Utility and/or Rent Assistance Application - WestCAP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Utility and/or Rent Assistance
Application
Spanish: http://homeenergyplus.wi.gov/docview.asp?docid=29053&locid=25
Si necesita servicios de interpretación: envíe un correo electrónico a westcap@wcap.org para obtener ayuda.
Hmong: http://homeenergyplus.wi.gov/docview.asp?docid=29052&locid=25
Yog tias koj xav tau cov kev pabcuam intrepreter thov xa email mus rau westcap@wcap.org.
How do I qualify?
Your household may qualify if at least one or more individuals in your home meet the following:
• Has a household income at or below 80% of the county median. Link:
http://homeenergyplus.wi.gov/docview.asp?docid=29022&locid=25
How do I apply?
1. To determine income eligibility you must complete a WHEAP Energy Assistance application for this
program year.
2. Provide proof of previous month’s income that may include:
• Wages
• Unemployment compensation
• Self-employment income
• Social security/Supplemental and Social Security Disability Insurance
• Statement of person-to-person loan or gift of money
• Pensions, annuities, IRA’s
• Child support payments
• Temporary Assistance for Needy Families (TANF)/WI Works (W2) benefits
3. You may proof of income with submittal of your completed application to westcap@wcap.org
If you have any questions or need any further information or assistance, please do not hesitate to schedule a
phone appointment at www.westcap.org or contact us at 715-265-4271. Please understand that we are
experiencing a high volume of calls at this time, but we will return your call as soon as possible.
STATE OF WISCONSIN HOME ENERGY PLUS PROGRAM
DEPARTMENT OF ADMINISTRATION http://homeenergyplus.wi.gov
DIVISION OF ENERGY, HOUSING AND /
COMMUNITY RESOURCES
(R07/2021)
Home Energy Plus Application
To apply for Energy Assistance online go to https://energybenefit.wi.gov
For Office Use Only – shaded areas to be completed by agency
Application Date (mm/dd/ccyy): Worker Number: Withdrawn
Outreach Type: Local Agency Alternate Site ____________________________ Home Visit Mail Phone
This form is authorized under Wisconsin State Statute 16.27(2)(a). All information on the application is required in order to determine
eligibility for benefits under the Wisconsin Home Energy Assistance Program and the Wisconsin Weatherization Assistance
Program. Collection of your Social Security number is not prohibited by federal law and is required for tracking applicant benefits
granted by this Program. By providing application information, you are authorizing the Wisconsin Department of Administration and
its authorized agents to verify the data provided against federal, state, county, energy provider, employer and landlord databases or
records. The information collected on this form may be disclosed to energy programs operating under the Wisconsin Public Benefit
Program Authority or Wisconsin Public Service Commission Approval, and may be used for the purposes of referral, research,
evaluation, and analysis.
1. Territory (County or Tribe) in which you live: Person ID (This number is provided by the Program):
2. First Name: Middle Initial: Last Name: (As shown on Social Security card)
3. Alias First Name (if applicable): Alias Last Name (if applicable):
4. Birth Date (mm/dd/ccyy): 5. Gender:
M F
6. Primary Phone Number:
( ) Home Work Cellular Contact
Secondary Phone Number:
( ) Home Work Cellular Contact
7. Email address:
8. Preferred method of household communication: Primary Phone Email Mail Text message
9. Housing type you live in:
Single family house For office use only: Ineligible Dwelling
2 to 4-unit building (including condos) – Number of units/apartments in your building:
Apartment or multi-unit building (including condos) – Number of units/apartments in your building:
Mobile home
Rooming house, motel, hotel, YMCA or YWCA
Other (describe)
10. Mailing Address (if different than residence address):
Address
City State Zip
11. Residence Address (must complete):
Address
City State Zip
112. Own or rent your residence: (choose rent if no one living in the home owns the residence)
NOTE: Choose ‘Own’ if you own
Own Rent If rent, the following landlord information is required: a mobile home and pay lot rent
13.
Management Company or Business Name (if applicable): Point of Contact or Landlord Name:
Landlord Email Address: Landlord Phone Number:
( )
Landlord Address:
City: State: Zip:
13. Identify the number of rooms in your residence: Worker completes total number of rooms: _______
Living Room Dining Room
Kitchen Family Room
Number of Bedrooms Den/Office
List any other rooms:
Do not count bathrooms, unfinished basements, laundry rooms, entryways, hallways, unheated attics and porches or closets.
14. Select the response that best describes your living arrangement as of the date of this application:
Live in a group home, half-way house, Community Based Residential Facility (CBRF) or foster home
Live in a nursing home
Live in a government institution or prison or jail
Are currently in a homeless situation moving to a permanent residence
None of the above
15. Do you receive rental assistance (Section 8 or other government assisted housing)? Yes No
16. Is there a guardian or designated representative? Yes No If yes, complete representative information:
Authorization of Representative Legal Guardian Power of Attorney (POA) Protective Payee
Guardian/Representative Name: Guardian Phone Number: ( )
Guardian/Representative Address:
City: State: Zip:
OR: List someone you are authorizing to discuss your application with who is not listed as a guardian or designated
representative: Relationship:
17. Are you (the applicant) a student under the age of 25 and enrolled at least half-time in an institution of higher learning?
Yes No
If yes, check any of the following conditions that meet your situation:
Currently working twenty or more hours per week making at least minimum wage
Financially responsible for a child under age 18 who is living with you
Physically or mentally disabled (verification needed from government program)
Receiving Unemployment Compensation (UC) benefits resulting from TAA / NAFTA (must be a full-time student)
Receiving TANF or W-2 Benefits
Spouse lives with you who is not a student
None of the above apply
18. Applicant’s Ethnic Group (check one):
American Indian or Alaskan Native Hispanic Not Reported
Asian or Pacific Islander White, not of Hispanic origin
Black, not of Hispanic origin Other
19. Is anyone in the household under the age of 18 and related to any adult household member? Yes No
220. Enter total number of household members (including the applicant listed on page 1): _____________
Identify the preferred household language:
If preferred household language is not English, list an English-speaking household member or representative who can answer
application questions. (Completing this field is providing authorization for the Program to discuss your application with this person.)
Name: Phone Number: ( )
HOUSEHOLD MEMBERS:
Worker
• List every person who lives at your residential address Instructions at bottom of page are related to these initials
today. fields below by number indicated:
•
Is this person a U.S.
shared placement?4
Worker will contact you for Social Security numbers for first
Is this a child with
time applicants and new household members.
(M)ale, (F)emale
Military Service3
Is this person
(Office use only)
•
FoodShare2
Line 1 must be the applicant listed on page 1 (date of birth
disabled?
Gender1:
and gender must match information entered on page 1).
Citizenship5
Citizen?
Birth Date
mm/dd/ccyy
Name Enter “Y” for Yes and “N” for No
Applicant from page 1 must be listed here
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
1 Indicate the gender the individual most closely identifies with.
2 Enter “Y” in the box for FoodShare if that person received FoodShare in the month prior to the date of this application.
3 Enter “Y” in the box for Military Service, if that person is serving or has ever served, or is a surviving spouse of someone who served
in a branch of the United States military (Army, Navy, Air Force, Marine Corps, Coast Guard) as active duty, Reserve, or National
Guard.
4 List
all children living in your household who are in a minimum of 50% shared placement. Verification of child placement (such as a
copy of court order) is required when children are living in a shared physical placement living arrangement.
5 The office worker will enter “C”, “E”, or “I” in the Citizenship box to identifiy if that person is a U.S. (C)itizen, (E)ligible Non-Citizen, or
(I)neligible Non-Citizen. Worker who completed this box should initial at the top of the column.
3INCOME:
Is your household a zero income household? Yes No
Note: A zero income household has no sources of income, either earned or unearned, in the month prior to date of application.
Income Types: If anyone in the household is paying court-ordered child support (CS Paid) include that in the income below. Cash jobs
should be reported as Self-Generated Income.
(A) Alimony Received (GF) Gift/donations (SSDI) Social Security Disability Insurance
(CS RECD) Child Support Received (GV) Government Relief or Disaster (SSI) Supplemental Security Income
(CS Paid) Child Support Paid (LC) Land Contract Payment2 (T) TANF/W2
(CTS) SSI Caretaker Supplement (O) Other (TR) Tribal per Capita1
1
(DL) Disability Long-term (P) Pensions, Annuities, and IRAs (UC) Unemployment Compensation3
1
(DS) Disability Short-term (R) Rental Income (V) Veterans Benefits
(D) Dividends/Interest1 (SE) Self-Generated Income1 (W) Wages & Tips3
(G) Gambling/Lottery/Bingo (SP) Spousal Impoverishment (WK) Workers Compensation
(GR) General Relief (SS) Social Security
Instructions: List all household gross income in the chart below. Enter income code above in the income type column and where that
income comes from in the income source column. REQUIRED: Proof of gross income received is needed for each income listed below.
Income Prior Month Worker
Household Member’s Name Income Source4 Verification Item
Type Initials
Example:
W ABC Corporation $1,278.25 Attach Documentation
John Doe
Total Monthly Household Income
1 Thisincome is based on the average of the prior 12 months of income. A copy of the most recent federal income tax return is required
to complete this application.
2 Only the interest income received is counted. A copy of the amortization schedule or the 1099 form issued for tax purposes will need
to be provided to complete this application.
3 Wages:provide verification of wages that were received in the month prior to date of application based on check date.
If the household member is a seasonal employee (a person whose main source of income is earned in less than 12 months of a
calendar year), the annual income must be provided for both wages and unemployment compensation received in the prior tax year.
Copies of the W2 and 1099 forms will need to be provided to complete this application.
4Source examples: wages, include name of employer such as ABC Corporation; if self-employed, include type of business or business
name; if pension, include the payee of the pension; if interest and dividends, include the payee of this income.
4ENERGY USAGE: Complete every section of energy usage – continued on next page
Primary Heat Source: Select one:
Electric Heat Fuel Oil Natural Gas Propane Wood or Other
Select how the fuel bill is paid (check only one):
Directly pay the bill sent from the energy supplier (must complete account information)
Rental payment includes the energy in the monthly rent payment (not government assisted housing)
Separate payment is made to the landlord, mobile home park owner, or no direct account with a vendor
Do not pay: energy included in the monthly rent when residing in government assisted housing or renters who pay neither rent or
heating/electric costs because of an in-kind arrangement
Name on Account: _____________________________________________________________
Is this account in a household member’s name? Yes No
If no, the account is in the name of: A Deceased Spouse A Protective Payee Other
If other, identify relationship of the account holder:
Is this meter shared with another dwelling unit? Yes No
Is there business or recreational use on this account (including farm, other self-employment, pool or hot tub)? Yes No
Vendor Name: Vendor Number (office use):
Account Number: Annual Fuel Costs:
Electric (Non-Heating): If your primary heat source (above) is electric, do not complete this section.
Select how the electric bill is paid (check only one):
Directly pay the bill sent from the energy supplier (must complete account information)
Rental payment includes the energy in the monthly rent payment (not government assisted housing)
Separate payment is made to the landlord, mobile home park owner, or no direct account with a vendor
Do not pay: energy included in the monthly rent when residing in government assisted housing or renters who pay neither rent or
heating/electric costs because of an in-kind arrangement
Name on Account: _____________________________________________________________
Is this account in a household member’s name? Yes No
If no, the account is in the name of: A Deceased Spouse A Protective Payee Other
If other, identify relationship of the account holder:
Is this meter shared with another dwelling unit? Yes No
Is there business or recreational use on this account (including farm, other self-employment, pool or hot tub)? Yes No
Vendor Name*: Vendor Number (office use):
Account Number: Annual Fuel Costs:
*A vendor must be entered showing who provides electricity to this dwelling even if electricity is included in rent or a separate payment
is made to landlord.
5Additional Energy Account Information – answer the following questions regarding the household energy situation.
These answers will not affect your benefit amount but must be answered.
Primary Heat Source:
If your primary heat source is natural gas or electric, have you received a past due or disconnect notice within the last 90 days?
Yes No Does not apply
If your primary heat source is propane or fuel oil, does your tank currently have equal to or less than 20% of fuel remaining?
Yes No Does not apply
Hot Water: Identify fuel type that heats the water in your home:
Electric Fuel Oil Natural Gas Propane Wood or Other None
Supplemental Heat Source (Do you use additional heat sources such as fireplace, wood burner, space heaters, or other alternate
heating type from the primary heat?) Identify, if any, what supplemental heat is used in your home (select only one):
Electric Heat Wood or Other (Specify other) None
Air Conditioning:
Identify the method used to cool your home (select only one): Central Air Wall/Window Unit A/C None
PLEASE SIGN PAGE 7
Proof of income is required to complete the application
Case Notes
6Certification Page
Person ID: Application #:
Read each item on this page before signing the application.
If you do not understand any item, ask the worker for assistance.
1. I understand I am responsible for providing all required information within 30 days of the date of this application or the
application is void and will be denied. I may reapply but a new application will be required.
2. I understand I am responsible for reporting the names of all persons living at my address and the Social Security number and
income of all persons in my household. Collection of Social Security number is not prohibited by federal law and is a required
data element for tracking applicant benefits granted by this Program. Failure to provide this information will result in delayed
processing of my application and the inability to determine benefit amounts.
3. I understand I am responsible for using the payments I receive to pay for the heating/electric costs for the residence listed in
my application or for paying the heating/electric costs for any future permanent residence I may move to in Wisconsin.
4. I understand I have the right to apply for Energy Assistance benefits and to receive either a payment or letter of explanation
within 45 days from the date the application process is completed. I understand that the payment or letter of explanation may
be delayed depending on when the Program year begins and/or when payments are being processed.
5. I understand I have the right to request a fair hearing within 15 days after receiving a notification letter if I believe my Energy
Assistance application has not been processed timely, has been incorrectly denied, or my payment is incorrect. I may also
request a fair hearing if I have not received payment or explanation. I may ask for a fair hearing by contacting the local office
that processed my application because I applied directly to their office or submitted an online application.
6. I understand I have the right to file a complaint if I believe I have been discriminated against in any unlawful way. I may file a
complaint by contacting the authorized person within my county or tribe.
7. I understand that by providing application information I am authorizing the Wisconsin Department of Administration and its
authorized agents to verify the data provided against federal, state, county, energy provider, water utility, employer and
landlord databases or records.
8. I understand that by providing the account numbers for my household energy supplier(s) I am authorizing the energy
provider(s) to provide details about the account and energy use to the Wisconsin Department of Administration for the
purposes of eligibility determination of this and future applications, benefit determination, and program evaluation and analysis
including before and after receiving any weatherization services.
9. I understand that the rights, requirements, and authorizations I certified to on this application may also apply to multiple heating
seasons, crisis, and furnace applications, when supplemental benefits are issued, and to outreach activities.
10. I understand the information collected on this form may be disclosed to energy programs operating under the Wisconsin Public
Benefit Program Authority, Wisconsin Public Service Commission Approval, or other programs administered by the State of
Wisconsin and may be used for the purposes of referral, research, evaluation, and analysis.
11. I understand if eligible for energy assistance benefits, I may be referred to other residential weatherization and/or energy
programs. I authorize the weatherization agency to provide weatherization services to my residence. If I am not the owner of
the residence, I authorize the weatherization agency to contact my landlord and I will cooperate with the agency providing
weatherization services.
I certify that the information on this application and all information given in connection with this application are true and complete
statements of facts. I further certify that I have read and understand the statements above. I understand that I may be required to
provide proof of any information on this application and that giving false information will invalidate this application, require the return of
any benefits received and possibly subject me to criminal prosecution. By typing my name in the ‘Applicant Signature’ field, I indicate
that I am the person named, and this entry is the legal equivalent of a manual/handwritten signature. I further understand that I may
print out the document and sign by hand.
Applicant Signature Date (mm/dd/ccyy)
FOR OFFICE USE ONLY
Agency Worker Signature Date (mm/dd/ccyy)
I certify that I have verified the information on this application in accordance with Home Energy Plus policies and to the best
of my knowledge this information is complete and accurate. I further certify that I do not have a personal relationship to any
individual listed on this application in accordance with the Home Energy Plus Conflict of Interest Policy.
This application can be made available in alternate formats to individuals with disabilities upon request.
7NOTE: Paper applications must be mailed to the local agency.
Send to: West CAP, westcap@wcap.org or PO box 308, Glenwood City, WI 54013
If the local agency address was not provided, you can obtain the correct mailing address for your
local agency from:
http://homeenergyplus.wi.gov/
Click on the ‘Where to Apply’ tab and select the county or tribe where you live.
Agency: Attach a mailing sticker here with correct mailing address for application to be submitted.
DID YOU SIGN PAGE SEVEN?
---------------------------------------------------------------------------------------------------------------------------------------
Please tell us how you heard about the Energy Assistance Program this year:
Insert in my utility bill Bus ad
Phone call from agency Email from agency
Mailed notice from agency Website (Identify Site)
Radio (Identify Radio Station) TV news
(Identify TV Station)
Notice in local paper or mailer
(Identify paper or mailer)
Energy Assistance flier
(Where did you get the flier)
Other
(Identify the source)
To apply online for Energy Assistance go to https://energybenefit.wi.gov/
8Rent Assistance Application
Complete the following fillable form if you
need rental assistance.
Spanish: http://homeenergyplus.wi.gov/docview.asp?docid=29053&locid=25
Si necesita servicios de interpretación: envíe un correo electrónico a westcap@wcap.org para obtener ayuda.
Hmong: http://homeenergyplus.wi.gov/docview.asp?docid=29052&locid=25
Yog tias koj xav tau cov kev pabcuam intrepreter thov xa email mus rau westcap@wcap.org.
How do I qualify?
Your household may qualify if at least one or more individuals in your home meet the following:
• Qualifies for unemployment, or has experienced a reduction in household income or an increase in major
costs/financial struggles due to COVID-19.
• Experiencing a risk of being evicted or losing your home.
• Has a household income at or below 80% of the county median.
Link: http://homeenergyplus.wi.gov/docview.asp?docid=29022&locid=25
How do I apply?
1. To determine income eligibility you must complete a WHEAP Energy Assistant application for this
program year. (Previous form included)
2. You must complete an income attestation form, if COVID-19 pandemic has had a financial impact on
your household or at risk for homelessness.
3. You must also complete a renter verification form found within this document or online (must be
completed by you and your existing landlord). www.westcap.org Home Page.
4. Email your completed application along with income proof to westcap@wcap.org. Your landlord may
choose to send their landlord information separately.
Should you have any questions or need any further information or assistance, please do not hesitate to
schedule a phone appointment at www.westcap.org or contact us at 715-265-4271. Please understand that we
are experiencing a high volume of calls at this time, but we will return your call as soon as possible.Wisconsin Emergency Rental Assistance (WERA) Program
Income and Housing
Attestation due to COVID-19
Shaded area to be completed by WERA agency.
Eligible clients (i) qualified for unemployment benefits or (ii) experienced a reduction in income, incurred
significant costs, or experienced other financial hardship due directly or indirectly to COVID-19 that
threaten the household’s ability to pay the costs of the rental property when due.
Application Date WERA Agency Person ID
Applicant First and Last Name
Applicant Phone Applicant Email
Income Type impacted by COVID-19
Please check why income was impacted by COVID-19:
Business Closed Seasonal Job Hours Cut Furlough Laid Off Schools Closed
Other (Please explain):
Please acknowledge by checking the box, that you have been unable to pay rent/utilities and are at risk of
loosing your housing or facing eviction due to COVID related events.
Please acknowledge by checking the box, that you have been not receiving other federally funded
emergency rental assistance.
I hereby certify that the information given is complete and accurate to the best of my knowledge. I
understand that I may be required to present records and documents to support the information
provided. I understand that inaccurate or incomplete information reported could cause my
rental/utility assistance benefit(s) to change. By typing my name in the ‘Applicant Signature’ field, I
indicate that I am the person named, and this entry is the legal equivalent of a manual/handwritten
signature. I further understand that I may print out the document and sign by hand.
Applicant Signature Date Signed
Return Completed Form to:
West CAP
PO Box 308
Glenwood City, WI 54013
Created 2/2021STATE OF WISCONSIN WISCONSIN EMERGENCY RENTAL ASSISTANCE
DEPARTMENT OF ADMINISTRATION P.O. BOX 7970
DIVISION OF ENERGY, HOUSING AND COMMUNITY RESOURCES MADISON, WI 53707-7970
HEAT@WISCONSIN.GOV
Vendor Landlord Agreement (VLA)
Vendor Landlord Agreement (VLA) – one signed form is required per landlord or property management
company. Do not complete multiple forms. A separate form is not required for each tenant and may
delay the processing of the rental assistance. This form should be submitted directly to the local agency
and not sent to the tenant.
NOTE: VLAs previously submitted for the Wisconsin Rental Assistance Program (WRAP) are considered
valid for the Wisconsin Emergency Rental Assistance (WERA) program. A new VLA should not be
submitted.
Vendor/Landlord Name – Provide the name that the payment should be issued to. If there is a property
management company accepting payment for multiple owners, list the property management company
– property/owner name. Example: Wisconsin Property is a management property for Odana Hills and
Lockwood Estates. If it is necessary to identify payments to different properties (and there are separate
TINs for each), two separate VLAs are required. One for Wisconsin Property – Odana Hills and one for
Wisconsin Property – Lockwood Estates. Note that the payment will be issued in the name provided in
this field. The information provided in this field must match the information provided on the Renter
Verification form to ensure that the correct property management/landlord is selected for payment.
Primary Contact – Person who can answer general questions including tenant verification information
Payment Contact – Payment is mailed to the attention of this person. For property management
companies that need checks made out to the owner yet sent to the property management company, the
Payment Contact must be the Property Management Company Name instead of an individual to ensure
delivery by the post office. Example: Vendor/Landlord Name is completed as John Smith (this is to whom
the check is issued). The Payment Contact should be listed as Wisconsin Property Management with
their address listed. It is not necessary to provide an individual’s name in this scenario.
NOTE: Electric Fund Transfer (ETF) payments and other direct deposits to banks are not
available. Payments are mailed by check to the payment address provided on the VLA.
Payment Contact Address – Address where payment is mailed
Taxpayer Identification Number (TIN) – The TIN and TIN type is required. Processing the VLA and rental
assistance request will be delayed and ultimately denied if TIN info is not provided. There should only be
one VLA per TIN. If multiple VLA’s are received for the same TIN, processing of the VLA may be delayed
until the landlord information is verified.
Counties/Tribes – Identify all counties/tribes where all rental property is located. Territories should be
identified for all rental properties owned. Counties/Tribes table can be updated without completing a
new VLA.
Landlord statement: Must be initialed by the landlord to indicate payment will be applied to tenants’
rent and cannot be evicted for non-payment of rent for the period that rental assistance is covering.
Vendor/Landlord Signature: Must be signed by an individual. Company name for the signature is not
acceptable.
Page 1 of 2STATE OF WISCONSIN WISCONSIN EMERGENCY RENTAL ASSISTANCE
DEPARTMENT OF ADMINISTRATION P.O. BOX 7970
DIVISION OF ENERGY, HOUSING AND COMMUNITY RESOURCES MADISON, WI 53707-7970
HEAT@WISCONSIN.GOV
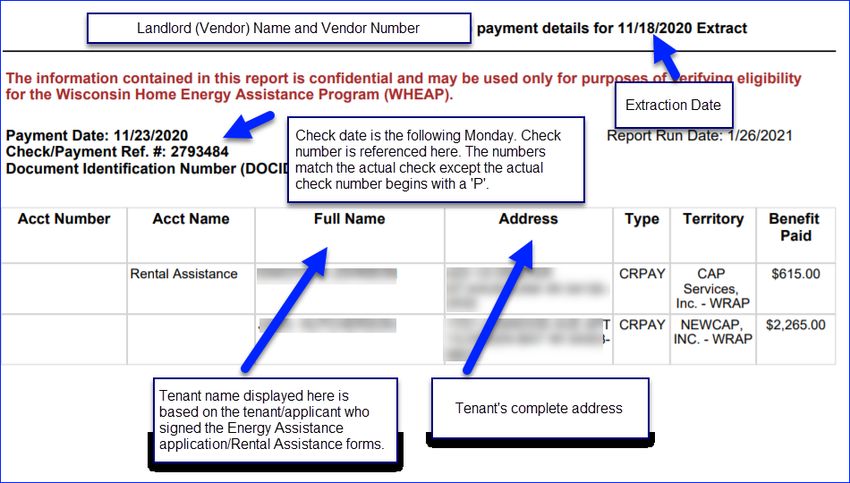
Payment Process
• Rental Assistance applications are processed every Wednesday night with payments issued the
following Monday. This payment process is called an ‘extraction’. Summary payments are made
each week and may include payment for multiple tenants.
• Payment notices are mailed the next day following the extraction (Thursdays) and should arrive
prior to receipt of the check. Information provided on the payment notice must be matched up
to the associated check to ensure payment is applied to the correct tenant(s). Persons opening
mail should be made aware of this and direct these notices to the proper person.
• Payment notices include a summary of the payment issued and includes the tenant name and
address. Note that summary payments list each tenant and the amount of assistance that was
issued for that tenant/address. See sample below of Payment Details:
Inquiries
For questions regarding how to complete the VLA, contact the Division of Energy, Housing and
Community Resources (DEHCR) Help Desk via heat@wisconsin.gov or (608) 267-3680. If contacting
DEHCR via phone, follow the prompts and select ‘Vendor’.
For questions regarding checks already issued, contact(DEHCR) Help Desk via heat@wisconsin.gov or
(608) 267-3680.
For Questions regarding the Renter Verification Form and/or tenant status of WERA request, contact the
local rental assistance agency that provided the Renter Verification Form. Tenants should contact the
local agency where they applied for Rental Assistance.
Page 2 of 2STATE OF WISCONSIN WISCONSIN EMERGENCY RENTAL ASSISTANCE PROGRAM
DEPARTMENT OF ADMINISTRATION P. O. BOX 7970
DIVISION OF ENERGY, HOUSING AND COMMUNITY RESOURCES MADISON, WI 53707-7970
HEAT@WISCONSIN.GOV
Return Completed Form to: Vendor/Landlord Number
West CAP (Department Use Only)
P O Box 308 Vendor/Landlord Agreement
Glenwood City, WI 54013 Wisconsin Emergency Rental Assistance (WERA) Program
Vendor/Landlord Name (payment is issued in this name)
Primary Contact Primary Contact Phone Customer Service Phone*
Primary Fax Primary Contact E-mail
Primary Contact Address City State Zip
Payment/Check Contact Payment/Check Contact Phone
Payment/Check Fax Payment/Check Contact E-mail
Payment/Check Contact Address City State Zip
*Appears on WERA customer notices
Legal Name
Taxpayer Identification Number (TIN) ________________________________ Identify the TIN type below
Employer ID Number (FEIN) Individual Taxpayer Identification Number (ITIN) Social Security Number (SSN)
Type of Entity:
Individual/Sole Proprietor Corporation Limited Liability Company Government Entity
Counties/Tribes with rental property (Please check all that apply for all rental properties for this landlord)
1-Adams 2-Ashland 3-Barron 4-Bayfield 5-Brown
6-Buffalo 7-Burnett 8-Calumet 9-Chippewa 10-Clark
11-Columbia 12-Crawford 13-Dane 14-Dodge 15-Door
16-Douglas 17-Dunn 18-Eau Claire 19-Florence 20-Fond du Lac
21-Forest 22-Grant 23-Green 24-Green Lake 25-Iowa
26-Iron 27-Jackson 28-Jefferson 29-Juneau 30-Kenosha
31-Kewaunee 32-La Crosse 33-Lafayette 34-Langlade 35-Lincoln
36-Manitowoc 37-Marathon 38-Marinette 39-Marquette 40-Milwaukee
41-Monroe 42-Oconto 43-Oneida 44-Outagamie 45-Ozaukee
46-Pepin 47-Pierce 48-Polk 49-Portage 50-Price
51-Racine 52-Richland 53-Rock 54-Rusk 55-St. Croix
56-Sauk 57-Sawyer 58-Shawano 59-Sheboygan 60-Taylor
61-Trempealeau 62-Vernon 63-Vilas 64-Walworth 65-Washburn
66-Washington 67-Waukesha 68-Waupaca 69-Waushara 70-Winnebago
71-Wood 72-Menominee 85- Red Cliff Tribe 86-Stockbridge-Munsee Tribe
88-Lac du 89-Bad River 91-Mole Lake/ 92-Oneida Tribe 94 - Lac Courte Oreilles Tribe
Flambeau Tribe Tribe Sokaogon Tribe
The landlord may not evict for non-payment of rent during the period of time they are receiving Wisconsin Rental Assistance payments. This may be enforced
by the State, the Community Action Agency, or the tenant as a third-party beneficiary. Please initial the statement and provide signature below. By typing
my name in the ‘Agency/Landlord Agency Signature’ field, I indicate that I am the person named, and this entry is the legal equivalent of a
manual/handwritten signature. I further understand that I may print out the document and sign by hand.
I verify that I will apply the WERA payment to the tenant’s rent.
Vendor/Landlord Signature Date (mm/dd/ccyy)
Send back to West CAP:
mail PO Box 308, Glenwood City, WI 54013, email westcap@wcap.org, or Fax 715-265-4271, att Core ServicesWisconsin Rental Assistance Program (WERA)
Request for Assistance / Renter’s Verification
This document provides a way for the landlord/rental agent to verify the terms of tenancy of the applicant. This
document can be used in the place of providing a written lease I but does not replace a written lease between the
tenant and landlord. If this form is utilized, it must be completed and signed by the landlord/rental agent.
Applicant Name
Unit Address
City, State, Zip
Phone Email
Total Assistance $ Description of
Requested Assistance Requested
Tenancy Information:
Property Owner
Manager/Rental Agent
Address
City, State, Zip
Phone Fax
Email
Rental Agreement Information:
Rent Amount $
Rent Due ☐ weekly ☐ monthly ☐ other (Click or tap here to enter text.)
Total Past Due Rent $
☐ one year (term: Click or tap here to enter text.)
☐ months (term: Click or tap here to enter text.)
Type of tenancy
☐ month-to-month (start date: Click or tap here to enter text.)
☐ week-to-week (start date: Click or tap here to enter text.)
Payment method for Heat Electric
heat and electric ☐ Included in the rent ☐ Included in the rent
☐ Separate Payment is made to the ☐ Separate Payment is made to the
Landlord Landlord
☐ Tenant pays directly to utility vendor ☐ Tenant pays directly to utility vendor
By typing my name in the ‘Agency/Landlord Agency Signature’ field, I indicate that I am the person named, and this entry is the legal
equivalent of a manual/handwritten signature. I further understand that I may print out the document and sign by hand.
Signature of owner, landlord or rental agent Date
Signature of applicant Date
Rev: 03/31/2021 Page 1 of 2Send to: West CAP, westcap@wcap.org or PO box 308, Glenwood City, WI 54013
Emergency Rental Assistance: Completed by WERA Staff Only:
Rent Assistance Arrears $
Rental Assistance Needed $
Lot Assistance Arrears $
Lot Assistance Needed $
Security Deposit $
Description of Assistance Please list the total amount of arrearages and late fees due for each month below.
Requested Please list rent amount and any fees separately.
For example: August 2020 - $550 Late Fees: $50
Total Past Due Rent $
(including fees)
Rev: 03/31/2021 Page 2 of 2You can also read