Guidelines for Nursing - Ergonomics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Guidelines
for Nursing
Homes
OSHA 3182-3R 2009
Ergonomics
for the Prevention of
Musculoskeletal DisordersGuidelines for Nursing Homes
Ergonomics for the Prevention
of Musculoskeletal Disorders
U.S. Department of Labor
Elaine L. Chao, Secretary
Occupational Safety and Health Administration
John L. Henshaw, Assistant Secretary
OSHA 3182-3R 2009
Guidelines for Nursing Homes 12 Guidelines for Nursing Homes
Table of Contents
5 Executive Summary
7 SECTION I:
Introduction
9 SECTION II:
A Process for Protecting Workers
9 Provide Management Support
9 Involve Employees
10 Identify Problems
10 Implement Solutions
10 Address Reports of Injuries
11 Provide Training
11 Evaluate Ergonomics Efforts
12 SECTION III:
Identifying Problems and Implementing Solutions for Resident
Lifting and Repositioning
12 Identifying Problems for Resident Lifting and Repositioning
■ Figure 1. Transfer to and from: Bed to Chair, Chair to Toilet,
Chair to Chair, or Car to Chair
■ Figure 2. Lateral Transfer to and from: Bed to Stretcher, Trolley
■ Figure 3. Transfer to and from: Chair to Stretcher
■ Figure 4. Reposition in Bed: Side-to-Side, Up in Bed
■ Figure 5. Reposition in Chair: Wheelchair and Dependency Chair
■ Figure 6. Transfer a Patient Up From the Floor
17 Implementing Solutions for Resident Lifting and Repositioning
■ Transfer from Sitting to Standing Position
■ Resident Lifting
■ Repositioning in Chair
■ Ambulation
■ Lateral Transfer; Repositioning
■ Lateral Transfer in Sitting Position
■ Transfer from Sitting to Standing Position
■ Weighing
■ Transfer from Sitting to Standing Position; Ambulation
■ Repositioning
■ Bathtub, Shower, and Toileting Activities
Guidelines for Nursing Homes 3Table of Contents
27 SECTION IV:
Identifying Problems and Implementing Solutions for
Activities Other than Resident Lifting and Repositioning
■ Storage and Transfer of Food, Supplies, and Medications
■ Mobile Medical Equipment
■ Working with Liquids in Housekeeping
■ Working with Liquids in Kitchens
■ Hand Tools
■ Linen Carts
■ Handling Bags
■ Reaching into Sink
■ Loading or Unloading Laundry
■ Cleaning Rooms (Wet Method)
■ Cleaning Rooms (Electrical)
31 SECTION V:
Training
31 Nursing Assistants and Other Workers at Risk of Injury
31 Training for Charge Nurses and Supervisors
31 Training for Designated Program Managers
33 SECTION VI:
Additional Sources of Information
35 References
36 Appendix: A Nursing Home Case Study
4 Guidelines for Nursing HomesExecutive Summary
These guidelines provide Although these guidelines are
recommendations for nursing home designed specifically for nursing
employers to help reduce the number homes, OSHA hopes that employers
and severity of work-related muscu- with similar work environments, such
loskeletal disorders (MSDs) in their as assisted living centers, homes for
facilities. MSDs include conditions the disabled, homes for the aged,
such as low back pain, sciatica, and hospitals will also find this
rotator cuff injuries, epicondylitis, information useful.
and carpal tunnel syndrome. The OSHA also recognizes that small
recommendations in these guidelines employers, in particular, may not
are based on a review of existing have the need for as comprehensive a
practices and programs, State OSHA program as would result from
programs, as well as available implementation of every action and
scientific information, and reflect strategy described in these guidelines.
comments received from representatives Additionally, OSHA realizes that
of trade and professional associations, many small employers may need
labor organizations, the medical assistance in implementing an
community, individual firms, appropriate ergonomics program.
and other interested parties. OSHA That is why we emphasize the
thanks the many organizations availability of the free OSHA
and individuals involved for their consultation service for smaller
thoughtful comments, suggestions, employers. The consultation service is
and assistance. independent of OSHA’s enforcement
More remains to be learned about activity and will be making special
the relationship between workplace efforts to provide help to the nursing
activities and the development of home industry.
MSDs. However, OSHA believes These guidelines are advisory in
that the experiences of many nursing nature and informational in content.
homes provide a basis for taking They are not a new standard or
action to better protect workers. regulation and do not create any new
As the understanding of these injuries OSHA duties. Under the OSH Act,
develops and information and the extent of an employer’s obligation
technology improve, the recommenda- to address ergonomic hazards is
tions made in this document may governed by the general duty clause,
be modified. 29 U.S.C. 654(a)(1).
Guidelines for Nursing Homes 5Executive Summary
An employer’s failure to implement While specific measures may
the guidelines is not a violation, or differ from site to site, OSHA
evidence of a violation, and may not recommends that:
be used as evidence of a violation, of ■ Manual lifting of residents be
the general duty clause. Furthermore, minimized in all cases and
the fact that OSHA has developed eliminated when feasible.
this document is not evidence and ■ Employers implement an effective
may not be used as evidence of an ergonomics process that:
employer’s obligations under the ■ provides management support;
general duty clause; the fact that a ■ involves employees;
measure is recommended in this ■ identifies problems;
document but not adopted by an ■ implements solutions;
employer is not evidence, and may ■ addresses reports of injuries;
not be used as evidence, of a ■ provides training; and
violation of the general duty clause. ■ evaluates ergonomics efforts.
In addition, the recommendations These guidelines elaborate on
contained herein should be adapted these recommendations, and include
to the needs and resources of each additional information employers
individual place of employment. can use to identify problems and
Thus, implementation of the guide- train employees. Of particular value
lines may differ from site to site are examples of solutions employers
depending on the circumstances can use to help reduce MSDs in their
at each particular site. workplace. Recommended solutions
for resident lifting and repositioning
are found in Section III, while
recommended solutions for other
ergonomic concerns are in Section
IV. The appendix includes a case
study describing the process one
nursing home used to reduce MSDs.
6 Guidelines for Nursing HomesSECTION I
Introduction
Nursing homes that have of weight involved, awkward postures
implemented injury prevention efforts that may result from leaning over a
focusing on resident lifting and bed or working in a confined area,
repositioning methods have achieved shifting of weight that may occur if a
considerable success in reducing resident loses balance or strength
work-related injuries and associated while moving, and many other
workers’ compensation costs. Pro- factors. The risk factors that workers
viding a safer and more comfortable in nursing homes face include:
work environment has also resulted in ■ Force - the amount of physical
additional benefits for some facilities, effort required to perform a task
including reduced staff turnover and (such as heavy lifting) or to main-
associated training and administrative tain control of equipment or tools;
costs, reduced absenteeism, increased ■ Repetition - performing the same
productivity, improved employee motion or series of motions contin-
morale, and increased resident ually or frequently; and
comfort. These guidelines provide ■ Awkward postures - assuming
recommendations for employers to positions that place stress on the
help them reduce the number and body, such as reaching above
severity of work-related musculoskele- shoulder height, kneeling,
tal disorders in their facilities using squatting, leaning over a bed, or
methods that have been found to be twisting the torso while lifting (3).
successful in the nursing home
environment.
Providing care to nursing home
residents is physically demanding Wyandot County Nursing Home in Upper
work. Nursing home residents often Sandusky, Ohio, has implemented a policy
require assistance to walk, bathe, or of performing all assisted resident
perform other normal daily activities. transfers with mechanical lifts, and has
In some cases residents are totally purchased electrically adjustable beds.
dependent upon caregivers for According to Wyandot, no back injuries
mobility. Manual lifting and other from resident lifting have occurred in over
tasks involving the repositioning of five years. The nursing home also reported
residents are associated with an that workers’ compensation costs have
increased risk of pain and injury to declined from an average of almost
caregivers, particularly to the back (2, $140,000 per year to less than $4,000 per
3). These tasks can entail high physical year, reduced absenteeism and overtime
have resulted in annual savings of
demands due to the large amount
approximately $55,000, and a reduction in
costs associated with staff turnover has
saved an additional $125,000 (1). (see
Reference List)
Guidelines for Nursing Homes 7Introduction
Excessive exposure to these risk
factors can result in a variety of After implementing a program designed
disorders in affected workers (3, 5). to eliminate manual lifting of residents,
These conditions are collectively Schoellkopf Health Center in Niagara
referred to as musculoskeletal Falls, New York, reported a downward
disorders, or MSDs. MSDs include trend in the number and severity of
injuries, with lost workdays dropping
conditions such as low back pain,
from 364 to 52, light duty days
sciatica, rotator cuff injuries,
dropping from 253 to 25, and workers’
epicondylitis, and carpal tunnel
compensation losses falling from
syndrome (6). Early indications of
$84,533 to $6,983 annually (4).
MSDs can include persistent pain,
restriction of joint movement, or soft
tissue swelling (3, 7).
While some MSDs develop gradu-
ally over time, others may result At Citizens Memorial Health Care Facility
from instantaneous events such as a in Bolivar, Missouri, establishment of an
single heavy lift (3). Activities outside ergonomics component in the existing
of the workplace that involve safety and health program was reportedly
substantial physical demands may followed by a reduction in the number of
also cause or contribute to MSDs (6). OSHA-recordable lifting-related injuries of
In addition, development of MSDs at least 45% during each of the next four
may be related to genetic causes, years, when compared to the level of
gender, age, and other factors (5, 6). injuries prior to the ergonomics efforts.
Finally, there is evidence that reports The number of lost workdays associated
of MSDs may be linked to certain with lifting-related injuries was reported
psychosocial factors such as job to be at least 55% lower than levels
dissatisfaction, monotonous work, during each of the previous four years.
and limited job control (5, 6). These Citizens Memorial reported that these
guidelines address only physical reductions contributed to a direct savings
factors in the workplace that are of approximately $150,000 in workers’
related to the development of MSDs. compensation costs over a five year
period (8).
8 Guidelines for Nursing HomesSECTION II
A Process for Protecting Workers
The number and severity of sustained effort, allocation of
injuries resulting from physical resources, and frequent follow-up
demands in nursing homes — and that can only be achieved through
associated costs — can be substan- the active support of management.
tially reduced (2, 9). Providing an
alternative to manual resident lifting Involve Employees
is the primary goal of the ergonomics Employees are a vital source of
process in the nursing home setting information about hazards in their
and of these guidelines. OSHA workplace. Their involvement adds
recommends that manual lifting of problem-solving capabilities and
residents be minimized in all cases hazard identification assistance,
and eliminated when feasible. OSHA enhances worker motivation and job
further recommends that employers satisfaction, and leads to greater
develop a process for systematically acceptance when changes are made
addressing ergonomics issues in their in the workplace. Employees can:
facilities, and incorporate this ■ submit suggestions or concerns;
process into an overall program to ■ discuss the workplace and
recognize and prevent occupational work methods;
safety and health hazards. ■ participate in the design of
An effective process should be work, equipment, procedures,
tailored to the characteristics of and training;
the particular nursing home but ■ evaluate equipment;
OSHA generally recommends the ■ respond to employee surveys;
following steps: ■ participate in task groups with
responsibility for ergonomics; and
Provide Management Support ■ participate in developing the nurs-
Strong support by management ing home’s ergonomics process.
creates the best opportunity for
success. OSHA recommends that
employers develop clear goals, assign
responsibilities to designated staff
members to achieve those goals,
provide necessary resources, and
ensure that assigned responsibilities
are fulfilled. Providing a safe and
healthful workplace requires a
Guidelines for Nursing Homes 9A Process for Protecting Workers
An Identify Problems eliminate hazards and improve the
Nursing homes can more work environment. These changes
successfully recognize problems by usually include the use of equipment,
establishing systematic methods for work practices, or both. When
identifying ergonomics concerns in choosing methods for lifting and
their workplace. Information about repositioning residents, individual
where problems or potential factors should be taken into account.
problems may occur in nursing Such factors include the resident’s
homes can be obtained from a rehabilitation plan, the need to restore
variety of sources, including OSHA the resident’s functional abilities,
300 and 301 injury and illness medical contraindications, emergency
information, reports of workers’ situations, and resident dignity and
compensation claims, accident and rights. Examples of solutions can be
near-miss investigation reports, found in Sections III and IV.
insurance company reports,
employee interviews, employee Address Reports of Injuries
surveys, and reviews and observations Even in establishments with
of workplace conditions. Once effective safety and health programs,
information is obtained, it can be injuries and illnesses may occur.
used to identify and evaluate elements Work-related MSDs should be
of jobs that are associated managed in the same manner and
with problems. Sections III and IV under the same process as any other
contain further information on occupational injury or illness (10).
methods for identifying ergonomics Like many injuries and illnesses,
concerns in the nursing home employers and employees can benefit
environment. from early reporting of MSDs. Early
diagnosis and intervention, including
Implement Solutions alternative duty programs, are
When problems related to particularly important in order to
ergonomics are identified, suitable limit the severity of injury, improve
options can then be selected and the effectiveness of treatment,
implemented to eliminate hazards. minimize the likelihood of disability
Effective solutions usually involve or permanent damage, and reduce
workplace modifications that the amount of associated workers’
compensation claims and costs.
OSHA’s injury and illness recording
and reporting regulation (29 CFR
1904) requires employers to keep
records of work-related injuries and
illnesses. These reports can help the
nursing home identify problem areas
10 Guidelines for Nursing HomesA Process for Protecting Workers
and evaluate ergonomic efforts. needed. Evaluation and follow-up are
Employees may not be discriminated central to continuous improvement
against for reporting a work-related and long-term success. Once solutions
injury or illness. [29 U.S.C. 660(c)] are introduced, OSHA recommends
that employers ensure they are
Provide Training effective. Various indicators (e.g.,
Training is necessary to ensure OSHA 300 and 301 information
that employees and managers can data and workers’ compensation
recognize potential ergonomics issues reports) can provide useful empirical
in the workplace, and understand data at this stage, as can other tech-
measures that are available to niques such as employee interviews.
minimize the risk of injury. Ergo- For example, after introducing a new
nomics training can be integrated lift at a nursing home, the employer
into general training on performance should follow-up by talking with
requirements and job practices. employees to ensure that the problem
Effective training covers the problems has been adequately addressed. In
found in each employee’s job. More addition, interviews provide a
information on training can be found mechanism for ensuring that the
in Section V. solution is not only in place, but is
being used properly. The same methods
Evaluate Ergonomics Efforts that are used to identify problems in
Nursing homes should evaluate many cases can also be used for
the effectiveness of their ergonomics evaluation.
efforts and follow-up on unresolved
problems. Evaluation helps sustain
the effort to reduce injuries and
illnesses, track whether or not
ergonomic solutions are working,
identify new problems, and show
areas where further improvement is
Guidelines for Nursing Homes 11SECTION III
A Identifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
Identifying Problems The resident assessment should
for Resident Lifting include examination of factors
and Repositioning such as:
Assessing the potential for work ■ the level of assistance the resident
to injure employees in nursing homes requires;
is complex because typical nursing ■ the size and weight of the resident;
home operations involve the repeated ■ the ability and willingness of
lifting and repositioning of the the resident to understand and
residents. Resident lifting and cooperate; and
repositioning tasks can be variable, ■ any medical conditions that may
dynamic, and unpredictable in influence the choice of methods
nature. In addition, factors such as for lifting or repositioning.
resident dignity, safety, and medical These factors are critically
contraindications should be taken important in determining
into account. As a result, specific appropriate methods for lifting and
techniques are used for assessing repositioning a resident. The size
resident lifting and repositioning and weight of the resident will, in
tasks that are not appropriate for some situations, determine which
assessing the potential for injury equipment is needed and how many
associated with other nursing caregivers are required to provide
home activities. assistance. The physical and mental
An analysis of any resident lifting abilities of the resident also play an
and repositioning task involves an important role in selecting
assessment of the needs and abilities appropriate solutions. For example,
of the resident involved. This a resident who is able and willing to
assessment allows staff members to partially support their own weight
account for resident characteristics may be able to move from his or her
while determining the safest methods bed to a chair using a standing assist
for performing the task, within the device, while a mechanical sling lift
context of a care plan that provides may be more appropriate for those
for appropriate care and services for residents who are unable to support
the resident. Such assessments their own weight. Other factors
typically consider the resident’s related to a resident’s condition may
safety, dignity and other rights, as need to be taken into account as
well as the need to maintain or well. For instance, a resident who
restore a resident’s functional abilities. has recently undergone hip
replacement surgery may require
specialized equipment for assistance
in order to avoid placing stress on
the affected area.
A number of protocols have been
developed for systematically examining
resident needs and abilities and/or
12 Guidelines for Nursing HomesIdentifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
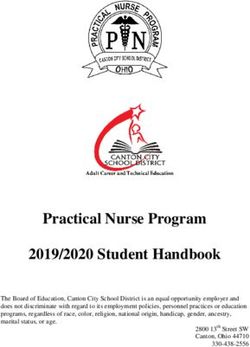
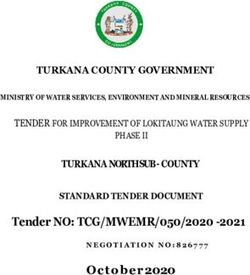
FIGURE 1 Transfer to and from: Bed to Chair, Chair to Toilet, Chair to Chair, or Car to Chair
Caregiver assistance not needed;
Can patient stand by for safety as needed.
Fully
bear weight?
Partially
Is the patient
No cooperative? Stand and pivot technique using a gait/transfer belt
Yes (1 caregiver) -or- powered standing assist lift
No (1 caregiver)
Is the patient
No Use full body sling lift and
cooperative?
2 caregivers.
Yes
■ For seated transfer aid, must have chair with arms that
Does the recess or are removable.
patient have No ■ For full body sling lift, select a lift that was specifically
upper extremity designed to access a patient from the car (if the car is
strength? the starting or ending destination).
Yes
■ If partial weight bearing, transfer toward stronger side.
■ Toileting slings are available for toileting.
■ Bathing mesh slings are available for bathing.
Seated transfer aid; may use gait/transfer belt until the
Source: The Patient Safety Center of Inquiry (Tampa, FL).
patient is proficient in completing transfer independently. Veterans Health Administration & Department of Defense.
October 2001.
FIGURE 2 Lateral Transfer to and from: Bed to Stretcher, Trolley
Caregiver assistance not needed;
stand by for safety as needed.
Yes
If patient is 200 pounds: Use a lateral sliding aid
and 3 caregivers -or- a friction-reducing device or
must be taken to avoid shearing force.
lateral transfer device and 2 caregivers -or-
a mechanical lateral transfer device.
Source: The Patient Safety Center of Inquiry (Tampa, FL). Veterans
Health Administration & Department of Defense. October 2001.
Guidelines for Nursing Homes 13Identifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
for recommending procedures and Program Policy and Guide,
equipment to be used for performing recommends solutions for resident
lifting and repositioning tasks. The lifting and repositioning problems,
following are some examples: based on the CMS classification
■ The Resident Assessment Instrument, system. (A rating of “4” indicates
published by the Centers for a totally dependent resident; a “3”
Medicare and Medicaid Services rating indicates residents that need
(CMS), provides a structured, extensive assistance; a “2/1”
standardized approach for assessing rating indicates residents that need
resident capabilities and needs only limited assistance/general
that results in a care plan for each supervision. Residents rated “0”
resident. Caregivers can use this are independent.) Employers can
information to help them determine access this information from
the appropriate method for lifting www.osha.gov.
or repositioning residents. Many The nursing home operator should
nursing homes use this system to use an assessment tool which is
comply with CMS requirements appropriate for the conditions in an
for nursing homes. Employers individual nursing home. The special
can access this information from needs of bariatric (excessively heavy)
www.cms.hhs.gov/medicaid/ residents may require additional
mds20/. focus. Assistive devices must be
■ Patient Care Ergonomics Resource capable of handling the heavier
Guide: Safe Patient Handling and weight involved, and modification of
Movement is published by the work practices may be necessary.
Patient Safety Center of Inquiry, A number of individuals in nursing
Veterans Health Administration and homes can contribute to resident
the Department of Defense. This assessment and the determination of
document provides flow charts appropriate methods for assisting in
(shown here in Figures 1-6) that transfer or repositioning. Interdisciplinary
address relevant resident assessment teams such as staff nurses,
factors and recommends solutions certified nursing assistants, nursing
for resident lifting and repositioning supervisors, physical therapists,
problems. This material is one physicians, and the resident or his/her
example of an assessment tool that representative may all be involved. Of
has been used successfully. Employers critical importance is the involvement
can access this information from of employees directly responsible for
www.patientsafetycenter.com. resident care and assistance, as the
Nursing home operators may needs and abilities of residents may
find another tool or develop an vary considerably over a short period
assessment tool that works better in of time, and the employees responsible
their facilities. for providing assistance are in the
■ Appendix A of the Settlement best position to be aware of and
Agreement between OSHA and accommodate such changes.
Beverly Enterprises, entitled Lift
14 Guidelines for Nursing HomesIdentifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
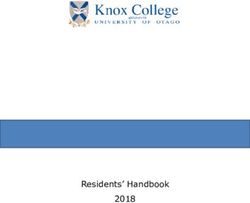
FIGURE 3 Transfer to and from: Chair to Stretcher
Is the patient Use full-body sling lift and
No
cooperative? 2 or more caregivers.
Yes
Caregiver assistance not needed;
stand by for safety as needed.
Fully
Can the patient
bear weight?
If exam table/stretcher can be positioned
No to a low level, use a non-powered
stand-assist aid. If not, use a full-body sling lift.
Use full-body sling lift and Comments:
2 or more caregivers. High/low exam tables and stretchers would be ideal.
Source: The Patient Safety Center of Inquiry (Tampa, FL).
Veterans Health Administration & Department of Defense.
October 2001.
FIGURE 4 Reposition in Bed: Side-to-Side, Up in Bed
Caregiver assistance not
Fully needed; patient may/may
not use positioning aid.
If patient is >200 pounds:
Can Patient
Use a friction-reducing device
assist?
and at least 3 caregivers.
Partially Encourage patient
No Able to assist using a
positioning aid or cues.
If patient isIdentifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
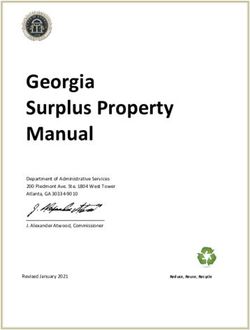
FIGURE 5 Repostition in Chair: Wheelchair and Dependency Chair
Can patient Caregiver assistance not needed;
Fully
assist? stand by for safety as needed.
Partially
No If patient has upper extremity strength in
both arms, have patient lift up while
caregiver pushes knees to reposition.
Does chair If patient lacks sensation, cues may
recline? Yes be needed to remind Patient to reposition.
No Recline chair and use a friction-reducing
device and 2 caregivers.
Is patient Yes Use full-body sling lift -or- non-powered
cooperative? stand-assist aid and 1 to 2 caregivers.
No
Comments:
■ This is not a one person task: DO NOT PULL FROM BEHIND CHAIR. Use full-body sling lift and
■ Take full advantage of chair functions, e.g., chair that reclines, or use of 2 or more caregivers.
arm rest of chair to facilitate repositioning.
■ Make sure the chair wheels are locked.
Source: The Patient Safety Center of Inquiry (Tampa, FL). Veterans Health Administration & Department of Defense. October 2001.
FIGURE 6 Transfer a Patient Up From the Floor
Was patient Was the Depends on type and severity of injury
Yes No
injured? injury minor? (follow Standard Operating Procedures).
No1 Yes
Is patient Full-body sling lift needed with
No
independent? 2 or more caregivers.
Comments: Yes
Use full-body sling that goes all the way down to the
floor (most of the newer models are capable of this).
Caregiver assistance not
1
Modifications made with concurrence of Dr. Audrey needed; stand by for
Nelson at Veterans Administration Hospital, Tampa, safety as needed.
Florida.
Source: The Patient Safety Center of Inquiry (Tampa, FL).
Veterans Health Administration & Department of Defense. October 2001.
16 Guidelines for Nursing HomesIdentifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
Implementing Solutions Employers should establish close
for Resident Lifting working relationships with equipment
and Repositioning suppliers. Such working relationships
The recommended solutions help with obtaining training for
presented in the following pages are employees, modifying the equipment
not intended to be an exhaustive list, for special circumstances, and
nor does OSHA expect that all of procuring parts and service when
them will be used in any given needed. Employers will want to pay
facility. The information represents a particular attention to the effectiveness
range of available options that a of the equipment, especially the
facility can consider using. Many of injury and illness experience of other
the solutions are simple, common nursing homes that have used the
sense modifications to equipment or equipment. The following questions
procedures that do not require are designed to aid in the selection of
substantial time or resources to the equipment and supplier that best
implement. Others may require more meets the needs of an individual
significant efforts. The integration of nursing home.
various solutions into the nursing ■ Availability of technical service - Is
home is a strategic decision that, if over-the-phone assistance, as well
carefully planned and executed, will as onsite assistance, for repairs
lead to long-term benefits. Equip- and service of the lift available?
ment must meet applicable regula- ■ Availability of parts - Which parts
tions regarding equipment design and will be in stock and available in a
use, such as the restraint regulations short time frame and how soon can
from the Centers for Medicare and they be shipped to your location?
Medicaid. In addition, administrators ■ Storage requirements - Is the equip-
should follow any manufacturers’ ment too big for your facility? Can
recommendations and review guide- it be stored in close proximity to the
lines, such as the FDA Hospital Bed area(s) where it is used?
Safety Workgroup Guidelines, to ■ If needed, is a charging unit and
help ensure patient safety. Manage- back up battery included? What is
ment should also be cognizant of the simplicity of the charging unit
several factors that might restrict the and space required for a battery
application of certain measures, such charger if one is needed?
as residents’ rehabilitation plans, the
need for restoration of functional
abilities, other medical contra-
indications, emergency conditions,
and residents’ dignity and rights.
The procurement of equipment
and the selection of an equipment
supplier are important considerations
when implementing solutions.
Guidelines for Nursing Homes 17Identifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
■ If the lift has a self-contained Based on many factors, including
charging unit, what is the amount the characteristics of the resident
of space necessary for charging population and the layout of the
and what electrical receptacles are facility, employers should determine
required? What is the minimum the number and types of devices
charging time of a battery? needed. Devices should be located so
■ How high is the base of the lift that they are easily accessible to
and will it fit under the bed and workers. If resident lifting equipment
various other pieces of furniture? is not accessible when it is needed, it
How wide is the base of the lift or is likely that other aspects of the
is it adjustable to a wider and ergonomics process will be ineffective.
lockable position? If the facility can initially purchase
■ How many people are required to only a portion of the equipment
operate the lift for lifting of a needed, it should be located in the
typical 200-pound person? areas where the needs are greatest.
■ Does the lift activation device Employers should also establish
(pendant) have remote capabilities? routine maintenance schedules to
■ How many sizes and types of ensure that the equipment is in good
slings are available? What type of working order.
sling is available for optimum The following are examples of
infection control? solutions for resident lifting and
■ Is the device versatile? Can it be a repositioning tasks.
sit-to-stand lift, as well as a lift
device? Can it be a sit-to-stand lift
and an ambulation-assist device?
■ What is the speed and noise level
of the device? Will the lift go to
floor level? How high will it go?
18 Guidelines for Nursing HomesIdentifying Problems and Implementing Solutions
for Resident Lifting and Repositioning
Transfer from Sitting to Resident Lifting
Standing Position
Description: Description:
Powered sit-to-stand Portable lift device (sling
or standing assist type); can be a universal/
devices. hammock sling or a band/
When to Use: leg sling.
Transferring When to Use:
residents who are Lifting residents who are
partially depen- totally dependent, are
dent, have some partial- or non-weight
weight-bearing bearing, are very heavy,
capacity, are or have other physical
cooperative, can sit limitations. Transfers
up on the edge of from bed to chair (wheel
the bed with or chair, Geri or cardiac
without assistance, and are able to bend hips, knees, chair), chair or floor to
and ankles. Transfers from bed to chair (wheel chair, bed, for bathing and toileting, or after a resident fall.
Geri or cardiac chair), or chair to bed, or for bathing Points to Remember:
and toileting. Can be used for repositioning where More than one caregiver may be needed. Look for a
space or storage is limited. device with a variety of slings, lift-height range,
Points to Remember: battery portability, hand-held control, emergency
Look for a device that has a variety of sling sizes, lift- shut-off, manual override, boom pressure sensitive
height range, battery portability, hand-held control, switch, that can easily move around equipment, and
emergency shut-off, and manual override. Ensure has a support base that goes under beds. Having
device is rated for the resident weight. Electric/battery multiple slings allows one of them to remain in place
powered lifts are preferred to crank or pump type while resident is in bed or chair for only a short
devices to allow smoother movement for the resident, period, reducing the number of times the caregiver
and less physical exertion by the caregiver. lifts and positions resident. Portable compact lifts may
be useful where space or storage is limited. Ensure
device is rated for the resident weight. Electric/battery
powered lifts are preferred to crank or pump type
devices to allow a smoother movement for the resi-
dent, and less physical exertion by the caregiver.
Enhances resident safety and comfort.
Guidelines for Nursing Homes 19Repositioning in Chair Ambulation
Description: Description:
Variable position Ambulation assist device.
Geri and Cardiac
chairs. When to Use:
When to Use: For residents who are weight
Repositioning bearing and cooperative and
partial- or non- who need extra security and
weight-bearing assistance when ambulating.
residents who are
cooperative. Points to Remember:
Increases resident safety
Points to during ambulation and
Remember: reduces risk of falls. The
More than one caregiver is needed and use of a friction- device supports residents as
reducing device is needed if resident cannot assist to they walk and push it along
reposition self in chair. Ensure use of good body during ambulation. Ensure height
mechanics by caregivers. Wheels on chair add versatility. adjustment is correct for resident before ambulation.
Ensure that chair is easy to adjust, move, and steer. Ensure device is in good working order before use
Lock wheels on chair before repositioning. Remove and rated for the resident weight to be lifted. Apply
trays, footrests, and seat belts where appropriate. brakes before positioning resident in or releasing resi-
Ensure device is rated for the resident weight. dent from device.
Resident Lifting
Description:
Ceiling mounted lift device.
When to Use:
Lifting residents who are totally dependent, are partial- or non-weight bearing, very
heavy, or have other physical limitations. Transfers from bed to chair (wheel chair,
Geri or cardiac chair), chair or floor to bed, for bathing and toileting, or after a
resident falls. A horizontal frame system or litter attached to the ceiling-mounted
device can be used when transferring residents who cannot be transferred safely
between 2 horizontal surfaces, such as a bed to a stretcher or gurney while lying on
their back, using other devices.
Points to Remember:
More than one caregiver may be needed. Some residents can use the device without
assistance. May be quicker to use than portable device. Motors can be fixed or portable
(lightweight). Device can be operated by hand-held control attached to unit or by
infrared remote control. Ensure device is rated for the resident weight. Increases residents’
safety and comfort during transfer.
20 Guidelines for Nursing HomesLateral Transfer; Repositioning
Description:
Devices to reduce friction force when transferring a resident such as a draw
sheet or transfer cot with handles to be used in combination slippery sheets,
low friction mattress covers, or slide boards; boards or mats with vinyl
coverings and rollers; gurneys with transfer devices; and air-assist lateral
sliding aid or flexible mattress inflated by portable air supply.
When to Use:
Transferring a partial- or non-weight bearing resident between 2
horizontal surfaces such as a bed to a stretcher or gurney while lying on
their back or when repositioning resident in bed.
Points to Remember:
• More than one caregiver is needed to perform this type of transfer or repositioning.
Additional assistance may be needed depending upon resident status, e.g., for heavier or
non-cooperative residents. Some devices may not be suitable for bariatric residents.
When using a draw sheet combination use a good hand-hold by rolling up draw sheets or use other
friction-reducing devices with handles such as slippery sheets. Narrower slippery sheets with webbing handles
positioned on the long edge of the sheet may be easier to use than wider sheets. When using boards or mats
with vinyl coverings and rollers use a gentle push and pull motion to move resident to new surface.
• Look for a combination of devices that will increase resident’s comfort and minimize risk of skin trauma. Ensure
transfer surfaces are at same level and at a height that allows caregivers to work at waist level to avoid extended
reaches and bending of the back. Count down and synchronize the transfer motion between caregivers.
Lateral Transfer; Repositioning
Description:
Convertible wheelchair, Geri or cardiac chair to bed; beds that
convert to chairs.
When to Use:
For lateral transfer of residents who are partial- or non-weight
bearing. Eliminates the need to perform lift transfer in and out of
wheelchairs. Can also be used to assist residents who are partially
weight bearing from a sit-to-stand position. Beds that convert to
chairs can aid repositioning residents who are totally dependent, non-
weight bearing, very heavy, or have other physical limitations.
Points to Remember:
More than one caregiver is needed to perform lateral transfer. Additional assistance
for lateral transfer may be needed depending on residents status, e.g., for heavier or non-cooperative residents.
Additional friction-reducing devices may be required to reposition resident. Heavy duty beds are available for
bariatric residents. Device should have easy-to-use controls located within easy reach of the caregiver, sufficient
foot clearance, and wide range of adjustment. Motorized height adjustable devices are preferred to those
adjusted by crank mechanism to minimize physical exertion. Always ensure device is in good working order
before use. Ensure wheels on equipment are locked. Ensure transfer surfaces are at same level and at a height
that allows caregivers to work at waist level to avoid extended reaches and bending of the back.
Guidelines for Nursing Homes 21Lateral Transfer in Transfer from Sitting to
Sitting Position Standing Position
Description: Description:
Transfer boards – wood or plastic Lift cushions and lift chairs.
(some with movable seat). When to Use:
When to Use: Transferring residents who are
Transferring (sliding) weight-bearing and cooperative
residents who have good but need assistance when standing
sitting balance and are and ambulating. Can be used for
cooperative from one independent residents who need
level surface to another, an extra boost to stand.
e.g., bed to wheelchair,
Points to Remember:
wheelchair to car seat or toilet. Can also be used by
Lift cushions use a lever that
residents who require limited assistance but need addi-
tional safety and support. activates a spring action to
assist residents to rise up. Lift
Points to Remember: cushions may not be appropriate for heavier residents.
Movable seats increase resident comfort and reduce
Lift chairs are operated via a hand-held control that
incidence of tissue damage during transfer. More than one
tilts forward slowly, raising the resident. Residents
caregiver is needed to perform lateral transfer. Ensure
need to have physical and cognitive capacity to be
clothing is present between the resident’s skin and the
able to operate lever or controls. Always ensure device
transfer device. The seat may be cushioned with a small
is in good working order before use and is rated for
towel for comfort. May be uncomfortable for larger
residents. Usually used in conjunction with gait belts for the resident weight to be lifted. Can aid resident inde-
safety depending on resident status. Ensure boards have pendence.
tapered ends, rounded edges, and appropriate weight
capacity. Ensure wheels on bed or chair are locked and
transfer surfaces are at same level. Remove lower bedrails
from bed and remove arms and footrests from chairs as
appropriate.
Transfer from Sitting to Weighing
Standing Position
Description: Description:
Stand-assist devices can be fixed to bed or chair or be Scales with ramp to accommodate
free-standing. There is a variety of such devices on wheelchairs; portable-powered lift
the market. devices with built-in scales; beds
When to Use: with built-in scales.
Transferring residents who are weight-bearing and When to Use:
cooperative and can pull themselves up from sitting to To reduce the need for additional
standing position. Can be used for independent residents transfer of partialor non-weight-
who need extra support to stand. bearing or totally dependent
Points to Remember: residents to weighing device.
Check that device is stable before use and is rated for Points to Remember:
resident weight to be supported. Ensure frame is firmly Some wheelchair scales can accommo-
attached to bed, or if it relies on mattress support that date larger wheelchairs. Built-in bed scales
mattress is heavy enough to hold the frame. Can aid may increase weight of the bed and prevent it from
resident independence. lowering to appropriate work heights.
22 Guidelines for Nursing HomesTransfer from Sitting to Standing Position;
Ambulation
Description:
Gait belts/transfer belts with handles.
When to Use:
Transferring residents who are partially dependent, have some weight-bearing
capacity, and are cooperative. Transfers such as bed to chair, chair to chair, or
chair to car; when repositioning residents in chairs; supporting residents during
ambulation; and in some cases when guiding and controlling falls or assisting a
resident after a fall.
Points to Remember:
• More than one caregiver may be needed. Belts with padded handles are easier
to grip and increase security and control. Always transfer to resident’s strongest
side. Use good body mechanics and a rocking and pulling motion rather than lifting
when using a belt. Belts may not be suitable for ambulation of heavy residents or residents
with recent abdominal or back surgery, abdominal aneurysm, etc. Should not be used for
lifting residents. Ensure belt is securely fastened and cannot be easily undone by the resident during
transfer. Ensure a layer of clothing is between residents’ skin and the belt to avoid abrasion. Keep
resident as close as possible to caregiver during transfer. Lower bedrails, remove arms and foot rests
from chairs, and other items that may obstruct the transfer.
• For use after a fall, always assess the resident for injury prior to movement. If resident can regain standing
position with minimal assistance, use gait or transfer belts with handles to aid resident. Keep back straight,
bend legs, and stay as close to resident as possible.
If resident cannot stand with minimal assistance, use a powered portable or ceiling-mounted lift device to
move resident.
Repositioning Repositioning
Description: Description:
Electric powered Trapeze bar; hand blocks and
height adjustable bed. push up bars attached to the
When to Use: bed frame.
For all activities When to Use:
involving resident Reposition residents that have
care, transfer, reposi- the ability to assist the caregiver
tioning in bed, etc., to during the activity, i.e., residents
reduce caregiver bending with upper body strength and
when interacting with resident. use of extremities, who are
Points to Remember: cooperative and can follow
Device should have easy-to-use controls located within instructions.
easy reach of the caregiver to promote use of the electric Points to Remember:
adjustment, sufficient foot clearance, and wide range of Residents use trapeze bar by grasping bar suspended from
adjustment. Adjustments must be completed in 20 an overhead frame to raise themselves up and reposition
seconds or less to ensure staff use. For residents that may themselves in a bed. Heavy duty trapeze frames are
be at risk of falling from bed some beds that lower closer available for bariatric residents. If a caregiver is assisting,
to the floor may be needed. Heavy duty beds are available ensure that bed wheels are locked, bedrails are lowered,
for bariatric residents. Beds raised and lowered with an and bed is adjusted to caregiver’s waist height. Blocks also
electric motor are preferred over crank-adjust beds to enable residents to raise themselves up and reposition
allow a smoother movement for the resident and less themselves in bed. Bars attached to the bed frame serve
physical exertion to the caregiver. the same purpose. May not be suitable for heavier
residents. Can aid resident independence.
Guidelines for Nursing Homes 23Repositioning Bathtub, Shower,
and Toileting Activities
Description: Description:
Pelvic lift devices (hip lifters). Height adjustable
When to Use: bathtub and easy-
To assist residents who entry bathtubs.
are cooperative and can When to Use:
sit up to a position on a Bathing residents
special bed pan. who sit directly in
Points to Remember: the bathtub, or to
Convenience of device assist ambulatory
may reduce need for resident residents climb
lifting during toileting. Device is positioned more easily into a
under the pelvis. The part of the device located under low tub, or easy-
the pelvis gets inflated so the pelvis is raised and a access tub. Bathing resi-
special bedpan put underneath. The head of the bed is dents in portable-powered or ceiling
raised slightly during this procedure. Use correct body mounted lift device using appropriate bathing sling.
mechanics, lower bedrails, and adjust bed to caregivers Points to Remember:
waist height to reduce bending. Reduces awkward postures for caregivers and those
who clean the tub after use. The tub can be raised to
eliminate bending and reaching for the caregiver. Use
correct body mechanics, and adjust the tub to the
caregiver’s waist height when performing hygiene
activities. Increases resident safety and comfort.
Bathtub, Shower, Bathtub, Shower,
and Toileting Activities and Toileting Activities
Description: Description:
Shower and toileting chairs. Toilet seat risers.
When to Use: When to Use:
Showering and toileting For toileting partially
residents who are partially weight-bearing residents
dependent, have some who can sit up unaided,
weight bearing capacity, use upper extremities
can sit up unaided, and are (have upper body
able to bend hips, knees, strength), are able to
and ankles. bend hips, knees, and
Points to Remember: ankles, and are coop-
Ensure that wheels move easily and erative. Independent
smoothly; chair is high enough to fit over toilet; chair residents can also use these devices.
has removable arms, adjustable footrests, safety belts, Points to Remember:
and is heavy enough to be stable; and that the seat is Risers decrease the distance and amount of effort
comfortable, accommodates larger residents, and has a required to lower and raise residents. Grab bars and
removable commode bucket for toileting. Ensure that height-adjustable legs add safety and versatility to the
brakes lock and hold effectively and that weight device. Ensure device is stable and can accommodate
capacity is sufficient. resident’s weight and size.
24 Guidelines for Nursing HomesBathtub, Shower,
and Toileting Activities
Description:
Bath boards and transfer benches.
When to Use:
Bathing residents who are partially weight bearing, have good sitting balance, can use
upper extremities (have upper body strength), are cooperative, and can follow instruc-
tions. Independent residents can also use these devices.
Points to Remember:
To reduce friction and possible skin tears, use clothing or material between the
resident’s skin and the board. Can be used with a gait or transfer belt and/or
grab bars to aid transfer. Back support and vinyl padded seats add to bathing
comfort. Look for devices that allow for water drainage and have height-
adjustable legs. May not be suitable for heavy residents. If wheelchair is used,
ensure wheels are locked, the transfer surfaces are at the same level, and device
is securely in place and rated for weight to be transferred. Remove arms and
foot rests from chairs as appropriate and ensure that floor is dry.
Bathtub, Shower,
and Toileting Activities
Description:
Grab bars and stand assists; can be fixed or mobile.
Long-handled or extended shower heads, or brushes can be used for
personal hygiene.
When to Use:
Bars and assists help when toileting, bathing, and/ or showering residents
who need extra support and security. Residents must be partially weight
bearing, able to use upper extremities (have upper body strength), and be
cooperative.
Long-handled devices reduce the amount of bending, reaching, and
twisting required by the caregiver when washing feet, legs, and trunk of
residents. Independent residents who have difficulty reaching lower
extremities can also use these devices.
Points to Remember:
Movable grab bars on toilets minimize workplace congestion.
Ensure bars are securely fastened to wall before use.
Guidelines for Nursing Homes 25Bathtub, Shower, Bathtub, Shower,
and Toileting Activities and Toileting Activities
Description: Description:
Height adjustable Built-in or fixed
shower gurney or lift bath lifts.
bath cart with When to Use:
waterproof top. Bathing residents
When to Use: who are partially
For bathing non- weight bearing,
weight bearing have good sitting
residents who are balance, can use
unable to sit up. upper extremities
Transfer resident to (have upper body
cart with lift or lateral strength), are cooperative, and can
transfer boards or other follow instructions. Useful in small bathrooms where
friction-reducing devices. space is limited.
Points to Remember: Points to Remember:
The cart can be raised to eliminate bending and Ensure that seat raises so resident’s feet clear tub, easily
reaching to the caregiver. Foot and head supports rotates, and lowers resident into water. May not be
are available for resident comfort. May not be suitable for heavy residents. Always ensure lifting de-
suitable for bariatric residents. Look for carts that vice is in good working order before use and rated for
are power-driven to reduce force required to move the resident weight. Choose device with lift mechanism
and position device. that does not require excessive effort by caregiver
when raising and lowering device.
26 Guidelines for Nursing HomesSECTION IV
A Identifying Problems and Implementing Solutions for
Activities Other than Resident Lifting and Repositioning
Some reports indicate a significant the task, by discussing with employees
number of work-related MSDs in the activities and conditions that
nursing homes occur in activities they associate with difficulties, and
other than resident lifting. (2, 3) checking injury records. Observation
Examples of some of the activities provides general information about
that the nursing home operator may the workstation layout, tools,
want to review are: equipment, and general environmental
■ bending to make a bed or feed a conditions in the workplace.
resident; Discussing tasks with employees
■ lifting food trays above shoulder helps to ensure that a complete
level or below knee level; picture of the process is obtained.
■ collecting waste; Employees who perform a given task
■ pushing heavy carts; are also often the best sources for
■ bending to remove items from a identifying the cause of a problem,
deep cart; and developing the most practical
■ lifting and carrying when receiving and effective solutions. Once
and stocking supplies; information is obtained and problems
■ bending and manually cranking identified, suitable improvements can
an adjustable bed; and be implemented. Finally, there are a
■ removing laundry from washing number of resources available to help
machines and dryers. determine if specific activities have
These tasks may not present the potential for causing injuries. For
problems in all circumstances. example, support is available from
Employers should consider the OSHA’s consultation program,
duration, frequency, and magnitude insurance companies, and state
of employee exposure to forceful workers’ compensation programs.
exertions, repetitive activities, and The following are examples of
awkward postures when determining possible solutions for activities other
if problems exist in these and other than resident lifting and repositioning.
areas. In the vast majority of cases,
job assessments can be accomplished
by observing employees performing
Guidelines for Nursing Homes 27Storage and Transfer of Food, Mobile Medical
Supplies, and Medications Equipment
Description: Description:
Use of carts. Work methods and tools to
When to Use: transport equipment.
When moving food trays, When to Use:
cleaning supplies, When transporting assistive
equipment, maintenance devices and other equipment.
tools, and dispensing Points to Remember:
medications. • Oxygen tanks: Use small
Points to Remember: cylinders with handles to
Speeds process for accessing and storing reduce weight and allow for easier gripping. Secure
items. Placement of items on the cart should keep the oxygen tanks to transport device.
most frequently used and heavy items within easy • Medication pumps: Use stands on wheels.
reach between hip and shoulder height. Carts should • Transporting equipment: Push equipment, rather than
have full-bearing wheels of a material designed for the pull, when possible. Keep arms close to the body and
floor surface in your facility. Cart handles that are push with whole body and not just arms. Remove
vertical, with some horizontal adjustability, will allow unnecessary objects to minimize weight. Avoid obstacles
all employees to push at elbow height and shoulder that could cause abrupt stops. Place equipment on a
width. Carts should have wheel locks. Handles that rolling device if possible. Take defective equipment out of
can swing out of the way may be useful for saving service. Perform routine maintenance on all equipment.
space or reducing reach. Heavy carts should have • Ensure that when moving and transporting residents,
brakes. Balance loads and keep loads under cart additional equipment such as oxygen tanks and IV/
weight restrictions. Ensure stack height does not medication poles are attached to wheelchairs or gurneys
block vision. Low profile medication carts with easy- or moved by another caregiver to avoid awkwardly
open side drawers are recommended to accommodate pushing with one hand and holding freestanding
hand height of shorter nurses. equipment with the other hand.
Working with Liquids in Working with Liquids in
Housekeeping Housekeeping
Description: Description:
Filling and Filling and emptying liquids
emptying liquids from containers.
from containers. When to Use:
When to Use: In dietary when pouring
In housekeeping soups or other liquid foods
areas when filling that are heavy.
and emptying Points to Remember:
buckets with Reduces risk of spills and
floor drain burns, speeds process, and
arrangements. reduces waste.
Points to Remember: Use an elevated faucet or hose to fill large pots. Avoid
Reduces risk of spills, slips, speeds process, and lifting heavy pots filled with liquids. Use ladle to empty
reduces waste. The faucet and floor drain is used in liquids, soups, etc., from pots. Small sauce pans can also
housekeeping. Ensure that casters don’t get stuck in be used to dip liquids from pots. If the worker stands
floor grate. Use hose to fill bucket. Use buckets with for more than 2 hours per day, shock-absorbing floors
casters to move mop bucket around. Ensure casters or insoles will minimize back and leg strain. With hot
are maintained and roll easily. liquids, ensure a splash guard is included.
28 Guidelines for Nursing HomesYou can also read