Hampshire and Isle of Wight ICS Population Health Summary. April 2021 - Hampshire, Southampton and Isle of Wight ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hampshire and Isle of Wight ICS
Population Health Summary.
April 2021
Contents
• Key Points
• Demographics and Life Events
• Long Term Conditions, Morbidity and Risk Factors
• Wider Determinants and Inequalities
• Picture of COVID-19
• Priorities and Local JSNA Work Programmes
Early data and evidence around the impact of COVID have been highlighted in red text,
these are not of course all inclusive and are for discussion and consideration as the
evidence of the short and long term impacts grows.
Key Points • The 10th largest ICS in the country, but estimates forecast slower resident population growth than that Nationally. • Ageing demographic – increasing frailty and multimorbidity, continue to be a big driver in health and social care needs. This is particularly expected in West Hampshire and Isle of Wight. During the first wave of the pandemic, age ≥ 70 years and male sex, increased vulnerability to COVID-19. • The population is ethnically less diverse than England but diversity is increasing. Individuals from Black and Asian ethnicities had a higher risk of COVID-19 infection compared to White individuals. • Addressing behavioural risk factors, such as smoking, unhealthy weight and physical inactivity, are important for the prevention and treatment of long term conditions. Body mass index (BMI) and specific health conditions increase the risk of a person catching coronavirus and becoming seriously unwell. • COVID-19 has exposed, exacerbated, and created health and social care needs and new inequalities. • JSNA work programme - understand how the effects of COVID have disproportionally affected different population groups across HIOW and resultant population health and social care vulnerabilities and needs.

Population & changes
• With a registered population of 1,902,230, the HIOW ICS
is the 10th largest of the 42 ICSs in the country.
• Ageing demographic – increasing frailty and
multimorbidity, this will be a big driver in health and social
care needs. This is particularly expected in West
Hampshire and Isle of Wight
• Young population structure’s in Southampton and
Portsmouth - driven by the student residents health and
social care needs would be different to that of an ageing
demographic.
Ethnicity
• 93.8% white population – Census shows population
becoming more diverse
• Diversity is greatest in the cities and north east
Hampshire
Life expectancy
• Inequalities exist within the ICS with males in the most
deprived areas living 3 yrs. less and females living 2.8
yrs. less than the most affluent areas of the ICS.
For the first time in the history of ‘patients registered at a GP’ Vital statistics - births and deaths
publication, the ICS had a decrease in the number of patient • Birth data show a steady decrease in the number of live
registrations in May 2020, and over the next 5 months till births and general fertility rate.
September 2020 (1,897,555 to 1,894,963). From October 2020, • Cancer and circulatory disease account for over half of
the number of patient registrations started to rise again, although the deaths (55%) across the ICS in 2019
there was another decrease in February 2021 (1,899,425). The
decrease in registered patients seen in these periods is likely
due to an increase in deaths, a decrease in immigration, and
potentially increased list cleansing activities brought about by
additional activities to contact vulnerable patients. Data source: NHS Digital interactive dashboard
Resident Population Projections, 2021 to 2026
(Hampshire, Southampton, Portsmouth and IOW combined)
IMPACT OF COVID-19 ON
POPULATION AGE GROUPS
Older population/care home
residents - decreased social
connectiveness through
restricted visiting, staff/visitors
wearing PPE.
Clinically vulnerable ‘conditioned
population’ social isolation -
deliveries of medication,
shopping – fears of returning to
‘normal’ following over 12 months
of isolating.
Working population ‘decreased
social connectiveness’ – remote
working from home, furloughed
staff.
Health and social care staff –
mental impact/trauma.
Young working population –
economic impact - decrease in
job opportunities
Children and Young People- ‘lost
learning generation’, missing out
on key social events. Vulnerable
children became a ‘hidden
population’ – reduced contact
with educational and health
professionals.
HIOW Population by age, sex and ethnic group
Ethnicity data are poorly recorded across health care records
and still heavily reliant on Census 2011 data.
The population is less diverse than England as a whole with
93.4% describing themselves as belonging to White ethnic
groups compared to the national average of 86.7%. The
diversity of the population is increasing, 6.2% of the
population described themselves as of an ethnic background
other than White in 2011, up from 3.1% in the previous
Census conducted in 2001.
Overall, the white population of Hampshire and Isle of Wight
has higher proportions of people in the older age groups.
Southampton and Portsmouth both have peaks in younger
age groups in their White ethnic population.
The Asian and Asian British population is younger than the
Individuals from Black and Asian
white population. The same pattern is seen in the Black and
ethnicities had a higher risk of
COVID-19 infection compared to Black British population.
White individuals.
When compared with the White population, residents
HIOW Ethnic Minority Groups and identifying as of Mixed Ethnicity are far younger in age, with
Covid-19, Rapid Needs Assessment peaks in residents aged between 0 and 4 years of age.
(Feb 2021) has been undertaken,
soon to be published
Data source: HIOW Ethnic Minority Groups and Covid-19, Rapid Needs Assessment (Feb 2021)
Life Expectancy (LE) at birth and inequality Life expectancy at birth is an estimate of the
average number of years a newborn baby would
MALE & FEMALE LE: 2017 to 2019 data MALE & FEMALE INEQUALITY IN LE: 2017 to 2019 data survive if he or she experienced the age-specific
mortality rates for that area and time period
throughout his or her life.
Across the ICS local authorities there is:
• 3 years variation in the male LE
• 2.8 years variation in the female LE
• Life expectancy for Portsmouth and
Southampton is significantly lower than the
England average
Inequality in life expectancy at birth is an
estimate of how much life expectancy varies with
deprivation and represents the range in years of life
expectancy across the social gradient from most to
least deprived
A male or female born in the most deprived areas
have lower life expectancy and live in poor health
for longer.
Across the ICS local authorities:
• A boy born today in the most deprived areas will
live on average between 6.3 years to 8.8 years
MALE: LE trend data 2010 to 2019 FEMALE: LE trend data 2010 to 2019 less compared to a boy born in a least deprived
area.
• A girl born today in the most deprived areas will
live on average between 3.0 years to 6.5 years
less compared to a boy born in a least deprived
area.
• The social gradient is greatest in Southampton.
Trends in LE
LE fluctuates vary slightly over time. Hampshire
has seen a slight increase in both male and female
LE between the recent two time periods, by 0.3
and 0.2 years respectively. Southampton males
LE has also increased by 0.3 years.
The other areas in the ICS have experienced very
small decreases between the recent time periods.
The largest decrease in LE was observed in
Southampton and Portsmouth both decreased by
0.1 years.
Healthy Life Expectancy (HLE) at birth
MALE: HLE 2016 to 2018 data FEMALE: HLE 2016 to 2018 data
Healthy life expectancy (HLE)
is the proportion of life spent in
good health. On average
females live longer than males
however they live in poor health
for longer.
Isle of Wight residents live
longer in poor health than other
authorities across HIOW.
A male or female born in the
most deprived areas has lower
life expectancy and lives in poor
health for longer.
MALE: HLE trend data 2010 to 2018 FEMALE: HLE trend data 2010 to 2018
Trends in HLE
The average years males and
females spend in good health
has fluctuated over time and
the trends vary across the
areas.
Isle of Wight data suggest that
since 2012-14 for males, and
2014-16 for females, the time
spent in good health has
decreased and is significantly
worse than England. This is
also evident for Southampton
females who spend the least
time in good health compared
to the other areas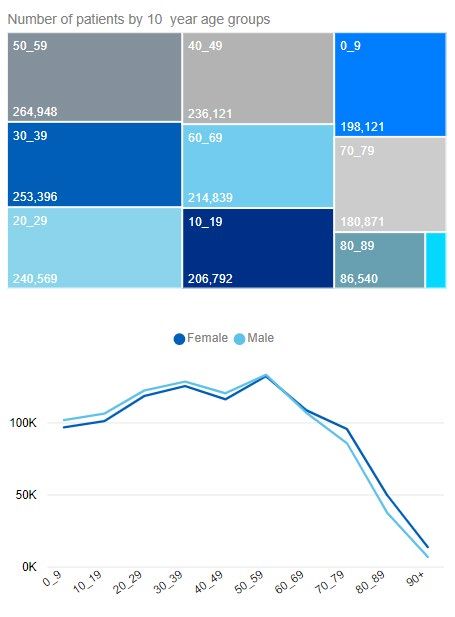
Births
In 2019 there were 19,569
live births across the ICS
Trend data from 2013 show
a steady decrease in the
number of live births and
general fertility rate*.
In line with these trends
there have been fewer
births in 2020 so far,
compared with the same
stage in 2019.
All areas have a lower
general fertility rate than
England and show a
decline over time
*General Fertility Rate (GFR) is the number of live births per 1,000 15-44yrs female population
In response to the COVID-19 pandemic, birth registration services in England and Wales were suspended in March 2020. Since June 2020, birth
registrations have restarted where it was safe to do so but the 2020 birth registration data the Office for National Statistics (ONS) has access to is
currently incomplete. However, NHS birth notification data have not been impacted by the coronavirus pandemic unlike birth registrations. The
pandemic will affect birth rates and types of care (home/hospital) and these characteristics are yet to fully manifest.
Deaths
In 2019 across the four authorities
there were there were 18,160 deaths
the main causes of deaths were:
• Cancer – 29% of deaths
• Diseases of the circulatory
system - 26% of deaths
• Diseases of the respiratory
system - 12% of deaths
• –9% of deaths
• Diseases of the nervous system -
8% of deaths
COVID-19 will impact on the causes of death
data for 2020 and 2021 death registrations.
• In February 2021 COVID-19 was the
leading cause of death in February 2021 in
England and Wales
• England recorded the highest excess
deaths in the spring 2020.
• The number of deaths involving COVID-19
were higher among men than women
• Caring, leisure and other service
occupations saw high COVID-19 death
ratesData source: NHS Digital interactive dashboard
Optimal management of long
term conditions is essential for
not only the patients own health
and wellbeing but also reduces
the risk of severe COVID-19
illness.
ICS Prevalence is higher than national
Risks
• Smoking remains the biggest preventable killer. But recording of smoking status in medical conditions across the ICS is low. It needs to be more strongly committed to tackling smoking by
improving identification, offering help and support to quit, especially for smokers admitted to hospital and in specialist mental health services
• Obesity is a priority for the ICS, - it accounts for the second highest QOF recorded prevalence rate. Targeted weight management support is key especially in obese people with Type 2
diabetes or hypertension and the challenge of keeping people active and eating healthily is a concern.
Both these risks increase the likelihood of getting severely ill from COVID-19. Obesity prevalence may have increased over the pandemic due to increasing sedentary lifestyles.
Ill health
• Across the ICS, cancer, cardiovascular disease, diabetes, respiratory disease, mental health and musculoskeletal conditions are increasing and are likely to continue to rise as they are
linked to lifestyle-related risks and an ageing demographic. The burden of multimorbidity also needs to be better managed, as does palliative care.
• Pressures are increasing, but there are significant opportunities to focus on - reducing the risk of people becoming ill or having increasing need; making use of the ICS’s assets, focusing on
prevention particularly working with the middle ages (40-64 years) adult population to promote healthy ageing, to reduce future risk of disease or to support active management of health
conditions that improve outcomes and help people retain independence for longer.
This is important because conditions such as cardiovascular disease, respiratory disease, metabolic (diabetes), renal and liver conditions, neurological and psychiatric conditions, immune and
haematological conditions and immunosuppressants, cancer conditions and treatments are known to increase the risk of becoming severely ill from COVID-19. And a number of these patients
would have been risk assessed as being clinically extremely vulnerable (CEV) and added to the Shielded Patient List (SPL).Long Term Conditions – Multi-morbidity (Southampton)
By age 80-84 over
a third (34%) have
at least 6 LTCs
By 40-44 over half
have at least 1 LTC By age 60-64 over
a third (38%) have
at least 3 LTCs
89.0% have no
LTCs at age 0-4Leading causes and risk factors of disability
Deprivation
Large variation of place based deprivation across the ICS
Hart ranked least deprived local authority in England. Southampton is the
most deprived local authority across the ICS ranked 55th nationally out of
317 local authorities (where 1 = most deprived), Portsmouth is ranked 57th.
11% (approx. 203,500 residents) of the population live in one of the 20%
most deprived areas nationally
Across the four authorities;
• a boy born today in the most deprived areas will live on average
between 6.3 years to 8.8 years less compared to a boy born in a least
deprived area.
• a girl born today in the most deprived areas will live on average
between 3.0 years to 6.5 years less compared to a boy born in a least
deprived area.
The inequality in life expectancy is greatest in Southampton for both males
and females
National analysis of wave one found that people who live in deprived areas have higher COVID-19 diagnosis rates and death rates
than those living in less deprived areas. The mortality rates from COVID-19 in the most deprived areas were more than double the
least deprived areas, for both males and females. This is greater than the inequality seen in mortality rates in previous years,
indicating greater inequality in death rates from COVID-19. Source: PHE: Disparities in the risk and outcomes from COVID-19Deprivation - Southampton
Focussing in on Southampton, the
city has a large variation in
deprivation between it’s
neighbourhoods
Whilst 12% of Southampton’s
population live in the 10% most
deprived areas nationally, this rises
to 18% for under 18s….suggesting
deprivation has a disproportionate
impact on young people in the cityDeprivation and inequalities among wider determinants
Covid cases and Covid-related mortality Cases Deaths These figures are likely to be an underestimate These figures include deaths where as1 in 3 cases are asymptomatic and may not coronavirus (COVID-19) was mentioned on the be tested for death certificate.
Hampshire and Isle of Wight Priorities
Cardiovascular Disease
• Addressing behavioural risk factors, such as smoking, unhealthy weight and physical inactivity, are important for the prevention
and treatment of CVD. Providing advice on management of behavioural risk factors is typically recommended before, or
alongside, any medical interventions.
• During the pandemic there have been excess deaths recorded due to CVD. Several behavioural risk factors have also been
found to be important in relation to CVD outcomes. Some population groups experience worse outcomes; these can relate to
socio-economic, behavioural and clinical risk factors. Action on modifiable risk factors provides an opportunity to address the
health inequalities that may have been exacerbated as a result of the pandemic.
Need to ensure better recording of lifestyle and risk factors – potential to link in with
the Health and Wellbeing coaches being recruited by PCN’s
Health and Wellbeing Coaches holistically support patients’ wider health and well-
being, public health, and contribute to the reduction of health inequalities.
CASE STUDY : Expansion of the Hampshire Healthy Hearts Programme
Programme vision
To develop an operational model for CVD prevention and to support the practical
implementation of opportunities in an equitable way.
Programme outcomes:
• Support behaviour change and promote CV health by MECC
• Optimise medication
• Extend work on cholesterol across HIOW and adapt risk review model
• Initiate work on blood pressure
• Increase technology use for diagnosis and monitoring
• Adapt programme when PCN CVD DES is published, assisting ‘struggling’
practicesHampshire and Isle of Wight ICS Priorities
• Diabetes
o Estimated 123,251 (8.1%) people with diabetes across the STP
o Significantly higher proportion of minor and major diabetic lower-limb amputation procedures across the ICS compared to England
o Higher median and adjusted length of stays for diabetic foot disease compared to England
o Risk of severe COVID-19 and complications
• Mental health
o 12.6% recorded with depression, 1.7% new diagnosis. Prevalence has increased significantly year on year since 2012/13
o 0.89% with serious mental Illness. Prevalence has remained stable over previous 3 reporting years.
o More than two-thirds of adults in the UK (69%) report feeling somewhat or very worried about the effect COVID-19 is having on their life.
The most common issues affecting wellbeing are worry about the future (63%), feeling stressed or anxious (56%) and feeling bored (49%).
o UCL report found symptoms were highest among young people, those with lower household income, people with a diagnosed mental
illness, people living with children, and people living in urban areas suggesting a possible widening of pre-existing inequalities in mental
health.
• Long Term Condition management
o Multimorbidity is often associated with reduced quality of life, higher mortality, polypharmacy and high treatment burden, higher rates of
adverse drug events, and much greater health services use (NICE Guidance QS153)
o Approximately 150,000 residents across the ICS have moderate or severe frailty and are at higher risk of adverse outcomes such as falls,
disability, admission to hospital, or the need for long-term care.
o Long COVID care and management will disproportionately fall on Primary Care, including Rehab.
• Elective/Planned Care activity
o Pandemic’s full impact on access to elective care still emerging - Recovery, backlog clearance, 18-week waiting times (waiting lists),
specialities affected Trauma & Orthopaedics, Ophthalmology, Oral surgery, Cancer. Need more radical options as services resume that are
not derailed by further waves of COVID-19.Hampshire CC and IOW JSNA Proposed Work Programme
JSNA Core Documents: Late spring to summer 2021
Demographics including protective characteristics, deprivation and life expectancy/health life expectancy
Vital Statistics – mortality and birth data
Hampshire and Isle of Wight COVID-19 Health Impact Assessment: Summer 2021
On the 11th March 2021 the World Health Organisation declared COVID-19 a pandemic, 18 months on this
report aims to look at the impact COVID-19 has had on the residents of Hampshire & IOW.
COVID-19 has exposed, exacerbated, and created new inequalities. People across the UK, and indeed the
world, have been harmed by the virus in very different ways. What has COVID-19 meant for our local
population groups and their future population health and social care needs.
JSNA Main Chapters: Autumn /Winter 2021 linked to the social
determinants of health model
Detailed JSNA Topic
reports informed by HIA Healthy People Healthy Living Healthy Places
Children and Young people - the impact •Mortality: healthy life expectancy, avoidable •Physiological risk factors: diabetes, overweight and •Access to green space: public green space,
COVID-19 has had on this generation. deaths obesity in adults, hypertension private outdoor space
Obesity, smoking, physical activity, substance •Physical health conditions: dementia, •Behavioural risk factors: alcohol misuse, drug •Local environment: air pollution, transport
misuse, mental health, learning disabilities, musculoskeletal conditions, respiratory misuse, smoking, physical activity, healthy eating noise, neighbourhood noise, road safety, road
diabetes, cancer, heart/cardiac, conditions, cardiovascular conditions, cancer, •Unemployment traffic volume
lung/respiratory, heart, kidney/renal, kidney disease •Working conditions: job-related training, low pay, •Access to housing: household overcrowding,
neurological), musculoskeletal, •Difficulties in daily life: disability that impacts workplace safety rough sleeping, housing affordability
gastrointestinal, long-COVID, rehabilitation, daily activities, difficulty completing activities •Risk factors for children: infant mortality, children’s •Access to services: distance to GP services,
maternity/pregnancy, screening & of daily living (ADLs), frailty social, emotional and mental health, overweight distance to pharmacies, distance to sports or
immunisation, end of life, air quality & •Personal well-being: life satisfaction, life and obesity in children, low birth weight, teenage leisure facilities
climate change, medicines worthwhileness, happiness, anxiety pregnancy, child poverty, children in state care •Crime: personal crime, Mental well-being
management(steroids). •Mental health: suicides, depression, self-harm •CYP education: young people’s education, tool, Social isolation
employment and training, pupil absence, early years
development, GCSE achievement
Demography •Protective measures: cancer screening, vaccination
including protective coverage, sexual health
characteristics
Inequalities: age, ethnicity, religion, learning or physical disability, sex, sexual orientation,Hampshire and Isle of Wight Priorities: HIA
COVID-19 has exposed, exacerbated, and created health There are a range of actions that are needed if we
and social care needs and new inequalities. People across are to robustly address the inequalities observed
during COVID-19. There is an absolute need to do
the UK, and indeed the world, have been harmed by the more, and focus on the specifics of the pandemic
virus in very different ways. We need to understand how response, but we must also use this opportunity to
the effects of COVID-19 have disproportionally affected have a robust conversation about how we tackle
these inequalities longer term. We cannot continue
different population groups across HIOW (age, gender, to accept these inequalities as inevitable*.
ethnicity, occupations, co-morbidities, deprivation).
To date;
• Over 63,200 residents of Hampshire and 6,700 Isle of Just as COVID-19 has
exacerbated existing
Wight residents have tested positive for COVID-19.
inequalities in other
o Using ONS estimates this equates to approximately parts of life, access to
7,000 people across the Hampshire and IOW with Long elective treatment
COVID symptoms. fell further in the
• Across the 4 trusts 12,249 patients have been admitted most deprived areas
of England during
to hospital for COVID-19.
2020 than in less
o National analysis suggest patients in hospital with deprived areas. Far
COVID-19 experienced elevated rates of metabolic, more people are now
cardiovascular, kidney and liver disease compared with waiting longer for
patients of similar demographic and clinical profiles over treatment*.
the same period
o The rates of diabetes and cardiovascular disease were
particularly pronounced among patients. *ADPH Guidance: Living Safely with Covid: Moving toward a Strategy for Sustainable Exit from the Pandemic – ADPH
Longer waits, missing patients and catching up | The Health FoundationFurther resources • HIOW STP JSNA (2019) can be accessed here • Southampton Data Observatory can be accessed here • Hampshire PCN data packs can be accessed here • Hampshire JSNA pages can be accessed here
You can also read