Update on COVID-19 Projections - Science Advisory and Modelling Consensus Tables March 17, 2022
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Update on COVID-19 Projections
Science Advisory and Modelling Consensus Tables
March 17, 2022
Key findings • COVID-19 case numbers, hospital and ICU occupancy have stopped declining; there is considerable regional variation. • Given the relaxation of public health measures and consequent increase in transmission, hospital and ICU occupancy will likely increase over the next few weeks, but less than in January 2022 and for a limited period of time if changes in behaviour are only moderate. • The extent of this increase, and of a person’s risk of contracting COVID-19, will depend on the number of close contacts (especially indoors without masking), vaccination status, and the spread of the more transmissible BA.2 subvariant. • Older adults, immunocompromised, unvaccinated and marginalized individuals and groups are still susceptible to severe illness from COVID-19. • A complete vaccine series (currently two doses in children, three doses in adults, four in long-term care residents and other eligible high-risk groups) is the best defence against getting and spreading COVID-19. 2

Ontario’s COVID-19 wastewater signal stopped declining
and is now increasing slightly
• Based on 101 wastewater treatment Province-Wide COVID-19 Wastewater Signal
plants, pumping stations and 2.0
Incomplete Data, Provisional Estimates*
Standardized Concentration of SARS-CoV-2 Gene Copies
sewersheds in all 34 public health Complete Data
units
• Plausible range of SARS-CoV-2 1.5
infections since Dec 1, 2021, based on
wastewater: 3 to 4.5 million
• Current daily number of infections 1.0
estimated based on daily case growth
from wastewater curve: 15,000 to
20,000 0.5
• Until mid Dec 2021, an estimated 30
to 45% of infections were reported;
after change of testing strategy end of 0.0
Dec 2021, an estimated 10% of
2
2
1
1
1
21
21
22
2
2
2
2
2
22
22
22
22
22
-2
-2
-2
-2
-2
-2
-2
-2
-2
-2
n-
c-
c-
b-
b-
n-
n-
n-
ar
ar
ec
ec
ec
ar
ar
ar
eb
eb
De
De
Ja
infections are reported
- Ja
- Ja
- Ja
Fe
Fe
M
M
-M
-M
-M
-D
-D
-D
-F
-F
5-
1-
8-
2-
9-
2-
9-
12
19
26
15
22
29
16
23
16
23
30
Sampling Date
Data: Wastewater Dashboard hosted by Ontario’s Ministry of the Environment, Conservation and Parks (MECP) 3
Analysis: Secretariat of the Science Advisory Table (https://covid19-sciencetable.ca/ontario-dashboard/) – see dashboard for explanations of the methods
The wastewater signal shows considerable variation across
regions
Data: Wastewater Dashboard hosted by Ontario’s Ministry of the Environment, Conservation and Parks (MECP) 4
Analysis: Secretariat of the Science Advisory Table (https://covid19-sciencetable.ca/ontario-dashboard/) – see dashboard for explanations of the methods
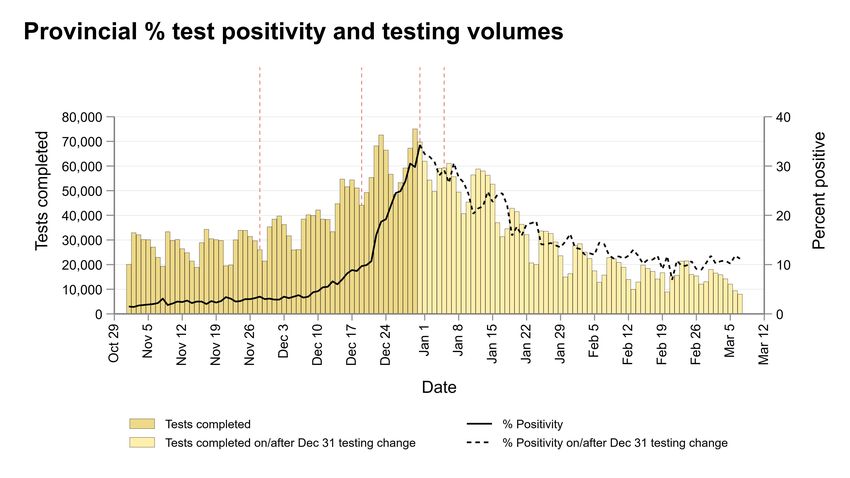
Provincial test positivity has stopped declining
Nov. 28 Dec. 19 Dec. 31 Jan. 5 Feb. 17
First Ontario New public Changes to Additional public Public health
Omicron case health PCR testing health measures measures lifted for
reported restrictions criteria and shift to online all but large venues
implemented school
5
Data source: Public Health Ontario. PDNOC lab reporting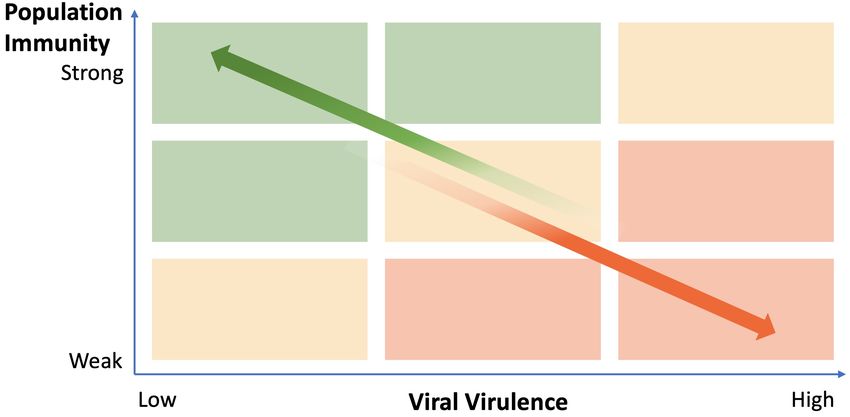
Test positivity in selected populations is stable or increasing
slightly
Workplace screening People requiring frequent testing Hospital Admission Screening
Workplace rapid screening program across Individuals with 40+ tests since pandemic start, Selected Ontario hospitals, 4 for adult
Canada, twice per week, Ontario data shown 20-79 years of age, excluding LTC residents admissions, 5 for pediatric admissions
3.0% 30%
Fraction of presumptive positive on total screens (%)
14%
2.5% 25%
12%
Percent Positive (%)
2.0% 10% 20%
Percent Positive (%)
8%
1.5% 15%
6%
1.0% 10%
4%
0.5% 5%
2%
0.0% 0% 0%
15 Dec 21
30 Dec 21
14 Jan 22
29 Jan 22
15 Dec 21
30 Dec 21
1 Jan 22
14 Jan 22
29 Jan 22
16 Jan 22
31 Jan 22
13 Feb 22
28 Feb 22
2 Mar 22
13 Feb 22
28 Feb 22
15 Feb 22
20-39 years 40-59 years 60-79 years All Adult Adm Labour&Deliver y Adm All Pediatr ic Adm
6
Data/Analysis: Creative Destruction Lab-Rapid Screening Consortium (Workplace screening). MCT using OLIS data (repeat testers), Hospital IPAC Teams and Data Analytics (hospital admission screening)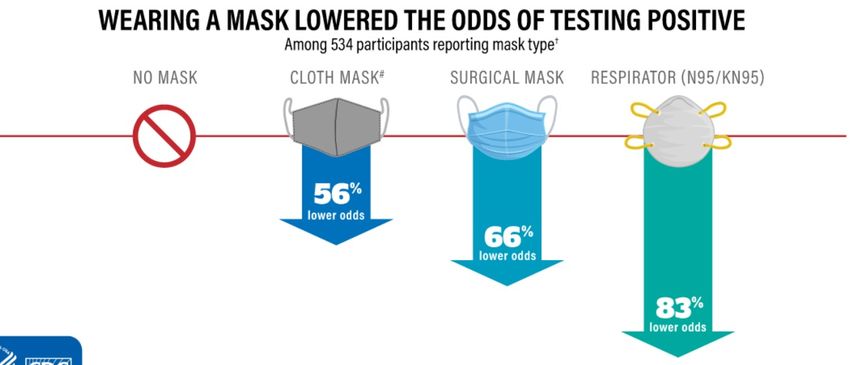
Lower income neighbourhoods continue to be hit hardest by
the pandemic, also during the fifth wave caused by Omicron
Cumulative COVID-19 Deaths per 100,000 Population per Wave
30
Cumulative COVID-19 Deaths per 100,000 Population
25
20
15
10
5
0
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5
Lowest Income Highest Income
Ontario’s population was divided into 5 equally sized groups (quintiles) according to household income measured at neighbourhood level. Analysis excludes residents
of long-term care homes. Wave 1: Feb 26 – Aug 31, 2020; Wave 2: Sep 1, 2020 - Feb 28, 2021; Wave 3: Mar 1 – Jul 31, 2021; Wave 4: Aug 1 – Dec 14, 2021; Wave 5:
Dec 15, 2021 – present. 7
Analysis: COVID-19 Heterogeneity Research GroupMobility, which is correlated with contacts, continues to increase,
but retail & recreation are still below summer 2021 levels
Data: https://covid19.apple.com/mobility/ and https://www.google.com/covid19/mobility/ 8
Analysis: Secretariat of the Science Advisory Table (https://covid19-sciencetable.ca/ontario-dashboard/)We expect hospital occupancy to increase when public
health measures are lifted and behaviours change
Figure shows projections based on models from Example scenarios
two scientific teams. Moderate increase in transmission*
• Different models use different approaches No increase in transmission
and assumptions. 3000
• Models are calibrated to different data
Hospital occupancy (ward only)
including case counts, hospital occupancy,
and ICU occupancy.
• Models assume 7M to 8M Ontarians will have
received booster dose by end of March. 2000
• Scenarios differ by levels of immunity and
changes in contacts and behaviour.
• COVID-19 transmission, which drives hospital
occupancy, can be reduced by wearing high-
quality masks, full vaccination and not 1000
increasing contacts.
Range of
• There remains uncertainty on current scenarios considered
community levels of immunity, future changes
in behaviour, and future spread of the more
transmissible BA.2 subvariant. 0
Jan 2022 Feb 2022 Mar 2022 Apr 2022 May 2022
*Examples of scenarios that could result in a moderate increase in transmission include an approximate increase in contacts of 40%, with half of
contacts maskless, or an approximate 30% increase in contacts if BA.2 becomes dominant, with half of contacts maskless.
Projections informed by modelling from McMasterU, WesternU 9
Data (hospitalisations): covid-19.ontario.caWe expect ICU occupancy to increase when public health
measures are lifted and behaviours change
Figure shows projections based on model from Example scenarios
two scientific teams. 600
Moderate increase in transmission*
• Models are calibrated to different data
No increase in transmission
including case counts, hospital occupancy,
and ICU occupancy.
• Models assume 7M to 8M Ontarians will have
received booster dose by end of March.
• Range of scenarios shown correspond to
ICU occupancy
400
scenarios in previous slide on hospital
occupancy.
• COVID-19 transmission, which drives ICU
occupancy, can be reduced by wearing high-
quality masks, full vaccination and not
increasing contacts. Range of
• There remains uncertainty on current 200
scenarios considered
community levels of immunity, future changes
in behaviour, and future spread of the more
transmissible BA.2 subvariant.
Jan 2022 Feb 2022 Mar 2022 Apr 2022 May 2022
*Examples of scenarios that could result in a moderate increase in transmission include an approximate increase in contacts of 40%, with half of
contacts maskless, or an approximate 30% increase in contacts if BA.2 becomes dominant, with half of contacts maskless.
Projections informed by modelling from McMasterU, WesternU 10
Data (hospitalisations): covid-19.ontario.caVaccine coverage with 3rd doses has plateaued in all age groups
and is lower in marginalized communities
Number of Vaccinated Individuals & Doses Administered Percentage Vaccinated with 3 Doses by Age and Material Deprivation
250,000
100
Daily Number of Vaccine Doses Administered (7-Day Average)
12,000,000 1 Dose 90
Cumulative Number of Vaccinated Individuals
2 Doses
80
Percentage of People witih 3 Doses
200,000
10,000,000 3 Doses
Doses per Day 70
8,000,000
150,000 60
50
6,000,000
100,000 40
4,000,000 30
50,000 20
2,000,000
10
0 0 0
12 to 17 years 18 to 29 years 30 to 59 years 60 to 79 years 80+ years
1
21
1
1
21
1
21
22
1
1
1
2
1
21
1
22
0
02
02
02
02
02
02
02
02
02
02
02
20
20
20
20
20
20
-2
-2
-2
-2
-2
-2
-2
r-2
-2
-2
l-2
b-
c-
b-
n-
n-
n-
ov
ep
ug
pr
ay
ar
ct
ar
ec
- Ju
Ap
De
- Ju
Ja
Ja
Fe
Fe
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5
-O
M
M
-A
-N
-M
-D
-A
-S
7-
6-
22
4-
1-
9-
3-
24
4-
3-
29
16
14
10
19
11
27
Date Highest Material Deprivation Lowest Material Deprivation
Ontario’s population was divided into 5 equally sized groups (quintiles) according to material deprivation measured at
neighbourhood level. Analysis excludes residents of long-term care homes.
Data: https://data.ontario.ca and Public Health Ontario 11
Analysis: Secretariat of the Science Advisory Table (https://covid19-sciencetable.ca/ontario-dashboard/)Modelling suggests that 3rd doses substantially reduced COVID-19
hospitalization and ICU occupancy
COVID-19 hospital occupancy COVID-19 ICU occupancy
6000
1000
5000
34% 800 30%
Hospital Occupancy (ward only)
fewer fewer
4000 people people
at peak at peak
ICU Occupancy
600
3000
400
2000
200
1000
0 0
15 Dec 21
30 Dec 21
14 Jan 22
29 Jan 22
13 Feb 22
28 Feb 22
15 Dec 21
30 Dec 21
14 Jan 22
29 Jan 22
13 Feb 22
28 Feb 22
Observed 7-day Average If no
No 3rd doses had been given
Boosters Observed 7-day Average If no
No 3rd doses had been given
Boosters
The orange and yellow curves show the estimated hospital occupancy (wards only) and ICU occupancy in Ontario that would have occurred if no 3rd doses had been given. The grey curves show the 7-
day average of hospital and ICU occupancy observed in Ontario during the Omicron wave.
12A 3rd COVID-19 vaccine dose offers better protection against
Omicron infection over time than 2 doses
3.00
2 Doses 3 Doses
Mean of protective antibody levels (log10 ID50 )
2.50
2.00
1.50
1.00
0.50
0.00
se
se
se
se
do
do
do
do
nd
rd
rd
nd
r3
r3
r2
r2
fte
te
fte
te
af
af
sa
sa
th
th
th
th
on
on
on
on
M
M
M
M
1
1
6
7
Shown are mean log 10 neutralizing antibody titers against Omicron over time after Moderna COVID-19 mRNA vaccine 13
Adapted from: Pajon et al, N Engl J Med 2022 (https://www.nejm.org/doi/full/10.1056/NEJMc2119912)Future scenarios in Ontario will depend on population immunity,
the virulence and severity of future variants
The severity of COVID-19 High
experienced in a population (risk of
Immunity in the Population
serious outcomes: hospitalization,
ICU admission and death) will
depend on:
1. The immunity of the
population resulting from
vaccination and previous
infection
2. The virulence of the variant
(the likelihood that the variant
will cause serious outcomes)
Low
Low High
Risk of Serious Outcomes Caused by a Future Variant
14
Adapted from: https://www.covidroadmap.org/Masks are still an effective public health measure to reduce
COVID-19 transmission
• Public health measures, including increased ventilation and filtration, physical
distancing and wearing a well-fitted, high-quality mask can help reduce SARS-
CoV-2 transmission in places where people gather indoors.
• Recent studies from the United States analysed the impact of mask-wearing on
SARS-CoV-2 community transmission: mandatory masking reduced the
incidence of SARS-CoV-2 infection consistently.
• Masking protects both the person who wears the mask and others.
• Community benefits from masking
are most pronounced when
adopted widely.
Example of a matched case-control
study in 1,828 people from the United
States, Feb 10-Dec 1, 2021
15
Donovan et al. MMWR Morb Mortal Wkly Rep 2022; Brooks et al. JAMA. 2021; Figure adapted from Andrejko et al. MMWR Morb Mortal Wkly Rep 2022.Ontario built strong pandemic control tools, which can be
used to maintain readiness
Ontarians should:
• Ensure that they have a complete vaccine series (includes three doses in adults, four in eligible,
high-risk groups).
• Use high-quality masks whenever necessary to protect vulnerable people or themselves.
• Stay home when sick or symptomatic.
Ontario should:
• Continue improvement of ventilation and air filtration in public indoor spaces.
• Create rapid paths to testing and treatment (e.g., Paxlovid, antibodies) with a focus on equity.
• Be prepared to renew mass COVID-19 vaccination campaigns if needed.
• Be prepared to renew vaccine certificates requiring a recent booster dose for high-risk settings if
needed.
• Be prepared to reintroduce mask mandates if needed.
• Maintain protective measures that are appropriate for the general health and wellbeing of those
living and working in congregate care settings such as long-term care.
16Ontario remains vulnerable as long as the global pandemic
continues
• New variants are more likely to develop if a large number of people who are
immune-compromised do not receive appropriate treatment and vaccination
• 2-3% of global population is immunosuppressed
• Many of the more than 40 million people living with HIV/AIDS are not appropriately treated
• Although 56% of the world population has now received two COVID-19 vaccine
doses, that is still too few to build sufficient immunity globally.
• Broad-acting and intranasal vaccines now under development could play a key role in the
future.
• Global surveillance and public health controls remain insufficient.
• Global wastewater surveillance and genomic sequencing will continue to be essential in
the future.
• Improved ventilation, air filtration and adoption of high-quality masks will continue to be
important worldwide. 17Key findings • COVID-19 case numbers, hospital and ICU occupancy have stopped declining; there is considerable regional variation. • Given the relaxation of public health measures and consequent increase in transmission, hospital and ICU occupancy will likely increase over the next few weeks, but less than in January 2022 and for a limited period of time if changes in behaviour are only moderate. • The extent of this increase, and of a person’s risk of contracting COVID-19, will depend on the number of close contacts (especially indoors without masking), vaccination status, and the spread of the more transmissible BA.2 subvariant. • Older adults, immunocompromised, unvaccinated and marginalized individuals and groups are still susceptible to severe illness from COVID-19. • A complete vaccine series (currently two doses in children, three doses in adults, four in long-term care residents and other eligible high-risk groups) is the best defence against getting and spreading COVID-19. 18
Contributors
• Creative Destruction Lab-Rapid Screening Consortium
• Hospital Infection Prevention And Control (IPAC) Teams and Data Analytics: Suhair AlShanteer, Michelle Barton Forbes, Steven
Bernard, Craig Campbell, Michael Chow, Robert Crawford, Gerald Evans, Jayvee Guerrero, Kevin Katz, Erin Kelleher, Sarah Khan,
Ethel Lagman, Melanie Lavigne, Kirk Leifso, Sheri Levesque, Reena Lovinsky, Tracy Macleod, Jennifer McCallum, Dominik Mertz,
Vydia Nankoosingh, Kasey Parker, Paul Sandor, Michelle Science, Shawna Silver, Celia So, Rachel Solomon, Nisha Thampi, Alon
Vaisman, Elisa Vicencio, Eugene Wong
• ICES: Sarah Buchan, Hannah Chung, Kevin Brown, Peter Austin, Deshayne Fell, Jonathan Gubbay, Sharifa Nasreen, Kevin Schwartz,
Maria Sundaram, Mina Tadrous, Kumanan Wilson, Sarah Wilson, Jeff Kwong
• McMasterU: Irena Papst, Ben Bolker, Jonathan Dushoff, David Earn
• Modelling Consensus Table: Kali Barrett, Isha Berry, Sharmistha Mishra, Ashleigh Tuite, Beate Sander
• Ontario Health: Erik Hellsten, Stephen Petersen, Anna Lambrinos
• Science Advisory Table: Peter Jüni, Nicolas Bodmer, Karen Born, Shujun Yan, Pavlos Bobos
• TAHSN Human Resources Network: Sunnybrook Health Sciences Centre, North York General Hospital, Trillium Health
Partners, Women’s College Hospital, Hospital for Sick Children, Unity Health Network, Humber River Regional Hospital,
Scarborough Health Network
• Western University/London Health Sciences Centre: Lauren Cipriano, Wael Haddara
• St. Michael’s Hospital/University of Toronto: Bruno R. da Costa
• COVID-19 Heterogeneity Research Group: Huiting Ma, Adrienne Chan, Stefan Baral, Beate Sander, Sharmistha Mishra
19Content and review by Modelling Consensus and Scientific
Advisory Table members and secretariat
Beate Sander,* Peter Jüni, Brian Schwartz,* Upton Allen, Vanessa Allen, Kali Barrett, Isha Berry,
Pavlos Bobos, Nicolas Bodmer, Isaac Bogoch, Karen Born, Kevin Brown, Sarah Buchan, Swetaprovo
Chaudhuri, Yoojin Choi, Lauren Cipriano, Troy Day, David Earn,* Gerald Evans, Jennifer Gibson, Anne
Hayes,* Michael Hillmer, Jessica Hopkins, Jeff Kwong, Fiona Kouyoumdjian, Audrey Laporte, John
Lavis, Gerald Lebovic, Stephanie Lockert, Linda Mah, Kamil Malikov, Doug Manuel, Roisin McElroy,
Allison McGeer, Michelle Murti, John McLaughlin, Sharmistha Mishra, Andrew Morris, Samira
Mubareka, Christopher Mushquash, Ayodele Odutayo, Menaka Pai, Alyssa Parpia, Samir Patel, Anna
Perkhun, Justin Presseau, Fahad Razak, Rob Reid, Paula Rochon, Laura Rosella, Michael Schull,
Arjumand Siddiqi, Chris Simpson, Arthur Slutsky, Janet Smylie, Robert Steiner, Ashleigh Tuite, Tania
Watts, Ashini Weerasinghe, Scott Weese, Xiaolin Wei, Jianhong Wu, Diana Yan, Emre Yurga
*Chairs of Scientific Advisory, Evidence Synthesis, and Modelling Consensus Tables
For table membership and profiles, please visit the About and Partners pages on the Science
Advisory Table website.
20You can also read