Original Article Association of gestational diabetes mellitus with preeclampsia: a retrospective cohort study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Int J Clin Exp Med 2021;14(1):573-580 www.ijcem.com /ISSN:1940-5901/IJCEM0120902 Original Article Association of gestational diabetes mellitus with preeclampsia: a retrospective cohort study Shuyan Qu1*, Liyuan Dong2* Departments of 1Endocrinology, 2Gynaecology and Obstetrics, Daqing Oilfield General Hospital, Daqing, Heilongjiang Province, China. *Equal contributors and co-first authors. Received August 23, 2020; Accepted October 19, 2020; Epub January 15, 2021; Published January 30, 2021 Abstract: Objective: To explore the impact of gestational diabetes mellitus (GDM) on preeclampsia. Methods: Singleton pregnant women who registered in our hospital between January 2010 and January 2020 were enrolled in this retrospective cohort study. GDM is diagnosed according to the criteria of the International Association of Diabetes and Pregnancy Study Groups Consensus. Univariate and multivariate logistic regression analyses were conducted to estimate the relative risk between GDM and preeclampsia. Results: Among the 800 singleton preg- nancy women analyzed, 66 (8.25%) was diagnosed with GDM. We found that women with GDM had a higher risk of developing preeclampsia than women with non-GDM (12.12% vs. 4.09%, P
Association of gestational dabetes mellitus with preeclampsia
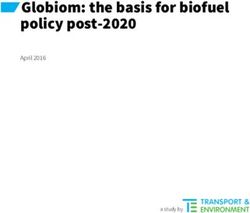
Figure 1. Study flowchart.
Pregnancy Study Groups Consensus [12]. obtain approval from an ethics committee of a
Briefly, GDM received a 75 g oral glucose toler- Daqing Oilfield General Hospital. The study
ance test (OGTT) between 24 and 28 weeks received no special funding from funding agen-
gestation and they had fasting blood glucose cies in the public, commercial or non-profit
≥5.1 mmol/L (92 mg/dL), 1-hour plasma glu- sectors.
cose ≥10.0 mmol/L (180 mg/dL) and 2-hour
plasma glucose ≥8.5 mmol/L (153 mg/dL). Statistical analysis was performed using Stata
13.0 software (Stata Corp, USA). Continuous
Preeclampsia was diagnosed at 20 to 39 weeks variables were compared using student T-test
of gestation and confirmed as preeclampsia if or Mann-Whitney U test. The Chi-square test
the pregnant women had systolic or diastolic and Fisher’s exact test were used to compare
blood pressure of >140/90 mmHg and 24 h uri- categorical variables. Associations between
nary albuminuria >300 mg [13]. GDM and the risk of preeclampsia were tested
Inclusion criteria: Singleton pregnant women by univariate analysis and multivariate logistic
who successfully live delivery in a hospital. regression analysis. The dependent variable
Exclusion criteria: pregnant women with type 1 that we studied was preeclampsia. Results of
or type 2 diabetes mellitus diagnosed before logistic regression were expressed as adjusted
pregnancy; pregnant women with hypertension OR with the 95% confidence interval (CI), and
or cardiovascular disease diagnosed before potential confounders include age, pregnancy
pregnancy; pregnant women with a history of a BMI, education level, folic acid supplement,
serious systemic disease, such as cirrhosis, dyslipidemia, family history of hypertension
severe anemia, chronic renal failure or immune and polycystic ovary syndrome. PAssociation of gestational dabetes mellitus with preeclampsia
Table 1. Demographics and pregnancy characteristics data
No. of pregnant No preeclampsia Preeclampsia
P value
women (n = 800) (n = 762, [95.25%]) (n = 38, [4.75%])
Age 800 30.62±4.94 31.24±4.17 0.451
Pregnancy BMI (kg/m2) 800 20.99±2.84 23.31±2.10 0.000
Pregnancy BMI (kg/m2) 0.002Association of gestational dabetes mellitus with preeclampsia Table 2. Assignment of related factors Relevant factor Variable assignment Age Continuous variables Pregnancy BMI (kg/m2)
Association of gestational dabetes mellitus with preeclampsia
Table 4. Multivariate risk analyses for preeclampsia
Preeclampsia Multivariate analysis
(n = 38, [4.75%]) Adjusted OR (95% CI) P Value
Age 38 1.04 (0.96-1.11) 0.352
Pregnancy BMI (kg/m2) 0.007Association of gestational dabetes mellitus with preeclampsia
ed with preeclampsia (1.26 [1.06-1.50]) [14]. established in this study has high predictive
At present, the reason for the higher risk of pre- value.
eclampsia in patients with gestational diabetes
is still unclear. Beysel et al. reported that the Through this retrospective cohort study, we
HNF1αp.I27L TT genotype was associated with explored the association between gestational
preeclampsia risk in patients with GDM [15]. A diabetes and preeclampsia, and adjusted the
study suggests that GDM combined with pre- influence of confounding factors on the out-
eclampsia may be involved in the endothelial come. But there are still some limitations in our
injury [16]. On the other hand, patients with research. Firstly, this study is a retrospective
GDM have a higher risk of preeclampsia, which cohort study, there may be bias in the process
might be related to insulin resistance [17]. of collecting patient data, which may affect the
accuracy of the results. Secondly, although our
Compared with pregnant women and with nor- study shows that gestational diabetes is asso-
mal blood lipid level, pregnant women with dys- ciated with preeclampsia, the sequential rela-
lipidemia were more likely to develop pre- tions between preeclampsia and GDM remains
eclampsia. Cao et al. found that pregnant wom- unclear. Thirdly, we don’t know whether patients
en’s dyslipidemia is related to GDM and pre- with GDM can effectively control their blood
eclampsia [16]. In a study done by Kandimalla, sugar, and we cannot compare the effect of
et al., 156 pregnant women were included prior blood sugar control on the results. Fourthly, we
to 20 weeks of gestation and their lipid levels adjusted the impact of some confounding fac-
were detected. They found that the mean TG tors on the results, but there may still be some
levels were found to be significantly higher in confounding factors missing.
the preeclampsia group, and women with TG
In summary, GDM, pre-pregnancy BMI ≥25 kg/
levels above 130 mg/dL had an increased risk
m2 and dyslipidemia are significantly associat-
of developing preeclampsia compared with
ed with preeclampsia. Pregnant women with
those with TG levels of 91 mg/dL or less [18]. A
GDM or who are obese before pregnancy or
retrospective analysis of 9911 pregnant women
dyslipidemia have a significantly increased risk
found that dyslipidemia was significantly asso- of developing preeclampsia. We suggest that
ciated with preeclampsia after adjustment for patients with GDM should be actively tested for
confounding factors [19]. preeclampsia, and it is recommended to reduce
weight and regulating dyslipidemia before preg-
Studies from different populations have consis-
nancy to reduce the risk of preeclampsia.
tently reported that elevated pre-pregnancy
BMI is associated with an increased risk of pre- Disclosure of conflict of interest
eclampsia [20-26]. Our study found that the
risk of preeclampsia in women with pre-preg- None.
nancy BMI ≥25 kg/m2 is 3.15 times than that of
those with pre-pregnancy BMIAssociation of gestational dabetes mellitus with preeclampsia
[3] Charlton F, Tooher J, Rye KA and Hennessy A. [14] Hiersch L, Berger H, Okby R, Ray JG, Geary M,
Cardiovascular risk, lipids and pregnancy: pre- McDonald SD, Murray-Davis B, Riddell C, Hal-
eclampsia and the risk of later life cardiovas- perin I, Hasan H, Barrett J and Melamed N.
cular disease. Heart Lung Circ 2014; 23: 203- Gestational diabetes mellitus is associated
212. with adverse outcomes in twin pregnancies.
[4] Yang JJ, Lee SA, Choi JY, Song M, Han S, Yoon Am J Obstet Gynecol 2019; 220: 102.e1-102.
HS, Lee Y, Oh J, Lee JK and Kang D. Subsequent e8.
risk of metabolic syndrome in women with a [15] Beysel S, Pinarli FA, Eyerci N, Kizilgul M, Hep-
history of preeclampsia: data from the Health sen S, Alhan A, Kan S, Caliskan M, Bozkurt E
Examinees Study. J Epidemiol 2015; 25: 281- and Cakal E. HNF1A gene p.I27L is associated
288. with co-existing preeclampsia in gestational
[5] Hartling L, Dryden DM, Guthrie A, Muise M, diabetes mellitus. Gynecol Endocrinol 2020;
Vandermeer B, Aktary WM, Pasichnyk D, Seida 36: 530-534.
JC and Donovan L. Screening and diagnosing [16] Cao W, Wang X, Chen T, Xu W, Feng F, Zhao S,
gestational diabetes mellitus. Evid Rep Technol Wang Z, Hu Y and Xie B. Maternal lipids, BMI
Assess (Full Rep) 2012; 1-327. and IL-17/IL-35 imbalance in concurrent gesta-
[6] Hiersch L and Yogev Y. Impact of gestational tional diabetes mellitus and preeclampsia. Exp
hyperglycemia on maternal and child health. Ther Med 2018; 16: 427-435.
Curr Opin Clin Nutr Metab Care 2014; 17: 255- [17] Mate A, Blanca AJ, Salsoso R, Toledo F, Stiefel
260. P, Sobrevia L and Vázquez CM. Insulin therapy
[7] Metzger BE, Lowe LP, Dyer AR, Trimble ER, in pregnancy hypertensive diseases and its ef-
Chaovarindr U, Coustan DR, Hadden DR, fect on the offspring and mother later in life.
McCance DR, Hod M, McIntyre HD, Oats JJ, Curr Vasc Pharmacol 2019; 17: 455-464.
Persson B, Rogers MS and Sacks DA.
[18] Kandimalla BH, Sirjusingh A, Nayak BS and
Hyperglycemia and adverse pregnancy out-
Maiya SS. Early antenatal serum lipid levels
comes. N Engl J Med 2008; 358: 1991-2002.
and the risk of pre-eclampsia in Trinidad and
[8] Aviram A, Guy L, Ashwal E, Hiersch L, Yogev Y
Tobago. Arch Physiol Biochem 2011; 117: 215-
and Hadar E. Pregnancy outcome in pregnan-
221.
cies complicated with gestational diabetes
[19] Wiznitzer A, Mayer A, Novack V, Sheiner E, Gi-
mellitus and late preterm birth. Diabetes Res
lutz H, Malhotra A and Novack L. Association of
Clin Pract 2016; 113: 198-203.
lipid levels during gestation with preeclampsia
[9] Klemetti M, Hiltunen LM, Heino S, Heinonen S,
and gestational diabetes mellitus: a popula-
Kajantie E and Laivuori H. An obesity-related
tion-based study. Am J Obstet Gynecol 2009;
FTO variant and the risk of preeclampsia in a
Finnish study population. J Pregnancy 2011; 201: 482 e481-488.
2011: 251470. [20] Wei YM, Yang HX, Zhu WW, Liu XY, Meng WY,
[10] Chan SE, Pudwell J and Smith GN. Effects of Wang YQ, Shang LX, Cai ZY, Ji LP, Wang YF, Sun
preeclampsia on maternal and pediatric health Y, Liu JX, Wei L, Sun YF, Zhang XY, Luo TX, Chen
at 11 years postpartum. Amer J Perinatol HX and Yu LJ. Risk of adverse pregnancy out-
2019; 36: 806-811. comes stratified for pre-pregnancy body mass
[11] Košir Pogačnik R, Trojner Bregar A, Lučovnik index. J Matern Fetal Neonatal Med 2016; 29:
M, Krajec M, Verdenik I, Blickstein I and Tul N. 2205-2209.
The effect of interaction between parity, gesta- [21] Vinturache A, Moledina N, McDonald S, Slater
tional diabetes, and pregravid obesity on the D and Tough S. Pre-pregnancy Body Mass In-
incidence of preeclampsia. J Matern Fetal Neo- dex (BMI) and delivery outcomes in a Canadi-
natal Med 2020; 33: 931-934. an population. BMC Pregnancy Childbirth
[12] International Association of Diabetes and 2014; 14: 422.
Pregnancy Study Groups Consensus Panel, [22] Fox NS, Roman AS, Saltzman DH, Klauser CK
Metzger BE, Gabbe SG, Persson B, Buchanan and Rebarber A. Obesity and adverse pregnan-
TA, Catalano PA, Damm P, Dyer AR, Leiva Ad, cy outcomes in twin pregnancies. J Matern Fe-
Hod M, Kitzmiler JL, Lowe LP, McIntyre HD, tal Neonatal Med 2014; 27: 355-359.
Oats JJ, Omori Y and Schmidt MI. International [23] Paré E, Parry S, McElrath TF, Pucci D, Newton A
association of diabetes and pregnancy study and Lim KH. Clinical risk factors for preeclamp-
groups recommendations on the diagnosis sia in the 21st century. Obstet Gynecol 2014;
and classification of hyperglycemia in pregnan- 124: 763-770.
cy. Diabetes Care 2010; 33: 676-682. [24] Liu L, Hong Z and Zhang L. Associations of pre-
[13] Weissgerber TL and Mudd LM. Preeclampsia pregnancy body mass index and gestational
and diabetes. Curr Diab Rep 2015; 15: 9. weight gain with pregnancy outcomes in nul-
579 Int J Clin Exp Med 2021;14(1):573-580Association of gestational dabetes mellitus with preeclampsia
liparous women delivering single live babies. [26] Swank ML, Marshall NE, Caughey AB, Main EK,
Sci Rep 2015; 5: 12863. Gilbert WM, Melsop KA and Chung JH.
[25] Baker AM and Haeri S. Estimating risk factors Pregnancy outcomes in the super obese, strat-
for development of preeclampsia in teen moth- ified by weight gain above and below institute
ers. Arch Gynecol Obstet 2012; 286: 1093- of medicine guidelines. Obstet Gynecol 2014;
1096. 124: 1105-1110.
580 Int J Clin Exp Med 2021;14(1):573-580You can also read