WALKING THE TALK ON SUSTAINABILITY | P6 - Association of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

T H E M AG A Z I N E O F T H E A S S O C I AT I O N O F S A L A R I E D M E D I C A L S P E C I A L I S T S 124 | SEPTEMBER 2020
WALKING THE TALK ON SUSTAINABILITY | P6
THE GAP BETWEEN HEALTH POLICY
AND DELIVERY | P10
HOW THE PARTIES STACK UP | P13
INSIDE
THIS
ISSUE
ISSUE 124 | SEPTEMBER 2020
WANT TO KNOW MORE?
Find our latest resources and
information on the ASMS website
www.asms.org.nz or follow us on
Facebook and Twitter.
Also look out for our ASMS Direct
email updates.
03 WE NEED A STRONG UNIFIED VOICE ON HEALTH CARE
This magazine is published by the
Association of Salaried Medical
05 KINDNESS IS EASY TO SAY BUT HARD TO DO
06
Specialists and distributed by post and
email to union members. WALKING THE TALK ON SUSTAINABILITY
Executive Director: Sarah Dalton
Magazine Editors: Elizabeth Brown 09 HOW THE HEALTH SYSTEM IS BEING SHORT-CHANGED BY ACC
and Lydia Schumacher
Designer: Dink Design 10 CLOSING THE GAP BETWEEN HEALTH POLICY AND DELIVERY
If you have any feedback on the
magazine or contribution ideas, please
get in touch at asms@asms.org.nz.
12 SIMPSON REPORT: A DISSENTING VIEW - PETER CRAMPTON
PREFER TO READ THE 13 HOW THE PARTIES STACK UP
SPECIALIST ONLINE?
We have listened to your feedback
14 A MULTI-MEDIA HUI FOR BRANCH OFFICERS
and are aware that some members
prefer not to receive hard copies 15 COVID-19 SHINES A LIGHT ON OCCUPATIONAL MEDICINE
of the magazine. If you want to
opt out of the hard copy, just email
membership@asms.nz and we can
17 IMGS IN FOCUS
let you know via email when the next
issue is available to read online. 18 ASMS WORKING BRIEFS
19 WILL WE GO BACK TO OUR LOVE AFFAIR WITH JET TRAVEL?
BOOK REVIEW – THE BAREFOOT SURGEON
20
The Specialist is produced with the generous
support of MAS.
NEW FACE FOR THE SOUTH
ISSN (Print) 1174-9261
ISSN (Online) 2324-2787
21 WOMEN IN MEDICINE
22 FIVE MINUTES WITH DR ROGER WANDLESS
The Specialist is printed on Forestry
Stewardship Council® (FSC®) certified paper
24 INDEMNITY CLAUSES IN EMPLOYMENT CONTRACTS
25 ASMS HEALTH SOLIDARITY
26 BY THE NUMBERS
DR PETER STORMER
REMEMBERING A VISIONARY AND HIS GIFT
2 THE SPECIALIST | SEPTEMBER 2020
WE NEED A STRONG
UNIFIED VOICE ON
HEALTH CARE
PROF MURRAY BARCLAY | ASMS NATIONAL PRESIDENT
O ne thing the Covid-19 pandemic has done is to sharpen the focus on our health system’s shortcomings. Most notable have been
the dangerously low number of public health specialists and the shortage of ICU beds and ICU specialists compared to other
similar countries. There is little doubt our hospitals would have been overwhelmed without our Covid-19 elimination policy, and our
ability to deal with our usual patient demands would have suffered badly. However, the deficiencies highlighted by Covid-19 reflect
deficiencies across all specialist areas, resulting from more than 10 years of underinvestment in health care.
Another result of systemic mismanagement but by government and staff/management culture at CDHB
underinvestment, and the Ministry Ministry policy) has seen a tragic series of developed over more than a decade.
ignoring clinician advice and placing events culminating in the loss of arguably This tragedy appears to be the result of
cost-cutting ahead of patient care, is the the most highly regarded DHB executive poor leadership at the highest levels, i.e.
situation now occurring at Canterbury management team in the country. The government and Ministry.
DHB (CDHB). The Ministry appointments strident and unified support for this EMT This poor leadership and underinvestment
of Crown Monitor Lester Levy and Board by all CDHB staff and the public, and the in health is also manifest in fragmentation
Chair John Hansen to slash the CDHB disdain for the decisions of the Hansen- and disunity at all levels of health care
deficit (which was generated not by CDHB led Board, is a testament to the fantastic around New Zealand. When everyone
WWW.ASMS.ORG.NZ | THE SPECIALIST 3
is fighting for the scraps, the natural see exactly what needed to be done and strengthen the health voice nationally for
tendency is to fend for oneself. DHB his priorities were good. He was, however, our patients.
chief executives seem not to have united quickly derailed by Ministry officials with
You will have noted that ASMS recently
views around the country; individual faulty logic, plus the Labour Government’s
ran a survey to gauge members’ views
departments are often having to fight for imperative to display ‘fiscal responsibility’
on a range of important issues before
their survival and for their own patient for their political survival, leading to
the next MECA negotiations and also to
group, at the expense of a unified voice; under-correction of investment in health
reassess levels of member burnout to see
and even at the union level, divisions are and patients continuing to suffer.
whether this has improved or worsened
being seen, with two unions now for junior A strong clear voice for health in New since our previous similar survey in 2016.
doctors and some divisions within the New Zealand is urgently needed. This requires The response rate was 45%, which
Zealand Nurses Organisation. intelligent, compassionate and mature is fantastic when we know members
leadership. Leaders must recognise that are so extremely busy. The survey was
their primary responsibility is provision comprehensive, so analysis will take
of sufficient, high quality health care for time, but we hope to get results back to
Another result of systemic all New Zealanders, rather than making members soon.
underinvestment, and the budget-cutting the prime goal. They also
Ministry ignoring clinician need to work together to reach agreement
advice and placing cost- and present a unified voice at all levels,
especially when addressing the Ministry A strong clear voice for
cutting ahead of patient care, health in New Zealand is
and government, who can easily blame lack
is the situation now occurring of unity for their own faulty decisions. urgently needed.
at Canterbury DHB.
Over many years, ASMS has worked hard
to ensure that we represent members’
views as accurately as possible, and With the political and economic situation
The most significant problem with this to avoid divisions occurring. We have in a state of flux, the MECA negotiations
fragmentation is the lack of a strong managed to keep membership levels at are unlikely to be straightforward, and we
unified voice in health care. This becomes around 90% of eligible SMOs/SDOs, need to portray member views accurately.
an issue at government caucus where and membership continues to grow At this point, indicators suggest what
the important funding allocations are steadily. ASMS has earned respect from members need most right now is more
debated. As I have discussed previously, DHB management, media, and other colleagues to share the patient load. This
David Clark had the potential to be one of organisations, and might have a growing would go a long way to resolving our
our best Health Ministers. At first, he could role in bringing together various parties to worst problems in health delivery.
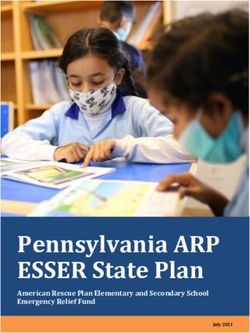
ESTIMATED SMO STAFFING SHORTFALL AS PERCENT OF CURRENT STAFFING ALLOCATIONS
100
AVERAGE 24% STAFF SHORTAGE
80
PERCENTAGE OF FULL STAFFING
60
40
20
0
CAPITAL & COAST (2016)
NELSON-MARLBOROUGH (2016/17)
COUNTIES-MANUKAU (2016/17)
CANTERBURY (2017)
WAITEMATA (2018)
WAIKATO (2019)
NORTHLAND (2019)
WHANGANUI (2019)
TAIRAWHITI (2019)
AUCKLAND (2019)
HUTT (2019)
WAIRARAPA (2019)
SOUTHERN (2019)
LAKES (2019)
WEST COAST (2019)
SOUTH CANTERBURY (2019)
TARANAKI (2019)
BAY OF PLENTY (2020)
HAWKES BAY (2020)
MIDCENTRAL (2020)
Data from ASMS staffing surveys
4 THE SPECIALIST | SEPTEMBER 2020
KINDNESS IS EASY TO SAY
BUT HARD TO DO
SARAH DALTON | ASMS EXECUTIVE DIRECTOR
Iam writing this in the last week of August – a huge week by any measure. We met with our branch officers for our annual workshop,
in a mixed medium webinar. It was held as Auckland continued under Level 3 lockdown and Christchurch found some closure in the
sentencing of the terrorist responsible for the mosque shootings.
I want to take a moment to acknowledge the next DHB, and the next, will not have Canterbury DHB. We may not always
the terrible loss of so many lives at the to pay the heavy price of losing an entire have agreed with each other, and at times
Linwood and Al Noor mosques – including leadership team? Here is some of what we have shared difficult conversations. But
one of our people, Dr Amjad Hamid – and I think. we have never stopped the conversation.
the efforts of our friends and colleagues • Innovating for integrated and timely
at Canterbury DHB who worked so We must only hope that those tasked with
patient care is not cheap and costs governance in the future learn better
tirelessly in the service of those injured in money up front – it is an investment. than the current Board, Chair, and Crown
the attacks.
• Sometimes longer-term benefits and Monitor, who seem to have abandoned
savings do not show up on the balance kindness, and whose eyes and ears are
sheets. closed to the most important part of our
It is galling that so many • People are the most important thing health system – our people.
of those people who have about our health system, and we forget
this at our peril.
sowed the seeds of kindness
• Political cycles are not very compatible
in Christchurch are reaping People are the most
with long-term planning for best patient
a very different outcome care. Wouldn’t it be great if we could important thing about our
from the one they deserve. agree some fundamentals and be given health system, and we forget
time to put them in place? this at our peril.
• Closed-door decision-making is
It makes me think about what being kind unacceptable.
really looks like. As a team of five million • Clinical good practice needs to And to those of you tasked with leading
we grieved with the families of those drive the work of the planners and from the centre, we will be holding you
caught up in the mosque attacks. Now we funders. Remember that doctors have to account. Like our members, whose
are trying to remember to be kind as we obligations that are wider and deeper professional and ethical obligations require
navigate the restrictions and frustrations than those of employees to employers. that they speak up on issues of patient
of the various Covid-19 lockdown levels • Being kind is easy to say and hard to do. safety, health decision-making, and access
as weeks and months go by with closed to care, we will continue to advocate for
It is galling that so many of those people
borders, limited travel, and tired hospital standards of health care that are sufficient,
who have sowed the seeds of kindness in
and community buildings that make that are sustainable, and that are needed
Christchurch are reaping a very different
infection prevention and control so outcome from the one they deserve. by our team of five million.
challenging, not to mention the massive
I want to acknowledge the service and He waka eke noa – te-na- koutou, te-na-
social and economic pressures on many of
leadership of those who are leaving koutou, te-na- ta-tau katoa.
our communities.
But I cannot help but wonder where that
sits in the minds of those charged with
overseeing hospital planning and funding.
Many of you will have been following the
unravelling of Canterbury DHB over the
last few weeks and will have seen many of
our members passionately taking protest
action to voice their concern about the
future of health care in the region.
And while money (or lack of it) is the
subject of this cautionary tale, it’s the
breakdown of key relationships, the
adversarial and dictatorial approaches
adopted by the DHB’s Board Chair and
the Crown Monitor (both appointed on
advice from the Ministry of Health) that
are its theme.
What can we learn? What crumbs can
we pick up and scatter in the hopes that Cartoon: Sharon Murdoch
WWW.ASMS.ORG.NZ | THE SPECIALIST 5
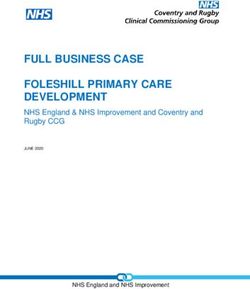
Dr Rob Burrell with a single use intubation device Dr Marty Minehan munching a potato starch tray
WALKING THE TALK ON
SUSTAINABILITY
ELIZABETH BROWN | SENIOR COMMUNCIATIONS ADVISOR
T he Lancet has billed climate change as the greatest threat to human health in the 21st century. In many hospitals, specialists are
at the forefront of sustainability initiatives, driving culture change with clinical expertise and a desire to make things better for
patients, the planet, and the next generation.
When it comes to climate change, millions of single-use plastic and plastic- environmental steering group to measure
sustainability and health care, Middlemore wrapped items. and reduce the DHB’s carbon emissions.
Hospital anaesthetist Dr Rob Burrell
BRINGING CHANGE At its last audit last year, it had reduced its
describes what he sees as “cognitive
carbon footprint by 26% through a number
dissonance”. But the worm is slowly turning, prodded of initiatives, including the use of reusable
“You are supposed to be here to help along by clinicians and hospital staff cups, rideshare programmes, reducing
people, but we are creating so much havoc concerned by the impact of climate change anaesthetic gases, and better recycling.
and mess around us by putting piles of crap on human health and the environment. It has been recognised as one of Toitu-
into the atmosphere and the ground and Envirocare’s top carbon reducers for 2020.
leaving it for future generations to sort. It’s
not acceptable or sustainable.” ICU specialist Dr David Galler was
“You are supposed to be involved from the start and describes it as
It is estimated that New Zealand’s health here to help people, but we life changing.
care sector contributes as much as 8%
of New Zealand’s total greenhouse gas are creating so much havoc “We started off just doing carbon
emissions, and according to the Energy and mess around us by reduction around waste, energy and
Efficiency and Conservation Authority, putting piles of crap into the travel, and it’s turned into a regenerative
health is the largest emitter in the philosophy which has completely changed
atmosphere and the ground
public sector. my world view.”
and leaving it for future
Our hospitals generate a huge Standing in a theatre next to recycling
generations to sort.”
environmental footprint as high-end users bins and cleaner anaesthetic gases, which
of gas, electricity, water, and transport. he successfully lobbied for, Rob Burrell
They churn out hundreds of thousands says a lot of progress has been made but
of tonnes of waste each year, which are In 2011 staff at Counties Manukau DHB there is so much more to do, especially in
dumped into our landfills. They consume took a ground-breaking step and formed an terms of procurement.
6 THE SPECIALIST | SEPTEMBER 2020
Auckland Renal Department recycling champions Drs David Semple and Jason Wei
A 2019 report by the Ministry of Health popular worldwide for intubating Covid-19 his mind, not to mention the cost of
titled Sustainability and the Health Sector patients, are made in Canada and cost landfill disposal.
stated: “Procurement is responsible for $30 each. Dr Burrell says the same
Thinking big, Dr Burrell says New Zealand
an estimated 61 percent of all carbon company makes a reusable but much
more expensive titanium option. should be making compostable gowns or
emissions related to health care … This
investing in upcycling to turn the waste into
is the carbon emitted while extracting,
“In the long run, buying five of the items like combs, park benches or cabling.
manufacturing, packaging, storing, expensive ones would be cheaper because
and transporting pharmaceuticals we hoover through the disposable ones.
and supplies … Making sustainable Plus, our environmental footprint would
procurement part of decision-making be a tiny fraction. We wouldn’t have “We tell the registrars if
processes across all health care sectors thrown anything away, there’d almost be they’re hungry, to grab a
will help signal a shift in demand toward a no packaging, we’d be safe if Covid hit
more sustainable health care system.” bottle of sauce and start
hard because the supply chain would be
local, we’d be employing locals to clean eating them.”
stuff and our carbon emissions would drop
because we’re not constantly re-supplying
“The system is set up to from overseas.” PROVING A POINT
consume. We need to keep
pushing hospitals to change Frustratingly, he says the disposable Up the road at Auckland Hospital, Dr Marty
items come out of the DHB’s operational Minehan is another anaesthetist putting a
the way they make decisions budget, which is huge, while the reusable sustainability lens on clinical practice with
about what they purchase.” devices would come out of the capital some interesting results. Approximately
budget, which is tightly held. 175,000 plastic drug trays annually were
“The system is set up to consume. We being used across Auckland DHB each
A DISPOSABLE CULTURE need to keep pushing hospitals to change year. While the trays could be recycled,
the way they make decisions about what most were being sent directly to landfill.
Holding up a plastic packet with a single
they purchase,” he says.
disposable intubation device, Dr Burrell Dr Minehan, who works in Women’s
says hospitals are great at throwing things The volume of waste created by surgical Health, took matters into his own hands.
away. The devices, which are currently gowns and plastic drapes also weighs on He conducted a life-cycle product
WWW.ASMS.ORG.NZ | THE SPECIALIST 7
“We transport patients about 600,000
kilometres a year to and from dialysis
because we have a treatment model
which is convenient for us, but often not
for our patients. If we have units closer
to where people are, that’s going to save
travel time, carbon emissions and achieve
equity goals and better patient care.”
“When you’re a junior doctor you focus
on the patient in front of you, but as I’ve
moved through my SMO role I’ve realised
my responsibility to the health of my
population and my country as a whole and
that health is more than the drugs I can
prescribe,” Dr Semple says.
‘POCKETS OF BRILLIANCE’
The number of clinical sustainability
initiatives is steadily growing, but the reality
is they require corporate sponsorship and
partnerships so they can be cost neutral to
the DHB. Many of the opportunities have
been identified, followed through, and
endorsed by senior doctors.
They include a recycling pilot in which
plastic syringes are being collected and
repurposed into things like fenceposts, a
programme in which single use medical
instruments are converted back to their
Surgical tool recycling mineral content so they can enter the
recycling chain, and the recycling of PVC
products like fluid bags and oxygen masks
analysis, and after a successful pilot, drug by Clinical Director Dr David Semple.
into playground matting.
trays made from potato starch are now They conducted a waste audit and have
being rolled out across the hospital. successfully decreased medical waste SMOs have also been behind a push to
from each dialysis process by 40%. get more charging stations for electric
The trays are compostable and vehicles in DHB carparks.
biodegradable. He jokes, “We tell the According to Dr Wei, “For our clinical related
registrars if they’re hungry, to grab a projects to be successful it was up to SMOs’ Auckland DHB has reduced its emissions by
bottle of sauce and start eating them.” 28% in four years, and the achievement has
support because if they are not on board,
been recognised with several global and
He took the project on to prove a point. other staff won’t be confident to ensure all
local awards. Like Counties Manukau DHB,
changes will be implemented properly.” Auckland DHB has also been recognised
“I rang each of the suppliers and sent
Green initiatives are now a standing this year by Toitu- Envirocare as one of the
them an email with 20–30 questions
item in the department’s regular service country’s top carbon reducers.
about their products. We did a
spreadsheet of all the different products management meetings. It is estimated Deputy CMO and Director of Cancer and
and how much they cost. four million litres of water a year could Blood Services at Auckland DHB Dr Richard
be saved from water-heavy dialysis Sullivan believes the challenge is to take the
“We took it to the senior leadership processes. As a result, staff are being “pockets of brilliance” around sustainability
team and what we’ve ended up with is educated around simple ways to reduce and embed them into the organisation’s
a cheaper product, with a significantly water use, and Dr Semple has been culture and leadership structure.
smaller footprint, something which is
in discussions with Watercare about “Ideally, when we have our strategic
easy to dispose of, has virtually zero
potential large-scale infrastructure imperatives such as Te Tiriti, equity, and
environmental impact, is locally made so
changes to help achieve that. digital enablement, in two to three years,
the money goes back into the economy –
there will be one around sustainability.
and you can eat it.”
“We are one of the biggest employers in
His advice to his fellow SMOs is to New Zealand and we should be leading that
question suppliers about their products. “When you’re a junior doctor
space, and the reality is that doctors have a
you focus on the patient in major influence in those decisions,” he says.
“Ask what their environmental credentials
are, what makes their product better in front of you, but as I’ve moved
terms of its environmental footprint, how through my SMO role I’ve
The Specialist is distributed by a
is their company engaged in terms of realised my responsibility to marketing company which is Enviro-
sustainability?” the health of my population Mark Gold certified. The plastic
WASTE AUDITING AND REDUCTION and my country as a whole.” wrapping is treated with EcoPure – an
organic additive which helps plastic to
A few floors down in the hospital’s Renal biodegrade. The magazine is printed
Department, green initiatives began on Forestry Stewardship Council
about two years ago, led by technical Changing models of care are also being approved paper.
advisor Dr Jason Wei and supported looked at.
8 THE SPECIALIST | SEPTEMBER 2020
HOW THE HEALTH SYSTEM IS
BEING SHORT-CHANGED BY ACC
DR PETER ROBERTSON | AUCKLAND ORTHOPAEDIC SURGEON & LYNDON KEENE | HEALTH POLICY ANALYST
A CC appears to be under-paying its share of the cost of public hospital trauma care by hundreds of millions of dollars a year,
according to Ministry of Health and ACC data and modelling by one DHB.
While ACC is responsible for funding the indicated by official case-weight estimates. INVISIBLE FUNDING SHORTFALL
care for those injured in accidents, its The study involved a relatively small
funding for those who need acute care in number of patients, so strong conclusions This funding shortfall has most likely
public hospitals, covering the first seven cannot be drawn from it. However, if grown over many years but has remained
days from injury, is not paid directly to anything, it probably understates the invisible due to a lack of regular accurate
DHBs. Instead, each year it bulk funds the extent to which case-weight estimates fall assessment and monitoring. Since the
Crown for Public Hospital Acute Services short of the true costs of care because PHAS funding is absorbed into Vote
(PHAS) costs, amounting to more than it excluded patients who needed urgent Health’s general DHB funding, there is
$500 million a year. The Crown in effect transfer to a tertiary centre, who are no indication of how much of the PHAS
purchases public hospital acute services likely to be the most complex of patients funding each DHB receives. The calculation
on behalf of ACC. This is included as requiring ICU care and surgery. of the value of the PHAS is equally opaque.
an un-itemised part of DHBs’ budget Accurate financial accounting of the true
allocations in Vote Health. It also means the funding gap indicated in costs of trauma – and therefore ACC
Figure 1 is conservative. patients – does not appear to occur in
But while the PHAS funding increased by most DHBs. There is at best an antiquated
15.5% in real terms between 2009/10 Recently, Canterbury DHB calculated
costings for injury patients that would come classification system for injuries that in
and 2018/19 (slightly higher than the no way adequately represents current
population 12.7% growth), accident-related under the ACC umbrella and compared
this to their DHB share of PHAS funding classification of surgical events. There
hospital discharges are increasing at a
(estimated according to its share of appears to be no recognition of the extent
much higher rate. Acute (case weighted)
national DHB population-based funding). to which acute accident-related surgery
discharges for injury or poisoning, for
has grown in complexity over the years,
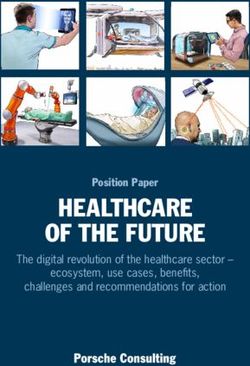
example, increased by nearly 23% over the Several models of costings were used
same period (Figure 1). (The low number of often requiring the work to be done in
and resulted in estimates suggesting
discharges prior to 2012/13 is due in part daylight hours – which means that as well
that PHAS funding is little more than
to incomplete data up until that time.) as being under-funded, the work displaces
half of what the costs of ACC patients
other elective surgery.
Further, the indications that acute injury would actually be. Given that PHAS
related discharges are growing at a much funding for the year of this study was in The Ministry has explained that the
higher rate than ACC funding are only the order of $500 million, Canterbury PHAS funding has been calculated “after
part of the story. A study on the costs of DHB’s modelling suggests underfunding periodic reviews that require significant
major trauma care in Northland found the of trauma care provided by the DHBs resource yet have low levels of confidence”
total actual cost was markedly higher than nationwide is likely to be in the hundreds (presumably related to accuracy). So,
of millions of dollars. it seems that both ACC and the DHBs
have little idea as to the true cost of
FIGURE 1: CUMULATIVE PERCENTAGE GROWTH IN ACC FUNDING (DEFLATED) trauma and accident services. The PHAS
AND ACUTE TRAUMA HOSPITAL DISCHARGES contribution is simply based on the prior
25 Real ACC funding Acute discharges (caseweighted)
year’s contribution plus an increase in
line with general DHB funding increases,
CUMULATIVE % GROWTH
20 thereby perpetuating a head-in-the-sand
approach to trauma care funding.
15
A prominent health advisor commented
10
privately that “there is no appetite for
5 change” on this issue. But given the
evident gross underfunding of acute
0
services and its flow-on effects for
2009/10
2010/11
2011/12
2012/13
2013/14
2014/15
2015/16
2016/17
2017/18
2018/19
non-acute services, the New Zealand
public will surely expect to see a more
responsible attitude from government
Sources: National Minimum Data Set, Ministry of Health; ACC annual reports; Stats NZ decision-makers.
Notes: Acute trauma discharges include those categorised as ‘injury or poisoning’, including inpatients and day-
patients. Data prior to 2012/13 are incomplete. Such funding neglect, to the detriment of
Deflated in 2009 dollars using Reserve Bank of NZ inflation calculator. many patients, demands urgent attention.
WWW.ASMS.ORG.NZ | THE SPECIALIST 9
CLOSING THE GAP BETWEEN
HEALTH POLICY AND
DELIVERY
LYNDON KEENE | HEALTH POLICY ANALYST
A striking feature of the Simpson Health and Disability System Review is the extent to which its recommendations resemble the
policy intentions of the New Zealand Health Strategy of 20 years ago. Similarly, the Mental Health and Addiction Inquiry found
that over the past couple of decades the mental health and addiction system ‘has not shifted’, despite the stated intentions of earlier
strategies. It concluded that “a fundamental disconnect exists between stated strategic direction, funding and operational policy and
ultimately service delivery”. Health policy analyst Lyndon Keene examines why such ‘disconnects’ occur and what is needed to close
the gap, including the part that doctors have to play.
A great irony in democracies is that the their promises due to the coalition the same results elsewhere. And those
people entrusted to make them work tend arrangements and negotiations. The operating at higher levels cannot
to be among the least trusted by their literature on the policy-implementation succeed without having some grasp of
populations. gap, or ‘policy failure’, identifies at least what happens on the ground.
four broad contributors. In short: • Inadequate collaborative policymaking:
Prior to the last election in 2017, a Stuff/
Massey University Election Survey found • Over-optimism: Political party Policymaking has tended to be developed
only 16% of nearly 40,000 respondents policymakers underestimate the in silos. But good policy design requires
were prepared to vouch that in general complexity of the delivery challenges continuous collaboration with a range of
New Zealand’s politicians ‘keep their and often lack the evidence base stakeholders at different levels as well
promises’, while 58% preferred the option (insufficient objective, accurate and as engagement with local communities
that said they ‘only sometimes keep their timely information on costs, timescales, and the people who are critical to
promises’, and 26% chose ‘usually break benefits, and risks). implementing the policy on the front line.
their promises’.
• The local context: In complex systems • Vagaries of the political cycle – short-
In New Zealand, under MMP, it can an intervention that is successful in one termism: Politicians are too easily
be harder for candidates to keep all location does not necessarily deliver attracted to the prospect of short-term
10 THE SPECIALIST | SEPTEMBER 2020results that suit the election cycle, problems in the political system, not But the public’s concerns about the
rather than investing in policies which just in terms of making government effects of under-investment in our
may take years to bear fruit. This more transparent, but also improving health system, as reflected in at least
can lead to the pushing through of its capacity to involve more public one opinion poll before the pandemic
policies as quickly as possible, often participation. struck, further reinforced with reports
half-baked, and the neglect of longer- on the system’s lack of capacity to
Certainly, talk of engagement may
term projects, which are usually more respond to pandemics, has raised public
invite more cynicism among senior
complex. Think health workforce awareness of just how precarious many
doctors than a belief that it might make
development, clinical leadership, parts of the system have become.
a difference. The lack of meaningful
integrated care and ‘health equity’, engagement between doctors and This, along with many of the findings of
for starters – all of which have been management in DHBs, let alone the Health and Disability System Review,
talked about for years by successive between doctors and government, is a highlights the need to develop with
governments and are still being long-standing sticking point. But that urgency a strong health system fit for the
talked about. does not negate the critical need for future with policies that are informed by
HOW TO ENSURE POLICIES ARE engagement if policy development is to the best evidence and knowledge, and
IMPLEMENTED be well informed and gets traction in with accountability measures to ensure
practice, especially where the policy is those policies are implemented.
For solutions, there’s no shortage complex and long term. If information
of ideas from policy think tanks and Policies must undergo regular and open
flow and openness to engagement from
political commentators, ranging reviews to ensure they are working as
the ‘top’ are weak, there is arguably
from strengthening the roles and intended, and modified as necessary,
more reason that activity from the
functions of ombudsmen and rather than quietly fading away as
bottom-up must be strong.
parliamentary committees, to setting has often happened in the past. The
up policy ‘delivery units’ to track Researchers suggest engagement evidence shows this can work when
the implementation of policy, and between the front line and centre may governments are truly open and engage
establishing parliamentary policy require some form of intermediary body with the public and specifically those
costings units. or bodies that work alongside and often with the knowledge to provide the best
at the direction of government to support policy advice – and when parliamentary
Of the various themes running through, effective policy implementation. Whether debate is constructive rather than
one is worth a special mention for the such arrangements are needed in New destructive. These together have been a
critical role senior doctors could play Zealand may be worth considering. standout lesson from the pandemic.
concerning collaborative policymaking
In the meantime, there is a lot that The Simpson Review calls for the
and delivery.
senior doctors can do to strengthen development of a more positive culture
current engagement avenues, such and working conditions, improved
as through ASMS branches and Joint collaboration and integration, and
The lack of meaningful Consultation Committees, simply by clinically led service development. All
engagement between participating in them. The information are laudable, but these things do not
flow from those forums then feeds into happen just because you want them to.
doctors and management the national forums involving ASMS, They require deliberate strategies, hard
in DHBs, let alone between as well supporting a range of national work, and a commitment to change.
doctors and government, advocacy work.
is a long-standing sticking When all else fails, particularly where
point. there are specific local issues that Policies must undergo
remain unresolved due to poor policy
or failure to implement good policy,
regular and open reviews
senior doctors have the right to speak to ensure they are working
It’s well recognised that those who work
on the front line of the health system out publicly, as outlined in Speaking up as intended, and modified
know more about the challenges of for patients and staff (ASMS website). as necessary, rather than
delivery than national policymakers. And the experience has been that when quietly fading away as has
doctors do speak up, people, including
A crucial part of developing and often happened in the past.
implementing policy, therefore, is to tap those in government, tend to listen (The
into the experiences of those tasked with Specialist, March 2020).
delivering it. It involves assessing existing LESSONS FROM THE COVID-19
capacity to deliver, knowing what is Whatever the colour of the new
PANDEMIC
being done well, what needs improving, Government, 2021 is shaping up to be
and how best to build new capacity. The public’s expectation for a strong a significant year for developments in
health system underpinned by good health policy, whether it is putting the
The need for a bottom-up, top-down health policy and delivery has been meat onto the bones of the Simpson
flow of information in both directions under the spotlight this year like no Review recommendations or something
is emphasised in Max Rashbrooke’s other. The extraordinary sacrifices made entirely different. The participation
research report Bridge Both Ways by the ‘team of five million’ to protect of senior doctors, in whatever form it
about transforming the openness the country’s collective health, despite takes, in shaping those developments
of New Zealand Government and the devastating effects on the economy, could help to ensure that some of the
improving democracy. Rashbrooke puts have underlined the high value people much-needed policies identified 20
forward some key ideas about fixing place on health above all else. years ago are finally brought to life.
WWW.ASMS.ORG.NZ | THE SPECIALIST 11SIMPSON REPORT
A DISSENTING VIEW -
PETER CRAMPTON Prof Peter Crampton
O ne of the most controversial recommendations of the Simpson Health and Disability System Review is around a new Ma-ori
Health Authority (MHA). The final report proposes an advisory entity sitting alongside the Ministry of Health and the
newly created Health New Zealand. It would be responsible for monitoring and reporting on Ma-ori health outcomes, managing
Ma-ori workforce initiatives, controlling Ma-ori-specific innovation funds, and advising Health New Zealand, the Ministry and the
Minister of Health on how to redress inequities in the system.
However, four of the six panel members, the implementation phase of any associated with integration of hospital
along with the Ma-ori Expert Advisory future changes. This matter was not and community-based services. From
Group, believe that for health outcomes considered in detail by the panel and a system design perspective, MHA
for Ma-ori to improve, the MHA must requires further work. Part of the commissioning would bring focus to
have the power to control both funding challenge is the lack of knowledge commissioning services for Ma-ori.
and commissioning of services. In a and understanding as to what is
highly unusual step, that dissenting currently spent on services in this Your alternate view suggests
position was included in a separate domain. It is important to note that the MHA “could more effectively
chapter of the Simpson Report, known costs associated with many of the tackle institutional racism via its
as the ‘alternate view’. report’s recommendations are yet to be commissioning role”. Would there
quantified, including the entire change be a risk that those services not
Dr Peter Crampton, Professor of commissioned by the MHA may feel
Public Health in Ko-hatu, the Centre management budget. There is much
more work to be done to understand that addressing institutional racism is
for Hauora Ma-ori at the University of less of a priority?
Otago, is one of the panel members the financial implications of change.
who favoured that view. We asked him Would the MHA commission services I agree that this is a risk, but it is a
more about how it might work. from hospitals as well as from risk that has been manifest within our
community service providers, and if so, health system for a very long time. Our
Given the new Health New Zealand hope is that a fully empowered Ma-ori
agency would have “equal numbers how would that work in practice?
commissioning agency would model
of Crown and Ma-ori members”, and A fully empowered Ma-ori commissioning approaches to commissioning that
the MHA’s potentially powerful role of agency could commission services from would inspire change across the whole
monitoring and reporting the system’s hospital and community-based providers. health system. We do not envisage
performance for Ma-ori, why do you see The commissioning process would that MHA commissioning would be
a need for a fully empowered Ma-ori be carried out in close consultation undertaken in isolation of Health New
funding and commissioning agency? and partnership with Health New Zealand and DHBs.
The proposal to have 50% Ma-ori Zealand and relevant DHBs. Mixed
commissioning is already a well- Could private health care providers be
composition of the Board of Health
established model within the system commissioned under either system?
New Zealand is indeed a positive step.
As a powerful addition to the leadership (e.g. services funded by the Ministry Yes, the existence of a Ma-ori
and governance of the health system, of Health, DHBs, ACC, Wha-nau Ora). commissioning agency is entirely
we believe a Ma-ori-led and controlled Again, persistent inequities show us that consistent with the ability to contract
commissioning agency, with a we need to do something differently in with private health care providers.
meaningful budget, would bring a focus order to shift the trajectory of the system
of expertise and strategic clarity to from an equity perspective. Could there be public/private
the task of commissioning services for partnerships, and if so, do you see
Integrating hospital and community-
Ma-ori that has proven to be hard to based services remains an important if
potential for conflicts of interest which
achieve in mainstream organisations. could be exacerbated with a separate,
elusive goal. Would a separate funding empowered entity?
History has clearly shown that it will
agency create additional challenges?
take more than a seat at the table to Public–private partnerships are possible
effect sustainable change. The role of service commissioners is to within the proposed new system. I don’t
clarify expectations and outcomes, and see any additional risks or potential
If, as in your alternate view, the MHA
the role of health service leaders and
was a budget-holder for commissioning conflicts arising as a result of a fully
clinicians at all levels of the health system
services for Ma-ori, how would you empowered Ma-ori commissioning agency.
is to deliver on these expectations. The
envisage that budget being set?
existence of a Ma-ori commissioning ASMS has not yet formed a policy position
This is an important question that agency would not necessarily, in itself, on whether it favours the MHA as laid out
would need to be answered during either amplify or diminish the challenges in the report, or the alternate view.
12 THE SPECIALIST | SEPTEMBER 2020HOW THE PARTIES STACK UP
A SMS reached out to the main political parties in the lead up to the 17 October general election to ask about their policies
and priorities on health.
Full responses and comments are on the ASMS website www.asms.org.nz
Research conducted by ASMS shows an average 24% shortfall
in the number of senior doctors working in DHBs nationwide.
Does your party agree that this shortage must be addressed
by increasing the workforce accordingly?
ü ü ü ü ü ü
According to the Health Coalition Aotearoa New Zealand has the
third highest rate of obesity within the OECD which is inextricably
linked to unhealthy diets. Does your party support self-regulation
by the food industry as an appropriate way to manage obesity
û ü ü û ü ü
rates and the wider impact of obesity on society?
Would your party ensure DHBs were sufficiently funded to
meet their communities’ health needs without clocking up huge
deficits every year?
*Comment
only
*Comment
only ü ü ü ü
Would your party be willing to commit to cross-party
agreements on longer term health investment and health
policies that require long time-frames for implementation, such
as workforce development, illness prevention and integration
ü ü ü ü ü ü
of services?
ASMS estimates there are nearly 450,000 people with
an unmet need for hospital care due largely to inadequate
hospital service capacity. Does your party agree that unmet
need is a significant issue for New Zealand; and would your
party increase hospital capacity to ensure unmet need is
ü ü ü ü *Comment
only ü
addressed?
* Full comments available on the ASMS website
TOP THREE INVESTMENT PRIORITIES FOR HEALTH
• Equity of access for vulnerable populations and those in rural isolation.
• Future proof St John Ambulance funding.
• Reduce the number of DHBs.
• Sector capital, funding for district health boards to address demographic and cost pressures.
• Funding to implement recommendations from the Government Inquiry into Mental Health and Addiction.
• The Health and Disability System Review.
• Devolve primary health care services to allied staff.
• Ensure funding follow the patient not the practice.
• Increase the remuneration of our nursing workforce.
• Increasing public health funding to keep pace with need and the growing population.
• Ensure everyone can access healthcare services, regardless of their ability to pay, at the earliest stage possible. This
includes working towards providing adequate funding for community-based care and increased resources for wellness
and preventative health measures.
• Incorporate ma- tauranga Ma-ori into the health system, and fund a provision of primary healthcare through Ma-ori
organisations, overseen by a new Ma-ori health agency that focuses on remote areas with significant health disparities.
• Primary care funding.
• DHB infrastructure.
• Workforce development.
• Protecting public health in response to COVID-19.
• Mental Health.
• Addressing the shortfall of qualified medical professionals in the health sector.
WWW.ASMS.ORG.NZ | THE SPECIALIST 13Gaeline Phipps Drs Gareth Harris, Katie Ben, Anette van Zeist-Jongman, Alain Marcuse
Drs Lizi Thirsk, Tanya Wilton, Norman Gray, Neil Stephen Drs Kai Haidekker, Geoff Shaw, Roger Wandless
A MULTI-MEDIA HUI FOR
BRANCH OFFICERS
LYDIA SCHUMACHER | COMMUNICATIONS ADVISOR
I t was a multi-media affair when ASMS branch officers met for their annual hui at Te Papa in Wellington late last month.
Level 3 Covid-19 restrictions in Auckland and explained the rules for state sector Lloyd Woods also discussed the initial
meant branch officers in the northern employees around political statements bargaining strategy for MECA 2021 and
region joined in virtually by webinar. For during election time. Her message was said planning is well underway.
everyone else who was able to make it to to use your union, and that speaking out
makes patients and colleagues safer. A briefing was given by senior industrial
Wellington, social distancing rules applied.
officer Steve Hurring on the Holidays
The annual hui provides branch officers The current MECA and the bargaining Act remediation so that branch
with the opportunity to look at and discuss process for the next MECA were also the representatives are fully aware of the
some of the big issues facing members. focus of discussions. processes around rectification.
“You can see what challenges are faced ASMS senior industrial officer Lloyd
There was much discussion about the
by other DHBs and compare it to yours. Woods detailed what had happened
Simpson Health and Disability Review and
It’s also an opportunity to discuss with during this year’s negotiations with
what the recommendations might mean
the executive what the current issues are Covid-19 resulting in an early settlement
and outlined some of the changes for ASMS members.
with health in New Zealand with an SMO
focus,” said Waitemata- Branch President included in the current MECA. Branch officers were also given a sneak
Jonathan Casement. Canterbury Branch Vice-President preview of the preliminary findings from
Siobhan Cross said finding out about the our recent membership survey.
Lawyer Gaeline Phipps delivered the key
changes to shift work and sabbatical was Thanks to all the branch officers who took
session of the day about the importance
particularly useful. part. The feedback we got was that the
of senior doctors and dentists speaking
out on issues of patient safety. She spoke “I think most people are under the webinar aspect of the meeting worked
in depth about the provisions in the impression that there was only the CPI well, but here’s hoping that everyone can
MECA which enable public comment pay rise,” she said. get together in person next year.
14 THE SPECIALIST | SEPTEMBER 2020Dr Roderick Douglas out on the job
COVID-19 SHINES A LIGHT
ON OCCUPATIONAL
MEDICINE
ELIZABETH BROWN | SENIOR COMMUNCIATIONS ADVISOR
W hile the Government and health officials have been working to keep the public safe during the Covid-19 pandemic, stretched
occupational health teams have been focused on protecting the health workforce.
Hospitals have struggled to manage staff of DHBs have occupational medical to identify vulnerable staff. That meant
risk assessments and applications from physicians employed directly on staff. screening thousands of DHB employees.
workers with underlying health conditions, There is no funding in hospital budgets to
Dr Kenny says at Waitemata- DHB alone
due to poorly resourced and understaffed train occupational registrars.
about 1,000 people had an underlying
occupational medical services at DHBs
During ASMS’ recent round of JCC condition who needed risk allocation and
across the country.
meetings, occupational health was a work plan. Insufficient PPE early on
Occupational medicine is about the identified by most DHBs as a vulnerable caused extra problems and anxiety.
effect of health on work and work on service with serious training pipeline issues. “We developed systems and protocols. We
health. Specialist occupational physicians
GAPS EXPOSED co-opted other doctors whose services
deal with a range of occupation-related
weren’t seeing patients along with GPs. We
health conditions and try and optimise a The Covid-19 pandemic exposed the gaps. had assistance from clerical, admin people,
person’s ability to work or return to work.
Dr Courtenay Kenny is an occupational and nurses, and some occupational health
They also look at a raft of work-related
medicine physician at Waitemata- DHB in specialists outside the hospital service were
risks such as heavy lifting, exposure to
Auckland. He says, “While most specialists able to come and help.”
chemicals, dusts and radiation, night duty,
and infectious diseases. in hospitals were quiet, we were incredibly The workload at Waitemata- was
busy. It was a stressful time as we had compounded by a Covid-19 outbreak at
According to the Medical Council to develop new understandings and Waitakere Hospital involving
register, there are around 60 practising
procedures as we went along.” several nurses.
occupational medicine specialists in
New Zealand. Most work in private A National Occupational Health and Safety “Covid told us that there is a great
companies, ACC or WorkSafe. Some are Group was formed to look at Covid-19 need for the health and wellbeing of a
contracted by DHBs, but only a handful and develop a mass screening strategy workforce to be looked at and that health
WWW.ASMS.ORG.NZ | THE SPECIALIST 15Dr Courtenay Kenny is concerned about the workforce pipeline
workers are valued for what they do,” Medicine, which sits within the Royal according to the statistics, workplace
Dr Kenny says. Australasian College of Physicians. disease and illness is much more
There are currently only 11 occupational significant in terms of morbidity
HISTORICALLY LOW NUMBERS
medicine specialist trainees, and only and mortality.
He explains that occupational medicine one is working in a DHB setting. He cites accelerated silicosis – a newly-
as a specialty has had historically low
numbers because many years ago FUNDED TRAINING NEEDED identified, and very serious lung disease
training was abandoned to industry. associated with artificial stone bench
In his view, what is needed is a funded
manufacture.
occupational medicine clinic within
each of the larger DHBs, which would
have a registrar working alongside an
“Covid told us that there occupational physician. He would also
“If you are a junior
is a great need for the like to see better lines of communication
health and wellbeing of a between occupational specialists and hospital doctor you can
workforce to be looked at hospital specialists in general. go into orthopaedics,
and that health workers are “Having a regular presence within a rheumatology or public
valued for what they do.” DHB would help improve this and bring health and remain in
us to mind when other specialists are the hospital service and
considering their patients’ needs,” he says.
vocationally register –
Dr Kenny has concerns about the but you can’t do that in
“If you are a junior hospital doctor you impact the lack of occupational health
can go into orthopaedics, rheumatology specialists in DHBs has on wider occupational medicine.”
or public health and remain in the community health.
hospital service and vocationally
register – but you can’t do that in “People from the community who are in
hospital or are outpatients can’t access He also says greater awareness of
occupational medicine. You have to
an occupational medical assessment workplace health and safety, along
do all your own training, earn the
through the publicly funded system.” with legislative changes, have driven
income yourself by contracting with
demand for occupational medicine
organisations and then arrange to learn “The only way people in the community
can be seen by an occupational services up, but the occupational
everything for your exams and finally
medicine specialist and ensure they can medicine workforce has not changed to
become vocationally registered in
occupational medicine.” go back to their job safely is generally meet that demand.
to pay for it independently or do it Both doctors agree that DHBs are
Dr Roderick Douglas is an occupational under ACC,” he says.
physician in Tauranga and is the waking up to the value of occupational
director of training for the New Zealand Dr Douglas points out that the focus medicine and are hopeful some
division of the Australasian Faculty of the government agency WorkSafe is meaningful investment in funded
of Occupational and Environmental on accident and injury, prevention but training programmes may follow.
16 THE SPECIALIST | SEPTEMBER 2020IMGS IN
FOCUS Erin and Michael with their three children
ELIZABETH BROWN | SENIOR COMMUNCIATIONS ADVISOR
W hen American couple Dr Erin Doherty and Dr Michael Howard packed up their three children and moved from New Mexico to
New Zealand six years ago, they thought they knew what to expect, but there have been a lot of surprises along the way.
New Zealand is highly reliant on make competent decisions that were “To go back to a place where that doesn’t
international medical graduates (IMGs). appropriate for the system here.” happen would be a real crisis. I cannot
They make up about 40% of the specialist overstate it.”
She felt disadvantaged having never worked
workforce, which is one of the highest
in the NHS or a similar system. After feeding MAKING A DIFFERENCE
proportions of IMGs among the 37 OECD
back to her department, she is happy to say
nations. Dependency on IMGs is also Working in a place where they felt they
changes have been made to the induction
greater in the provinces where SMO could make a difference was important.
process to better support newcomers.
shortages and recruitment difficulties Both had worked in areas in the US
often bite hard. Her husband says working in a socialised, with poverty and need, including Native
universal health care system has been a American reservations.
Dr Doherty is an acute general medicine
revelation which has changed his practice.
specialist who also does outpatient “In New Zealand you get to practise
cardiology, while Dr Howard is an emergency “The thing that really burns out a lot medicine that is going to be more
medicine specialist. Finding a place where of American doctors is the thought of challenging,” says Dr Doherty.
they could each work was a priority. bankrupting a patient or putting undue debt “When you’re working in a provincial place
on them because they don’t have adequate with less specialists and speciality care,
insurance and can’t get the equitable you really get to practise at the top of
outcomes that you get to see more often in your licence. We get incredible diversity
“It probably took me a year New Zealand,” says Dr Howard. of patients with complex needs. I’ve seen
to feel like I could make He adds, “Even though I might sometimes things here that I had only read about.”
competent decisions that feel that I can’t as easily access speciality
were appropriate for the services for my patients, I certainly see that
system here.” outcomes are likely comparable, and the
costs are much better controlled. It makes “Even though I might
my mental, spiritual and moral health better.” sometimes feel that I can’t
He also a big fan of ACC and believes any as easily access speciality
After a two-week recce to check out
IMG wanting to come to New Zealand services for my patients, I
a few job offers, Dr Howard (a California-
born surfie) landed firmly on Ngunguru
should school themselves up on Te Tiriti. certainly see that outcomes
in Northland, and it was not long “I realise there are deficits, but trying to are likely comparable, and
before they had taken up positions at attempt to be faithful to a single treaty the costs are much better
Wha-nga-rei Hospital. and bring it out through the health system controlled. It makes my
has been a remarkable thing to witness
FUNDAMENTAL DIFFERENCES and one of the best surprises that I
mental, spiritual and moral
For Dr Doherty, the adjustment was more wasn’t expecting.” health better.”
difficult than she had expected due to what
she says are the fundamental differences
with the American health system. In turn, they believe having a diverse
“I’ve seen things here that I IMG specialist workforce in New Zealand
“I had to unlearn some habits and had only read about.” enhances the system and means everyone
completely change how I approached benefits from what Michael describes
patients because the kind of practice as “the worldwide cross pollination of
I’d fallen into in the US involved a lot of expertise and information”.
defensive medicine where patients have Having a union and collective bargaining
high expectations about getting tests and has also been an eye-opener. He says the Their advice to any IMG thinking of
having things done.” opportunity to sit in a JCC and “watch coming to New Zealand is do your
ASMS go toe-to-toe with the DHB and homework, ask lots of questions, be
“You think medicine is a universal thing, hold them accountable on issues of staff humble, and approach it with an open
but it was apples and oranges. It probably safety and welfare” is something he had mind and an attitude of learning because
took me a year to feel like I could never witnessed or experienced. the system can be full of surprises.
WWW.ASMS.ORG.NZ | THE SPECIALIST 17You can also read