013 - 2017 Rate of Improvement
3 Competitor 2
4 Competitor 3
5 Competitor 4
60
2 6 Competitor 5
7 Competitor 6
8 Competitor 7
40
Quintile Key
> 80 to 100
7 > 60 to 80
20
> 40 to 60
5
3 > 20 to 40
4
> 0 to 20
0
0 20 40 60 80 100
2017 Performance
*CMS area wage index and casemix adjusted
Watson Health © IBM Corporation 2019 14100 Top Hospitals, 2019
Adjusted Operating Profit Margin*
2017 Performance and 2013-2017 Rate of Improvement
100
Hospital Key
1 Client Hospital
80 2 Competitor 1
2013 - 2017 Rate of Improvement
3 Competitor 2
4
4 Competitor 3
5 Competitor 4
60 6 Competitor 5
2 7 Competitor 6
3
8 Competitor 7
1 7
40
Quintile Key
> 80 to 100
6 > 60 to 80
20
8 > 40 to 60
> 20 to 40
5 > 0 to 20
0
0 20 40 60 80 100
2017 Performance
*Adjusted for net related organization expense
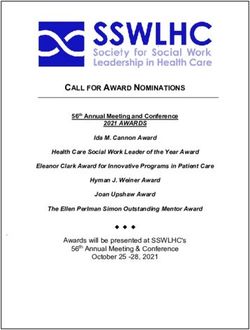
Watson Health © IBM Corporation 2019 15100 Top Hospitals, 2019
HCAHPS Score (Overall rating question)
2017 Performance and 2013-2017 Rate of Improvement
100
Hospital Key
1
1 Client Hospital
80
2 Competitor 1
3 Competitor 2
2013 - 2017 Rate of Improvement
3 4 Competitor 3
5 Competitor 4
60 6 Competitor 5
7 7 Competitor 6
8 Competitor 7
40
5 Quintile Key
> 80 to 100
> 60 to 80
20 6
> 40 to 60
4 2 > 20 to 40
8 > 0 to 20
0
0 20 40 60 80 100
2017 Performance
Watson Health © IBM Corporation 2019 16Methodology
Overview
17Watson Health All non-federal U.S. acute care hospitals are eligible
– Must have Medicare patient claims with valid POA coding
100 Top Study (2016-2017)
Eligibility – Must have a complete 2017 cost report
– Must have data for all included measures*
Specialty and Critical Access hospitals are not included
Note: This year we are offering a separate analysis and reports
for CAHs
We exclude hospitals with the following characteristics:
– Federally-owned
– Non-U.S.
– Fewer than 25 beds
– Fewer than 100 Medicare discharges
– Medicare average length of stay greater than 30 days
– No Medicare deaths reported
*Exceptions: For hospitals missing individual 30-day measures, BUT NOT ALL, we substitute
the class median.
Watson Health © IBM Corporation 2019 18Hospital
Comparison
Groups
100 Top Hospitals® Comparison Groups Winners Total
Major Teaching Hospitals – 3 ways to qualify: 15 217
─ 400+ acute beds, 0.25 GME student to acute beds ratio, 10
GME sponsored programs or 20 GME affiliated programs
─ 30 GME affiliated programs
─ 0.6 GME student to acute beds ratio
Teaching Hospitals – 2 ways to qualify: 25 488
─ 200+ acute beds and 0.03 GME student to acute beds ratio
─ 200+ acute beds and 3 GME affiliated programs
Large Community Hospitals – 250+ beds 20 290
Medium Community Hospitals – 100 to 249 beds 20 914
Small Community Hospitals – 25 to 99 beds 20 843
Totals 100 2,752
SOURCES: 2017 cost report – acute beds in service; GME student FTEs. AMA &
AOA residency program lists.
Watson Health © IBM Corporation 2019 19Scorecard Domains,
Measures and
Rank Weights
2017 Class 1 Trend
Domain Performance Measure
Weight 2017* Weight
Risk-adjusted inpatient mortality 1 1.25 1
Clinical Outcomes Risk-adjusted complications 1 1.25 1
Mean HAI index* 1 na na
Quality
Mean 30-day mortality rate (AMI, HF, PN,
COPD, STK) 1 1.25 1
Extended
Outcomes
Mean 30-day readmission rate (AMI, HF, PN,
THA/TKA, COPD, STK) 1 1.25 1
Severity-adjusted average length of stay 1 1 1
Operations
Efficiency Mean emergency department throughput 1 1 1
Inpatient expense per discharge, AWI and
case mix adjusted 1 1 1
Financial Adjusted operating profit margin 1 1 1
Patient Experience
HCAHPS Overall Patient Rating Score 1 1 1
*HAI metrics are not ranked for small community hospitals. 2017 weights for inpatient mortality, complications, 30-day
mortality and 30-day readmission ranks were increased to 1.25 to balance quality and operational group weights for them.
Watson Health © IBM Corporation 2019 20Data
Sources and
Time Periods
2017 Performance (100 Top
Performance Measure 5-Year Trend
Award)
MEDPAR Federal Fiscal Year
Inpatient mortality MEDPAR FFY 2012-2017*
(FFY) 2016 and 2017*
Complications
Healthcare-associated infection (HAI) CMS Hospital Compare
Not Trended
indices (CMSHC) CY 2017
30-day mortality rates CMSHC July 1, 2014-June 30, CMSHC 3 yr data sets ending June 30,
2017 2013, 2014, 2015, 2016, 2017
30-day readmission rates
Average length of stay MEDPAR FFY 2017 MEDPAR FFY 2013-2017
CMSHC CY 2014, 2015, 2016, 2017
CMSHC CY 2017
Emergency department wait times FFY 2013 (CY2013 unavailable)
CMS HCRIS 2018 Q3
Inpatient expense/disch CMS HCRIS 2018 Q3
Hospital 2013, 2014, 2015, 2016, 2017
Hospital 2017 cost reports
Operating profit margin cost reports
CMSHC CY 2013, 2014, 2015, 2016,
HCAHPS Score CMSHC CY 2017
2017
*Two years of MEDPAR data are combined to calculate each study year data point.
.
Watson Health © IBM Corporation 2019 21Winner Exclusion Hospitals are ineligible to be considered 100 Top
hospital winners if any of the following apply:
Rules
– An observed inpatient mortality or complications rate that is
statistically worse than expected (99% confidence) and
above the outlier group 75th percentile trim point
– An outlier value for inpatient expense or operating profit
margin (Interquartile Range (IQR) Methodology)
– A negative operating profit margin
– Hospital had data for only 1 of the 3 HAI measures included
in the medium community hospital comparison group (See
HAI for details)
– Hospital has had a 100 Top hospital award rescinded by the
Watson Health 100 Top Program within 3 years
Note: If a hospital meets a winner exclusion rule, this does NOT mean
the hospital would have been a winner. It means they are excluded from
consideration when final ranking and selection of winners occurs.
Watson Health © IBM Corporation 2019 22General Ranking
Methodology
2017 performance 2013-2017 rate of improvement
– Uses most current public data (various – Regression line t-statistic is produced
data sets ending in 2017) to rank each measure
– Each measure ranked independently – Each measure ranked independently
by peer comparison group by peer comparison group
– Ranks are weighted, summed and the – Ranks are weighted, summed and the
sum is re-ranked by comparison group sum is re-ranked by comparison group
to determine each hospital’s overall to determine each hospital’s overall
performance score rate of improvement score
– Winners are the top scoring overall – Trend results are presented to inform
performers in each comparison group leadership decision-making. They are
not used in the selection of winners.
Watson Health © IBM Corporation 2019 23Inpatient Mortality Two years of MEDPAR data are combined for each
data point (2016, 2017)
and Complications – Includes Medicare Advantage (HMO) encounter
records
Watson Health risk models are used to produce
expected values (See methodology notes for details)
Normalized z-score is the ranked metric
– Indicates whether the observed is significantly different than
the expected value; takes into account the effect of small
numbers
Risk-adjusted index is reported (Ratio of observed to
normalized expected value)
Hospitals with statistically bad performance on one or
more of these metrics are winner excluded (See winner
exclusions)
Watson Health © IBM Corporation 2019 24Healthcare- CY 2017 data from CMS Hospital Compare 2018 Q3
Release
Associated – CMS Standardized Infection Ratio (SIR) for six healthcare-
Infections associated infections (HAIs)
– Observed HAI count for all eligible inpatient days of service
or procedures for all inpatients (eligible days/procedures vary
by HAI)
– CMS risk models are used to produce expected values
Composite measure is the mean of the included HAIs
– For each HAI, we calculate a normalized z-score
– The mean of the normalized z-scores is the ranked
composite metric
– We report the mean of the included HAI SIRs; also the
individual HAI SIRs
Included HAIs vary by comparison group, due to data
availability
– A hospital must have data for the study minimum required
number of HAIs to be in-study (See table next page)
– Medium community hospitals with only 1 of the 3 required
HAIs are in-study but winner excluded
Watson Health © IBM Corporation 2019 25Included Healthcare-Associated Infections by Comparison Group
Compare Group Included HAIs Min # HAIs
Major Teaching HAI-1, HAI-2, HAI-3, HAI-4, HAI-5, HAI-6 4
Teaching HAI-1, HAI-2, HAI-3, HAI-5, HAI-6 (SSI:Hyst 4
excluded)
Large Community HAI-1, HAI-2, HAI-3, HAI-5, HAI-6 (SSI:Hyst 4
excluded)
Medium Community* HAI-1, HAI-2, HAI-6 (CLABSI, CAUTI, C. diff 1
INCLUDED)
Small Community HAIs NOT RANKED for Small Community NA
Hospitals
* Medium community hospitals with only 1 of the 3 included HAIs are in-study
but winner excluded
HAI Name Definition
HAI-1 CLABSI Central line-associated bloodstream infections in ICUs and select wards
HAI-2 CAUTI Catheter-associated urinary tract infections in ICUs and select wards
HAI-3 SSI: Colon Surgical site infection from colon surgery
HAI-4 SSI: Hyst Surgical site infection from abdominal hysterectomy
HAI-5 MRSA Methicillin-resistant Staphylococcus aureus blood laboratory-identified events
HAI-6 C. diff Clostridium difficile laboratory-identified events (intestinal infections)
Watson Health © IBM Corporation 2019 2630-Day Mortality CMS Hospital Compare 2018 Q3 Release
– 3-years combined for each reported data point (July 1-June 30)
and Readmission – Medicare Fee For Service ONLY
Rates CMS determines pre-existing conditions for risk-
adjustment from documentation in patient claim history;
not POA coding*
– Mortality: Rates for 5 patient groups are included (heart attack, heart
failure, pneumonia, COPD, stroke)
– Readmissions: Rates for 6 patient groups are included (heart attack,
heart failure, pneumonia, THA/TKA arthroplasty, COPD, stroke)
The unweighted mean of the included mortality or
readmission rates is the ranked and reported metric
– The comparison group median value is substituted for individual
missing measures
– When all mortality rates or all readmission rates are missing, the
hospital is excluded
*Exception: CMS pneumonia mortality rates use POA codes to identify the initial
pneumonia patient cohort. The measures include patients with a principal
discharge diagnosis of sepsis (not including severe sepsis) that have a secondary
diagnosis of pneumonia (including aspiration pneumonia) coded as POA and no
secondary diagnosis of severe sepsis coded as POA.
Watson Health © IBM Corporation 2019 27Severity-Adjusted One year of MEDPAR data is used for each data point
(2017)
Average Length of – Includes Medicare Advantage (HMO) encounter records
Stay Watson Health risk models are used to produce
expected values (See methodology notes for details)
– Expected values are normalized by comparison group
We convert each LOS index (observed/normalized
expected) to average length of stay in days (ALOS) by
multiplying the index by the Grand Mean LOS of all in-
study hospitals
ALOS is the ranked and reported metric
Watson Health © IBM Corporation 2019 28Emergency CY 2017 data on emergency department (ED)
patients*, from CMS Hospital Compare 2018 Q3
Department Release
Throughput We include two ED throughput metrics that are reported
Measures in median minutes
– Time to admission
– Time to discharge for non-admitted patients
We calculate the unweighted mean of the two included
ED metrics to produce the mean ED throughput
measure, which is the ranked and reported measure
We also report the individual ED measures for
information only
*Note: CMS requires hospitals to meet a minimum sample size of
submitted records based on ED population per quarter
Watson Health © IBM Corporation 2019 29HCRIS cost report data for hospital fiscal years ending
Inpatient Expense in 2017
per Discharge We calculate inpatient expense for each hospital
department, sum the results and divide by acute
inpatient discharges
– Department-level inpatient expense is calculated by
multiplying fully allocated cost by the ratio of inpatient
charges to total charges for that department
– Expense is adjusted for area wage index and casemix
(Sourced from CMS)
– Research, non-reimbursable and subacute cost centers are
excluded
We rank and report wage- and casemix- adjusted
inpatient expense per discharge
Hospitals that are high or low outliers for this measure
are not eligible to be benchmark hospitals (IQR
methodology)
Watson Health © IBM Corporation 2019 30HCRIS cost report data for hospital fiscal years ending
Operating Profit in 2017
Margin We calculate the difference between a hospital’s total
operating revenue and total operating expense divided
by the total operating revenue
We adjust operating expense by adding the net related
organization expense (this can be a negative number)
– Where a hospital reports expense additions on worksheet G-
2 lines 30-35, with titles containing home office, related org,
or other corporate allocation text, we remove the lesser of
‘net related organization expense’ or ‘expense additions’
from total operating expense to avoid double counting net
related organization expense (Exception: where reported net
related organization expense is negative, we subtract it from total
operating expense and do not make any further adjustments)
We rank and report adjusted operating profit margin
Hospitals that are high or low outliers for this measure
are not eligible to be benchmark hospitals (IQR
methodology)
Watson Health © IBM Corporation 2019 31HCAHPS Score HCAHPS: Hospital Consumer Assessment of
Healthcare Providers and Systems inpatient survey
public data set
CMS Hospital Compare 2018 Q3 release
– All payer dataset (January 1 - December 31, 2017)
HCAHPS Score calculated for the overall rating
question (“How do patients rate the hospital, overall?”)
– For each hospital, the percentage of patients who rated the
hospital low, medium or high were multiplied by a factor of 1,
2 or 3, respectively.
– The resultant weighted percent for each rating were summed
to produce the HCAHPS Score (Max: 300)
We rank and report the HCAHPS Score
We also report individual questions for information only
Watson Health © IBM Corporation 2019 32Methodology Notes Watson Health risk-adjustment models used to develop expected values for inpatient mortality and complications; severity-adjustment model for average length of stay – Inpatient mortality model only • Excludes records with ‘Do Not Resuscitate’ (Z66; V49.86) coded as POA • Excludes patients admitted to hospice care (discharged from acute care) – All models • Include palliative care patient records (Z515; V66.7) All models use Agency for Healthcare Research & Quality (AHRQ) Clinical Classifications Software (CCS) grouping to develop rate tables for calibrating risk and severity adjustment models Watson Health © IBM Corporation 2019 33
Methodology Notes Inpatient mortality and complications expected values are normalized by multiplying them by the observed/expected ratio for each hospital’s comparison group. A z-score is calculated from each observed and normalized expected value. The z-score is the ranked metric. Inpatient mortality and complications high outliers, used for winner exclusions, are determined by finding the hospitals with statistically worse than expected results at 99% confidence that are also above the outlier group 75th percentile trim point. Length of stay (LOS) expected values are normalized by multiplying them by the observed/expected ratio for each hospital’s comparison group. The LOS Index (observed/normalized expected) is converted into average length of stay in days by multiplying by the mean LOS of the in-study population. Watson Health © IBM Corporation 2019 34
Methodology Notes
Due to high frequency of invalid POA indicator code ‘0’ in MEDPAR, we have
modified our MEDPAR data processing.
– Valid POA codes are retained (N,Y,W,U,1)
– Where invalid POA code ‘0’ appears records are processed as follows:
• All principal diagnosis codes (dx) are treated as ‘present on admission’
• All secondary dx on the CMS exempt list are treated as exempt
• Secondary dx coded ‘Y’ or ‘W’ more than 50 percent of the time in the Watson Health all-payer data
base are treated as ‘present on admission’
• All others are treated as not present on admission
Note: This reduces false positives for complications and more accurately determines the risk of death and complications,
and expected length of stay.
Watson Health © IBM Corporation 2019 35Legal Disclaimer © IBM Corporation 2019. All Rights Reserved. The information contained in this publication is provided for informational purposes only. While efforts were made to verify the completeness and accuracy of the information contained in this publication, it is provided AS IS without warranty of any kind, express or implied. In addition, this information is based on IBM’s current product plans and strategy, which are subject to change by IBM without notice. IBM shall not be responsible for any damages arising out of the use of, or otherwise related to, this publication or any other materials. Nothing contained in this publication is intended to, nor shall have the effect of, creating any warranties or representations from IBM or its suppliers or licensors, or altering the terms and conditions of the applicable license agreement governing the use of IBM software. References in this presentation to IBM products, programs, or services do not imply that they will be available in all countries in which IBM operates. Product release dates and/or capabilities referenced in this presentation may change at any time at IBM’s sole discretion based on market opportunities or other factors, and are not intended to be a commitment to future product or feature availability in any way. Nothing contained in these materials is intended to, nor shall have the effect of, stating or implying that any activities undertaken by you will result in any specific sales, revenue growth or other results. Performance is based on measurements and projections using standard IBM benchmarks in a controlled environment. The actual throughput or performance that any user will experience will vary depending upon many factors, including considerations such as the amount of multiprogramming in the user's job stream, the I/O configuration, the storage configuration, and the workload processed. Therefore, no assurance can be given that an individual user will achieve results similar to those stated here. All customer examples described are presented as illustrations of how those customers have used IBM products and the results they may have achieved. Actual environmental costs and performance characteristics may vary by customer. IBM, the IBM logo, ibm.com, and Watson Health are trademarks of International Business Machines Corp., registered in many jurisdictions worldwide. Other product and service names might be trademarks of IBM or other companies. A current list of IBM trademarks is available on the Web at “Copyright and trademark information” at ibm.com/legal/copytrade. Watson Health © IBM Corporation 2019 36
IBM's statements regarding its plans, directions and intent are subject to change or withdrawal without notice at IBM's sole discretion. Information regarding potential future products is intended to outline our general product direction and it should not be relied on in making a purchasing decision. The information mentioned regarding potential future products is not a commitment, promise, or legal obligation to deliver any material, code or functionality. Information about potential future products may not be incorporated into any contract. The development, release, and timing of any future features or functionality described for our products remains at our sole discretion. Watson Health © IBM Corporation 2019 37
Forward-Looking Statements Certain statements contained in this presentation may constitute forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. Forward-looking statements are based on the company’s current assumptions regarding future business and financial performance. These statements involve a number of risks, uncertainties and other factors that could cause actual results to differ materially, including the following: a downturn in the economic environment and client spending budgets; the company’s failure to meet growth and productivity objectives; a failure of the company’s innovation initiatives; risks from investing in growth opportunities; failure of the company’s intellectual property portfolio to prevent competitive offerings and the failure of the company to obtain necessary licenses; cybersecurity and data privacy considerations; fluctuations in financial results; impact of local legal, economic, political and health conditions; adverse effects from environmental matters, tax matters and the company’s pension plans; ineffective internal controls; the company’s use of accounting estimates; the company’s ability to attract and retain key personnel and its reliance on critical skills; impacts of relationships with critical suppliers; product quality issues; impacts of business with government clients; currency fluctuations and customer financing risks; impact of changes in market liquidity conditions and customer credit risk on receivables; reliance on third party distribution channels and ecosystems; the company’s ability to successfully manage acquisitions, alliances and dispositions; risks from legal proceedings; risk factors related to IBM securities; and other risks, uncertainties and factors discussed in the company’s Form 10-Qs, Form 10-K and in the company’s other filings with the U.S. Securities and Exchange Commission (SEC) or in materials incorporated therein by reference. The company assumes no obligation to update or revise any forward-looking statements. These charts and the associated remarks and comments are integrally related, and are intended to be presented and understood together. Watson Health © IBM Corporation 2019 38
You can also read