Unusual Patterns of HER2 Expression in Breast Cancer: Insights and Perspectives
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review Article
Pathobiology 2022;89:278–296 Received: October 12, 2021
Accepted: March 13, 2022
DOI: 10.1159/000524227 Published online: May 2, 2022
Unusual Patterns of HER2 Expression in
Breast Cancer: Insights and Perspectives
Dora Grassini a, b Eliano Cascardi a, b Ivana Sarotto a Laura Annaratone a, b
Anna Sapino a, b Enrico Berrino a, b Caterina Marchiò a, b
aPathology
Unit, Candiolo Cancer Institute FPO-IRCCS, Candiolo, Italy; bDepartment of Medical Sciences, University
of Turin, Turin, Italy
Keywords which HER2 expression is unusual and/or difficult to define.
Breast cancer · Human epidermal growth factor receptor-2 · We will dissect HER2 heterogeneity, HER2 conversion from
Expression · Immunohistochemistry · Receptor conversion · primary to relapsed/metastatic breast cancer, and we will in-
HER2-low carcinomas troduce the new category of HER2-low breast carcinomas.
© 2022 The Author(s).
Published by S. Karger AG, Basel
Abstract
The biomarker human epidermal growth factor receptor-2 Introduction
(HER2) has represented the best example of successful tar-
geted therapy in breast cancer patients. Based on the con- The human epidermal growth factor receptor-2
cept of “oncogene addiction,” we have learnt how to iden- (HER2) has represented the main character of the preci-
tify patients likely benefitting from anti-HER2 agents. Since sion medicine era for breast cancer patients and holds a
HER2 gene amplification leads to marked overexpression of profound impact on tumour boards in the process of
the HER2 receptors on the cell membrane, immunohisto- treatment decision-making that ascertains the need to
chemistry with clinically validated antibodies and scoring tackle the disease with anti-HER2 agents. This biomarker
system based on intensity and completeness of the mem- has taught us the concept of “oncogene addiction,” i.e.,
branous expression constitute the screening method to sep- the phenomenon of dependency of certain tumour cells
arate negative (score 0/1+) and positive (score 3+) carcino- on a single activated oncogenic protein or pathway to
mas and to identify those tumours with complete yet only maintain their malignant properties, despite the likely ac-
moderate HER2 expression (score 2+, equivocal carcino- cumulation of multiple gain- and loss-of-function muta-
mas), which need to be investigated further in terms of gene tions that contribute to tumorigenicity [1]. As a proof of
status to confirm the presence of a loop of oncogene addic- principle, oncogene-driven tumours in preclinical mod-
tion. This process has demanded quality controls and led to els have been shown to undergo regression (in association
recommendations by Scientific Societies, which patholo- with proliferative arrest, apoptosis, and/or differentia-
gists routinely need to follow to guarantee reproducibility. tion) following the acute inhibition of oncoprotein func-
In this review, we will span from the description of classical tion [1].
HER2 evaluation to the discussion of those scenarios in
Karger@karger.com © 2022 The Author(s). Correspondence to:
www.karger.com/pat Published by S. Karger AG, Basel Caterina Marchiò, caterina.marchio @ unito.it
This is an Open Access article licensed under the Creative Commons
Attribution-NonCommercial-4.0 International License (CC BY-NC)
(http://www.karger.com/Services/OpenAccessLicense), applicable to
the online version of the article only. Usage and distribution for com-
mercial purposes requires written permission.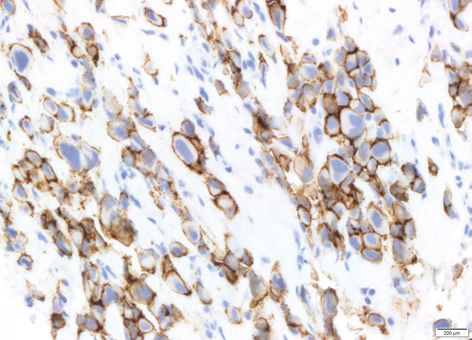
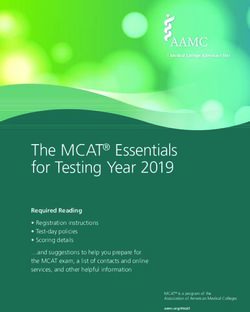
From this concept, we have learnt how to deal with the and on the percentage of positive cells. A four-tier scoring
identification of patients benefitting from the addition of system is used (shown in Fig. 1) and acknowledged as fol-
anti-HER2 agents. The impact of HER2 addiction in lows:
HER2-positive breast carcinomas is evident from the tre- • A score 0 (negative), where no staining can be ob-
mendous responses obtained over the course of a neoad- served or if it is incomplete and faint/barely percepti-
juvant therapy with anti-HER2 therapy associated with ble in ≤10% of tumour cells (shown in Fig. 1).
chemotherapy, with 60% of patients experiencing a path- • A score 1+ (negative) with an incomplete membrane
ological complete response (pCR) [2]. staining that is faint/barely perceptible in >10% of tu-
From a pathologist standpoint, this process has de- mour cells (shown in Fig. 1).
manded quality controls on pre-analytical, analytical, and • A score 2+ representing equivocal cases that show a
post-analytical factors and has led to specific recommen- weak to moderate complete membrane staining in
dations by Scientific Societies, which pathologists rou- >10% of tumour cells (shown in Fig. 1).
tinely follow to adhere to standard assessment, thus guar- • A score 3+ (positive) whenever there is a complete and
anteeing reproducibility. More recently, we have wit- intense circumferential membrane staining in >10% of
nessed exciting data stemming from novel antibody-drug tumour cells (shown in Fig. 1).
conjugates (ADCs) that seem to have efficacy even in In all IHC score 2+ cases, a reflex test on the same
those patients affected by breast carcinomas that would sample using ISH or a new test on a new sample using
be classically classified as HER2-negative but show a cer- IHC or ISH must be ordered. HER2 amplification is ex-
tain degree of HER2 protein on the tumour cell mem- pected in about 25% of score 2+ cases that are reflexed to
brane. This scenario is likely to drive a paradigm shift in ISH [3].
how we deal with HER2 evaluation, thus integrating the The evaluation of membrane staining intensity is sub-
spectrum of “HER2-low breast carcinomas.” We are cur- jected to human-eye perception. Especially when it comes
rently revisiting the importance of HER2 (over)expres- to distinguish between scores 1+ and 2+, the subjectivity
sion assessment under a new perspective, where the ex- of the interpretation of the scoring may lead to discordant
pression of a given protein may represent an anchor to a results among pathologists and/or institutions. Given the
novel therapeutic option. IHC is therefore currently un- central role of IHC HER2 evaluation in guiding therapy,
der the spotlight and is playing an essential role beyond a some authors have developed the so-called magnification
screening method to investigate HER2 oncogene addic- rule [4]. The latter uses the different magnifications of the
tion. objectives to perform a sort of triage across scores. A
In this review, we will span from description of classi- clear-cut intense staining perceived at low magnification
cal HER2 evaluation to the discussion of those scenarios (×2.5–×5) corresponds to a score 3+; stainings that can be
in which HER2 expression is unusual and/or difficult to appreciated at 10–20× would most likely fit into a score
define. Hence, we will deepen the description of HER2 2+, whereas whenever a 40× objective lens is needed to
heterogeneity, HER2 loss/conversion from primary to re- identify some staining, a score 1+ should be assigned.
lapsed/metastatic breast carcinomas, and the new catego- This rule may assist pathologists and may lead to an in-
ry of HER2-low breast carcinomas, from theory to prac- creased reproducibility in IHC scoring, especially with
tice. the perspective of introducing the new category of HER2-
low breast carcinomas; see below. Some national guide-
lines have already implemented the rule in both breast [5,
Evaluation of HER2 Expression “by the Guidelines”: 6] and gastric cancer [7].
Usual and Unusual Patterns The ASCO/CAP guidelines acknowledge the presence
of staining patterns that are not exactly fulfilling the defi-
HER2 status is assessed by combining IHC to assess nitions, yet they should be recognized and categorized
the protein levels and in situ hybridization (ISH) to assess accordingly (score 2+ is assigned) in order not to miss a
gene amplification. Although a frontline approach by ISH possible HER2-amplified tumour [8]. The unusual pat-
can be pursued, most pathology laboratories adopt a terns are mainly grouped into two categories, one featur-
screening by IHC to assess the degree of HER2 (over)ex- ing cases with IHC staining that is moderate to intense
pression, followed by reflex ISH testing in equivocal cas- but incomplete (basolateral or lateral) and one represent-
es. A scoring system has been devised, and it is based on ing carcinomas with a limited extent of bold HER2 over-
the intensity and completeness of the membrane staining expression.
Unusual HER2 Patterns Pathobiology 2022;89:278–296 279
DOI: 10.1159/000524227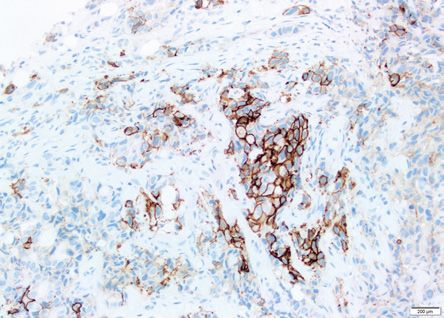
Score 0 Score 1+ Score 2+ Score 3+ Fig. 1. Scoring system for IHC reactions for HER2 assessment in equivocal and perfectly defines the cell membrane of the tumour breast cancer. Representative micrographs of breast carcinomas cells. Score 2+ is assigned when weak to moderate complete mem- showing a score 0, score 1+, score 2+, and score 3+ are illustrated brane staining is observed. Score 1+ emerges when an incomplete in the top panel. In the circles at the bottom, areas with different membrane staining that is faint/barely perceptible can be ob- HER2 scores within the same tumour are illustrated to best appre- served. The features here described all share a cut-off of pervasive- ciate the difference among scoring categories. Score 3+ is assigned ness of >10% across the tumour cell population. When an incom- when tumour cells show a complete and intense circumferential plete membrane staining that is faint/barely perceptible is ob- membrane staining. The intensity of the staining is markedly un- served in
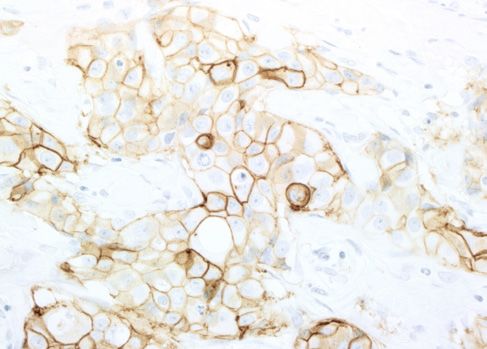
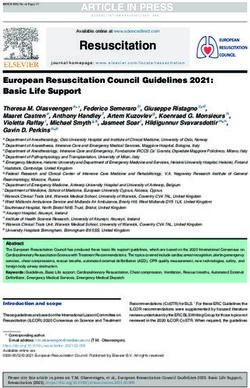
Fig. 2. Unusual pattern of HER2 positivity in micropapillary carcinomas. Micropapillary carcinomas have been
described to show the so-called U-shaped pattern of HER2 expression, featuring a basolateral lining of the cell
membrane with lack of HER2 expression on the luminal portion of the membrane, which is facing the stroma in
micropapillary carcinomas due to the reverted polarity. The intensity of expression can be variable, typically
moderate to intense. These cases must be considered score 2+ and reflexed to ISH analysis given that these car-
cinomas harbour HER2 amplification in about 30% of cases.
of HER2 amplification, thus raising the number of ISH normal HER2 status (“clustered or clonal type”) or, more
tests. Finally, we should mention that cytoplasmic granu- frequently, an intermingling of cells with different HER2
lar staining can be occasionally encountered (for instance, statuses that can be either diffuse or featuring only scat-
in apocrine carcinomas), as well as nuclear staining (often tered isolated HER2-amplified cells in a HER2-negative
in conjunction with cytoplasmic staining) and basal tumour cell population (“mosaic type”).
membrane pattern or pseudo-luminal staining (in well- When deepening the analysis of the relative frequency
differentiated breast carcinomas): these types of staining of HER2 heterogeneity in breast cancer, it should be ac-
are best considered artefactual and not associated with knowledged that the clustered type is reported to be much
HER2 gene alterations. rarer compared to the mosaic type [13, 14]; nevertheless
although many studies have reported prevalence of HER2
heterogeneity, few specify the granular data about type of
The Challenge of Heterogeneous Patterns of HER2 heterogeneity observed (clustered vs. mosaic type). Data
Expression from our institutional series of unselected breast carcino-
mas (cases diagnosed in year 2021, reported according to
Heterogeneity is present across breast carcinomas and the latest ASCO/CAP guidelines update [8]), which were
expressed across several features. HER2 expression/am- reviewed with the specific purpose of assigning the type
plification is no exception to this rule with a variable fre- of HER2 heterogeneity, revealed 0.01% of clustered-type
quency spanning from 1% to 40% [11, 12]. It is well known HER2 heterogeneity in an unselected cohort (i.e., all new-
that heterogeneity of HER2 expression/amplification fea- ly diagnosed breast carcinomas), 4% of all score 3+ and
tures three main patterns: we can encounter either two score 2+ cases subjected to fluorescence ISH (FISH), and
topographically distinct tumour clones of tumour cells, 10% of all positive cases. Conversely, the mosaic-type het-
one harbouring HER2 amplification, and the other with erogeneity was observed in 3% of the unselected cohort
Unusual HER2 Patterns Pathobiology 2022;89:278–296 281
DOI: 10.1159/000524227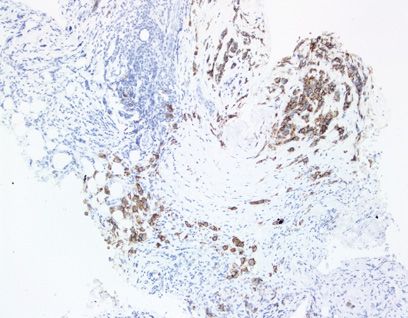
and in 15% of score 3+ and score 2+ subjected to FISH signals >6 typically harbour low levels of HER2 amplifica-
analysis and was restricted to score 2+ cases. These data tion [15, 18, 21, 23, 25].
are in line with reports from unselected [15] and HER2- The clustered type of HER2 heterogeneity is easier to be
positive cohorts [14]. defined as the tumour cell populations are clear-cut and
HER2 heterogeneity has also been reported to be sig- easily recognized on IHC and ISH grounds. This pattern
nificantly more common in cases with HER2 equivocal also suggests the presence of two different tumour types
status by ISH and/or IHC [13, 16–20], and some authors into one lesion or a sort of “collision tumour.” Whether
have shown that HER2 heterogeneity is an important one tumour cell population may derive from the other is
cause of equivocal HER2 results in breast cancer by FISH yet to be demonstrated. A genomic study exploiting gene
and IHC [19, 21, 22]. We have demonstrated that when- copy number (CN) profiling and massively parallel se-
ever assessing HER2 status in breast carcinomas with a quencing separately analysed the HER2-negative and
diffuse intermingling of HER2-amplified and nonampli- HER2-positive components of a small series of 12 HER2
fied cells, the overall scoring leads to HER2 equivocal heterogeneous breast carcinomas and identified potential
counts [23], the so-called Group 4 by ISH, as reported by driver genetic alterations restricted to the HER2-negative
Press et al. [24]. Of note, in these cases, cells with HER2 cells, thus suggesting that the HER2-negative compo-
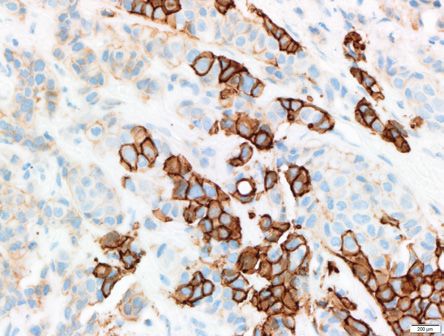
Usual pattern Unusual pattern
SCORE 3+
Report as score 2+, perform ISH, consider
addi�onal blocks
Usual patterns, different degrees of intensity
ISH
SCORE 2+
Unusual patterns, medium to strong intensity, incomplete membrane staining/fragmented membrane staining
Fig. 3. Usual and unusual HER2 patterns in breast carcinomas, as ISH to ascertain the degree of HER2 gene amplification within the
assessed by IHC. In these images, usual and unusual patterns of invasive tumour. In the middle panel examples of variable inten-
HER2 expression in breast cancer are summarized. On the top sity of usual HER2 stainings compatible with a score 2+ (weak to
panel, cases with score 3+ intensity and complete circumferential moderate complete membrane staining in >10% of tumour cells).
staining. When this pattern is encountered in >10% of tumour In the bottom panel a portfolio of unusual HER2 patterns scored
cells, we can report the usual score 3+. On the other hand, when- as score 2+ (basolateral staining in micropapillary carcinomas and
ever a breast carcinoma shows a very limited proportion (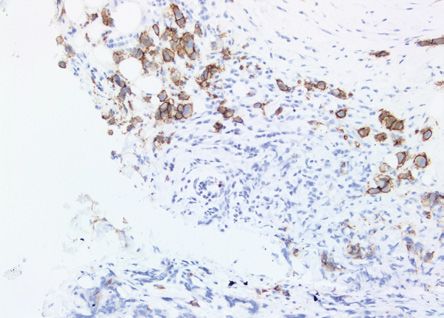
a b
c d
e f
g h
4
Unusual HER2 Patterns Pathobiology 2022;89:278–296 283
DOI: 10.1159/000524227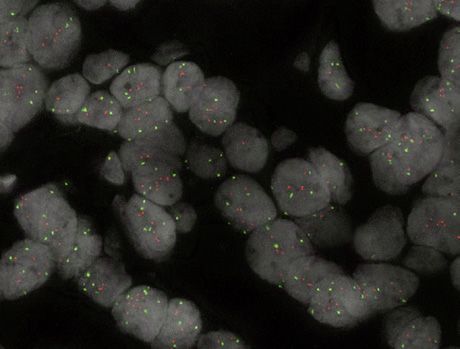
Fig. 5. Mosaic-type heterogeneity applied
to HER2. An invasive breast carcinoma
showing a score 2+ overexpression of
HER2 with scattered cells showing intense
and complete membranous staining (score
3+, a). Corresponding FISH images (b)
show a diffuse intermingling of tumour
cells with different HER2 statuses (red,
HER2 gene signals; green, CEP17 signals).
Arrow-headed lines point to nuclei har-
a b
bouring >6 signals.
nents are likely driven by genetic alterations not present negative). HER2 heterogeneity (defined as an area with
in the HER2-positive component [26]. HER2 amplification in >5% but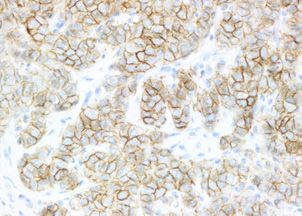
in a cohort of patients treated with neoadjuvant trastu- identify score 2+ cases to a lesser extent compared to hu- zumab-containing chemotherapy and observed that pCR man eye [30]. The implementation of computer-aided rates were significantly lower in double-equivocal carci- IHC scoring led to FDA approval of many of these algo- nomas with HER2 heterogeneity compared with HER2- rithms [28, 31], and in 2019, the College of American Pa- positive (score 3+) carcinomas (10% vs. 60%, Fisher exact thologists published recommendations to improve accu- test, p value = 0.009) [23]. Three cases showed a near-pCR racy, precision, and reproducibility of HER2 interpreta- (minimal residual disease [RD]/near-total effect/
breast cancer previously treated with T-DM1 [35] show- positive/HER2-low and 40% of HR-negative/HER2-low
ing an overall response rate (ORR) of 60.9% (6.0% com- metastatic breast carcinomas [43] indicating that SYD985
plete response, 54.9% partial response) and leading to might represent, in future, another treatment option in
Food and Drug Administration (FDA) and European the metastatic setting.
Medicines Agency (EMA) approval for HER2-positive Taken together, these data suggest that patients with
metastatic breast cancer already treated with two or more lesions showing low levels of HER2 might still benefit
anti-HER2 therapeutic regimens [36, 37]. The ongoing from new-generation ADCs, even if lacking HER2 ampli-
phase III DESTINY-Breast03 trial is comparing efficacy fication. Hence, it does not come as a surprise if experts
and safety of DS-8201 and T-DM1 in 524 HER2-positive in the field have developed an interest in the identifica-
metastatic breast cancer patients already treated with tax- tion of a new category labelled as “HER2-low” breast car-
ane + trastuzumab. Early results presented at the ESMO cinomas, i.e., tumours displaying some degree of expres-
2021 meeting showed an improvement in progression- sion of the HER2 protein not stemming from HER2 gene
free survival (PFS) of DS-8201 over T-DM1 and an ORR amplification (Fig. 6). These carcinomas would not be
of 79.7% and 34.2%, respectively [38]. These data encour- therefore “HER2-addicted,” but rather “HER2-equipped”
aged FDA to grant the breakthrough therapy designation or “HER2-scaffolded.” The scaffold offered by the degree
for DS-8201 in HER2-positive unresectable or metastatic of HER2 receptors expressed on the membrane seems to
breast cancer patients already treated with at least one be enough to favour the delivery of a cytotoxic agent
anti-HER2 therapeutic regimen [39]. This decision may through anchorage of the anti-HER2 antibody to the
soon lead to a change in the second line of therapy for HER2 receptors that here serve as simple vehicles.
HER2-positive metastatic breast cancer patients. Studies At present, HER2-low breast carcinomas are being de-
testing T-DM1 only included HER2-positive tumours, fined on immunohistochemical grounds by exploiting
but retrospective analyses conducted by reviewing HER2 the current scoring system and include tumours reported
status identified HER2-low tumours and showed that no as HER2 score 1+ or score 2+ with a negative ISH result.
benefit can be derived from T-DM1 in this subtype [40]. HER2-low tumours represent up to 55% of breast cancer,
On the other hand, DS-8201 showed antitumour activity estimated to be HR-positive in the 65–83% of the cases
in a cohort of 34 pretreated HER2-low metastatic breast and HR-negative in the remaining percentage. A study
cancers [41]. The ORR was 50%, increasing to 55.2% comparing HER2 status between primary versus relapsed
when only considering the HR-positive subgroup (29/34); lesions observed 15% of HER2-negative tumours con-
interestingly, when excluding patients already treated verting to HER2-low and 14% of HER2-low to HER2-
with an anti-HER2-containing regimen, the ORR lowers negative. HER2-low status was found in 34% and 38% of
to 46.2%. primary and relapsed tumours, respectively [44].
At present, the DESTINY-Breast06 trial is actively re- The reasons for the presence of HER2 protein expres-
cruiting patients with HER2-low disease. This study is de- sion without an underlying HER2 gene amplification
signed to evaluate the efficacy, safety, and tolerability of have not been clarified yet, but an increased HER2 CNs
DS-8201 compared with investigator’s choice chemo- may explain this phenomenon. In addition, the upregula-
therapy in HER2-low, HR-positive breast cancer patients tion of HER2 induced by NF-kB pathway activation in-
whose disease has progressed on endocrine therapy in the duced by chemotherapy and radiation therapy or by epi-
metastatic setting. genetic changes has been associated with increased HER2
Trastuzumab duocarmazine (SYD985) links the expression in the absence of HER2 gene amplification.
monoclonal antibody to the alkylating agent duocarmy- Furthermore, the crosstalk between HER2 and oestrogen
cin. Its safety and efficacy are now being compared to a receptor pathways or modifications deriving from adap-
treatment of physician’s choice in the phase III TULIP tation or resistance to treatments has been reported to
clinical trial in 437 HER2-positive locally advanced or upregulate HER2 protein levels [40].
metastatic breast cancer patients already treated with at In two retrospective analyses, Schettini et al. [45] and
least two therapeutic regimens or with T-DM1. Prelimi- Agostinetto et al. [46] investigated the molecular and
nary results showed an improvement in PFS (7 months pathological characteristics and prognostic impact of
vs. 4.9 months), while no significant differences were HER2-low breast cancer. Schettini retrospectively col-
found in terms of ORR [42]. SYD985 has also been tested lected clinicopathological and PAM50 gene expression
in a phase I dose-escalation and dose-expansion study data from 13 publicly available datasets deriving from dif-
and showed a partial objective response in 28% of HR- ferent studies for a total of 3,689 HER2-negative breast
286 Pathobiology 2022;89:278–296 Grassini/Cascardi/Sarotto/Annaratone/
DOI: 10.1159/000524227 Sapino/Berrino/MarchiòHER2 amp
HER2 amp
HER2 amp
mas
carcino
cted
- addi
HER2
not amp
HER2
not amp
HE
HER2
R2
-lo
w
ca
Assessment of HER2 expression by rci
nom
IHC using clinically validated anti- as
HER-antibodies
Fig. 6. Spectrum of HER2 overexpression by IHC across breast HER2 gene amplification or with a score 1+ are encountered in
carcinomas. A spectrum of distinct levels of HER2 expression in breast carcinomas, these have been correlated with response to
breast carcinomas as assessed by IHC is represented. ISH data are new anti-HER2 compounds, i.e., ADCs, formed by a monoclonal
annotated in italics in close proximity to the pictures. The combi- antibody anti-HER2 linked to a cytotoxic agent. These carcinomas
nation of the two data allows to show a category of breast carcino- are defined “HER2-low” and are “HER2-equipped”: they have the
mas with clear-cut HER2 overexpression, in the form of either a potential to respond to these drugs because the scaffold offered by
score 3+ or a score 2+, both driven by HER2 gene amplification. the degree of HER2 receptors expressed on the membrane seems
These carcinomas are HER2-positive and HER2-addicted: they to be enough to favour the delivery of a cytotoxic agent through
have the potential to be responsive to anti-HER2 agents that block anchorage of the anti-HER2 antibody to the HER2 receptors that
the signal transduction pathway activated by HER2 overexpres- here serve as simple vehicles.
sion. Whenever levels of HER2 compatible with a score 2+ without
cancers with known IHC and HER2 amplification status. compared to HR-negative/HER2-low tumours. No statis-
The purpose was to provide a first characterization of tically significant differences were observed between
HER2-low breast cancer and compare the features of HER2-low and non-HER2-low regarding progression-
HER2-low and HER2 0 disease. HER2-low tumours were free interval, disease-free interval, and OS.
found to be associated with larger tumour size and more In a recent analysis, Denkert et al. [47] compared clin-
nodal involvement, being mostly HR-positive. Luminal A ical and molecular features of HER2-low and HER2 0
was the most frequent intrinsic subtype, followed by the breast cancer with a particular focus on response to ther-
luminal B. Within the HR-positive disease, HER2-low apy by exploiting the neoadjuvant setting. Besides con-
presented higher levels of HER2 mRNA compared to firming a higher prevalence of HER2-low disease among
HER2 score 0 carcinomas. No differences in OS between HR-positive tumours, they detected a lower pCR rate in
HER2-low and HER2 score 0 carcinomas were observed. HER2-low/HR-positive compared to HER2 0/HR-posi-
To further unravel HER2-low features, Agostinetto tive, but no significant difference was found among the
performed a retrospective analysis of more homogeneous HR-negative disease. On the other hand, longer disease-
data from The Cancer Genome Atlas (TCGA) including free survival (DFS) and OS were present among HER2-
1,097 primary breast cancers with known HR and HER2 low/HR-negative tumours compared to HER2 score 0 but
status. They confirmed previous findings by observing not among HR-positive breast cancer patients.
HER2-low tumours to be mostly HR-positive, Luminal A. Based on the data available so far, it is still premature
HR-positive/HER2-low HER2 mRNA levels were higher to draw definitive conclusions on whether HER2-low car-
Unusual HER2 Patterns Pathobiology 2022;89:278–296 287
DOI: 10.1159/000524227cinomas may constitute a distinct subtype of breast car- tissue samples collected in clinical trials focused on the
cinomas. At present, the “HER2-low” definition may rep- treatment of HER2-low breast cancer patients may help
resent an umbrella term including different types of understand whether IHC is an adequate method to detect
breast carcinomas sharing different degrees of HER2 the best responders.
(over)expression. Nevertheless, as mentioned above the
promising results deriving from the ADCs studies even in
the HER2-low breast carcinomas have urged the need of HER2 Conversion and HER2 Loss
a change in the clinical classification of HER2-expressing
breast cancer. Pathologists have been used to applying a The so-called receptor conversion, i.e., the discor-
dichotomous separation of HER2 status, positive (score dance of HR or HER2 status between primary tumour
3+ and score 2+ to be verified by IHS) versus negative and metastatic deposits over the clinical history of a given
(score 0 and 1+). Hence, the distinction between score 0 patient, is a relevant issue since it would require to recon-
and 1+ has not been under the spotlight; however, this sider a possible shift in treatment decision-making. On
will have to be emphasized to reach the new categoriza- the one side, it is universally recommended to retest one
tion into (i) HER2-negative (score 0), (ii) HER2-low or multiple metastatic deposits for biomarker evaluation
(score 1+ and score 2+ not amplified), and (iii) HER2- to better target the disease under evolution. On the other
positive (score 2+ HER2 amplified and score 3+) carcino- side, it must be acknowledged that biomarker conversion
mas. Further data on the degree of response across HER2- in retesting does not necessarily lead to a prompt change
low carcinomas may also help in the fine tune of the real of therapy based on the new profile. In general, medical
needs from the pathological evaluation of these carcino- oncologists consider the issue of heterogeneity (whenever
mas. multiple metastases are present) and the availability of
It should be emphasized that, at least at present, IHC therapeutic options. Whenever the conversion is toward
protocols for HER2 testing should not be changed or a positivity in a biomarker, this would mean a therapeutic
adapted to be able to detect HER2-low carcinomas. As agent to be added to the treatment schedule, which holds
discussed above, the definition relies on the current IHC a potent therapeutic impact compared to loss of expres-
scoring system based on traditional IHC staining proto- sion of a given biomarker.
cols. The challenge lies in the reproducibility of the scor- Different studies have investigated the phenomenon
ing [45, 48], which in turn may suffer from technical is- of HER2 conversion between primary and relapsed/met-
sues, including pre-analytical factors. Quality assurance astatic diseases (Table 1), and early studies reported a
programmes are of utmost importance in this context. Of wide range of discordance rate varying from 0% to 44%.
note, some national expert groups such as the French GE- To best understand the true extent of this phenomenon,
FPICS group have already endorsed this new category in meta-analyses have been conducted. Aurilio et al. [50] se-
their guidelines [6] as well as in their quality assurance lected published data from 48 studies evaluating concor-
programmes (see, for instance, AFAQAP programme in dance in receptor expression and HER2 status between
France). primary tumour and both local and distant metastases.
Education on optimal HER2 scoring to adequately HER2 discordance rates were heterogeneous (0–24%).
identify score 1+ versus score 0 carcinoma may be benefi- The meta-analytic pooling assessed a discordance rate of
cial as well. Nevertheless, it is worth mentioning that at 8%. When stratified according to site of relapse, the dis-
the latest San Antonio Breast Cancer Symposium the cordance rate was 10% and 6% for distant and locore-
phase II study “DAISY” reported 30% of response rates in gional metastases, respectively. Regarding the quality of
score 0 breast carcinoma patients treated with DS-8201 HER2 conversion, 13% of patient changed from positive
[49]. Although data are still premature to draw any de- to negative and 5% from negative to positive.
finitive conclusions, HER2-low and ultra-low breast can- In a more recent meta-analysis, Schrijver et al. [51] an-
cers are now – even more than before – under the spot- alysed data from 39 studies considering only distant me-
light and the correct definition of the lowest limit of tastases, focusing on the type of technique used for HER2
HER2-low expression is still under proper definition. As assessment and on metastasis location-specific differenc-
a matter of fact, we should remember that the IHC pro- es. HER2 conversion was identified in a range between
tocols that we routinely use with clinically validated anti- 0% and 34%, with a mean of 10.3%. Conversion from
bodies have been devised to discriminate HER2-addicted HER2-positive to HER2-negative disease was observed in
versus HER2-not addicted carcinomas. Data analysis on 21.3% of cases, whereas in 9.5% of cases HER2 status
288 Pathobiology 2022;89:278–296 Grassini/Cascardi/Sarotto/Annaratone/
DOI: 10.1159/000524227 Sapino/Berrino/MarchiòUnusual HER2 Patterns
Table 1. Summary of studies reporting HER2 status conversion over treatment
Study Setting N Conversion, n HER2 loss HER2 gain Outcome main result
Aurilio et al. [50] Primary versus local and distant mts 2,987 8 13% of the HER2-positive 5% of the HER2-negative –
(meta-analysis)
Schrijver et al. [51] Primary versus distant mts 2,440 10.3 21.3% of the HER2-positive 9.5% of the HER2- –
(meta-analysis) negative
Chen et al. [52] Primary versus mts 320 13.7 28.7% of the HER2-positive 8.1% of the HER2- MFS and OS not
negative significant
ESME report [53] Primary versus mts 1,076 7.8 45.2% of the total cohort experiencing a 54.8% of the total cohort PFS and OS not
conversion experiencing a significant
conversion
Mittendorf et al. [54] Primary versus RD 25 32 32% of the cases with residual carcinomas – Significantly worse PFS
for HER2 loss
Guarneri et al. [55] CT versus CT + anti-HER2 107 – 40% of the cases with residual carcinoma – Significantly worse PFS
treated with CT versus 14.7% of the cases for HER2 loss
with residual carcinoma treated with CT +
anti-HER2
Niikura et al. [56] Primary versus RD 16,271 24.7 (trast) 21.4% of the cases with residual carcinoma 3.4% of the cases with –
DOI: 10.1159/000524227
18.2 (no trast) residual carcinoma
Pathobiology 2022;89:278–296
Wang et al. [57] CT versus CT + anti-HER2 459 – 19.8 (CT + trast) versus 9.4 (CT only) – Significantly worse PFS
for HER2 loss
Ignatov et al. [59] Primary versus RD 205 – 42% of the cases with residual carcinomas – Significantly worse PFS
and trend for OS (not
significant) for HER2 loss
Tural et al. [60] Primary versus RD 186 18 18% of the cases with residual carcinomas – Significantly worse PFS
for HER2 loss
Branco et al. [58] Primary versus RD 108 13 13% of the cases with residual carcinomas – Significantly PFS and OS
worse for HER2 loss
Katayama et al. [61] Primary versus RD 221 – 22.3% of the cases with residual carcinomas 15.9% of the cases with –
residual carcinomas
MFS, metastasis-free survival; PFS, progression-free survival; OS, overall survival.
289shifted from negative to positive. Total discordance rates with RD of cohort A and in 14.7% of patients of cohort B.
accounted for 11.5%, 12.7%, and 9.8% when using FISH, This study highlights that HER2 loss can be experienced
IHC, and both, respectively. No statistically significant also following chemotherapy regimens only. Patients
metastatic location-specific differences for pooled discor- with HER2 loss tended to have a poorer DFS compared
dance were found. to patients who maintained HER2 positivity. Niikura et
To produce data as homogenous as possible, Chen et al. al. [56] reported similar findings with 21.4% of HER2-
[52] studied 320 paired primary and metastatic breast car- positive tumours converting to HER2-negative after
cinomas from a single institution, considering also the treatment versus 3.4% of HER2-negative patients show-
prognostic impact of HER2 status conversion. HER2 con- ing a HER2-positive residual tumour. Discordance was
version was observed in 13.7% of cases, with positive to neg- observed in 24.7% of patients who received trastuzumab
ative conversion occurring in 28.7% of cases and negative and in 18.2% of who did not receive trastuzumab.
to positive conversion in 8.1% of cases. No statistically sig- Other neoadjuvant studies have reported HER2 loss
nificant site-specific differences were found; however, the over the course of a neoadjuvant treatment (range: 18–
author reports a 14.3% discordance among different sites of 42%), but with a higher percentage of HER2 loss in re-
relapse in patients with multi-organ metastasis. No signifi- sidual tumours of patients treated with trastuzumab-con-
cant differences were found in terms of OS. taining chemotherapy compared to chemotherapy only
The ESME report recently published results from a (Table 1) [57–60]. These studies have also reported a
large cohort of patients and showed that at time of diag- higher risk of relapse for patients experiencing HER2 loss
nosis of metastatic disease HER2 status discordance was [57–60].
detected in 7.8% of cases (loss of HER2 amplification in Interestingly, Ignatov et al. [59] reported comparative
45.2% of cases and HER2 gain in 54.8%), whereas after data for trastuzumab versus the dual blockade trastuzum-
first progression the discordance rate was 10% (loss = ab + pertuzumab. Out of the 205 patients with HER2-
50.9% and gain = 49.1%). HER2 discordance was not sig- overexpressing carcinomas that were studied, 42%
nificantly associated with OS [53]. showed HER2 loss over the course of the neoadjuvant
Taken together, these data suggest that HER2 discor- treatment. When the combination of trastuzumab and
dance between primary tumour and metastatic disease pertuzumab was adopted, 63.2% of cases experienced a
more frequently features “HER2 loss.” The underlying decrease in HER2 levels, whereas only 47.3% of cases had
mechanisms have not been clarified yet, but plausible ex- a HER2 loss when trastuzumab was employed. In terms
planations are represented by tumour heterogeneity, and of outcome, the 5-year DFS was 74.4% for HER2-concor-
selective selection due to clonal evolution or therapeutic dant and 59.6% for the HER2-discordant cases, respec-
pressure. As mentioned above, therapies are not neces- tively. No influence on OS was observed.
sarily modified based on the profile identified in a biopsy Finally, Katayama et al. [61] also performed assess-
of metastatic deposit; hence, insufficient data are avail- ment of ISH data. Out of the HER2-positive carcinomas,
able regarding the long-term effect of a possible therapy a subgroup of 22.3% shifted to HER2-negative; in addi-
switch. tion, 15.9% of the HER2-negative carcinomas became
HER2 discordance has also been studied between na- HER2-positive. Average HER2 gene and CEP17 CN on
ïve primary tumours and RD following neoadjuvant ther- pre- and post-treatment samples were also evaluated for
apy (Table 1). In one of the earliest studies, Mittendorf et IHC score 2+ cases. Within the patients who changed
al. [54] evaluated HER2 status in 25/142 patients who did from IHC2+/HER2-amplified to IHC2+/HER2-not-am-
not reach a pCR following neoadjuvant chemotherapy + plified, 65.2% maintained the same HER2 gene CN, while
trastuzumab and observed 32% of cases with HER2 loss 34.8% showed a decreased HER2 gene CN. Among those
on the RD. Moreover, loss of HER2 overexpression was that shifted from IHC2+/HER2-not-amplified to
associated with worse recurrence-free survival: the 3-year IHC2+/HER2-amplified, 76.9% maintained the same
recurrence-free survival estimates were 87.5% for pa- HER2 gene CN and 23.1% showed an increased HER2
tients maintaining HER2 amplification and 50% for pa- CN. These results may highlight that variability was min-
tients whose tumour showed HER2 loss. Guarneri et al. imal in terms of HER2 gene alterations and shifts from
[55] enrolled 107 patients in two cohorts and adminis- negative to positive tests were most likely because of val-
tered neoadjuvant chemotherapy (cohort A) or neoadju- ues close to thresholds of positivity.
vant chemotherapy + an anti-HER2 agent (cohort B). Taken together, these data suggest that HER2 status
Loss of HER2 expression was observed in 40% of patients may be influenced by neoadjuvant therapy. HER2 change
290 Pathobiology 2022;89:278–296 Grassini/Cascardi/Sarotto/Annaratone/
DOI: 10.1159/000524227 Sapino/Berrino/Marchiòoccurs more frequently as a loss, and it seems to be par- by using a vacuum storage up to 72 h [71]. The fixative of
ticularly influenced by the addition of anti-HER2 agents. choice is represented by 10% neutral buffered formalin
It remains unclear if this phenomenon is the reflection of [69, 72].
response/resistance to therapy or the expression of an un- In the context of HER2 testing, fixation issues have led
derlying HER2 heterogeneity. Nevertheless, HER2 loss to poor reproducibility of results [73]. To better under-
following neoadjuvant chemotherapy seems to represent stand the effect of fixation time, comparative studies were
a negative prognostic factor in terms of PFS, without af- conducted to show the consequences of a reduced or an
fecting the OS. excessive formalin incubation time. Studies assessing un-
Of note, HER2 re-assessment following neoadjuvant der-fixation (reviewed in [74]) or over-fixation [75]
chemotherapy is a debated matter for HER2-positive pa- alone, as well as comparative studies [76, 77], have shown
tients; nevertheless, it seems to be rather informative and a limited impact of formalin over tissues characterized by
would add prognostic information. The KATHERINE a “clear-cut” expression of the HER2 protein. Interest-
clinical trial [62], which has compared T-DM1 and trastu- ingly, a complete agreement in the interpretation for
zumab in the adjuvant setting of HER2-positive breast HER2-negative (score 0) and HER2-positive (score 3+)
cancer patients with residual-invasive disease after neo- cases was reported, regardless of the time of fixation [76,
adjuvant therapy containing taxanes + trastuzumab, has 77]. On the other hand, HER2 detection was affected in
shown that the risk of recurrence or death was 50% lower breast carcinomas showing intermediate levels of expres-
in the T-DM1 cohort, thus leading to a practice change sion (score 1+ and score 2+), thus suggesting a significant
on how we tackle HER2-positive RD following neoadju- impact of the fixation time on the HER2-low category
vant chemotherapy. Of note, the requirement for the tri- that may undergo important reclassifications in the con-
al was to have a positive HER2 assessment either in the text of poorly preserved tissues [75, 78–81].
pre-treatment core biopsy or in the RD. Given the known Another matter of interest related to pre-analytical
phenomenon of HER2 loss over the course of trastuzum- conditions is associated with the different types of speci-
ab-containing chemotherapy, it would be interesting to mens that may be subjected to HER2 testing. Both core
understand whether or not patients with RD character- needle biopsies (CNBs) and surgical resections represent
ized by HER2 loss would still benefit more from T-DM1 adequate specimens for HER2 testing (full sections of the
over trastuzumab-containing chemotherapy. tissue blocks) in primary tumours. A high level of agree-
ment has also been reported between both surgical resec-
tions and CNBs [82], in particular whenever multiple
Pre-Analytical Phase and Impact on HER2 Expression core biopsies are available for a given lesion [83]. The lat-
Assessment in Different Types of Tissue Samples ter helps capture intratumoral heterogeneity, whose full
picture is well obtained in samples from surgical speci-
The sensitivity of the IHC method and accuracy of in- mens. Recently, Miglietta et al. [84] have reported higher
terpretation of HER2 expression assessment in breast rates of HER2-low cases when assessing HER2 expression
cancer represent an old issue [63]. As a matter of fact, the on CNBs compared to surgical specimens, thus suggest-
protein detection on formalin-fixed, paraffin-embedded ing that the reliability of CNBs evaluation when including
tissue samples by IHC is strongly influenced by pre-ana- the HER2-low category needs to be deeper assessed. This
lytical variables, in particular by the fixation process [64, observation needs to be further explored in independent
65]. For instance, an uncontrolled formalin fixation tim- studies.
ing and duration modulate immunoreactivity, with struc- The advantages of using core biopsies are mainly re-
tural and macromolecular alterations caused by both un- lated to anticipation of the information about tumour
der- and over-fixation [66, 67]. phenotype before surgical intervention and the optimal
To maximize the standardization of the IHC proce- tissue fixation obtained thanks to the small size of CNB
dure, the ASCO/CAP guidelines for HER2 evaluation samples [85, 86]. Recent studies have shown that reduced
recommend (i) an immediate incubation of tissue sample fixation times (even a few hours) do not compromise the
in the fixative, thus minimizing ischemic time (≤1 h), and quality and concordance of the HER2 test [87, 88], thus
(ii) a fixation time of 6–48 h. The time between tissue col- confirming the indication of the original ASCO/CAP
lection and tissue fixation must not exceed 60 min [68, guidelines which indicate 6–8 h as the optimal fixation
69], with a potential reduction of macro-degradation time for biopsies, with reduction to 1 h in case of extreme
through a controlled temperature protocol (4°C) [70] or need [72].
Unusual HER2 Patterns Pathobiology 2022;89:278–296 291
DOI: 10.1159/000524227Biopsies are also the typical sample available for meta- HER2 testing. When dealing with histological samples,
static lesions, whose re-assessment in terms of biomark- research studies often exploit the advantage of tissue mi-
ers is mandatory in breast cancer. Heterogeneity across croarray (TMA). This is a technique that has also been
metastatic site can be encountered; hence, a change in explored to some extent for routine practice [99]. We re-
treatment schedule is typically embraced when a conver- ported, for instance, in the context of breast cancer bio-
sion from a HER2-negative to a HER2-positive result is marker assessment (hormonal receptors, HER2, and
observed on a metastatic site. In some instances, limited Ki67) a 95% agreement between TMA and full sections;
tumour material may be sampled with biopsies, thus fur- however, four cores per lesions were sampled to allow
ther complicating the conduction of a reliable evaluation proper representativeness of the tumoral lesion. Intratu-
of the real biomarker profile of the lesion. Active interac- moral heterogeneity greatly limits the implementation of
tion with medical oncologists is advised in this context. TMA in routine diagnostics, and TMA use is not recom-
Cytological specimens may also represent a tissue mended in diagnostic practice.
source in these scenarios; however, careful management
of the fixation method is needed. Although alcohol fixa-
tion has been reported to be very effective in preserving Conclusions
the molecular components of cytologic specimens [89,
90], the ASCO/CAP guidelines for the evaluation of HER2 expression assessment by IHC plays a central
HER2 status recommend formalin fixation for cytological role in breast cancer diagnostic pathology and has been
samples [8, 69, 72]. used to identify breast carcinomas addicted to HER2 gene
When discussing different types of tissue specimens amplification, which leads to a massive overexpression of
and metastatic lesions, bone tissue management merits a the HER2 protein on the cell membrane. We know that
separate chapter. Bone is the first metastatic site for breast HER2 overexpression can be present in variable degrees
cancer [91], thus representing an important sampling site and shapes, even featuring some unusual patterns that do
for re-evaluation of HER2 status. Decalcification proce- not exactly fulfil the categories according to the historical
dures aim to remove calcium phosphate, thus allowing scoring system proposed by ASCO/CAP. The ASCO/
sectioning, with several protocols available [92]. The det- CAP recommendations acknowledge such patterns and
rimental effect of decalcification mainly affects the qual- speak a word of caution on how to address these unusual
ity of nucleic acids [93], while methods such as IHC seem scenarios. HER2 heterogeneity can create difficulties in
not to be significantly affected [94]. Studies focusing on the final definition of the HER2 status of individual pa-
HER2 assessment have shown that decalcification does tients and needs to be discussed with medical oncologists.
reduce the success rate of the IHC [95, 96] resulting in the Another chance of active discussion with medical oncol-
lack of a decalcification protocol recognized as the “gold ogists is encountered whenever the HER2 status changes
standard” for the downstream IHC application [97]. The over the course of the clinical history of the patient. Loss
use of an EDTA-based method should be considered in of HER2 expression seems to be more frequent than ac-
view of the possible downstream FISH evaluation for quisition of HER2 positivity. HER2 loss has been de-
HER2 gene status, since better results have been shown scribed also following neoadjuvant chemotherapy and
with this protocol [98]. seems to hold prognostic information, thus highlighting
In the context of pre-analytical factors, it should be the informativeness of re-assessing biomarkers on carci-
emphasized that ASCO/CAP guidelines [69] highlight nomas not reaching pCR.
the importance of both internal and external quality con- Finally, at present we are revisiting the importance of
trol assessments for laboratories conducting HER2 as- HER2 (over)expression assessment under a new perspec-
says. External quality control assessment relies on the tive, where the expression of a given protein may repre-
participation and completion of external proficiency tests sent an anchor to a novel therapeutic option, as it has
and onsite inspections; moreover, the recommendations been shown for the subgroup of “HER2-low” carcinomas.
provide examples of international quality assurance pro- IHC is therefore again under the spotlight. Although sim-
grammes. On the other hand, internal quality assessment ple and widespread across pathology laboratories, IHC is
programmes are not well defined, besides the recommen- not free from pre-analytical issues and pathologists must
dation to use FDA-approved assays. be aware of the critical steps that may hamper immuno-
A final remark to exhaustively cover this section is histochemical performance of HER2 assays and their
dedicated to alternative tissue samples as a source for evaluation. This seems to be particularly important for
292 Pathobiology 2022;89:278–296 Grassini/Cascardi/Sarotto/Annaratone/
DOI: 10.1159/000524227 Sapino/Berrino/Marchiòthe lower end of the HER2 expression spectrum; hence, it Funding Sources
may have an impact on the identification of the so-called
We acknowledge funding from Fondazione AIRC under
HER2-low carcinomas. IG2019 id.22850, PI Caterina Marchiò, and FPRC 5X1000 MS2017
PTCRC.
Conflict of Interest Statement
Author Contributions
Caterina Marchiò has received personal consultancy fees from
Roche, Bayer, AstraZeneca, Daiichi Sankyo, and Novartis. Cateri-
Dora Grassini, Enrico Berrino, and Eliano Cascardi performed
na Marchiò serves as an Associate Editor for Pathobiology. Dora
literature search and contributed to writing and to illustrations.
Grassini, Eliano Cascardi, Ivana Sarotto, Laura Annaratone, Anna
Caterina Marchiò has drafted the review structure and wrote the
Sapino, and Enrico Berrino have no conflicts of interest to declare.
first draft of the manuscript, which was revised and integrated by
Laura Annaratone, Anna Sapino, and Ivana Sarotto.
References
1 Weinstein IB, Joe A. Oncogene addiction. 9 Vingiani A, Maisonneuve P, Dell’orto P, Far- breast carcinoma. J Clin Pathol. 2011 Dec;
Cancer Res. 2008 May 1; 68(9): 3077–80; dis- ante G, Rotmensz N, Lissidini G, et al. The 64(12):1112–6.
cussion 80 clinical relevance of micropapillary carcino- 18 Seol H, Lee HJ, Choi Y, Lee HE, Kim YJ, Kim
2 Miglietta F, Dieci MV, Griguolo G, Guarneri ma of the breast: a case-control study. Histo- JH, et al. Intratumoral heterogeneity of HER2
V. Neoadjuvant approach as a platform for pathology. 2013 Aug;63(2):217–24. gene amplification in breast cancer: its clini-
treatment personalization: focus on HER2- 10 Zhou S, Yang F, Bai Q, Li A, Li M, Zhong S, et copathological significance. Mod Pathol.
positive and triple-negative breast cancer. al. Intense basolateral membrane staining in- 2012 Jul;25(7):938–48.
Cancer Treat Rev. 2021 Jul;98:102222. dicates HER2 positivity in invasive micropap- 19 Shafi H, Astvatsaturyan K, Chung F, Mirocha
3 Sapino A, Maletta F, Verdun di Cantogno L, illary breast carcinoma. Mod Pathol. 2020 Jul; J, Schmidt M, Bose S. Clinicopathological sig-
Macri L, Botta C, Gugliotta P, et al. Gene sta- 33(7):1275–86. nificance of HER2/neu genetic heterogeneity
tus in HER2 equivocal breast carcinomas: im- 11 Hanna WM, Ruschoff J, Bilous M, Coudry in HER2/neu non-amplified invasive breast
pact of distinct recommendations and contri- RA, Dowsett M, Osamura RY, et al. HER2 in carcinomas and its concurrent axillary metas-
bution of a polymerase chain reaction-based situ hybridization in breast cancer: clinical tasis. J Clin Pathol. 2013 Aug;66(8):649–54.
method. Oncologist. 2014 Nov; 19(11): 1118– implications of polysomy 17 and genetic het- 20 Lee HJ, Seo AN, Kim EJ, Jang MH, Suh KJ,
26. erogeneity. Mod Pathol. 2014 Jan;27(1):4–18. Ryu HS, et al. HER2 heterogeneity affects
4 Scheel AH, Penault-Llorca F, Hanna W, Bar- 12 Marchio C, Annaratone L, Marques A, Casor- trastuzumab responses and survival in pa-
etton G, Middel P, Burchhardt J, et al. Physical zo L, Berrino E, Sapino A. Evolving concepts tients with HER2-positive metastatic breast
basis of the “magnification rule” for standard- in HER2 evaluation in breast cancer: hetero- cancer. Am J Clin Pathol. 2014 Dec; 142(6):
ized Immunohistochemical scoring of HER2 geneity, HER2-low carcinomas and beyond. 755–66.
in breast and gastric cancer. Diagn Pathol. Semin Cancer Biol. 2021 Jul;72:123–35. 21 Yang YL, Fan Y, Lang RG, Gu F, Ren MJ,
2018 Mar 12;13(1):19. 13 Allison KH, Dintzis SM, Schmidt RA. Fre- Zhang XM, et al. Genetic heterogeneity of
5 Penault-Llorca F, Vincent-Salomon A, Mac- quency of HER2 heterogeneity by fluores- HER2 in breast cancer: impact on HER2 test-
Grogan G, Roger P, Treilleux I, Valent A, et cence in situ hybridization according to CAP ing and its clinicopathologic significance.
al. 2014 update of the GEFPICS’ recommen- expert panel recommendations: time for a Breast Cancer Res Treat. 2012 Aug; 134(3):
dations for HER2 status determination in new look at how to report heterogeneity. Am 1095–102.
breast cancers in France. Ann Pathol. 2014 J Clin Pathol. 2011 Dec;136(6):864–71. 22 Buckley NE, Forde C, McArt DG, Boyle DP,
Oct;34(5):352–65. 14 Akashi M, Yamaguchi R, Kusano H, Yamagu- Mullan PB, James JA, et al. Quantification of
6 Franchet C, Djerroudi L, Maran-Gonzalez A, chi M, Akiba J, Kakuma T, et al. ER staining HER2 heterogeneity in breast cancer-impli-
Abramovici O, Antoine M, Becette V, et al. levels affect HER2 staining and heterogeneity. cations for identification of sub-dominant
2021 update of the GEFPICS’ recommenda- Breast Cancer. 2021 May;28(3):720–6. clones for personalised treatment. Sci Rep.
tions for HER2 status assessment in invasive 15 Lee S, Jung W, Hong SW, Koo JS. Evaluation 2016 Mar 21;6:23383.
breast cancer in France. Ann Pathol. 2021 of intratumoral HER-2 heterogeneity by fluo- 23 Marchio C, Dell’Orto P, Annaratone L, Geyer
Nov;41(6):507–20. rescence in situ hybridization in invasive FC, Venesio T, Berrino E, et al. The dilemma of
7 Baretton G, Dietel M, Gaiser T, Kirchner T, breast cancer: a single institution study. J Ko- HER2 double-equivocal breast carcinomas: ge-
Kreipe HH, Quaas A, et al. HER2 testing in rean Med Sci. 2011 Aug;26(8):1001–6. nomic profiling and implications for treatment.
gastric cancer : results of a meeting of German 16 Murthy SS, Sandhya DG, Ahmed F, Goud KI, Am J Surg Pathol. 2018 Sep;42(9):1190–200.
experts. Pathologe. 2016 Jul;37(4):361–6. Dayal M, Suseela K, et al. Assessment of 24 Press MF, Sauter G, Buyse M, Fourmanoir H,
8 Wolff AC, Hammond MEH, Allison KH, HER2/Neu status by fluorescence in situ hy- Quinaux E, Tsao-Wei DD, et al. HER2 gene
Harvey BE, Mangu PB, Bartlett JMS, et al. Hu- bridization in immunohistochemistry-equiv- amplification testing by fluorescent in situ hy-
man epidermal growth factor receptor 2 test- ocal cases of invasive ductal carcinoma and bridization (FISH): comparison of the ASCO-
ing in breast cancer: American Society of aberrant signal patterns: a study at a tertiary College of American pathologists guidelines
Clinical Oncology/College of American Pa- cancer center. Indian J Pathol Microbiol. 2011 with FISH scores used for enrollment in
thologists clinical practice guideline focused Jul–Sep;54(3):532–8. breast cancer international research group
update. J Clin Oncol. 2018 Jul 10; 36(20): 17 Ohlschlegel C, Zahel K, Kradolfer D, Hell M, clinical trials. J Clin Oncol. 2016 Oct 10;
2105–22. Jochum W. HER2 genetic heterogeneity in 34(29):3518–28.
Unusual HER2 Patterns Pathobiology 2022;89:278–296 293
DOI: 10.1159/00052422725 Lee HJ, Kim JY, Park SY, Park IA, Song IH, 37 Narayan P, Osgood CL, Singh H, Chiu HJ, 48 Modi S, Park H, Murthy RK, Iwata H, Tamu-
Yu JH, et al. Clinicopathologic significance of Ricks TK, Chiu Yuen Chow E, et al. FDA ap- ra K, Tsurutani J, et al. Antitumor activity and
the intratumoral heterogeneity of HER2 gene proval summary: fam-trastuzumab deruxte- safety of trastuzumab deruxtecan in patients
amplification in HER2-positive breast cancer can-Nxki for the treatment of unresectable or with HER2-low-expressing advanced breast
patients treated with adjuvant trastuzumab. metastatic HER2-positive breast cancer. Clin cancer: results from a phase Ib study. J Clin
Am J Clin Pathol. 2015 Oct;144(4):570–8. Cancer Res. 2021;27(16):4478. Oncol. 2020 Jun 10;38(17):1887–96.
26 Ng CK, Martelotto LG, Gauthier A, Wen HC, 38 Cortés J, Kim S, Chung W, Im S, Park YH, 49 Diéras V, Deluche E, Lusque A, et al. Trastu-
Piscuoglio S, Lim RS, et al. Intra-tumor ge- Hegg R, et al. LBA1 – trastuzumab deruxtecan zumab deruxtecan (T-DXd) for advanced
netic heterogeneity and alternative driver ge- (T-DXd) versus trastuzumab emtansine (T- breast cancer patients (ABC), regardless
netic alterations in breast cancers with hetero- DM1) in patients (Pts) with HER2+ metastat- HER2 status: a phase II study with biomarkers
geneous HER2 gene amplification. Genome ic breast cancer (mBC): results of the random- analysis (DAISY). San Antonio (TX): San An-
Biol. 2015 May 22;16:107. ized phase III DESTINY-Breast03 study. Ann tonio Breast Cancer Symposium; 2021.
27 Filho OM, Viale G, Stein S, Trippa L, Yardley Oncol. 2021;32:63. 50 Aurilio G, Disalvatore D, Pruneri G, Bagnardi
DA, Mayer IA, et al. Impact of HER2 hetero- 39 ENHERTU® (fam-trastuzumab deruxtecan- V, Viale G, Curigliano G, et al. A meta-analy-
geneity on treatment response of early-stage nxki) granted breakthrough therapy designa- sis of oestrogen receptor, progesterone recep-
HER2-positive breast cancer: phase II neoad- tion in US for patients with HER2-positive tor and human epidermal growth factor re-
juvant clinical trial of T-DM1 combined with metastatic breast cancer treated with one or ceptor 2 discordance between primary breast
pertuzumab. Cancer Discov. 2021; 11(10): more prior anti-HER2-based regimens. 2021 cancer and metastases. Eur J Cancer. 2014 Jan;
2474. Oct 4. 50(2):277–89.
28 Qaiser T, Mukherjee A, Reddy Pb C, Munugo- 40 Tarantino P, Hamilton E, Tolaney SM, Cortes 51 Schrijver WAME, Suijkerbuijk KPM, van Gils
ti SD, Tallam V, Pitkaaho T, et al. HER2 chal- J, Morganti S, Ferraro E, et al. HER2-low CH, van der Wall E, Moelans CB, van Diest
lenge contest: a detailed assessment of auto- breast cancer: pathological and clinical land- PJ. Receptor conversion in distant breast can-
mated HER2 scoring algorithms in whole scape. J Clin Oncol. 2020 Jun 10;38(17):1951– cer metastases: a systematic review and meta-
slide images of breast cancer tissues. Histopa- 62. analysis. J Natl Cancer Inst. 2018 Jun 1;110(6):
thology. 2018 Jan;72(2):227–38. 41 Modi S, Tsurutani J, Tamura K, Park H, Sag- 568–80.
29 Bui MM, Riben MW, Allison KH, Chlipala E, ara Y, Murthy R, et al. Abstract P6-17-02: 52 Chen R, Qarmali M, Siegal GP, Wei S. Recep-
Colasacco C, Kahn AG, et al. Quantitative im- trastuzumab deruxtecan (DS-8201a) in sub- tor conversion in metastatic breast cancer:
age analysis of human epidermal growth fac- jects with HER2-low expressing breast can- analysis of 390 cases from a single institution.
tor receptor 2 immunohistochemistry for cer: updated results of a large phase 1 study. Mod Pathol. 2020 Dec;33(12):2499–506.
breast cancer: guideline from the college of Cancer Res. 2019;79(4 Supplement):P6–1702. 53 Grinda T, Joyon N, Lusque A, Lefevre S, Ar-
American pathologists. Arch Pathol Lab Med. 42 Saura Manich C, O’Shaughnessy J, Aftimos nould L, Penault-Llorca F, et al. Phenotypic
2019 Oct;143(10):1180–95. PG, van den Tweel E, Oesterholt M, Escrivá- discordance between primary and metastatic
30 Helin HO, Tuominen VJ, Ylinen O, Helin HJ, de-Romaní SI, et al. LBA15 – primary out- breast cancer in the large-scale real-life multi-
Isola J. Free digital image analysis software come of the phase III SYD985.002/TULIP center French ESME cohort. NPJ Breast Can-
helps to resolve equivocal scores in HER2 im- trial comparing [vic-] trastuzumab duo- cer. 2021 Apr 16;7(1):41.
munohistochemistry. Virchows Arch. 2016 carmazine to physician’s choice treatment in 54 Mittendorf EA, Wu Y, Scaltriti M, Meric-Ber-
Feb;468(2):191–8. patients with pre-treated HER2-positive lo- nstam F, Hunt KK, Dawood S, et al. Loss of
31 Yousif M, van Diest PJ, Laurinavicius A, cally advanced or metastatic breast cancer. HER2 amplification following trastuzumab-
Rimm D, van der Laak J, Madabhushi A, et al. Ann Oncol. 2021;32. based neoadjuvant systemic therapy and sur-
Artificial intelligence applied to breast pathol- 43 Banerji U, van Herpen CML, Saura C, Thistle- vival outcomes. Clin Cancer Res. 2009 Dec 1;
ogy. Virchows Arch. 2021 Nov 18. thwaite F, Lord S, Moreno V, et al. Trastu- 15(23):7381–8.
32 Yue M, Zhang J, Wang X, Yan K, Cai L, Tian zumab duocarmazine in locally advanced and 55 Guarneri V, Dieci MV, Barbieri E, Piacentini
K, et al. Can AI-assisted microscope facilitate metastatic solid tumours and HER2-express- F, Omarini C, Ficarra G, et al. Loss of HER2
breast HER2 interpretation? A multi-institu- ing breast cancer: a phase 1 dose-escalation positivity and prognosis after neoadjuvant
tional ring study. Virchows Arch. 2021 Sep; and dose-expansion study. Lancet Oncol. therapy in HER2-positive breast cancer pa-
479(3):443–9. 2019 Aug;20(8):1124–35. tients. Ann Oncol. 2013 Dec;24(12):2990–4.
33 Wedam S, Fashoyin-Aje L, Gao X, Bloomquist 44 Miglietta F, Griguolo G, Bottosso M, Giar- 56 Niikura N, Tomotaki A, Miyata H, Iwamoto
E, Tang S, Sridhara R, et al. FDA approval ratano T, Lo Mele M, Fassan M, et al. Evolu- T, Kawai M, Anan K, et al. Changes in tumor
summary: ado-Trastuzumab emtansine for tion of HER2-low expression from primary to expression of HER2 and hormone receptors
the adjuvant treatment of HER2-positive ear- recurrent breast cancer. NPJ Breast Cancer. status after neoadjuvant chemotherapy in
ly breast cancer. Clin Cancer Res. 2020 Aug 2021 Oct 12;7(1):137. 21,755 patients from the Japanese breast can-
15;26(16):4180–5. 45 Schettini F, Chic N, Braso-Maristany F, Pare cer registry. Ann Oncol. 2016 Mar;27(3):480–
34 Delgado J, Vleminckx C, Sarac S, Sosa A, L, Pascual T, Conte B, et al. Clinical, patho- 7.
Bergh J, Giuliani R, et al. The EMA review of logical, and PAM50 gene expression features 57 Wang RX, Chen S, Jin X, Chen CM, Shao ZM.
trastuzumab emtansine (T-DM1) for the ad- of HER2-low breast cancer. NPJ Breast Can- Weekly paclitaxel plus carboplatin with or
juvant treatment of adult patients with HER2- cer. 2021 Jan 4;7(1):1. without trastuzumab as neoadjuvant chemo-
positive early breast cancer. ESMO Open. 46 Agostinetto E, Rediti M, Fimereli D, Debien therapy for HER2-positive breast cancer: loss
2021 Apr;6(2):100074. V, Piccart M, Aftimos P, et al. HER2-low of HER2 amplification and its impact on re-
35 Modi S, Saura C, Yamashita T, Park YH, Kim breast cancer: molecular characteristics and sponse and prognosis. Breast Cancer Res
SB, Tamura K, et al. Trastuzumab deruxtecan prognosis. Cancers. 2021 Jun 5;13(11):2824. Treat. 2017 Jan;161(2):259–67.
in previously treated HER2-positive breast 47 Denkert C, Seither F, Schneeweiss A, Link T, 58 Branco FP, Machado D, Silva FF, Andre S, Ca-
cancer. N Engl J Med. 2020 Feb 13; 382(7): Blohmer JU, Just M, et al. Clinical and mo- tarino A, Madureira R, et al. Loss of HER2 and
610–21. lecular characteristics of HER2-low-positive disease prognosis after neoadjuvant treat-
36 Agency EM. Enhertu summary of product breast cancer: pooled analysis of individual ment of HER2+ breast cancer. Am J Transl
characteristics; 2021. patient data from four prospective, neoadju- Res. 2019;11(9):6110–6.
vant clinical trials. Lancet Oncol. 2021 Aug;
22(8):1151–61.
294 Pathobiology 2022;89:278–296 Grassini/Cascardi/Sarotto/Annaratone/
DOI: 10.1159/000524227 Sapino/Berrino/MarchiòYou can also read