What's New In The 2nd Edition?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
What's New In The 2nd Edition?

Disclosure Statement • Faculty: • Jill Boulton • Kevin Coughlin • Deepak Manhas We have no affiliation (financial or otherwise) with a pharmaceutical, medical device or communications organization

Our Thanks To:
• Co Editors ACoRN 2021: • ACoRN Steering and Education
• Jill Boulton Committee Members
• Kevin Coughlin • Many many other contributors and
• Debra O’Flaherty reviewers
• Alfonso Solimano
• Tireless ACoRN instructors in
• Major Contributors: Canada and around the world
• Debbie Aylward
• Deepak Manhas
• CPS Staff
• Jackie Millette
• Elene Vanderpas
• Keisha Powell
• French Edition Contributors: • Jennifer Strickland
• Ahmed Moussa
• Genevieve Piuze
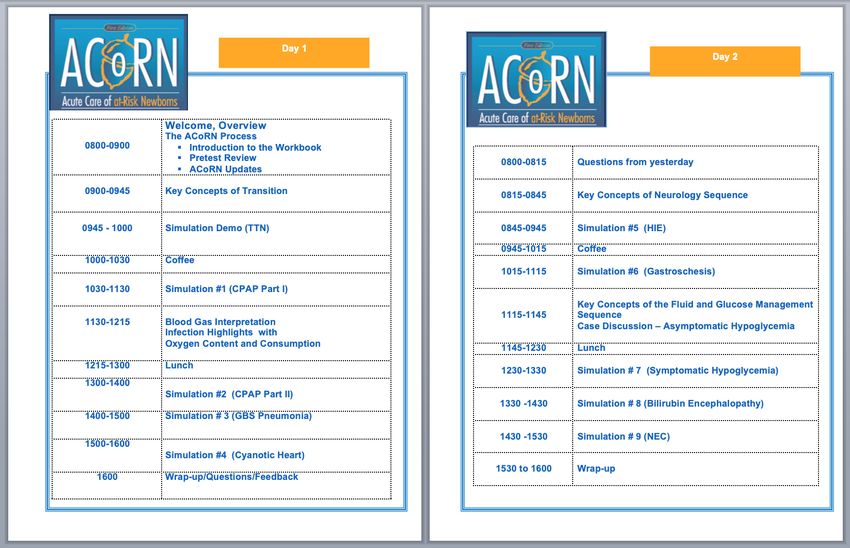
Agenda • The history of ACoRN • Highlight what’s new in the second edition • Present the ACoRN educational approach • Discuss what’s next? • Provincial and regional launches • CPS Practice Point
The history of ACoRN Jill Boulton, MD

From NRP Steering Committee breakfast
at CPS annual meeting, Winnipeg 1999…
2015
X3
Huntsville 1999
I think I get it
Calgary 2003
Explain How that
works again ?
Baby at risk
Unwell
Risk factors
Post-resuscitation
requiring stabilization
Resuscitation Support
Ineffective breathing
Heart rate < 100 bpm
Central cyanosis
Infection
Risk factor for infection
ACoRN alerting sign with *
Clinical deterioration
Respiratory Thermoregulation
Laboured respiration* T < 36.3 or > 37.2ºC axillary*
Respiratory rate > 60/min* Increased risk for
Receiving respiratory support* temperature instability
Problem List
Respiratory
Cardiovascular
Neurology
Surgical conditions
Cardiovascular Fluid & glucose Fluid & Glucose Management
Pale, mottled, or grey* Thermoregulation Blood glucose < 2.6 mmol/L
Weak pulses or low BP* Infection At risk for hypoglycemia
Cyanosis unresponsive to O2 Not feeding or should not be fed
Heart rate > 220 bpm
Sequences
Consider transport
Neurology Surgical Conditions
Abnormal tone* Anterior abdominal wall defect
Jitteriness Vomiting or inability to swallow
Seizures* Abdominal distension
Delayed passage of meconium
or imperforate anus
2012 2021
7
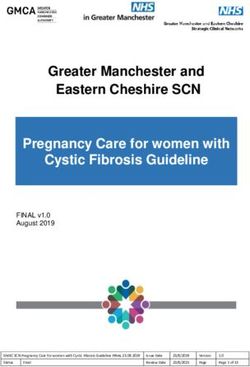
• Remains prioritized based around Primary Survey • Updates to clarify, add missing information asked for (i.e. HIE management, neural tube defects and jaundice) • Sequences maintain same structure ‘ACORNS’ • Two new chapters: • Transition • Jaundice
Primary Survey *
*
*Consolidated Core Steps • Creation of the Consolidated Core Steps (CCS) to better fit with actual practice and decrease repetition between sequences • CCS are now performed in parallel with the Primary Survey by a second ACoRN provider
• Level of Risk identification: • Consider consultation/transport
Alerting Signs
*
*
*
* *
* *
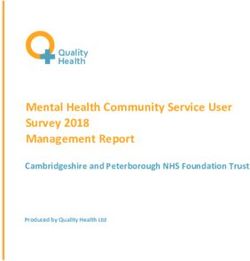
*7 new, 7 altered Alerting
• Sequence Signs:
New Alerting Sign Replaces
Resuscitation Apnea, gasping or ineffective Ineffective breathing
breathing
Respiratory Receiving CPAP or ventilation* Receiving respiratory support
Cardiovascular Failed CCHD screen
Neurology Abnormal tone or activity* Abnormal tone*
Abnormal level of alertness*
Abnormal movements* Jitteriness/ Seizures*
At risk for HIE
Surgical Conditions Neural tube defect
Fluid & Glucose Unwell, not feeding, or should Not feeding or should not be fed
not be fed
Jaundice At risk for jaundice
Visible jaundice
Bilirubin at treatment level
Thermoregulation T 37.5℃ axillary* T 37.2℃ axillary*
HIE managementChapters • Critical knowledge and physiology points at start of each chapter rather than presented in cases • Useful tools for many of the sequences • Cases continue to illustrate flow through the ACoRN Process and Level of Risk determination
Sequences • Reorganized with most acute/serious condition on the far left • Some additional qualifiers to alter Organization of Care after Core Steps (e.g. glucose level in Neurology Sequence)
Sequences • No significant change to Next Steps • Still point where you exit the sequence on first run through to address next item on Problem List • Consider the Level of Risk for each sequence • Patients final level of risk is highest achieved in any sequence
What's new in the
2nd edition?
Kevin Coughlin, MDOrientation to ACoRN Sequences
• Overall flow and structure of the
sequences has not changed
• Streamlined the Core Steps
• Re-organized Organization of Care so
most urgent is to the left of the
sequence
• First exit still at Next Steps
• Addition of Level of Risk assessment for
each sequenceResuscitation • Simplified • In line with ILCOR/NRP
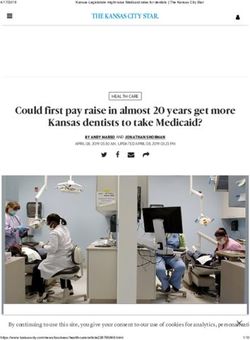
Respiratory • Respiratory support clarified as CPAP or ventilation • SpO2 targets updated to 90-95% • Respiratory Score remains the primary decision aid for Organization of Care • Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process
Respiratory • Respiratory support clarified as CPAP or ventilation • SpO2 targets updated to 90-95% • Respiratory Score remains the primary decision aid for Organization of Care • Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process
Respiratory • Respiratory support clarified as CPAP or ventilation • SpO2 targets updated to 90-95% • Respiratory Score remains the primary decision aid for Organization of Care • Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process
Respiratory • Respiratory support clarified as CPAP or ventilation • SpO2 targets updated to 90-95% • Respiratory Score remains the primary decision aid for Organization of Care • Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process
Core Steps: Respiratory Score • No major changes to previous respiratory score
Cardiovascular • Added failed CCHD screen • Clinical Assessment of Circulation table is primary decision aid for Organization of Care • Differentiation of shock vs circulatory instability without shock
Cardiovascular • Added failed CCHD screen • Clinical Assessment of Circulation table is primary decision aid for Organization of Care • Differentiation of shock vs circulatory instability without shock
Cardiovascular • Added failed CCHD screen • Clinical Assessment of Circulation table is primary decision aid for Organization of Care • Differentiation of shock vs circulatory instability without shock
Cardiovascular • Added failed CCHD screen • Clinical Assessment of Circulation table is primary decision aid for Organization of Care • Differentiation of shock vs circulatory instability without shock
Core Steps: Clinical Assessment of Circulation
Neurology • Updated Alerting Signs including abnormal level of consciousness and ‘At risk for HIE’ • Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care • Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE • Includes direction for HIE management
Neurology • Updated Alerting Signs including abnormal level of consciousness and ‘At risk for HIE’ • Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care • Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE • Includes direction for HIE management
Neurology • Updated Alerting Signs including abnormal level of consciousness and ‘At risk for HIE’ • Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care • Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE • Includes direction for HIE management
Neurology • Updated Alerting Signs including abnormal level of consciousness and ‘At risk for HIE’ • Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care • Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE • Includes direction for HIE management
Core Steps: Encephalopathy Assessment Table
Surgical Conditions • Addition of open neural tube defect to
Fluid & Glucose • Sequence is harmonized with CPS statement on hypoglycemia management • Balanced between appropriate treatment and maintaining breast feeding
Fluid & Glucose • Introduces simplified GIR calculation and maximal recommended fluid intakes to avoid dilutional hyponatremia • Stepwise treatment recommendations
Fluid & Glucose • Introduces simplified GIR calculation and maximal recommended fluid intakes to avoid dilutional hyponatremia • Stepwise treatment recommendations
Jaundice Sequence • New sequence to ACoRN introduced at providers’ request • 3 new Alerting Signs • Core Step involved plotting bilirubin values on standardized curves • Organization of Care depends on plotted results
Jaundice Sequence • New sequence to ACoRN introduced at providers’ request • 3 new Alerting Signs • Core Step involved plotting bilirubin values on standardized curves • Organization of Care depends on plotted results
Jaundice Sequence • New sequence to ACoRN introduced at providers’ request • 3 new Alerting Signs • Core Step involved plotting bilirubin values on standardized curves • Organization of Care depends on plotted results
Jaundice Sequence • New sequence to ACoRN introduced at providers’ request • 3 new Alerting Signs • Core Step involved plotting bilirubin values on standardized curves • Organization of Care depends on plotted results
Thermoregulation • Updated temperature range: 36.5-37.5℃ • Added HIE management as both an Alerting Sign and Response
Thermoregulation • Updated temperature range: 36.5-37.5℃ • Added HIE management as both an Alerting Sign and Response
Infection Sequence • Alerting Signs remain the same • Reorganized based on the Infection Assessment Table • Additional information in the chapter on common organisms causing EOS and LOS, biomarkers, non-bacterial causes of infection
Core Steps: Infection Assessment Table
The ACoRN Program Additional Tools & Resources: • Additional resource and tables in the textbook & appendices • ACoRN: The Essential Guide • The ACoRN Workbook • ACoRN Simulations • ACoRN Key Concepts • ACoRN Skills
Resources for the ACoRN Instructor/Provider
• ACoRN: The Essential Guide
• ’coles notes’ version of the text
• forms essential materials in the
reading lists we used to provide to
those coming to an ACoRN course
• meant to supplement the
textbook
• option for those providers who
use an institutional library copy of
the textbookResources for the ACoRN Instructor/Provider
• The ACoRN Workbook
• Replaces the laminates used
in the past
• Useful in the moment
• Include primary survey &
consolidated core steps,
sequences, core steps and
useful tools to navigate the
ACoRN processResources for the ACoRN Instructor/Provider
• ACoRN Key Concepts
• Brief 30 min talks
• Outline key learning concepts
• Developed/used based on need
• Anchors within the course agenda
• Examples:
• ACoRN 2nd Edition Updates
• Key Concepts of Transition
• Key Concepts of Neurology Sequence
• Key Concepts of Fluid & Glucose
SequenceResources for the ACoRN Instructor/Provider
• ACoRN Simulations
• Key component of the ACoRN
program
• Series of purpose-built simulation
scenarios to help instructor
navigate ACoRN providers through
learning the process
• 9-10 developed to date
• Template will be available to
instructors to develop your ownResources for the ACoRN Instructor/Provider
• ACoRN Skills
• Yet to be developed
• Many can be reused from past
edition
• Targeted to course/provider based
on need
• Chest Radiograph Interpretation
• Vascular Access (IO/UVC)
• Needle Thoracocentesis
• Chest Tube Insertion
• Blood Gas Interpretation
• CBCD InterpretationACoRN educational
approach
Deepak Manhas, MDEducational Supplements
• Updated Textbook Cases
• Pre-Test
• Draft Agenda
• Workbook
• Laminates
• Simulation Scenarios
• Case
• Equipment and Images
• Debriefing
• Demo VideoACoRN Workbook • ACoRN Algorithms • ACoRN Tables • Level of Risk
Demo simulation video coming soon to pedagogy@cps.ca
Administration of
ACoRN in Canada
Kevin Coughlin, MDACoRN Providers and Instructors
• Will follow a process similar to NRP
• 3-year renewal process
• Online exam prior to attending a course
• Requirement for teaching to maintain status as Instructor
• ACoRN is meant to be taught in a multidisciplinary team
• Within the teaching team, the content knowledge and skills must be present
to teach the entire core content of the ACoRN course
• Current ACoRN Instructors who have taught within the last 3 years
(before COVID) will be eligible for update and renewal of statusACoRN Courses • Flexibility in how ACoRN is taught • There will be clearly identified core content that is necessary for a complete course • Additional materials will be provided for Instructors to use as add on modules based on a site/provider groups’ needs • Instructor resources including “Key Concepts” videos, Simulation and Debrief guides etc will be on the Instructor side of the ACoRN website
Newborn Stabilization in Canada • It is recognized that newborn stabilization skills are variable across the country. • CPS Practice Point in process identifying the need for a standard stabilization program (similar to NRP) across the country.
ACoRN: The Vision
• ACoRN 2nd Edition is an update of the already fabulous ACoRN Program
• Move to more of a simulation-based content delivery
• Increased interactive nature with participant driven learning through
simulation, debrief and reflection
• Standardization and support of educational quality through the Key
Concepts anchoring talks and Simulation Scenarios
• Increased flexibility in design and delivery of the content
• Modular components with identified ‘Core Content’ and additional resources
available to Instructors as needed based on site/learners needs
• Evaluation and assessment through online pretest and participation in
simulationsImplementation Across the Country • Rolling out the new edition has been complicated by COVID • The change to increase the hands on, intensively simulation-based group learning nature of the 2nd edition pedagogy in this environment is further complicating things • Plan to reach out to each Regional/Provincial body to see how we can best support Instructor updates and roll out of the 2nd edition in the early fall. • We welcome your thoughts on how this can best be done
ACoRN: The Vision • Goal today: to highlight the newly developed content for you, a group of experienced ACoRN Instructors/Providers • We welcome feedback on things that you think will work and opportunities for improvement • We thank you, in advance, for your participation!
Questions and Comments?
You can also read