Lymphoedème du membre supérieur après cancer du sein - S. Vignes Unité de Lymphologie, Hôpital Cognacq-Jay, Paris - Centre des Maladies du Sein
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Lymphœdème du membre supérieur
après cancer du sein
S. Vignes
Unité de Lymphologie, Hôpital
Cognacq-Jay, Paris
Lymphœdème (LO)
• Lymphe : système //
veines,…
•Lymphœdèmes
– 140 millions de
personnes dans le
monde (filariose)
– MS (K sein), MI
(primitif, K col
utérin)
• Forme secondaire en
France +++
Karpanen T & Alitalo K. Annu Rev Pathol 2008;3:367
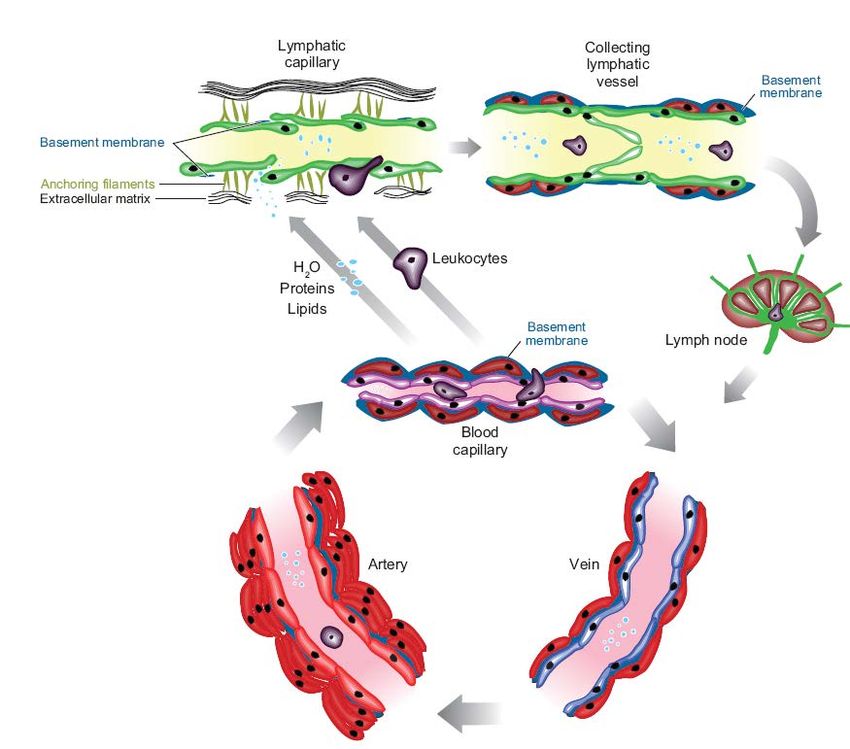
Physiopathologie du lymphœdème Szuba A & Rockson S. Vasc Med 1997;2:321
associated with a marked mononuclear
Mouse-Tail Model were similarly
cell inflammatory
fixed and decalcified
respons
but were
Regulation
RegulationofofAdipogenesis
We usedincrease
Adipogenesis bybyLymphatic
in CD45
Lymphatic Fluid
described cells;
mouse-ptail " 0.001). InOptimum
addition, theTemperature
authors not
#
our previously bedded in Cutting me
nificant
model to examine increase
the effects of lymphatic Fluid
in the number
fluid stasis of monocytes/macrophages
(Tissue-Tek, Hatfield, Pa.) and sectioned as atiden
8 to
Stasis: Part
Stasis: PartI.I.Adipogenesis,
n adipogenesis,
F4/80 Fibrosis,
Adipogenesis, Fibrosis,
fibrosis, and inflammation.
immunohistochemistry
Briefly, to disrupt superficial lymphatic vessels, we
6 –9
!m"for0.001).
(p fresh frozen analysis.
Hematoxylin and eosin staining and trichro
Conclusions: The mouse-tail model haswerepathologic findings
standardthat ar
andand
Inflammation
Inflammation
xcised a 2-mm, full-thickness, circumferential
egment of to skinclinical
from the lymphedema,
midportion (20including mm
staining
Oil fat
red O
performed using
deposition, fibrosis,onand
staining was performed
techniqu
inflam
frozen secti
rom the base Adipogenesis
Jamie of the tail)
C. Zampell,
Jamie C. Zampell, M.D.
M.D.of in
8- toresponse
10-week-old to lymphatic
to visualize lipid fluid stasisBriefly,
droplets. closely
Background: Although fat deposition is a defining clinical characteristic of
frozenresem
section
emale C57BL/6 process mice
Seth (n ! 20;
Aschen
in obesity. Jackson
Background:
This
lymphedema, Labora-
Although
model
the slides
cellular fat
thereforewere
deposition
mechanisms thatair adried
isregulate
defining
provides and
this submerged
clinical
an
response un-in a
characteristic
excellent
remain me0.
Seth Aschen
ory, Bar Harbor, Me.). Using
Evan S. Weitman, a known.
dissecting
M.D. lymphedema, micro-
theofcellular
The goals solution
mechanisms
this two-part of to
study were oil
that red Othe
regulate
determine inthispropylene
response
effect glycolu
remain
of lymphatic
Evan S.which
Weitman,
Alan to study
M.D.
Yan, M.D. the molecular mechanisms that regulate the pathoph
cope (StereoZoom SZ-4; Leica, fluidWetzlar,
known. Theon
stasis goalsGer- lowed
of this two-part
adipogenesis by washes
study
and inflammation toin
were(part graded
determine
I) and howthe propylene
effect
these glycol
of lymphat
changes
AlanElhadad,
Sonia Yan, M.D. Ph.D. fluid
ofElhadad,
lymphedema.
many), we identified
SoniaMarina
and M.D.
De Brot,
Ph.D.
ligated deep (Plast.
stasis
regulate Reconstr.lutions,
on adipogenesis
the temporal
collecting and Surg.
spatial 129:counterstained
and inflammation
expression
and 825,(part
of fat2012.)
I) andwithhow these
differentiation genes
Harrischang
hem
(part
regulate II).
the temporal
ymphatics Babak
adjacent to the
J. Mehrara, lateral
M.D. tail veins (Fig. and spatial
toxylin expression
(Dako, of fat differentiation
Carpinteria, Calif.). Analysis gen
Marina De Brot, M.D. Methods: Adult female mice underwent tail lymphatic ablation and were
(part II).
Babak J. Mehrara, M.D.
New York, N.Y. euthanized 6 weeks after surgery (n ! 20). Fat deposition, fibrosis, and
Methods: Adult female mice underwent tail lymphatic ablation and we
inflammation were then analyzed in the regions of the tail exposed to
New York, N.Y. euthanized
lymphatic fluid 6 weeks
stasis asafter surgery
compared with (nnormal
! 20). Fat deposition,
lymphatic flow. fibrosis, an
a chronic disorder that, inLymphatic
inflammation
Results: alsofluid
were asstasis
then aanalyzed
persistent in resulted
in the tail reminder
the regions of
tail cancer
of thesubcutane-
in significant exposed
lymphatic fluid stasis
ous fat deposition, withas acompared
2-fold increase withinnormal lymphatic
fat thickness (p " flow.
0.01). In
es, develops most commonly with associated
stasis was associated psychological
Results: Lymphatic fluid stasis in the tail resulted in significantand
addition, lymphatic with subcutaneous fat morbidity
fibrosis subcutan
he lymphatic system during collagen deposition.
ous fat deposition, with Development
Adipogenesis in response
a 2-fold increase ofintargeted
to fat thicknesstreatments
lymphatic
associated with a marked mononuclear cell inflammatory response (5-fold
fluid stasis was
(p " 0.01). I
reatment.1,2 Remarkably, addition,
it is lymphatic stasis was associated with subcutaneous fatafibrosis an
increase
collagen
in CD45 prevent
deposition.
#
cells; p "or treat
0.001). In lymphedema
addition, the authors has notedbeen sig- ham
nificant increase in theAdipogenesis in response to lymphatic
number of monocytes/macrophages fluidbystasis w
as identified
ny as 50 percent of patients associated with the
a marked
F4/80 immunohistochemistry lackmononuclear
of" 0.001).
(p animal models. This
cell inflammatory response defic
(5-fo
node dissection will go
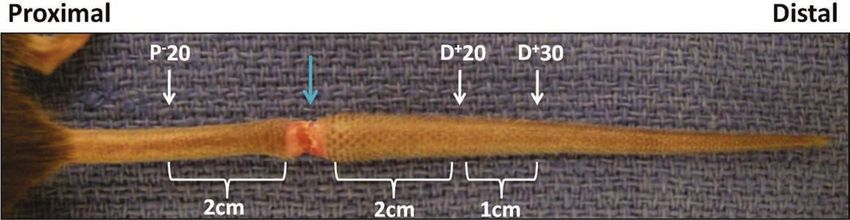
Fig. 1. Mouse-tail model
on
increase to
Conclusions:
of
in CD45
lymphatic
to clinical
served
The
fluid
#
cells; as
mouse-tail
stasis.
lymphedema,
p " a
modelsignificant
0.001).
Representative
In addition,
has pathologic
photomicrograph barrier
thethat
findings
of a mousefor
authors elucidat
noted a si
are similar
tail
nificant increase in theincluding
numberfat ofdeposition, fibrosis, and inflammation.
monocytes/macrophages as identified b
a.3 However, 6 weeksdespite the
after lymphatic fact
Adipogenesis
ligation. The molecular (p
in
wound
F4/80 immunohistochemistry response
is to
marked bymechanisms
lymphatic
the bluefluid
arrow.
" 0.001). stasis
Tissues that regulate
closely
are resembles
harvested this the
common, proximal
treatment
or distal toremains
the process
zone in obesity.
of lymphatic
Conclusions:
which to study the
The This model
lymphedema.
obstruction
mouse-tail therefore
6 weeks
As
afterhas
model providesP"an
a result,
surgery.
pathologic 20,excellent
it
20 findings
# molecular mechanisms that regulate the pathophysiology
means with
remains
mm proximal that areunkn
simil
to the zone of lymphatictoofclinical
obstruction;lymphedema,
D 20, 20 mm including Surg.fat
distal to the deposition,
zone
2012.)fibrosis,
of lymphatic and inflammatio
obstruction;
nd is designed# primarily to
lymphedema.
D 30, 30 mm distal toAdipogenesis
the zone of lymphatic lymphatic to lymphatic fluid stasis closely clinical
(Plast. Reconstr.
in response
obstruction. injury 129: results
825, in the resembles fi th
ession rather than to achieve process in obesity. fat This
deposition,
model therefore chronicprovides inflammation,
an excellent meansan wit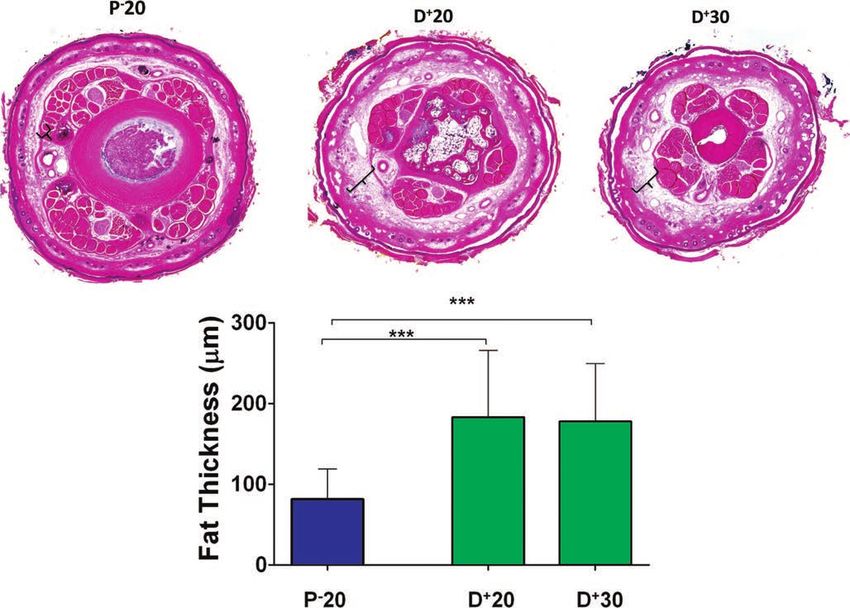
Plastic and Reconstructive Surgery • April 2012 Fig. 2. Lymph stasis increases subcutaneous fat deposition. (Above) Representative low-power mouse-tail cross-sections obtained 20 mm proximal (P!20) or 20 (D"20) or 30 mm distal (D"30) to the wound (hematoxylin and eosin; original magnification, #2.5). Note the marked deposition of subcutaneous fat in the distal sections (brackets). (Below) Quantification of fat thickness in the prox- imal and distal regions of the mouse tail 6 weeks after surgery. Note significant increases in fat thickness in the distal regions as designated by brackets (***p $ 0.001).
Lymphœdème MS après cancer du sein • Curage axillaire – fréquence lymphœdème :19% – ganglion sentinelle : 5,6% • Radiothérapie même si ne comprenant pas le creux axillaire • Obésité lors du cancer du sein (IMC > 30 kg/m2), risque ! 4 • Survenue post-chirurgie voire des années après… (médiane : 2 ans) DiSipio T et al. Lancet 2013;14:500
204 ESTIMATIONS NATIONALES DE LÌ INCIDENCE ET DE LA MORTALITÖ PAR CANCER EN FRANCE MÖ TROPOLITAINE ENTRE 1990 ET 2018
VOLUME 1 : TUMEURS SOLIDES / SEIN
Lymphœdème après cancer du sein
Tendances de lÌ incidence et de la mortalit» en France m» tropolitaine entre 1990 et 2018
• 58500 nx cas de cancer en 2018
Tendances tous Ç ges
TABLEAU 4 | Nombre de cas et d» cÀ s en France selon lÌ ann» e Sein
Ann» e
1990 1995 2000 2005 2010 2015 2018
INCIDENCE
Femme 29 970 34 835 41 882 48 468 50 755 55 698 58 459
MORTALITÖ
Femme 10 172 10 774 10 999 11 290 11 637 12 025 12 146
MORTALITÖ OBSERVÖ E
Femme 10 141 10 753 10 950 11 308 11 750 12 229
• Fréquence du LO après traitement
TABLEAU 5
Sein
| Taux dÌ incidence et de mortalit» en France selon lÌ ann» e (taux standardis» s monde)
– 13-28% après curage axillaire
Ann» e Variation Annuelle Moyenne (%)
De 1990 De 2010
1990 1995 2000 2005 2010 2015 2018 á 2018 á 20 18
– définitions différentes
INCIDENCE
Femme 72,8 79,8 90,7 97,0 95,2 98,0 99,9 1,1 [1,0 ; 1,2] 0,6 [0,3 ; 0,9]
MORTALITÖ
Femme 20,2 20,0 18,8 17,4 16,0 14,7 14,0 1,3 [ 1,4 ; 1,2] 1,6 [ 1,8 ; 1,4]
! 2 cm
MORTALITÖ OBSERVÖ E
Femme 20,1 19,9 18,7 17,4 16,1 14,8
! +10%
FIGURE 2 | Taux dÌ incidence et de mortalit» en France selon lÌ ann» e (taux standardis» s monde TSM)
Ö chelle logarithmique Sein
Armer J et al. Lymph Res Biol 2005;3:208
DiSipio T et al. Lancet 2013;14:500
Femme
https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Rapport-Volume-1-Tumeurs-solides-Estimations-
100
nationales-de-l-incidence-et-de-la-mortalite-par-cancer-en-France-metropolitaine-entre-1990-et-2018-juillet-2019
0
g
DOI: 10.1097/RLI.0000000000000386 sumptions about x-ray attenuation and impedance properties and
554 www.investigativeradiology.com Investigative Radiology • Volume 52, Number 9, September 2017
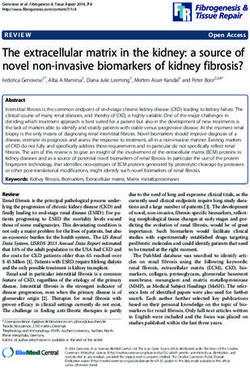
Magnetic Resonance Imaging–Based Assessment of Breast
Cancer–Related Lymphoedema Tissue Composition
Marco Borri, MPhys,* Kristiana D. Gordon, MD,†‡ Julie C. Hughes, BSc,* Erica D. Scurr, BSc,*
Dow-Mu Koh, MD, MRCP, FRCR,* Martin O. Leach, PhD, FMedSci, FInstP, FIPEM, FRSB,*
Peter S. Mortimer, MD, FRCP,†‡ and Maria A. Schmidt, PhD*
volumes, fluid accumulated prevalently around the elbow, with substantial involve-
Objectives: The aim of this study was to propose a magnetic resonance imaging
• LO MS : 15-20%
ment of the upper arm in only 3 cases. Fat excess volume was generally greater in
acquisition and analysis protocol that uses image segmentation to measure and
the upper arm; however, the relative increase in epifascial volume, which considers
depict fluid, fat, and muscle volumes in breast cancer–related lymphoedema
the total swelling relative to the original size of the arm, was in 9 cases maximal
(BCRL). This study also aims to compare affected and control (unaffected) arms
within the forearm.
of patients with diagnosed BCRL, providing an analysis of both the volume and
Conclusions: Our measurements indicate that excess of fat within the epifascial
• Stase lymphatique → modifications
the distribution of the different tissue components.
layer was the main contributor to the swelling, even when a substantial accumu-
Materials and Methods: The entire arm was imaged with a fluid-sensitive STIR
lation of fluid was present. The proposed approach could be used to monitor how
and a 2-point 3-dimensional T1W gradient-echo–based Dixon sequences, acquired
the internal components of BCRL evolve after presentation, to stratify patients for
in sagittal orientation and covering the same imaging volume. An automated image
treatment, and to objectively assess treatment response. This methodology pro-
postprocessing procedure was developed to simultaneously (1) contour the external
tissulaires, fibrose collagène,
vides quantitative metrics not currently available during the standard clinical as-
volume of the arm and the muscle fascia, allowing separation of the epifacial and
sessment of BCRL and shows potential for implementation in clinical practice.
subfascial volumes; and to (2) separate the voxels belonging to the muscle, fat,
and fluid components. The total, subfascial, epifascial, muscle (subfascial), fluid Key Words: breast cancer–related lymphoedema, tissue composition analysis,
(epifascial), and fat (epifascial) volumes were measured in 13 patients with uni- image segmentation, magnetic resonance imaging
accumulation de Btissu adipeux
lateral BCRL. Affected versus unaffected volumes were compared using a
(Invest Radiol 2017;00: 00–00)
2-tailed paired t test; a value of P < 0.05 was considered to be significant. Pearson
correlation was used to investigate the linear relationship between fat and fluid
reast cancer–related lymphoedema (BCRL) is a chronic swelling of
excess volumes. The distribution of fluid, fat, and epifascial excess volumes
the arm, which develops in approximately 20% of women after
Lymphœdème : 3 composantes,
(affected minus unaffected) along the arm was also evaluated using dedicated
breast cancer treatment.1 A defining characteristic of BCRL is the accu-
tissue composition maps.
mulation of both interstitial fluid and fat within the arm, which causes
Results: Total arm, epifascial, epifascial fluid, and epifascial fat volumes were
both physical and psychological morbidity.2 The buildup of protein-
significantly different (P < 0.0005), with greater volume in the affected arms.
rich fluid in the interstitium (edema) is caused by impaired lymphatic
The increase in epifascial volume (globally, 94% of the excess volume) consti-
liquidienne (la lymphe), collagène,
transport. However, the mechanisms leading to the abnormal deposition
tuted the bulk of the lymphoedematous swelling, with fat comprising the main
of fat are not fully understood and the links between the lymphatic
component. The total fat excess volume summed over all patients was 2.1 times
system and adiposity are still under investigation.3 Adipose tissue hy-
that of fluid. Furthermore, fat and fluid excess volumes were linearly correlated
pertrophy is likely to be promoted by the inflammatory response trig-
(Pearson r = 0.75), with the fat excess volume being greater than the fluid in
gered by the chronic lymph stasis.4 Furthermore, it has been
adipeuse
11 subjects. Differences in muscle compartment volume between affected and
hypothesized that the lymph itself might contain factors that stimulate
unaffected arms were not statistically significant, and contributed only 6% to
fat cell differentiation and growth.5 The ratio of fat and fluid varies
the total excess volume. Considering the distribution of the different tissue excess
greatly between lymphoedematous arms, yet first-line treatment for
BCRL addresses only the fluid, not the fat. Compression and drainage
Received for publication January 26, 2017; and accepted for publication, after revision, massage attempt to reduce the excess volume by enhancing fluid
April 4, 2017. clearance.6 For chronic lymphoedema, liposuction is proposed as a
From the *Cancer Research UK Cancer Imaging Centre, The Royal Marsden NHS
Foundation Trust and The Institute of Cancer Research; †Cardiac and Vascular
possible intervention.7
Sciences, St George's University of London; and ‡Skin Unit, The Royal Marsden Quantification of the volume, spatial distribution, and preva-
NHS Foundation Trust, London, United Kingdom. lence of the different lymphoedematous tissue components could
Conflicts of interest and sources of funding: The authors acknowledge the support of greatly improve patient selection for optimal treatment. However, stan-
the Cancer Research UK and the Engineering and Physical Sciences Research
Council Cancer Imaging Centre in association with the Medical Research Council
dard assessment of lymphoedema is currently limited to a measurement
and Department of Health (England) (grants C1060/A10334, C1090/A16464); the of the size of the affected arm relative to the unaffected arm performed
isolates the fat component, the Dixon water image contains the muscle Longitudinal Volume Plot
ps of and the other tissues, and the STIR image selectively depicts the fluid
This Cumulative tissue volumes are plotted along the length of the
(step 2, Fig. 1). The segmentation process is applied to the combined arm (Fig. 2). Different colors are assigned to different tissue components:
ualize images, and as a result, muscle, fat, and fluid voxels belong to 3 distinct
asure clusters (red, yellow, and blue clusters in Fig. 1). The k-mean algorithm
d and is initialized with k = 5 and assigns to the 2 additional clusters:
(1) voxels contributing no signal (image noise, gray cluster) and
(2) voxels with mixed composition at the tissue interfaces, including
connective or fibrotic tissue (white cluster).
3. Volume Extraction
The program scrolls through each slice and creates 2 separate masks,
containing the entire cross-section of the arm (noise excluded) and
uired the muscle, respectively. Erosion/dilation and triangulation algo-
n sep- rithms from the IDL library are then used to automatically extract
he pa- the external and fascial contours from the masks.17 The muscle and
g the the other subfascial tissue components are contained within the fas-
g the cial contour. Subfacial and total arm volumes are encompassed by
gainst the fascial and external contours, respectively, whereas the volume
main- between the 2 contours represents the epifascial volume.
e sur- Clinical Measurements
ative
fromRadiology • Volume 52, Number 9, September 2017 MRI for Lymphoedema Tissue Composition
with a Subjects
. The Both the affected and the unaffected arms of 13 patients with di-
agnosed unilateral arm lymphoedema after breast cancer treatment were
measured with this technique. All patients were adult women who gave
rsion- written informed consent as part of a prospective study approved by the
onds, National Research Ethics Service. Patient demographics and relevant
sition clinical data are reported in Table 1, specifying the arm affected by
lymphoedema and the arm predominantly used (dominant).
ence
Volume Measurement
grees,
onds). Muscle, fat, and fluid subvolumes can be computed by counting
the respective number of voxels (1 voxel = 1 mm3 = 0.001 mL) within
the volumes segmented with the image postprocessing procedure. The
lume
ingle FIGURE 1. following volumes
Step 1: Color were extracted:
representation total arm, Dixon
of the overlapped subfascial,
waterepifascial,
muscle (subfascial), fluid (epifascial), and fat
(red), Dixon fat (green), and STIR (blue) images. The sagittal (epifascial).
were (longitudinal) view displays the portion of the arm included in the
econ- FIGURE 2. Longitudinal plots of the different tissue volumes within the
Volumethe
analysis—between Visualization
wrist and the 65% mark (65% of the distance affected and unaffected arms of an example patient (patient 10):
d. between the elbowThree and the shoulder
different tip). The
graphical transversal (cross-sectional)
representations (Figs. 2, 3) are used to muscle (red), epifascial fat (yellow), epifascial fluid (blue), and total
view shows visualize
how different tissue components
the distribution (muscle,
of the tissue fat, and within
components fluid) arethe arm: (external, green line).
separated into different images (red, green, and blue images, respectively)
3.IDL on aofrepresentative
Intensity maps normalized tissueslice.
excessStep 2: Separated
volumes in an exampleDixon fat,(patient
patient Dixon10).water, andshows longitudinal intensity maps of the
A, Image
onThis STIR 556
transversal www.investigativeradiology.com
images, and segmentation map of a representative
of tissue excess along the arm for the 3 tissue components. For fluid and fat, the excess volume is measured as the difference between© 2017 Wolters Kluwer Health, Inc. All rights reserved.
slice.
and unaffected
ydicate The k-means
volumes, algorithm
whereas (k =
the epifascial 5) is used
increase to segment
is measured as thethe arm
differencevolume.
in volumeStep
as a 3:
percentage of the unaffected volume. Darker
per-greater values and are normalized to the peak values of each measure—for this patient, the peak values are 60 mL (fluid), 90 mL (fat), and
Fascial and external contours on a representative slice. These encompass,
d the increase).
pifascial B, Image shows the radial intensity map, which gives the distribution of fluid excess in different segments within the epifascial
summed overrespectively,
ascia) the longitudinalthe subfacial
extent andThe
of the arm. total arm volumes.
external The epifascial
segments represent the layervolume
below the skin, the internal segments the layermay assume others are assessing and addressing less press- Patients with less rigid or shorter cords may have minimal
ing physical symptoms such as AWS. The purpose of this cord tension and minimal symptoms until they approach full
article is to describe the signs and symptoms, diagnosis and extension and abduction. In our experience, they frequently
Autres FDR lymphœdème MS
management, and potential complications of AWS.
?@-)%'$).'%170% of cords are palpable, with the implication being that
the remainder were only visible.13 If the arm is straightened at
• Taxanes en adjuvant
the elbow and then abducted adequately essentially all cords
are palpable and many are visible as a linear “tenting” or “fur-
1%2"*3'/'AB@>>$"1'8#C'%1).":>$9
rowing” of the skin. When the arm is not in the “straightened” 4)&35'EF>&@0>#'*:".%'$"#';@%@C>#'@)'&/#'Breast surgery \0.0001
Original article
rates of BCRL have been decreasing. Patients und
Lumpectomy 854 (76 %)
207 (64 %) 647 (81 %)
sentinel lymph node biopsy (SLNB) have signi
Risk factors for lymphoedema Mastectomy in women with breast cancer: A267 large
(24 %) 117 (36 %) 150 (19 %)
lower rates of BCRL than those undergoing axillary
prospective cohort * Axillary surgery \0.0001
NoneThe Breast 28 (2016) 29e36 Taxanes164 and(14breast
%)
node dissection (ALND). The rate of BCRL in p
cancer-related
0 (0 %) lymphoedema
164 (21 %)
undergoing SLNB has been quoted as being as low
Chimiothérapie
S.L. Kilbreath a, *, K.M. Refshauge a
Sentinel, eJ.M. Beith b
node ,biopsy
L.C. Ward a, c d
(SLNB) , O.A. Ung , E.S. Dylke
a
, %)
per cent3 – 5 . However, ALND is the surgical proce
e a
lymph
,1 a, 1
738 (66 165 (51 %) 573 (72 %)
J.R. French , J. Yee , L. Koelmeyer , K. Gaitatzis Original article219 (20 %)
al. / The BreastFaculty
28 (2016) Axillary lymph
29e36 Contents lists available at ScienceDirect node dissection (ALND) 159 (49 %) 60 (8 %)
a
of Health Sciences, University of Sydney, Sydney, Australia choice for patients with metastasis to axillary lymph
b Tumor type
Chris O'Brien Lifehouse, Camperdown, Australia \0.0001
c
d
School of Chemistry and Molecular Biosciences, The University of Queensland, Brisbane, Australia
Invasive Carcinoma Adjuvant
Table 3 925 Multivariable
(83 %) and Cox
taxanes the proportional
320development
(99 %) hazards
of (76
605 %)age-adjusted
breast cancer-related T
Royal Brisbane and Women's Hospital, School of Medicine, The University of Queensland, Brisbane, Australia
e
The Breast
Westmead Breast Cancer Institute, Westmead Hospital, Westmead, Australia
Ductal Carcinoma in Situ (DCIS) arm lymphoedema
analysis of (17
196 risk%)of breast©cancer-related
2015 %) Society Ltdlymphoedema
4 (1 BJS 192 (24 %)
Published by John Wiley & Sons Ltd
by a
Pathologic characteristics chemotherapy status among women who underwent axillary
M. Cariati1,3 , S. K. Bains1 , M. R. Grootendorst1 , A. Suyoi3 , A. M. Peters5 , P. Mortimer4 , P. Ellis1,3 ,
c
a r t i c l e i n f o a binvasive c t size, cm!
s t r atumor M. lymph
Harries1,3node
Median ,1.4
M. Vandissection
Hemelrijck2 and1.9
(0.05–12.5) A. D. Purushotham1,3 1.1 (0.05–10.5)
(0.2–12.5) \0.0001 w
Article history:
j o u r n a l h oMedian
m eApprospective
a g e : lymph
number www . e ldissected
nodes
study was
sev
conducted
i e r . c o mSection
/atbincreased
rofsResearch
to identify womenDirectorate
t risk 1
2Oncology,
(0–43)
3for lymphoedema (LE) based
2
and School of Medicine, Cancer
6 on Epidemiology Group, Division1
(1–43) of (0–26) \0.0001
Cancer Studies, King’s College London,
4
of Haematology and Oncology, Guy’s and St Thomas’ NHS Foundation Trust, and Department of Clinical Sciences, St George’s,
Received 19 December 2015
Medianaxillary
numbersurgery. Assessment
positive lymph occurred
nodesprior to surgery, within
University 4 weeks,
of London, andand
0 London,
(0–39) at5 Department
6, 12 andof18 months
Nuclear1Medicine, Hazard
(0–39)Brighton and Sussex ratio
0 (0–26)
University \0.0001
Hospitals NHS Trust, Brighton, UK
Received in revised form following surgery. Following post-surgery assessment, women were asked to Purushotham,
complete weekly diaries
Correspondence to: Professor A. D. Department of Research Oncology, King’s College London, 3rd Floor Bermondsey Wing, Guy’s
18 April 2016
Accepted 24 April 2016
Radiation therapy
regarding events that occurred in the previous week. RiskLondon
Hospital, factors SE1were
9RT, UKgrouped into demographic,
Model 1
(e-mail: ea-purushotham@kcl.ac.uk)
Model 2 Model 3 \0.0001
Available online 13 May 2016
lifestyle, breast cancer treatment-related, arm swelling-related, and post-surgical activities. Bio-
None impedance spectroscopy thresholds were used to determine 216 (19
Despite
%)
affecting
presence of LE. At 18-months, 241 women
Background:
40
approximately
(12 %)
one-quarter of all
176
patients
(22 %)
undergoing axillary lymph
with
PartialBreast reconstruction and risk of arm
lymphedema development: A meta-analysis
Charalampos Siotos a, Mohamad E. Sebai b, Eric L. Wan a,
Ricardo J. Bello a, Mehran Habibi b, Damon S. Cooney a,
Michele A. Manahan a, Carisa M. Cooney a, Stella M. Seal c, ARTICLE
Gedge D. Rosson a,* Journal
ARTICLE INReconstructive
of Plastic, PRESS & Aesthetic Surgery (2018) ■■, ■
8 C. Siotos et al.
a
Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, 601 N. Caroline Street,
Baltimore, MD, USA
b
Department of Surgery, Johns Hopkins Hospital, 4940 Eastern Avenue, Baltimore, MD, USA
c
Welch Medical Library, Johns Hopkins University, 1900 E. Monument Street, Baltimore, MD, USA
Received 26 September 2017; accepted 21 January 2018
KEYWORDS Summary Background: Lymphedema remains a significant complication
Breast cancer; cancer surgery when there is axillary lymph node intervention. Previous systema
Breast identified risk factors for breast cancer-related lymphedema, including increa
reconstruction; Review
of lymph nodes dissected and radiotherapy. However, they have not examin
Lymphedema;
breast reconstruction on lymphedema occurrence. In this systematic review an
Breast reconstruction and
Upper-extremity
wereceiving
Figure 4 Forest plot analysis of patients soughttotal
to mastectomy
evaluate and
thebreast
association between
reconstruction breast
versus total reconstruction
mastectomy only and (BR) and
lymphedema;
lymphedema incidence (exclusion of breast conserving cases).
Meta-analysis Methods: We searched PubMed (1966–2016), Embase (1966–2016), Scopus (
Google Scholar (2004–2016) for studies involving breast reconstruction and
lymphedema or breast cancer-related lymphedema. Our primary outcome wBreast Cancer Res Treat 2015;154:455-61 1955 1962 1998 2006 2009 2010 2005
cohort of patients treated for breast cancer and screened for lymphedema.
, Patients and Methods
Between 2005 and 2014, patients undergoing treatment of breast cancer at our institution were
Impact of Ipsilateral
screened prospectively for lymphedema. Blood Draws,
Bilateral arm Injections,
volume measurements Blood Pressure were performed
e
, Measurements,
preoperatively and postoperatively andusing
Air aTravel on the
Perometer. Risk
At each of Lymphedema
measurement, for the
patients reported
number ofPatients
blood draws, injections,
Treated for blood
Breast pressure
Cancer measurements, trauma to the at-risk arm(s),
and number of flights taken since their last measurement. Arm volume was quantified using the
Chantal M. Ferguson, Meyha N. Swaroop, Nora Horick, Melissa N. Skolny, Cynthia L. Miller, Lauren S. Jammallo,
relative volume changeJean
Cheryl Brunelle, andA.weight-adjusted change
O’Toole, Laura Salama, Michelle formulas. Linear
C. Specht, and random
Alphonse G. Taghianeffects models were
used to assess the association between relative arm volume (as a continuous variable) and non-
f
treatment risk factors, as well as clinical
chusetts General
A characteristics.
B S T R A C T
edical School, Boston,
Results Purpose
In 3,041 measurements,
l of print at
ead there
The goal of this study was was no significant
to investigate association
the association betweenbetween relative
blood draws, volume
injections, blood change
scember 7, 2015.
or weight-adjusted
d No. R01CA139118
changetrauma,
pressure readings, increase andin undergoing
cellulitis the at-risk arm,one ortravel
and air moreand blood draws
increases (P volume
in arm = .62),ininjections
a
cohort of of
(P = .77), number
No. P50CA089393
patients
flightstreated
(one for
or breast
two [Pcancer
= .77]andand
screened
three for
or lymphedema.
more [P = .91] v none), or duration of
stional Cancer Institute,
flights (1 toPatients
tnnon Research Fund
and[P
12 hours Methods
= .43] and 12 hours or more [P = .54] v none). By multivariate analysis, factors
Between 2005 and 2014, patients undergoing treatment of breast cancer at our institution were
significantly
elated Lymphedema. associated with increases in arm volume included body mass index $ 25 (P = .0236),
screened prospectively for lymphedema. Bilateral arm volume measurements were performed
efined in theaxillary
glossary, lymph node dissection
preoperatively (P , .001),
and postoperatively usingregional lymph
a Perometer. node
At each irradiation patients
measurement, (P = .0364), and
reported the cellulitis
this article and online
(P , .001).number of blood draws, injections, blood pressure measurements, trauma to the at-risk arm(s),
and number of flights taken since their last measurement. Arm volume was quantified using the
Conclusionrelative volume change and weight-adjusted change formulas. Linear random effects models were
an Antonio Breast
, San Antonio, TX,
14.
This study usedsuggests that
to assess thealthough cellulitis
association betweenincreases
relative armrisk of lymphedema,
volume (as a continuous ipsilateral
variable) andblood
non- draws,
injections, treatment
y the responsibility of
blood pressure readings,
risk factors, as well and air travel
as clinical may not be associated with arm volume increases.
characteristics.
The resultsResults
es not necessarily may help to educate clinicians and patients on posttreatment risk, prevention, and
management3,041
In measurements, there was no significant association between relative volume change
l views of the National
the National Institutes
of lymphedema.
or weight-adjusted change increase and undergoing one or more blood draws (P = .62), injections
(P = .77), number of flights (one or two [P = .77] and three or more [P = .91] v none), or duration of
J Clin
s of potential conflictsOncol 33. © 2015 by American Society of Clinical Oncology
flights (1 to 12 hours [P = .43] and 12 hours or more [P = .54] v none). By multivariate analysis, factors
d in the article online at
or contributions are significantly associated with increases in arm volume included body mass index $ 25 (P = .0236),
this article. axillary lymph node dissection (P , .001), regional lymph node irradiation (P = .0364), and cellulitis
(P , .001).
the efficacy of such precautionary behaviors do
or: Alphonse G. INTRODUCTION
Department of
Conclusion
not exist, highlighted in a recent statement by the
, Massachusetts 5Yes v no 20.35 1.78 21.05 to 0.36 20.51 to 4.07 *
Abbreviations: ALND, axillary lymph node0.52
significantly 20.29
dissection; BMI, body mass index; RLNR,
associated
to 1.34
regional
with increases in arm vo
.1126
lymph node radiation; SLNB, sentinel lymph node biopsy
adjusted volume change.
Association Between guide patient
0.66 Precautionary 20.32
*Specified variable or comparison was not analyzed.
education
Behaviors
to 1.65
about
andlymphedema
Breast * risk re
20.14 breast cancer20.77 surgery.
to 0.49 .1781
Cancer–Related Lymphedema in Patients Undergoing
0.35 21.59 to 2.28 *
Bilateral14
Surgery
but one of the studies in our comprehensive
0.13 reviewJ Clin
had Oncol
cohorts 35.
fourfold©
20.43 to 0.69 2017
increased by American
incidence of Society
lymphedema
.8324 o
com
that underwent predominantly ALND, which made them higher- SLNB.8 Of note, other studies have demonstrated th
Maria S. Asdourian, Meyha N. Swaroop, Hoda E. Sayegh, Cheryl L. Brunelle, Amir I. Mina, Hui Zheng, Melissa N.
risk populations because ALND 20.09 skintopuncture
contributes to an approximately 20.63 0.46 does not represent a risk*factor for l
Skolny, and Alphonse G. Taghian1.78 20.51 to 4.07 .1179
INTRODUCTION
axillary lymph node dissection; BMI, body mass index; RLNR, regional lymph node radiation; SLNB, sentinel lymph node biopsy; WAC, weight-
nformation
ge. Risk Factor A B S T R A C T P 95% CI
d of this
comparison was not analyzed.
BMI ≥ 25 .0404 0.05 to 2.02
er 4, 2017.
Purpose Although surgical and targeted treatments for breast
This study examined the lifestyle and clinical risk factors for lymphedema in a cohort of patients who
SLNB cancer have improved .3792 survival,
−1.35 to 0.52 treatment com-
onsibility of underwent bilateral breast cancer surgery.
udies
essarily in our comprehensive review had cohorts
ALND
fourfold plications remain a of
increased incidence significant
0.03 to concern
lymphedema
.0464 4.15 for patients.
compared with
dominantly Patients
he National and Methods
ALND, which made them higher- 8
SLNB. Of note, cancer–related
Breast other studies havelymphedema
demonstrated that (BCRL) ipsilateral
Fig 2. is oneanaly
Multivariable
l Institutes Between 2013 and 2016, 327 patients who underwent bilateral breast cancer surgery
to 2.12 for lary
were pro-
lymph node dissecti
cause ALND contributes to an approximately
Neoadjuvant chemotherapy skin puncture does not represent a risk
.0899 −0.15factor lymphedema;
spectively screened for arm lymphedema ascomplication quantified by the caused by damagevolume
weight-adjusted tomass
lymph change
index; nodes
RLNR, region
1521741. (WAC) formula.
Adjuvant Arm perometry and subjective
chemotherapy data were collected preoperatively
.0161 radiation; SLNB,
0.22 to 2.19 and at regular sentinel lym
through surgical intervention and/or radiation,volu
WAC, weight-adjusted
se G. intervals postoperatively. At the time of each measurement, patients completed a risk assessment
nt of
Breast/chest wall radiation
survey that reported the number of blood draws, which may
P injections,
95% CI interrupt the −1.44
.3879
blood pressure circulation
to 3.70 of lymph
readings, trauma to thefluid
usetts at-risk
RLNR arm, and number of flights since the andprevious
precipitate edema
measurement. of tothe
1.75 arm,
Generalized
.9523 −1.86 breast, or
estimating
m St, .0404 0.05
1 -3 to 2.02
ghian@
equations were applied to ascertain the association among
trunk. arm volumesymptoms,
Associated changes, clinical
suchfactors, and
as decreased
risk exposures. −4 −3 −2 −1 0 1 2 3 4
DOI: https://doi.org/10.1200/JCO.2017.
Mean Difference in Arm
arm
.3792
Volume
functionality,
−1.35 to 0.52
(WAC) in Subgroup
pain,
(%)
heaviness, changes in skin
of Clinical Results
73.7494
The cohort comprised 327 patients and 654.0464
quality, and high rates of infection (eg, cellulitis),
at-risk arms, with a median postoperative follow-up
0.03 to 4.15
that ranged from 6.1 to 68.2 months. Of the 654 arms, 83 developed Fig 2. lymphedema, defined
Multivariable analysis. ALND,as axil-
jco.org © 2017 by American Society of Clin
otherapy a WAC $ 10% relative to baseline. On multivariable .0899 −0.15analysis,
to 2.12 lary lymph
none of thenode dissection;
lifestyle risk BMI,
factorsbody
mass index; RLNR, regional lymph node
examined through the risk assessment survey were significantly associated radiation; SLNB,
with increased WAC.
sentinel lymph node biopsy;
rapy .0161 0.22 to 2.19 2
Multivariable analysis
Downloaded demonstrated
from that having
ascopubs.org by Institut Nationaladebody
la Santmass
et de laindex $ 25
Recherche
WAC, kg/mon October
Mdicale at the volume
weight-adjusted time
5, 2017of breast
from 193.054.110.0
change.
Copyright © 2017 American Society of Clinical Oncology. All rights reserved.
cancer diagnosis (P = .0404), having undergone axillary lymph node dissection (P = .0464), and receiptmotherapy (P = .0161). None of the risk exposures with a larger sample that includes patients with SLNB
Risk Factor P 95% CI
No blood pressures −0.54 to 1.12
One or more blood pressures .0109 −1.26 to 0.03
No blood draws −0.73 to 0.74
One or more blood draws .4906 −1.20 to 0.58
No injections −0.68 to 0.74
One or more injections .0928 −2.09 to 0.24
No trauma −0.72 to 0.70
One or more traumas .5705 −3.11 to 1.66
No flights −0.72 to 1.13
One or more flights .2756 −1.09 to 0.40
No flying hours −0.72 to 1.14
1−12 flying hours .5223 −1.20 to 0.87
> 12 flying hours .2524 −1.48 to 0.46
−3 −2 −1 0 1 2 3
Mean Difference in Arm Volume (WAC) in Subgroup (%)
Fig 1. Univariable analysis. WAC, weight-adjusted volume change.
erican Society of Clinical Oncology JOURNAL OFeu un lymphœdème (réf. 16).
LA REVUE PRESCRIRE • AOÛT 2019 • TOME 39 N° 430 • PAGE 611
Repères
En pratique Ne pas compliquer inutilement
la vie quotidienne. Il est utile d’informer les
femmes qui ont eu un cancer du sein sur le risque
Prévention du lymphœdème de lymphœdème et de se limiter aux seuls conseils
étayés pour les aider à vivre le plus normalement
après cancer du sein possible. Proposer une kinésithérapie précoce
S’en tenir aux conseils argumentés adaptée après un curage axillaire, faciliter une reprise
progressive d’activités physiques, donner des
conseils pour éviter autant que possible un surpoids,
● Les femmes qui ont eu une chirurgie ou une limiter le risque de blessure du membre supérieur
radiothérapie pour un cancer du sein reçoivent du côté du cancer, notamment lors d’activités à
parfois des conseils contraignants au quotidien risque telles que le jardinage, semblent être des
afin de prévenir la survenue d’un lymphœdème du mesures suffisantes.
membre supérieur du côté du cancer. Des suivis En l’absence de lymphœdème, il ne semble pas
de centaines de femmes remettent en question le préjudiciable d’effectuer des ponctions, injections
bien-fondé de certains de ces conseils. ou prises de tension sur le membre supérieursupérieur à
risque. Un antécédent de chirurgie pour cancer du
sein sans apparition d’un lymphœdème ne justifie
pas de restreindre les voyages en avion, les expo-
L es femmes qui ont eu un cancer du sein traité
par chirurgie sont exposées à la survenue d’un
lymphœdème du membre supérieur du côté du
sitions au soleil, les expositions au froid ou au chaud,
le port de vêtements compressifs.
cancer, surtout après un curage ganglionnaire ou ©Prescrire
©Prescrire
une radiothérapie. Le lymphœdème est une aug-
mentation de volume du membre liée à l’altérationMesures "préventives" • â poids (Shaw C et al. Cancer 2007;110:1868) • Rééducation épaule, massage cicatrice (Torres Lacomba M et al. BMJ 2010) • Activités physiques : ↓ femmes avec LO, ↑ QOL (Johansson K et al. Lymphology 2002;35:59), intense : haltérophilie (Schmitz K et al. JAMA 2010;304:2699) • Pas de DLM post-opératoire (Devoogdt N et al. BMJ 2011;343:d5326)
Original Article
months. The main outcome was BCRL, defined as a relative volume change of
RESULTS: A total of 92 patients (7.9%) developed BCRL. Net weight loss vers
Weight Loss Does Not Decrease Risk of Breast Cancer–Related protective against developing BCRL (hazard ratio, 1.38; 95% confidence inter
loss may be recommended as part of an individualized lifestyle management
Arm Lymphedema crease the risk of developing BCRL. Cancer 2021;0:1-7. © 2021 American Can
1 KEYWORDS: breast cancer, breast cancer–related lymphedema, lymphedema
Sacha A. Roberts, BS ; Tessa C. Gillespie, BS1; Amy M. Shui, MA2; Cheryl L. Brunelle, PT, MS, CCS, CLT3;
Kayla M. Daniell, BS1; Joseph J. Locascio, PhD2; George E. Naoum, MD, MMSCI1; and Alphonse G. Taghian, MD, PhD 1
BACKGROUND: The goal of this study was to determine the relationshipImpact between of postoperative weight changeRisk/Roberts
and breast cancer–
INTRODUCTION Weight Change on BCRL
related lymphedema (BCRL). METHODS: In this cohort study, 1161 women underwent unilateral breast surgery for breast cancer from
et al
Advancements in breast cancer (BC) diagnosis and treatment have
2005 to 2020 and were prospectively screened for BCRL. Arm volume measurements were obtained via an optoelectronic perometer
TABLE 2. Impact
preoperatively, of Weightand
postoperatively, Changes From
in the follow- up the 1 every 6 to 12 months.
Preoperative
setting Baseline to follow-
Mean the Last Follow-
up from Up on BCRL
preoperative baseline was 49.1
Development: Multivariable Analysis (n = 1161)
months. The main outcome was BCRL, defined as a
years. As a result, there is a growing need to better understand how
relative volume change of the ipsilateral arm of ≥10% at least 3 months after surgery.
ship. One significant complication of BC treatment is breast cance
RESULTS: A total of 92 patients (7.9%) developed BCRL. Net weight loss versus net weight gain from baseline to last follow-up was not
Univariate
protective against developing BCRL (hazard ratio, 1.38; 95% confidence interval, Multivariable
0.89-2.13; P = .152). CONCLUSIONS: 2
Although weight
5 individuals treated for BC will develop BCRL. BCRL results fro
loss may be recommended as part of an individualized lifestyle management program for overall health, weight loss alone may not de-
HR (95%Cancer
CI) Society. P
3 HR (95% CI) P
space, leading to regional swelling. Patients treated for BC are at li
crease the risk of developing BCRL. Cancer 2021;0:1-7. © 2021 American
Net weight loss vs net weight gain 1.45 (0.96-2.18) weight change. .078 1.38 (0.89-2.13) .152
KEYWORDS: breast cancer, breast cancer–related lymphedema,
Baseline BMI, kg/m 2 able disease that necessitates.003
lymphedema,
1.04 (1.01-1.07)
stressful, time- consuming, and
1.04 (1.01-1.07) .005
expensiv
Age at baseline, y
Race: White vs non-White
BCRL has on patient quality.701of life, understanding
1.01 (0.99- 1.03)
0.87 (0.44-1.74)
.232 —
—
the causes
—
—
of this
Mastectomy vs lumpectomy Various studies
2.49 (1.64- 3.80) have identifiedEffect of manual lymph drainage in addition to
guidelines and exercise therapy on arm lymphoedema
related to breast cancer: randomised controlled trial
itation science , Marie-Rose Christiaens professor, breast surgeon,
12
OPEN ACCESS
s research fellow
BMJ 2011;343:d5326 1
, Steven
doi: 10.1136/bmj.d5326 Truijen scientific coordinator 2
, Ann Smeets
Nele Devoogdt doctor in rehabilitation science , Marie-Rose Christiaens professor, breast surgeon,
12
Page 9 of 12
gynaecological oncologist 3
, Patrick
and coordinator , Inge Geraerts
Neven professor in gynaecological
research fellow , Steven Truijen scientific coordinator , Ann Smeets RESEARCH
3 1 2
breast surgeon , Karin Leunen gynaecological oncologist , Patrick Neven professor in gynaecological
3 3
en professor oncology in rehabilitation science 1
, Marijke Van Kampen professor in rehabilitation science
3 1
1
Department of Rehabilitation Sciences, Katholieke Universiteit Leuven and Department of Physiotherapy, University Hospitals Leuven, Leuven,
Table 4| Comparison of cumulative incidence and point prevalence of arm lymphoedema after surgery for breast cancer
Belgium; 2Department of Health Care, Artesis University College of Antwerp, Antwerp; 3Multidisciplinary Breast Centre, University Hospitals Leuven
and Faculty of Medicine, Katholieke Universiteit Leuven, Leuven
at 3, 6, and 12
months for different definitions according to treatments to prevent lymphoedema
olieke Universiteit Leuven and Department of Physiotherapy, University Hospitals Leuven, Leuven,
Intervention (guidelines,3exercise, manual drainage;
University CollegeAbstract
of Antwerp,
Definition of lymphoedema
Antwerp; Multidisciplinary group/presumed cumulative incidence of no lymphoedema in intervention
Breast Centre, University Hospitals Leuven
Objective To determine the preventive effectn=77)
of manual lymph drainage Control cumulative
group)×(presumed (guidelines, exercise;
incidence n=81) Odds
of no lymphoedema ratio (95% CI) P value*
in control
eit Leuven,
PrimaryLeuven on the development of lymphoedema related to breast cancer.
outcome parameter
group/presumed cumulative incidence of lymphoedema in control group)
or (10/90)×(70/30).
Design Randomised single blinded controlled trial.
Cumulative incidence, ≥200 mL increase: Conclusion Manual lymph drainage in addition to guidelines and
Setting University Hospitals Leuven, Leuven, Belgium.
exercise therapy after axillary lymph node dissection for breast cancer
At 3 months Participants 160 consecutive patients with 8 (10%)
breast cancer and unilateral 6 (7%) 1.4 (0.5 to 4.4) 0.51
is unlikely to have a medium to large effect in reducing the incidence of
axillary lymph node dissection. The randomisation was stratified for body
At 6 months 11 (14%) arm lymphoedema in the short12 (15%)
term. 0.9 (0.4 to 2.3) 0.93
mass index (BMI) and axillary irradiation and treatment allocation was
At 12 months† group/presumed cumulative incidence of
18 (24%)from recruitment
concealed. Randomisation was done independently no lymphoedema
Trial registration Netherlands Trial Register No NTR 1055.
15 (19%) in intervention
1.3 (0.6 to 2.9) 0.45
and treatment. Baseline characteristics were comparable between the
Introduction
Secondary outcome
f manual lymph drainage
parameters
group)×(presumed cumulative incidence of no lymphoedema in control
Seule restriction : délai breast cancerd'intervention de 5
groups.
Cumulative incidence, ≥2 cm increase:
Intervention For six months the intervention group (n=79) performed a
Worldwide, is the most common cancer in women.
o breast At 3cancer.
group/presumed cumulative incidence
Detection and treatment of
of lymphoedema
breast in
cancer have significantly control group)
30-40 treatment programme consisting of guidelines about the prevention of
months
group (n=81) performed or
semaines
8 (10%)
lymphoedema, exercise therapy, and manual lymph drainage. The control
(10/90)×(70/30). après
rates. More1
attentionla
improved over past decades,
is
6 (7%)
now chirurgie…
therefore paid to
1.4 (0.5 to 4.4)
which results in higher survival
complications
0.51
trial. séancesdrainage. sur
At 6 months the same programme without manual lymph
12 (16%) 11 (14%) 1.2 (0.5 to 2.8) 0.72
related to treatment, such as arm lymphoedema.
At 12 months† 20 (27%) For a woman with breast16 (20%)lymphoedema is a debilitating
cancer, 1.4 (0.7 to 3.0) 0.35
12 semaines Conclusion Manual
Main outcome measures Cumulative incidence of arm lymphoedema
lymphand drainage
incurable problem inthat addition
is caused by to
reduced guidelines
transport and
Belgium. and time
Point prevalence, ≥200 to develop arm lymphoedema, defined as an increase in arm
mL increase:
capacity of the lymph system (related to the surgery or
At 3 months exercise therapy
volume of 200 mL or more in the value before surgery.
5 (7%) after axillary lymph
radiotherapy, or both),node 3 (4%)dissection
sometimes combined with anfor 1.8 breast
(0.4 to 7.8) cancer
increase 0.43
ast cancer and unilateral
Results Four patients in the intervention group and two in the control
in lymph load (related to hypertension, for example). Twelve
23
At 6 months is Atunlikely
group were lost to follow-up. 4 to
12 months after (5%) have
surgery, a medium
the cumulative
monthsto afterlarge effect
axillary lymph8 (10%)nodein reducing
dissection, the
the point0.5 (0.1incidence
to 1.7) of
0.28
on wasAtstratified
12 months† for bodygroup (24%)arm
incidence rate for arm lymphoedema was comparable between the
prevalence of arm lymphoedema ranges from 12% to 26%,
4 5
intervention
lymphoedema
and control group9(19%)
(12%)
in thethough
(odds ratio 1.3, 95%
confidence interval 0.6 to 2.9; P=0.45). The time to develop arm
short someterm. 8 (10%)
have reported point prevalence rates up to 70%.
1.2 (0.4 to 3.3)6
0.71
reatment allocationlymphoedema
was was comparable between the two group during the first This wide variety is related to differences in treatment of breast
Point prevalence, ≥2 cm increase:Table 3
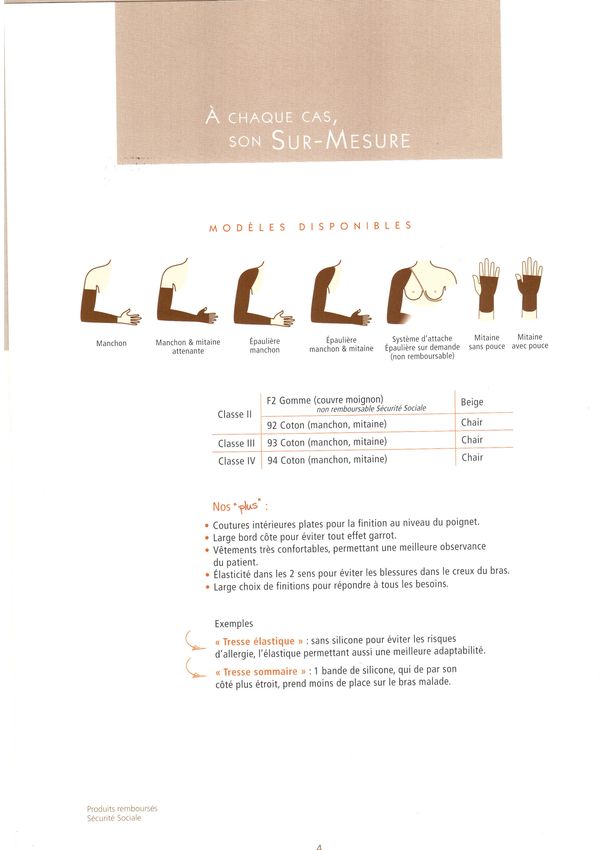
Preventive measure and evidence to support either fact or fiction.
NIH-PA Author Manuscript
Preventive measure Best scientific evidence for Best scientific evidence against Fact/Fiction/To be determined
Avoid needle sticks of any Clark [10] – level 2 prospective Winge 18—Level 3 questionnaire To be determined
type observational study (188 patients), study (311 patients of which 88 had
findings that 44% patients with intravenous procedures in affected
needle stick developed lymphedema limb). Only 4 patients developed
as compared with 18% of those lymphedema in relation to
without needle sticks venipuncture
P Avoid Pressure Louden & Petrek [15, 16] – level 5,
expert opinion hypothesising that
Dawson [22] – level 3,
retrospective cohort (317 patients),
Probably fiction
r blood pressure monitoring, tight
clothing increases blood pressure in
at risk limb resulting in increased
no new cases or exacerbations of
lymphedema in 15 patients with a
history of lymph node dissection
é
lymph production. who subsequently had elective
hand surgery with tourniquet
Leg/Limb precautions Ryan [24] – level 5, expert opinion, None found To be determined
v crossing legs hinders venous return,
prolonged standing/sitting results in
pooling of blood in legs and hence
e Avoid Air travel/wear
increased interstitial fluid leakage.
Casley-Smith [28] – level 4, Graham [29] – level 2, Cohort Probably fiction
n
compressive garments for questionnaire based retrospective study (293 patients), no cases of
air travel study (531 patients), 27 patients permanent or new onset
NIH-PA Author Manuscript
reported lymphedema symptoms lymphedema found after aircraft
started after aircraft flight & 67 flight taken.
t patients reported worsening
lymphedema symptoms after flying.
i Maintain a normal body
weight
Shaw [41] – level 1, randomised
clinical trial (21 patients),
interventions designed to promote
Villasor [6] – level 3 non-
consecutive cohort (51 patients),
47% patients with lymphedema had
Fact
o
weight loss after surgery normal weight, no correlation
significantly reduced excess arm between lymphedema formation
volume and lymphedema. and obesity or weight found.
n Avoid extremes of
temperature/apply
sunscreen/avoid burns
Hettrick [48] – level 4 prospective
analysis, 1% of burn population
found to have lymphedema.
Chang [45] – level 1 double blind
randomized study (60 patients),
heat added to placebo, or
Fiction
benzopyrone therapy significantly
improved symptoms of
lymphedema compared to placebo
or benzopyrone alone.
Avoid vigorous exercise Petrek/Foldi [1] level 5 Expert Schmitz [52] – level 1 randomized Fiction
opinion rationalising that vigorous trial (141 patients), no increased
exercise increases blood flow and incidence of lymphedema in
consequently lymphatic fluid exercise group compared to non-
production. exercise control group.
NIH-PA
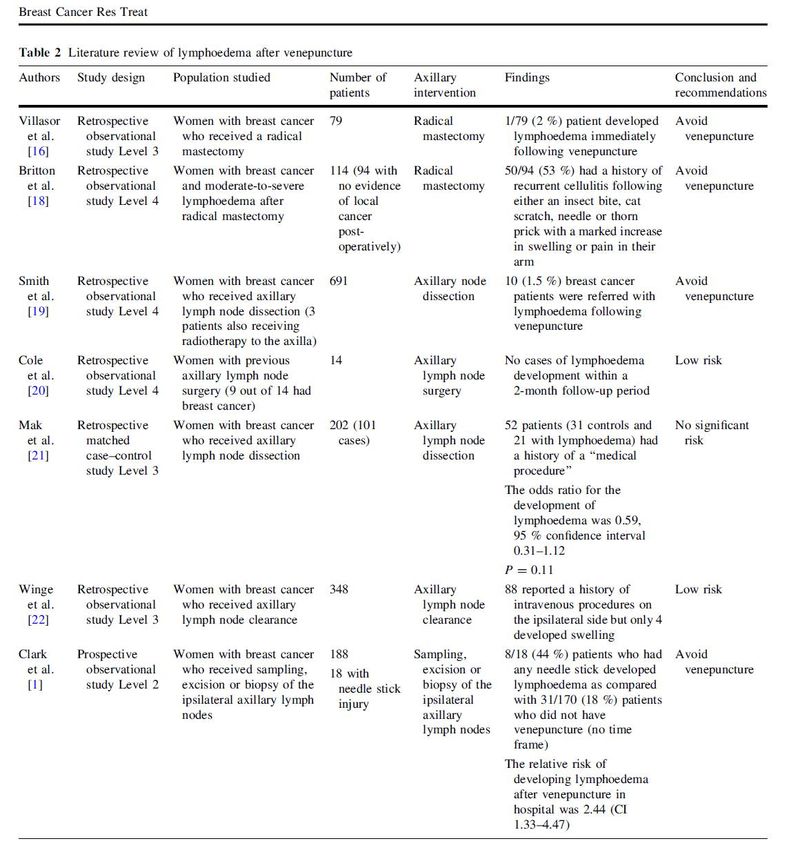
Cemal Y et al. J Am Coll Surg 2011;213:543Background
Clinical Epidemiology Weight lifting has generally been proscribed for women with breast-cancer related
niversity of Pennsyl-
icine and Abramson
Weight Lifting in Women with Breast-
lymphedema, preventing them from obtaining the well-established health benefits
delphia (K.H.S., A.T., of weight lifting, including increases in bone density.
C.T.W.-S., Q.P.G.); the Cancer Related Lymphedema
atology, University of Methods
School, Minneapolis Kathryn H. Schmitz, Ph.D., M.P.H., Rehana L. Ahmed, M.D., Ph.D.,
partment of Physical We performed a randomized, controlled trial of twice-weekly progressive weight
ilitation, Mayo Clinic, liftingAndreainvolving Troxel, Sc.D., Andrea
141 breast-cancer Cheville,
survivors M.D.,
with Background
stableRebecca Smith,
lymphedema ofM.D.,
the arm. The
). Address reprint re- Lorita Lewis-Grant,
primary outcome was the change M.P.H.,
in armM.S.W.,
and hand Cathy J. Bryan,
swelling at 1M.Ed.,
year, as measured
From the Center for Clinical Epidemiology Weight lifting has generally been
z at the Department
Catherine T. Williams-Smith,
with breast-cancerB.S., andlymphedema
Quincy P. Greene
pidemiology, Univer- through displaced water volume of the affected and unaffected limbs. Secondary
weight lifting in women related
and Biostatistics, University of Pennsyl-
, 423 Guardian Dr., outcomes included the incidence of exacerbations of lymphedema, number and lymphedema, preventing them f
vania School of Medicine and Abramson
iladelphia, PA 19104-
Table 3.severity ofOutcomes
lymphedema symptoms, and muscle strength. Participants were required
of weight lifting, including incre
Lymphedema at 12 Months, According to Study Group.*
mail.med.upenn.edu. A bs t r ac t
Cancer Center, to wear aPhiladelphia
well-fitted compression (K.H.S.,garment A.T., while weight lifting.Cumulative Incidence Ratio
61:664-73. or Mean Difference
R.S., L.L.-G.,
Variable
husetts Medical Society.
C.J.B., C.T.W.-S., Q.P.G.);
Weight Lifting the Control (95% CI) P Value
Results
Background
Department The of Dermatology,
proportion of
ical Epidemiology Weight lifting has generally been proscribed women
no.University
of patients
who had an of
increase Methods
no. of patients
ofwomen
5%value
or with
morebreast-cancer
in limb swelling was
with data value for
with data related
Minnesota
ersity of Pennsyl- Change in
lymphedema, Medical
interlimb
similar volume School,them
difference
in thepreventing
weight-lifting Minneapolis
group
from(11%) obtainingand the thecontrol group (12%)
well-established health(cumulative
benefits
ne and Abramson
(R.L.A.);
≥5%
of
increase
and
incidence
weight
no.
the
(%)
Department
ratio,
lifting, 1.00; 95%
including
70
of Physical
confidence
increases
8 (11)
ininterval,
bone
We
69
0.88
density.
performed
to
8 (12)
1.13).
1.00 (0.88 to a
As compared
1.13)randomized,
with
1.00
the c
phia (K.H.S., A.T., ≥5% decrease no. (%) 70 13 (19) 69 15 (22) 0.96 (0.81 to 1.14) 0.68
Medicine
W.-S., Q.P.G.); the Mean control
andvolume
interlimb
group, the weight-lifting
Rehabilitation,
discrepancy between Mayo 70
group
Clinic,
−0.69±5.87
had lifting
greater
69 involving
improvements
−0.98±7.31 141
in self-reported
−0.29 (−1.94 to 2.51) breast-cance
0.80
logy, University of Methods severity of lymphedema symptoms (P = 0.03) and upper- and lower-body strength
baseline and 12 mo (percentage points)
Rochester, MN (A.C.). Address65reprint re-
hool, Minneapolis (PYou can also read