Victorian Health Priorities Framework 2012-2022: Metropolitan Health Plan - Health.vic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan


Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan May 2011

If you would like to receive this publication in
an accessible format, please phone 03 9096 8337
using the National Relay Service 13 36 77 if required.
This document is also available in PDF format on the
internet at: www.health.vic.gov.au/healthplan2022
Published by the Victorian Government
Department of Health, Melbourne, Victoria
© Copyright, State of Victoria, Department of Health, 2011
This publication is copyright, no part may be reproduced by any process
except in accordance with the provisions of the Copyright Act 1968.
Authorised by the State Government of Victoria, 50 Lonsdale Street, Melbourne.
May 2011 (1104014)
iv
Foreword
Few things matter as much as our health. Being in The health system needs more support to
good health – and getting the care we need when improve management of these long-term chronic
we need it – allows us to live long, fulfilling lives conditions, as well as better managing health
and to participate fully in our community. But we issues faced by particular communities.
cannot stay healthy without a strong health system.
Health care costs are growing steadily, and
Health is important in itself, but it is also crucial for our workforce will need new skills to meet our
a strong economy. Healthy people mean a healthy changing needs. All Victorians must be better
workforce, and a healthy workforce combined informed about how to stay healthy and how to
with a strong health and medical research sector make the best use of the health system when they
will increase Victoria’s long-term productivity and need it. The Victorian Government is committed to
economic growth. The last factor is essential for more and better information for patients. Informed
the state’s stability and security, and to foster the consumers are able to make better choices for
conditions in which members of our community their health care and that of their family.
and leaders of our health system can plan for the
future with confidence. The implications are clear. Without change,
our health system will not be able to meet our
Although Australians, as compared to other future needs.
OECD countries, generally receive very good
health care services, service providers are feeling The Victorian health system is much more than
the pressure from increasing demands and public hospitals. Victorians have benefitted from
constrained resources. Our hospital system is a wide range of community health and community
clearly facing challenges. The historical role support services, public dental and community
and focus of hospitals has been acute illness, nursing services. Importantly, the Victorian health
usually relatively short term. system also includes the private sector. However,
this sector, including private hospitals and private
Victoria’s health system has not been planned health providers such as general practitioners,
properly to take account of population growth medical specialists, nursing, dental and allied
and the ageing of the population. Victoria’s health health clinicians, has been treated in isolation
system has been operating on planning that has from our major public institutions. Planning for
used 2002 population projections that are long out Victoria’s health system must recognise the role
of date and superseded by the rapid increase in and capacity of private services so that we
Victoria’s overall population. Victoria’s health system achieve the best possible health service system
is under pressure and Victorians are feeling it. for all Victorians.
We have known for a long time that our population The government undertook, during the 2010
has been ageing, and growing, and that this and election campaign, to provide the state with a
life style changes have contributed to chronic health services plan to 2022, based on current
health conditions, such as respiratory and heart and accurate demographic and population
disease, type 2 diabetes and mental illness, data, and on consultation with all sectors and
that are increasingly affecting many Victorians. stakeholders, to lay out a clear integrated and
These conditions are placing unprecedented coordinated agenda for the future of the entire
pressures on all health services, but particularly Victorian health system.
on hospitals. We have invested too little in
preventing and better managing these conditions.
v
Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
In fulfilment of this commitment, the Department The Health Plan, whilst focussed on the central
of Health has consulted with the health sector, role of the public sector in the provision of
and I have appointed a Ministerial Advisory health services, for the first time recognises the
Committee, chaired by the Hon. Rob Knowles increasingly valuable and complementary role
AO, to provide advice and information on the of the private sector. Together, the public and
best possible approach to planning for improved private sectors, including health funds and the full
health services in Victoria. range of private practitioners, make up Victoria’s
essential health services.
These consultations and discussions have asserted
the need for long-term health planning priorities The Victorian Government is committed to
for the state that recognise the impact of chronic confronting the challenges that lie ahead, and
illness and disease, the capacity to do much to to creating an equitable and sustainable health
prevent and reduce these conditions, and the system with people at its heart.
pressures resulting from the rapid increase in the
Victorian population. The government has already committed
to a strategic approach to improvement
The previous planning framework for metropolitan of our health system through its election
Melbourne, The Directions for your Health campaign commitments that included,
System: Metropolitan Health Strategy (2003) was amongst other features:
based on flawed population projections and is
now long outdated. The government, through —— additional health infrastructure and capacity
the Department of Planning and Community —— waiting list and emergency department reform
Development (DPCD), is preparing new —— improving ambulance services
population projections, available in June 2011, —— overhauling rural and regional health services
that will be essential information in the planning —— supporting Victoria’s leadership in health and
and delivery of health services. medical research
—— increasing transparency and accountability.
As a result of the advice from the consultations
and the Ministerial Advisory Committee, we have A key election promise was to undertake
prepared this Victorian Health Priorities Framework comprehensive planning for the future upon
2012–22: Metropolitan Health Plan (the Health coming to government.
Plan) to provide, for the first time ever, statewide
planning principles for the Victorian health system. The release of this Victorian Health Priorities
Framework 2012–2022: Metropolitan Health Plan
The Health Plan is the first step in our marks the delivery of that commitment.
ground-breaking statewide approach to the
implementation of those priorities within
metropolitan Melbourne. A companion
Metropolitan Health Plan – Technical Paper
provides the essential data and analysis to inform
implementation of these planning priorities in
metropolitan Melbourne.
vi
The Health Plan is focussed towards 2022 – a These priorities will help us to create the people-
longer time span than hitherto embraced by focussed, knowledge-focussed system Victorians
government. This will guide the preparation of deserve, laying out a path to the future.
the Rural and Regional Health Plan and the Health
Capital and Resources Plan 2012–2022, which I wish to thank the Hon. Rob Knowles AO and the
will be developed over the coming months with Ministerial Advisory Committee, and the many
the advice of the Ministerial Advisory Committee health professionals who were consulted in the
and in close consultation with the community and preparation of this document. Their advice and
health sector – a process we have already begun. input shaped these priorities that will now guide
our future work.
Together, these priorities and plans will put
strategic long-term health and hospital operation I encourage all Victorians to have your say
and development across the state on a firmer and on the priorities outlined in Victorian Health
more rational footing. This will also enable for the Priorities Framework 2012–2022: Metropolitan
first time, a focus on the special place of inter-face Health Plan. Your comments will help inform the
communities – those where the metropolitan and implementation of the government’s vision for our
rural communities intersect – and which have long state’s health service system in the future.
suffered from disconnected planning.
The Victorian Health Priorities Framework
2012-2022: Metropolitan Health Plan sets
out seven priority areas for metropolitan,
rural and regional and health capital planning
into the future:
The Hon David Davis MP
—— developing a system that is responsive Minister for Health
to people’s needs
—— improving every Victorian’s health status
and experiences
—— expanding service, workforce and
system capacity
—— increasing the system’s financial sustainability
and productivity
—— implementing continuous improvements
and innovation
—— increasing accountability and transparency
—— utilising e-health and communications
technology.
vii
Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan viii

Contents
Introduction 1
Executive summary 5
The Victorian health system in 2011 11
Services 12
Funding 15
Governmental responsibilities 17
The performance of the Australian health care system: a snapshot 18
The case for changing the Victorian and metropolitan Melbourne health system 19
Many people do not have optimal health care outcomes 19
There are not enough services when and where they are needed 22
Hospital utilisation could be better managed 24
Demand for health services is increasing rapidly 26
Rising health costs need to be well managed 30
The health workforce is not prepared for future needs 32
People need to be better informed about their health 33
Setting directions for change 35
Immediate action 36
Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan 40
The Victorian health system in 2022 40
Responsive to people’s needs 40
Rigorously informed and informative 40
Pathways that are responsive to people’s needs 44
Priorities Framework 46
Metropolitan Melbourne and statewide service priorities 48
Developing a system that is responsive to people’s needs 49
Improving every Victorian’s health status and health experiences 54
Expanding service, workforce and system capacity 56
Increasing the system’s financial sustainability and productivity 60
Implementing continuous improvements and innovation 62
Increasing accountability and transparency 64
Utilising e-health and communications technology 66
Next steps 68
Appendix 69
Glossary 69
Consultation 73
ix
Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
Introduction
Health is central to our lives. It underpins everything we do,
from choosing the food we eat every day, to consulting a specialist
about a serious life threatening illness.
The Victorian Government is committed to empowering people
to maintain their health and to make informed choices about the
most appropriate health care for their needs. Ensuring that Victorians
have optimal health and health care outcomes is essential to Victoria’s
economic and social future.
The Victorian health system has served our sick and injured people are essential. However,
community well over many decades but it is over many years, funding arrangements by
straining to meet current needs. At present, it is national and state governments have obliged
not designed to handle the rise of chronic and hospitals to become, in addition, providers of
complex conditions nor to fill the growing need urgent health care – regardless of whether or not
to provide individuals with access to information health conditions actually require hospitalisation.
about their health and health care. The current
health service configuration does not fulfil Hospitals were generally built where the majority
people’s desire for health services to be close by of people lived when they were first designed,
and available when they need them. but today many people live well away from these
locations. Many were designed for the medical
Previously, governments could be said to have systems of the past and did not consider people’s
run the public health system as a series of health experiences of going to hospital. In many cases,
factories in which illnesses and injuries are treated. our hospital buildings and technology are
As a result, the existing buildings and institutions, approaching obsolescence.
together with historical patterns of practice,
still influence many decisions made within the Health services often channel people into
system. Connections between publicly-funded, traditional treatment pathways rather than
private, and not-for-profit health services are assisting them to make informed choices
limited. As a consequence we do not use these about which treatments to take and providing
expensive resources as efficiently as possible. people with access to the most clinically effective
Better connections between all parts of the system, and most cost-effective places for obtaining
whether public, private or not for profit would those treatments.
help to maximise the benefits to be gained from
available resources. Furthermore, people are not When people are very unwell or have
fully informed of their options for care nor of the life-threatening conditions, they need to be in
various ways in which they might engage in the hospital. Hospitals will therefore continue to be
management of their own health care. pivotal in the health system. However, in many
instances of urgent medical conditions and
Hospitals have been and largely remain central complex and chronic illnesses, people could
to the health system. Many of our hospitals have receive as effective but more customised,
long histories and iconic relationships with their less costly care in their homes, or in clinics in
communities. Their contributions to the care of accessible community settings.
1Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
Victoria has a significant record of effective Current growth in the population and the
preventive health care, from the early public health steady ageing of our population each present
focus on basic infrastructure and immunisation challenges to health care that our services are
to the long, more recent campaign to reduce struggling to address. With the increasing growth
smoking rates and the poor health caused by in the population, the future acceleration of
smoking tobacco. Today, to ensure we capitalise ageing within the population and the increasing
on our strengths in health and wellbeing, prevalence of chronic and complex conditions,
Victoria needs to develop a systematic and meeting these challenges will become more
comprehensive approach to measuring public difficult and costly unless current planning
health, to informing people about health and develops a better designed and more effective
health care, and to helping people to maintain health system.
and improve their health.
Therefore, this Health Plan reviews Victoria’s
Limitations in the availability and use of relevant health system, sets out the case for change,
information in the health system undermine and proposes critical directions and priorities
accountability in the provision of health services, to guide detailed planning and development
undercutting both health experiences and into the future.
outcomes, and the system’s capacity to achieve
value for taxpayers. The government invites the community’s
feedback and comments on these priorities and
Whilst many people in our community use directions. Consultations will be held to enable
electronic technology to conduct their the community to comment on the identified
day-to-day business, the health system uses a priorities and directions of the Health Plan and
'pens and paper' approach for some of its most contribute to the further detailed blueprints
important tasks. This limit to capacity impedes for the development of health services that the
the fluent flow of information, reduces efficiency, government will publish this year: The Rural and
and increases the risk of error, while denying Regional Health Plan 2012–2022, and the Health
individuals and their health care providers Capital and Resources Plan 2012–2022.
essential information about their treatments and
outcomes in an accurate and timely manner. In formulating this approach and these priorities,
The provision of high-quality health care requires the government has been guided by its
the provision of detailed information to the public Ministerial Advisory Committee (the Committee).
so as to empower every individual to make healthy The Committee is chaired by the Hon. Rob
choices and to live healthy lives. Knowles AO, and its members, who come from
throughout the health care system, are experts
The Victorian Health Priorities Framework 2012– in public health, public and private sector health
2022: Metropolitan Health Plan (the Health Plan) services and health research, teaching and
establishes a framework for the planning and workforce. The advice of the Committee is noted
development priorities for health services across throughout the Health Plan. The priorities are
the whole Victorian health care system by the also informed by advice the government has
year 2022 and then articulates the particular received in workshops and consultations with
planning and development priorities for clinicians, managers, service providers, and other
metropolitan and statewide health services. people familiar with the Victorian health system.
2These consultations confirmed the pressing need As well, they will position Victoria to accommodate
for a strategic approach to system planning in the context in which the plans are being
Victoria, and for the development of a priorities developed: one of significant change and
and directions framework and health plan uncertainty. In particular, significant recent change
commencing with metropolitan Melbourne. through the Council of Australian Governments
(COAG) health reform initiatives that were agreed,
Together with the companion publication, in principle, in February 2011, have substantial
Metropolitan Health Plan – Technical Paper, implications for the state health system and
this Health Plan provides the first phase of a therefore future planning. These discussions have
comprehensive recasting of health planning implications for future Commonwealth funding
in Victoria. They reflect the government’s and governance arrangements for health services.
commitment to improving hospital capacity,
developing community-based health services, The Commonwealth’s commitment to provide
promoting healthy living, providing more an additional $16.4 billion in additional
extensive and higher quality health care health funding over the six years to 2020
information, improving emergency services, remains subject to further negotiation. As well
and creating more effective health care outcomes. recent Commonwealth Grants Commission
recommendations have reduced Victoria’s share
The Metropolitan Health Plan – Technical Paper of national GST revenue by the significant sum
provides, for the first time, the best available of $2.5 billion over the next four years putting
data on metropolitan Melbourne’s health needs additional pressure on Victoria’s ability to fund
and existing health services. Together with the appropriate health services.
government’s new population projections,
forthcoming in June 2011, the Metropolitan Health Meanwhile, national health reform discussions
Plan – Technical Paper will become a key evidence continue and many aspects of health system
base for planning by government and health governance remain unresolved. Victoria is
services across metropolitan Melbourne into committed to sustaining the current strengths
the future. of the Victorian health system and building on
those strengths. In order to respond to, and
Companion Technical Papers for Rural and continue to influence, Commonwealth economic
Regional Victoria and Victoria’s Health Capital and and health reform actions and to drive continuous
Resources, including the health workforce, will be improvements in planning and health services
produced later this year. development, the government will review
the Health Plan every four years, and revise
Together these will assist the government to the related blueprints for health services
take into account the complex economic, development accordingly.
demographic and social factors that affect
Victoria’s health system.
3Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan 4
Executive summary
Being in good health – and getting the care we need when we fall
ill – allows us to live long, fulfilling lives and to participate fully in
our community. But we cannot stay healthy without a strong health
system, and Victoria’s is under strain. The Victorian Government is
committed to confronting the many challenges that lie ahead,
and to creating an equitable, sustainable health system with people
at its heart. The release of the Victorian Health Priorities Framework
2012-2022: Metropolitan Health Plan marks the important first step
on that journey.
The Victorian health system is a complex web with limited ability to innovate and implement
of types and providers of services that are change to historical service arrangements.
managed and funded by the Commonwealth, state,
and local governments, and by private, and not- Overall, the system will face considerable challenge
for-profit organisations. These organisations and in the near future from increasing demand and from
governments vary in their approaches, and operate changing health care needs as the population grows
in an uncoordinated and fragmented way. and becomes older, and disease patterns change.
This complexity makes the system extremely Without change, the health system will struggle to
difficult for patients and clinicians to navigate. It is meet these future needs.
not easy for people to work out where they should
go to for information and get the right care to meet The government has a vision for the future, and a
their needs. plan to get there. Important commitments, have
already been made, such as increasing capacity
The health system is under increasing pressure as by an additional 800 new hospital beds and
a result of population growth, the ageing of the increasing the ambulance services capacity,
population, increasing levels and types of chronic but that is just the beginning.
disease, rapidly evolving technologies and the
rising costs of services. The Victorian Health Priorities Framework
2012–2022: Metropolitan Health Plan provides seven
The publicly funded health system in Victoria priority areas for the development and operation of
comprises a range of service providers that the Victorian health system for the future:
deliver services across the continuum of care.
Services include primary health care services, —— developing a system that is responsive to
such as general practitioners and community health people’s needs
centres; acute health services, including secondary, —— improving every Victorian’s health status and
tertiary and quaternary care provided by hospitals; experiences
and a range of services that seek to provide —— expanding service, workforce and system
coordinated care services for people who need capacity
specialist medical and other clinical care for chronic —— increasing the system’s financial sustainability
and complex health conditions; and public health and productivity
services that aim to improve health by reducing —— implementing continuous improvements
or removing risk factors that adversely affect the and innovation
health of our communities. —— increasing accountability and transparency
—— utilising e-health and communications technology.
These health service providers deliver high quality
health care in buildings that are often outmoded The Framework is the basis of the subsequent
in design and capacity; with financial, time and Rural and Regional Health Plan 2012–2022 and the
demand pressures that continue to increase; and Health Capital and Resources Plan 2012–2022.
5Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
The Victorian Health Priorities Framework the funding source with a focus on building
2012–2022: Metropolitan Health Plan capability and capacity for out-of-hospital care
subsequently proposes the following planning and improving access to primary medical and
and development priorities for metropolitan primary health care.
and statewide health services.
—— Development of the proposed statewide
To deliver a system that is responsive to primary health care plan for a stronger primary
people’s needs: health care system in consultation with the
Commonwealth Government (joint planning
—— The systematic development and for a Victorian General Practice and Primary
implementation of metropolitan municipal Health Plan).
health and wellbeing plans that will address
local population health determinants and —— Joint planning with the Commonwealth,
health care needs and support healthy particularly on the Medicare Locals initiative
communities. In addition, to deliver the to better connect primary care with other
Health Plan’s vision for services in 2022, the community-based services.
government will produce: The Victorian Health
and Wellbeing Plan 2011-2015.1 —— Development of opportunities for greater
private sector collaboration, coordination
—— The development of more sophisticated and integration.
planning approaches and tools such as:
• area-based planning —— Enhancement of existing plans and
• definitions of the role and scope of services development of relevant new plans for the
across the care continuum systematic improvement to care planning
• service capability frameworks that provide and management for specific patient groups
definitions for minimum standards, requiring detailed development of systems
workforce skills, and service arrangements capacity or patient pathways.
to ensure safe, sustainable and effective
health services
• a service-planning and asset development
and management framework that
establishes principles and criteria for
prioritising investments
• analysis of up-to-date and correct
population statistics that is summarised and
distributed to the Victorian health sector to
inform planning.
—— Evaluation of existing and development of new
care settings to ensure services are clinically
effective and cost-effective, irrespective of
1 Section 49 of the Public Health and Wellbeing Act (2008) stipulates
that a State Public Health and Wellbeing Plan must be developed no
later than 1 September 2011, and subsequently every four years after
6 that date.To improve every Victorian’s health status and To expand service, workforce and system capacity:
health experiences:
—— evaluation and development of existing
—— development of Victoria’s Health and Wellbeing efficient and effective service models and
Plan 2011–2015, a prevention strategy and settings, such as Hospital In The Home and
cross-government, cross-sector initiative community health, and development of new
(for release in September 2011) care settings to ensure services are clinically
effective and cost-effective, irrespective
—— a comprehensive metropolitan community of the funder, with particular emphasis on
engagement, development and experience expanding capacity in out-of-hospital care and
plan to enable effective partnership on increasing access to primary medical and
approaches to healthy communities by primary health care
supporting implementation of municipal health
plans for metropolitan municipalities —— allocation of additional investment in
workforce education, training, placements
—— identification of population groups in and role development towards a more
metropolitan municipalities who are interdisciplinary workforce with a more
vulnerable to poor health, and development of extensive range of skills, to improve clinical
interventions that address their health needs outcomes, and care coordination, working with
the Commonwealth, the AMA, nursing and key
—— a metropolitan and statewide strategy for allied health professions.
improving people’s health knowledge and
supporting patient choices, focusing on high To increase the system’s financial sustainability
demand patient cohorts such as the elderly, and productivity:
targeting metropolitan areas of high levels of
disadvantage, targeting at risk cohorts such —— Evaluation of alternative provider setting
as those for whom English is not their first options, such as day hospitals, super clinics
language, and expanding models for advanced and community health centres, to identify and
directives for end-of-life care.2 invest in services that are clinically effective
and cost-effective, irrespective of funder and
funding model.
—— Development of a resource allocation model
supporting greater fiscal management that
is sensitive to population health needs,
productivity, value for money and a more
sustainable system.
—— Refining and expanding the Victorian casemix
funding for inpatient and other health services
to ensure these arrangements meet future
population health needs.
2 Refer to Metropolitan Health Plan – Technical Paper for further details
of health literacy and health information in metropolitan Victoria. 7Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
—— Considering new funding models such as To increase accountability and transparency:
packages of care for targeted patient groups,
such as those with chronic and complex care —— development of a Health Outcomes Framework
needs. Since care for these groups of patients that encompasses the measurement of patient
is provided across the continuum, funding experiences, health outcomes (specifically
from state, Commonwealth, private, including a focus on quality and safety),
not-for-profit and non-government sources efficiency and effectiveness that does not
need to considered, coordinated and not generate any unnecessary additional data
limited by existing barriers. reporting and provides a framework for
coordinating existing reporting processes
—— Incorporating quality and outcome (both state and national)
performance measures into existing
funding models. —— mechanisms for auditing adherence to key
initiatives such as the establishment and
—— Identification of aspects of the metropolitan utilisation of clinical guidelines and patient
and statewide health system that show pathways (including monitoring through
potential for productivity improvement through Clinical Networks)
alternative models of care.
—— review of the existing legislative approaches
To implement continuous improvements that drive governance and accountability
and innovation: arrangements for health services such as
the Health Services Act as amended by the
—— facilitating clinician leadership of evaluations, Health Services (Governance) Act 2000, the
service improvements and innovation Mental Health Act 1986 and the Mental Health
Regulations 1998.
—— development of a more effective central clinical
data acquisition and management system To improve utilisation of e-health and
(including advanced analysis capability) that communications technology:
generates the evidence base for improved
or innovative clinical practice and population —— Articulate the system requirements and
health interventions, and supports the deliverable outcomes that increase clinical
development of better clinical pathways and time, ensure optimal health information and
service planning. reduce administrative time for both the patient
and system, to be developed in the Health
Capital and Resources Plan.
8Throughout this year, further plans for rural and
regional Victoria, and health capital and resources,
will be published, based on the Victorian Health
Priorities Framework 2012–2022: Metropolitan
Health Plan. Together, the health plans will guide
the development and operation of Victoria’s public
health services and enable the public and private
sector to work together to deliver improved health
services for all Victorians.
Over the coming two months, the government
wants to learn what the community and
the health sector think about implementing
the Victorian Health Priorities Framework
2012–2022: Metropolitan Health Plan. An extensive
consultation process will be undertaken, which
will include open forums, focussed small group
sessions, and many discussions with interested
parties around the state. In addition, the
government welcomes written submissions on this
paper. Further information about the consultation
process, including dates and other details,
is available online at http://www.health.vic.gov.au/
healthplan2022
9Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan 10
The Victorian health system in 2011
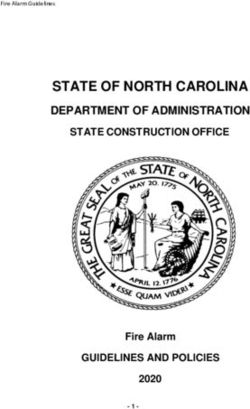
In the Victorian health system, there is a range The range and mix of services provided is typically
of services that are funded through multiple referred to as a continuum of care (Figure 1).
sources and across a broad range of settings.
Figure 1: Victoria’s health system – a representation
health
continuum promotion primary health
of care
Z and disease care
secondary care tertiary care Y
prevention
Specialised acute
Specialised acute
Health protection and subacute care
Primary medical care and subacute care
program in hospital and
in hospital settings
non hospital settings
Health promotion
Primary health care in
and illness prevention Residential care
community settings
programs
service
types
Public health and Assistance for
wellbeing programs independent living
Other sectors,
locations and
mediums
Public hospitals and Public hospitals and
Community health services
health services health services
General practitioners Private hospitals Private hospitals
Community health
Non-government organisations
service services
providers
Local government Aged care facilities
Psychiatric disability
Public hospitals and health services
services
General practitioners
State government Private health and Local government Commonwealth
funding individual contributions Government funding
11Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
Services
Health services in Victoria cater for the full range health care system. As the number of people
of health care needs, from prevention and with chronic and complex conditions increases,
primary health care services typically delivered in primary health care providers are developing new
community-based settings through to acute and service models that provide more specialised and
emergency care services provided in hospital coordinated care. In particular early intervention
settings. All levels of government and a complex and team care programs are being developed.
range of service providers, both public and
private, intersect with each other in the provision Primary health care includes general practice
of this continuum. services, including medical and nursing services,
community health including community nursing,
This continuum can be broadly described allied health, public oral health services and
as comprising four clusters of services: child and maternal health services, and private
public health, primary health care, secondary care allied health including oral health, optometry,
and acute care. psychology or physiotherapy services.
Specialised services to meet local community
Public health includes health promotion and needs have been developed across Victoria’s
disease prevention activities undertaken at both primary health care system including the
a population and individual level. At a population Early Intervention in Chronic Disease program,
level these activities include infrastructure services refugee health nurses and sexual health clinics.
that ensure clean water and clean air, as well as
social marketing campaigns about the dangers Like most parts of the health system, primary
of smoking or the importance of healthy eating. health care involves a mixture of public and private
For individuals these activities can include funding, with a mix of local government, public
programs that provide education to people and private service providers. Funding for general
at risk of developing a chronic condition such practitioner services principally comes from the
as diabetes. Commonwealth Government, but also has
out-of-pocket components. Community
The state government, in particular through the health services are funded principally by the
Department of Health and its funded agencies, state government, with a minor out-of-pocket
plays the most significant role in meeting public component. Private allied health services are
health needs. Local governments, via their many funded by a mixture of out-of-pocket expenses
services and municipal health and wellbeing and private health insurance subsidies. Many low
plans also play important roles in promoting income earners are able to access a core suite of
healthy communities. Additional providers and primary health care services with no or minimal
peak groups, such as VicHealth, a statutory out-of-pocket expenses.
authority with an independent chair and board of
governance, also play a critical role in promoting In Victoria and metropolitan Melbourne the
healthy individuals and communities. primary health care sector works in partnership
through Primary Care Partnerships. Through
Primary health care is the most commonly their activities Primary Care Partnerships aim to
accessed component of the health system. support primary health care providers working
It is most people’s first point of contact with collaboratively to improve the health and
the health system often to treat specific and wellbeing of their catchment's population by
immediate illnesses. Those people with ongoing better coordination of planning and service
or more complex conditions will have regular and delivery in response to identified needs.
ongoing contact with various parts of the primary
12In the future, Medicare Locals will have a role in Acute health care is accessed via emergency
supporting coordination across the primary health departments or outpatient clinics following a
care sector. The scope and function of this role referral from a primary health care professional.
is still being developed by the Commonwealth In emergency departments patients with acute and
Government. The impact of this on the primary immediate health needs are treated by a range
health care sector is unclear. of clinicians. Those requiring ongoing care are
admitted to the hospital for ongoing care. Those
Secondary care is typically provided by requiring short-term care are cared for within the
specialist health professionals and for people emergency department. In the public hospital
with specific illnesses and chronic and complex system patients requiring either emergency or
conditions. Examples include radiology and elective surgery will be prioritised based on the
pathology services or specialist services required acuity of their condition. Surgical hospital care
by a general practitioner as more detailed is provided on multi-day and, increasingly,
investigations of specific and immediate illnesses. same-day bases.
Ongoing secondary care is also provided by
specialist clinicians for a chronic or complex Victoria has an extensive network of public
condition. As new models of care are developed hospitals governed by health service boards,
for these conditions greater integration of with 86 independent hospital boards operating
secondary and primary health services is across the state. This includes 21 public health
occurring. Following treatment in an acute services (major health service networks),
facility, secondary care will often be provided 22 sub regional health services and 43 small
either in a hospital or through community care rural health services. These health services are
when the person returns to their home. governed by the Health Services Act 1988,
These services include rehabilitation, home which sets out their obligations to meet the health
nursing, and attendance at a specialist cardiac needs of their local communities. In Victoria the
clinic when recovering from cardiac surgery. private hospital sector comprises free-standing
day procedure centres, private hospitals operating
In Victoria, state government funding for on a not for profit basis (34 facilities) and a
secondary care includes some inpatient services commercial for profit basis (128 facilities).
and specialist ambulatory care clinics, such as Private hospitals are also regulated under the
those for continence, chronic pain management, Health Services Act 1988.
dementia and memory loss. Other secondary
services include Commonwealth-subsidised The principal source of funding for public
services by private specialist medical practitioners hospitals is the state government (although the
and diagnostic services to whom patients are Commonwealth indirectly provides about 40 per
referred by their general practitioner. cent of this funding through the Australian Health
Care Agreement). Public hospital services are free
Acute care, often referred to as tertiary and to the community, with generally no out-of-pocket
quaternary care, is typically provided in a hospital expenses. Private hospital services are funded by
setting as well as a range of same day surgical private health insurance, Medicare rebates, and
clinics and day hospitals and community-based out-of-pocket expenses.
agencies. Acute care is provided by both public
and private providers. There are two other important sub categories
of services provided across Victoria, these are
residential and community care.
13Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
Residential care is provided to people who Victorians access services from throughout the
can no longer be cared for in their home due to continuum of care according to their needs.
disability or the effects of ageing. Residential care When one part of the system is not working
is categorised as secondary care. These services properly, or is inadequately funded or
are provided through care facilities that provide inaccessible, the burden shifts to another part
for the full range of day to day needs of individuals of the system – including to public hospitals,
via personal care, medical and psycho social which are the most costly and possibly the most
services. Facilities that provide these services are pressured parts of the health system.
owned and run by public, private not for profit
and for profit organisations. The sources The services in the metropolitan health system
of funding for these services include the
Commonwealth and state government as well All elements of the service system described
as out-of-pocket expenses. previously operate within metropolitan Melbourne.
Public health care is provided through a system of
Community care includes a range of services integrated services located in multiple campuses
provided on an ongoing and short-term basis within broad geographical areas. It includes:
to people with either short or long-term health
conditions or personal care needs. Community —— statewide specialist centres of excellence
care is generally a component of primary health which lead the provision of complex,
care but can also include some secondary high acuity health care
services. These services include nursing, personal —— specialist services in major tertiary hospitals
care such as assistance with showering and —— a range of general acute and/or subacute
home cleaning or the provision of meals. The aim care for local communities
of these services is to enable individuals to be —— ambulatory services which provide same-day
cared for in their home for as long as possible. procedures and other ambulatory care.
Services are provided by a range of community-
based providers. The sources of funding for these Services range across acute, subacute, aged care,
services include the Commonwealth and state mental health and primary care. Integrated health
government as well as out-of-pocket expenses. services, such as Southern Health and Peninsula
Health, provide all levels of care within their region
People move through the continuum of care through services in various locations. Specialist
provided by these services according to their hospitals, such as The Royal Women’s Hospital,
health needs. Most Victorians navigate between provide the full range of services from specialist
the various services as and when they need to. to ambulatory, but only for a particular patient
However, for some people, particularly those with category or clinical specialty.
long-term multiple needs, including people with
chronic conditions, the aged and people with Each metropolitan health service collaborates
mental health problems, navigation is difficult with community-based providers such as general
and there is a need to ensure that these particular practitioners (GPs), community health services
patient groups have care that is coordinated and (CHS), community dental services and other health
integrated in order to facilitate optimal health care services throughout Victoria. Metropolitan
outcomes and to minimise duplication of services health services also play a role in teaching, training
and costs. Primary and secondary health care and research.
providers play a critical role in coordinating care
for these groups of clients.
14Funding
Funding and service provision structures in Private insurance contributes 7.6 per cent
Victoria, and, more generally, in Australia, of total health expenditure. Since 1999, at least
have evolved over time in response to 30 per cent of a private health insurance premium
contemporary economic and social policies and has been paid by the Australian Government
population health needs. The resulting system is through a rebate. In mid-2010, 44.6 per cent of the
complex and multi-layered, combining public population had private hospital insurance.
and private service provision, Commonwealth,
state and private funding, and a multiplicity Out-of-pocket spending accounted for
of service types largely shaped by funding 16.8 per cent of total health expenditure in
sources and requirements. 2007–08. Most of this expenditure was for
medications not covered by the PBS, dental
In 2008–2009, Australia spent $112.8 billion on services, aids and appliances, and co-payments
health goods and services – that is, on average, on medical fees.3
$5,190 per Australian. Of the total, 94.9 per cent
($107.1 billion) comprised recurrent expenditure Victorians have access to medical and
on health goods and services. The remaining pharmaceutical services through the Medicare
5.1 per cent was capital expenditure ($5.7 billion). and Pharmaceutical Benefits Schemes.
These schemes are regulated and administered
Spending on public hospital services in 2008–09 by the Commonwealth Government, and subsidise
is estimated to have been $33.7 billion; many pharmaceuticals, specialist medical
on medical services, $19.8 billion; and on and surgical care, general practitioners,
medications, $15.2 billion. and (for people who have chronic conditions)
limited dental and allied health services.
In 2008–2009 recurrent expenditure in Victoria
for public acute and psychiatric hospitals Close to half of Victorians maintain private health
totalled $8.2 billion and employed over insurance, subsidised by the Commonwealth
66,000 staff. Government. Private health insurance underpins
private hospital utilisation and other private
In 2007–2008, governments funded 69 per health care services such as physiotherapy,
cent of total health expenditure, the Australian dentistry, optometry, and podiatry, as well as
Government funded 43 per cent and state and complementary medicine services. Approximately
territory governments funded 26 per cent. one-third of hospital beds are in private hospitals,
complementing the public system by providing
additional inpatient capacity and enabling choice.
3 Australian hospital statistics 2008–2009, AIHW 2010, Cat no. HSE 84.
Canberra: AIHW. 15Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
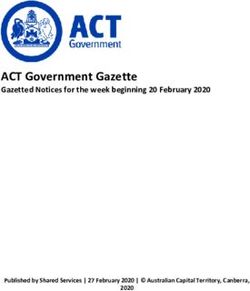
Figure 2: Recurrent health expenditure, by area of expenditure and source of funds,
current prices, 2008–2009
35000
Non-government
(total $31.784 billion)
30000 State/territory and
local governments
(total $27.160 billion)
25000 Australian Government
(total $48.155 billion)
20000
$ million
15000
10000
5000
0
Public hospital Private Medical Dental Other health Community and Medications Aids and Other health
services hospitals services services practitioners public health appliances
Notes: Public hospital services exclude certain services undertaken in hospitals. They sometimes include services provided off site
such as Hospital In The Home, dialysis and other services.
'Other health' comprises patient transport services, administration and research
16Governmental responsibilities
The Victorian Government’s primary responsibility in supporting independent living through
in health is to manage the Victorian public health the Home and Community Care Program.
care system and to support the health and
wellbeing of all Victorians. The government also The Council of Australian Governments (COAG)
is accountable for ensuring the most effective signed a new Heads of Agreement in February
resource allocation decisions are made within 2011.4 Although debate on national health
the limitations of the overall health budget. reform continues, this agreement has confirmed
In 2009–2010, the Victorian Government health and strengthened the role of the states as the
care budget was $12.5 billion, that is, around one managers of the public health system.
third of all Victorian Government expenditure.
Many of the initiatives agreed by COAG
The Victorian Government is responsible for remain to be decided. The roles, remits and
services delivered in public hospitals. Public inter-relationships of the National Health
hospitals deliver a range of services, including Performance Authority, Medicare Locals,
emergency care, surgery, multiday medical care, the National Health Pricing Authority, the Australian
sub acute and rehabilitation care, and palliative Safety and Quality in Health care Commission,
care. In addition, the Victorian Government also and the National Preventive Health Agency
funds ambulatory care services through specialist have not been settled. Nor are the intricacies of
clinics, some located in community settings, the workings of the national funding pool clear.
and community health centres throughout Most importantly, from the perspective of the
Victoria that provide a range of primary health Victorian health system, the impact these changes
care services such as community nursing, allied will have on the state as system manager, and on
health, community development, chronic disease Victoria’s health services, is as yet unclear.
management and health promotion services.
These services complement the primary health The Victorian Government sees great benefit in
care services funded by the Commonwealth Victoria’s unique model of Home and Community
Government. The Commonwealth has committed Care (HACC) service delivery, which involves a
to the establishment of Medicare Local close partnership with local government.
organisations which are to plan and support HACC services are particularly important in
the delivery of face-to-face GP services outside supporting Victorians at vulnerable points in
normal hours. their own homes and it is at these points that there
is on many occasions close interaction with the
The Commonwealth and Victorian Governments health care system.
fund a wide range of additional health services,
including health promotion, mental health, The support provided by HACC to patients is an
limited dental health, rural and Aboriginal health important factor in avoiding hospitalisation and in
programs, and health services for war veterans. supporting discharge of patients from hospital.
The Commonwealth Government provides the Current HACC arrangements remain a formal
greater proportion of funding for residential aged point of debate with the Commonwealth
care and various funders are responsible Government. The Victorian Government, together
for providing services to people whose needs with local government, is seeking to retain the
are met by community-based services. In Victoria, benefits of Victoria’s unique HACC model of
state and local government play a significant role service delivery.
4 For details about the National Health Reform,
see 17Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
The performance of the Australian health care system: a snapshot
Australians in general receive very good These rankings provide a focus for what needs
health care. By international comparison, to be done to improve the Victorian health care
the Australian health care system ranks third of system. Additional areas for improvement include
seven Organisation for Economic Co-operation overall health status, patient outcomes and
and Development (OECD) countries. experience, the health knowledge of the Victorian
community, managing accelerating demand, the
Australia ranks highest of the seven countries over-reliance on hospitals, and a discrepancy
compared for living long, healthy lives, and between service and workforce structures, on the
second in efficiency, but lower in quality of care one hand, and on the other hand, the distribution
and equity, and joint lowest for access. of population needs.
Recent inquiries, such as the reports of
the National Health and Hospitals Reform
Commission, have pointed to the need to change
current Australian health system arrangements.
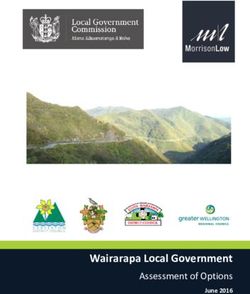
Figure 3: Comparison and ranking of national health care systems,
based on Commonwealth Fund surveys5
australia canada germany netherlands nz uk usa
Overall ranking 3 6 4 1 5 2 7
Quality of care 4 7 5 2 1 3 6
Access 6.5 5 3 1 4 2 6.5
Efficiency 2 6 5 3 4 1 7
Equity 4 5 3 1 6 2 7
Long healthy lives 1 2 3 4 5 6 7
Health expenditure
per capita (US$) $3,357 $3,895 $3,588 $3,837 $2,454 $2,992 $7, 290
5 Davis K, Schoen C, andStremikis K, June 2010, ‘Mirror, Mirror on the
Wall: How the Performance of the U.S. Health care System Compares
18 Internationally, 2010 Update’, The Commonwealth Fund.The case for changing the Victorian and metropolitan
Melbourne health system
The Ministerial Advisory Committee (the Committee) and the
preparatory health service consultations have identified a range of
issues that demonstrate the need for improvement in current health
services and health outcomes. These have been informed by the
Metropolitan Health Plan – Technical Paper.
Many people do not have optimal health care outcomes
A number of factors increase the risk of poor likely to suffer poor health, chronic conditions,
health and poor health outcomes for some and ambulatory-care sensitive conditions.
particular population groups. These include Some communities have less access to
education, income, housing, employment status, primary care services, and have a higher
geographical location and cultural background. prevalence of obesity, poor dietary choices,
and unhealthy behaviours (such as smoking).
Some groups in the population are more likely A number of these area- or population-based
to experience poor health and illness than others. differences are detailed within the
For example, a higher proportion of the rural Metropolitan Health Plan – Technical Paper.
population than of metropolitan Melbourne is
Figure 4: Potentially avoidable hospital admissions (ambulatory-care sensitive conditions)6
60
50
40
Per 1000 population
30
20 Least disadvantaged
quintile
Most disadvantaged
10 quintile
Victoria
0
2000–01 2001–02 2002–03 2003–04 2004–05 2005–06 2006–07 2007–08 2008–09 2009–10
Health Information Surveillance System (VHISS)
6 Note that the drop in rates of ambulatory-care sensitive conditions
between 2007–08 and 2008–09 are due to changes in coding practice
for diabetes and gastroenteritis. 19You can also read