Using available evidence to inform a prioritized and patient-centred National Strategic Plan - Maureen Kamene
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Using available evidence to inform a
prioritized and patient-centred
National Strategic Plan
Maureen Kamene
NSP 2015-2018
Evidence-based plan Strategic Priorities
Evidence was
epidemiological
and related to
1. Identify and treat all cases Everything was
1. Core DOTS equally “prioritized”
programmatic
performance 2. MDR-TB
3. Pediatric TB
4. Leprosy
2. Engage all care providers
3. Promote and strengthen community engagement
4. Enhance the multi-sectoral response to TB/HIV
5. Accelerate appropriate diagnosis
6. Ensure stable & quality supply of all commodities
7. Enhance evidence-based programme monitoring
& evaluation
8. Create an enabling, multi-sectoral environment
9. Support devolution
NSP Development Process
NSP 2015 – 2018
Global Fund
We thought we knew the epi.
We planned using it. application
1. Identify and treat all cases
1. Core DOTS
2. MDR-TB What’s New?
3. Pediatric TB
4. Leprosy Prevalence survey
• more TB than previously
2. Engage all care providers
estimated
3. Promote and strengthen community • non-specific symptoms &
engagement asymptomatic TB
4. Enhance the multi-sectoral response to
TB/HIV
5. Accelerate appropriate diagnosis Patient pathway analysis
6. Ensure stable & quality supply of all • people with TB in the health
commodities system, undiagnosed
7. Enhance evidence-based programme
monitoring & evaluation Etc.
8. Create an enabling, multi-sectoral
environment
9. Support devolution
NSP Development Process
NSP 2015 – 2018 NSP 2018 - 2023
We thought we knew the epi. We know more about the epi.
We planned using it. Now we know about patient behavior. We
can plan to local patient needs.
1. Identify and treat all cases
1. Core DOTS
2. MDR-TB 3 ways this NSP can be ground-breaking:
What’s New?
3. Pediatric TB
4. Leprosy Prevalence survey 1. Use consolidated national data to incorporate
• more TB than previously a robust evidence base to establish priorities
2. Engage all care providers
estimated for action
3. Promote and strengthen community
Patient pathway analysis
engagement • people with TB in the health
4. Enhance the multi-sectoral response to 2. Use sub-national data to build a plan that
system, undiagnosed
TB/HIV responds to county-specific needs and
5. Accelerate appropriate diagnosis Adherence study successes
6. Ensure stable & quality supply of all
commodities Inventory study 3. Use impact evaluations and modeling to
• Many patients on care, not optimize the effectiveness of packages of
7. Enhance evidence-based programme notified
monitoring & evaluation interventions
8. Create an enabling, multi-sectoral Epi review
environment enabling a prioritized / tiered plan
9. Support devolution
4
Framework for prioritization and planning
Reviewing the evidence about the biggest epidemiological challenges and the biggest challenges on a patient’s
pathway to care can help to identify which sets of problems should be priorities for the national TB program
Pre-work Day 1 Day 2 Day 3
1. Problem 2. Root Cause 3. Intervention
People are in Prioritization Analysis Identification
the health
system, but
not notified/
People don’t diagnosed
make it to the
What What are
health system What was
Which contributes to priority Implement
the impact of
are the biggest the problem? solutions to the best
People with these
problems? What does it optimize solutions
TB are look like? solutions?
impact?
notified, but
not cured
5
Framework for prioritization and planning
Reviewing the evidence about the biggest epidemiological challenges and the biggest challenges on a patient’s
pathway to care can help to identify which sets of problems should be priorities for the national TB program
Pre-work
1. Problem 2. Root Cause 3. Intervention
People are in Prioritization Analysis Identification
the health
system, but
not notified/
People don’t diagnosed
make it to the
What What are
health system What was
Which contributes to priority Implement
the impact of
are the biggest the problem? solutions to the best
People with these
problems? What does it optimize solutions
TB are look like? solutions?
impact?
notified, but
not cured
6
National data and evidence compiled (1/2)
Resource Title Year Problem Root Cause Analysis Solution
Prioritization Optimization
Surveillance, Surveys and Studies
TB Surveillance Data (TIBU) All X X
TB Prevalence Survey 2015/2016^ 2016 X X
Adherence survey 2017^ 2017 X
TB Patient cost survey 2017^ 2017 X
Inventory study 2014/2015^ 2016 X X
Drug resistant survey 2014/2015 2015 X
Delay in Diagnosis 2013/2014* 2014 X
Kenya Demographic and Health survey (KDHS) 2013^ 2013 X X
KAIS 2012* 2012 X X
GXpert Impact survey 2017* 2017 X X
Community survey 2017* 2017 X
Keheala study to improve Treatment Adherence* 2017 X X
SARAM Survey 2013 2013 X X X
Health Expenditure Utilization Survey 2016 2016 X X
Analyses
Patient Pathway analysis 2017^ 2017 X X
Legal environmental assessment by KELIN 2017* 2017 X X
Data for action for Key, Vulnerable and underserved population X X
2018
by Kelin 2017/2018*
Gender barriers to TB by KELIN 2017* 2018 X
TB/DM by AMPATH* 2017 X 7
NATIONAL DATA AND EVIDENCE COMPILED (2/2)
Resource Title Year Problem Prioritization Root Cause Analysis Solution Optimization
Reviews/Reports
WHO Global TB Report 2017^ 2017 X
GF concept note 2017 X
NTLDP Annual report 2017 2018 X
Mid term review 2017 2017 X X
Epi Review 2017^ 2017 X X
ACF Experience sharing report 2017 2017 X X
GLC AFRO Mission Kenya Report 2017 2017 X
Policy Documents
Kenya Health Sector Strategic and Investment Plan 2013-2017 2013 X
END TB Strategy 2015 X
Isolation policy 2018 X
Social protection policy 2018 X
Sustainability framework 2017 X
Investment case 2017 X
NSP 2015-2018 2015 X
8
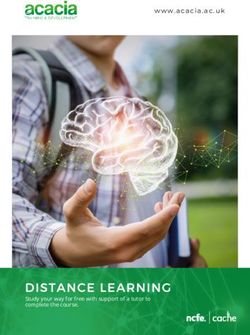
DATA AND EVIDENCE MAPPED TO THE CARE CONTINUUM
Epi
Priority setting requires : Know your epidemiology, know your patient, know your system
Patient People don’t make it to the health system
People with TB in the health system, but not People with TB are notified,
notified/diagnosed but not cured
People with Total
Asymptomatic Symptomatic Presenting to Diagnosed by Diagnosed by
TB infection, Notified, not Durable cure
disease, not disease, not health facilities, non-NTP, not NTP, not
high-risk for durable cure (relapse free)
seeking care seeking care not diagnosed notified notified
disease
5 6 DS-TB 1 2
DR-TB 3 4
TB/HIV
Epi
Total
# Important metrics from available evidence resources (see following slides)
9
EXAMPLE: EVIDENCE INPUT INTO THE CARE CONTINUUM (1/2)
2016 Prevalence Survey
5
Asymptomatic disease, not seeking
care
Screening for TB using any or all of the
four cardinal symptoms - cough of
more than two weeks, fever, night sweats
and weight loss - would have
missed 40% of the TB cases
6
Symptomatic disease, not seeking
5 care
Majority of people found to have TB had
not sought health care for their symptoms
6 prior to the survey
– Majority did not seek health care
because they did not perceive their
symptoms as
being serious
10EXAMPLE: EVIDENCE INPUT INTO THE CARE CONTINUUM (1/2)
2017 Patient Pathway Analysis
1 3
Presenting to health facilities, not
diagnosed
43% of people with TB are likely to visit a
health facility with capacity for TB
diagnosis on their first visit to the health
care system. Even fewer are likely to
2 receive a DR diagnosis on their first visit.
4
2 4
Diagnosed by non-NTP, not notified
Over 40% of people initiate their care
seeking journey in private (formal or
informal) facilities. Diagnostic capacity
exists in the private sector, however only
notifications from the private sector only
account for 13% of the estimated burden.
1
3
11Evidence Review Sessions
Patient People with TB in the health system, but not
People Who aren’t in the health system People with TB are notified, but not cured
notified/diagnosed
High-risk for TB
Asymptomatic Symptomatic Session 1 Presenting to Diagnosed by Diagnosed by People with TB On treatment Complete Tx,
infection, or
disease, not disease, not Burden of health facilities, private sector, not public sector, not notified to the without w/out durable,
breakdown to
seeking care seeking care Disease not diagnosed notified notified NTP treatment success relapse-free cure
disease
DS-TB*
Session 3 – Evidence related to people
Session 2 – Evidence related to people Session 4 – Evidence related to people
not in the health system
DR-TB in the health system not being
who are notified, but not cured
diagnosed/notified
TB/HIV
Epi
1
2WORKING GROUPS ACCESSED DATA / EVIDENCE SUMMARY SHEETS
Session 3 – People Session 4 – people
Session 1 – Burden Session 2 – People
in system, not notified, but not
of Disease not in health system
notified/dx cured
# 2016 Prevalence Survey # 2017 WHO TB Report # 2014 DHS # 2016 Inventory Study
# 2017 Patient Pathway Analysis # 2017 Epi Review # 2013 HEUS 13Session 1: Data
TEAMS DEALT WITH DISCORDANT DATA
1
EXAMPLE: 2016 PREVALENCE SURVEY [TB/HIV]
• Among prevalent TB patients in the
prevalence survey, 13.4% were recorded in
TIBU as HIV(+), while 23% of these patients
self-reported as HIV(+)
1
1
14Session 1: Data
2017 WHO GLOBAL TB REPORT [TB/HIV]
• According to the WHO report, 96%
10
of patients have known HIV status,
and 31% of patients with known HIV
10 status are HIV-positive;
10
15WORKING GROUP: DISCUSSION PROMPTS
Review available data and establish a level of
priority based on the evidence Comment on the quality of data
1. How big of a problem is this, within the context of the
overall TB burden? Either
(rank between 1-5; 1=not a big problem, low priority; 5= top priority) Sufficient to establish a level of priority
2. To what extent is there progress against this challenge Or
(1=no progress; 5 = solid progress, commensurate with problem)
Additional data are available and need to
be included
3. What level of priority should be given to filling the
remaining gaps related to this challenge? Or
(1=not a big problem, low priority; 5= top priority)
Data gaps - - Define
© 2017 Bill & Melinda Gates Foundation | 16Working group priority scores were consolidated
17Inventory of Evidence Gaps was compiled
Priorities based on available data
But….
Insufficient data in some instances
So….
Reconsider based on available evidence from newly
identified sources
or
Add to research agendaFRAMEWORK FOR PRIORITIZATION AND PLANNING
Step-wise approach to strategic planning that focuses on where people with TB may be “missing” from care
1. Problem 2. Root Cause 3. Intervention
People are in Prioritization Analysis Optimization
the health
system, but
not notified/
People don’t diagnosed
make it to the What are
What What was
health system Which priority Implement
contributes to the impact of
are the biggest the problem? solutions to the best
People with these
problems? What does it optimize solutions
TB are look like? solutions?
impact?
notified, but
not cured
19Participants were introduced to Root Cause analysis
Understanding the layers and determinants that contribute to priority challenges
Known priority problem
Determinants
Root cause
1. What is known about the factors
contributing to this problem?
2. What additional evidence is needed to
better understand the root cause of this
Interventions to address
problem?
determinants
3. Which can feasibly be addressed?
2
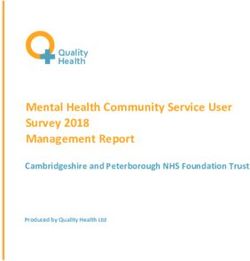
0ROOT CAUSE ANALYSIS
Additional data were made available to assist working groups to think about determinants and root causes
Patient People Who aren’t in the health system
People with TB in the health system, but
People with TB are notified, but not cured
not notified/diagnosed
High-risk for Presenting to On treatment Complete Tx,
Asymptomatic Symptomatic Diagnosed by Diagnosed by People with TB
TB infection, health without w/out durable,
disease, not disease, not private sector, public sector, notified to the
or breakdown facilities, not treatment relapse-free
seeking care seeking care not notified not notified NTP
to disease diagnosed success cure
1 1 1 2 4 1 1 1 5
DS-TB
2 3 5 2
1 2 2 6
2 3 3 7
DR-TB
4 4 8
TB/HIV
Epi
# 2016 Prevalence Survey # 2017 WHO TB Report # 2014 DHS # 2016 Inventory Study # 2017 Patient Cost Survey
# 2017 Patient Pathway Analysis # 2017 Epi Review # 2013 HEUS # 2017 Adherence Study 21EXAMPLE: 2017 ADHERENCE STUDY
•1 There was a statistically increased risk of non-
adherence in the groups 25-34, 35-44 and 55-64
years compared to age group 18-14 years (pROOT CAUSE ANALYSIS
Small working groups can map what is known / what evidence is still needed to inform evidence-based action
- What is known about the factors contributing to this problem?
- What additional evidence is needed to better understand the root cause of this problem?
- Of the possible root causes, which would be the most impactful to address? Which can feasibly be addressed?
People with TB in the health system, but
Group 6: People Who aren’t in the health system People with TB are notified, but not cured
not notified/diagnosed
Patient
DR-TB
High-risk for Presenting to On treatment Complete Tx,
Asymptomatic Symptomatic Diagnosed by Diagnosed by People with TB
TB infection, health without w/out durable,
disease, not disease, not private sector, public sector, notified to the
Group 7: TB or breakdown seeking care seeking care facilities, not
not notified not notified NTP
treatment relapse-free
in children to disease diagnosed success cure
Group 8: Group 4 –
Key M&E,
populations
Group 2 – Group 3 – including
Group 5 – Ensuring cure, including
Group 1 – Pre-care seeking, diagnostic Private initial
Group 9: treatment support and social protection
including community engagement gap and sector and default
TB/HIV PAL (lab) and
Epi
not notified
Group 10:
Leprosy
23Lack of knowledge of TB among HCWs
No or Inadequate training
Lack of pre-service Lack of OJT Focus only on TB
training on TB Rx sites – 40%
- Outdated Curriculum - Lack of need assessment for training - Supervision based on case notification
- Lack of engagement by by counties - Lack of policy on pre-Dx cascade
NTP - Lack of advocacy to donors & counties - Lack of M&E tools
- Lack of multi-sectoral - Lack of measurement of training - Lack of evidence on importance of pre-
approach impact Dx prior to prevalence survey
Patients visit
the HF, not
screened for TB
- Inadequate quantification to - Inability to plan around long
allow accurate forecasting - Lack of mechanisms
procurement cycles
- Forecasting based on at county level for
- Multiple donors/partners with
notification data not distribution of tools
different cycles/roles
presumptive
Stationary Distribution of tools Long TAT
printing not not prioritized by for printing
done in time counties tools
Tools for specimen collection not availableFRAMEWORK FOR PRIORITIZATION AND PLANNING
Step-wise approach to strategic planning that focuses on where people with TB may be “missing” from care
1. Problem 2. Root Cause 3. Intervention
People are in Prioritization Analysis Optimization
the health
system, but
not notified/
People don’t diagnosed
make it to the What are
What What was
health system Which priority Implement
contributes to the impact of
are the biggest the problem? solutions to the best
People with these
problems? What does it optimize solutions
TB are look like? solutions?
impact?
notified, but
not cured
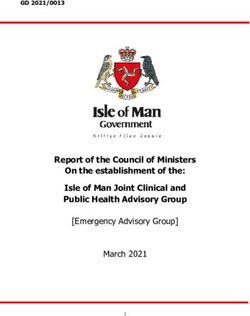
26Group: Not complete treatment (Treatment, UHC and social support)
Action Domain: Nutrition support
Objectives:
• Improve treatment outcome of patients with malnutrition (% death, % LTFU)
✓ All HCWs managing TB patients are competent in assessing and managing malnourished TB patients
✓ All TB patients are assessed for nutritional status (100%)
✓ All TB patients are provided with nutrition support according to their needs (100% for SAM, …)
High Feasibility
1. Universal nutritional assessment 3. Boldly address supply chain
and counselling management issues of nutritional 1
• ~18% patient not evaluated commodities up to beneficiary 4 3
• Systematic nutrition assessment at the • Align supply of TB drugs to nutritional 2
start of treatment, follow up and at the commodities
end of treatment • (Being the biggest constraint for the
Low
• System to alert if no improvement intervention 2) Impact
High
Impact
2. Universal nutrition management 4. Impact evaluation of nutrition
for all eligible patients interventions
• ~20% SAM; ~30% MAM • Compilation of existing evidence
• Micronutrient supplementation • Establish a robust impact Others-
• Therapeutic feeding for SAM • Multi-sector collaboration
evaluation framework • Case detection in other in-country
• Supplemental feeds for MAM nutritional interventions eg school,
community, LowMUAC screening
FeasibilityKey Results
1. Results along the care continuum can be used as the
context for understanding new data / evidence
2. Priorities established based on evidence, rather than
politics or emotions
3. Interventions identified that target the most important
determinants / root causes of remaining challenges
4. Priority data/evidence gaps documented; filling these
gaps will direct impact the ability of the programme to
make informed decisions
2
8Current thinking: NSP framework 2019-2023
3. Inclusion of TB,
Strategic 1. Close the gaps along 2. Differentiated 4. Prevent infection, 5. Patient centered
Leprosy and Lung
objectives for TB, the care continuum to response by county active disease, approach that
Disease within
Leprosy and Lung find and cure the to address TB in the morbidity and promotes quality of
National UHC
Disease missing cases local context mortality care
framework
29Next steps
1. Problem 2. Root Cause 3.
People are
in the Prioritization Analysis Intervention
health Identification
People system, but
don’t make not notified/
it to the diagnosed What are
health Which What What was
contributes to priority Implement
are the the impact
system
People with biggest
the problem? solutions to the best
of these
Preliminary national-level priorities
What does it optimize solutions
TB are problems? look like? solutions?
notified, but impact?
not cured
1. Refine at national level using additional available
evidence
2. Repeat with counties to identify sub-national priorities
3. Conduct patient and health worker focus groups
4. Triangulate for evidence-based NSP
3
0National Tuberculosis, Leprosy and Lung Disease Program
Email: mkamene@nltp.co.ke
nltp.co.ke @NTLDKenya NTLDKenya
Asante (Thank You)!You can also read