UNDERSTANDING THE SPATIAL ELEMENTS AT THE TUBERCULOSIS SANATORIA IN SWEDEN: 1887-1942 - DIVA PORTAL
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Understanding the spatial elements at
the tuberculosis sanatoria in Sweden:
1887-1942
Cartography and spatial interpretation through
geography information systems (GIS)
Elisa Serrano
Department of ALM
Theses within Digital Humanities
Master’s Master's thesis (two years), 30 credits, 2021, no.6.
1
Author
Elisa Serrano
Title
Understanding the spatial elements at the tuberculosis sanatoria in Sweden 1887-1942: cartography and
spatial interpretation through geography information systems (GIS)
Supervisor
Britt-Inger Johansson
Abstract
This project aspires to understand the tuberculosis sanatoria in Sweden from the perspective of their
location in space and the interpretation of the characteristics of their landscapes. The study has sorted
the areas of analysis in the following categories: [i] distribution, [ii] altitude, [iii] orientation, [iv]
proximity to the sea, [v] proximity to lakes or rivers, [vi] proximity to train stations, [vii] proximity to
forests, [viii] proximity to towns or hospitals, [ix] proximity to industries. The spatial analysis will rely
on observation and on GIS technology. Two different software have been used, Qgis and ArcGis, but
mainly the first due to its disposition as a free software and therefore available for all and easily
accessible. Thereafter, the results of these analyses have been interpreted in the light of hermeneutical
philosophy, seeking the understanding of each of the parts before understanding the whole, and
interpreting the spatial results in the light of the information about the anti-tuberculosis movement.
Tuberculosis sanatoria cannot be interpreted without the support of medical theories existing
during tuberculosis crisis' times. Sanatoria spatial interpretation is also executed under the premises of
Corner’s essential points across any spatial analysis: [i] the primacy of perception and [ii] the role of
tradition. Considering the primacy of perception, some of the buildings and their surroundings have been
visited “in situ” or studied through photos and images. This supported the understanding of the spatial
elements of the sanatoria. The weight of tradition existing in the sanatoria is strong. The sanatorium’s
environment as an element of the treatment for the patients roots in the 19th century and its hygienic
theories. This influenced the organic architecture movement that encouraged a return to nature in search
of health, fresh air, and well-being during the industrial revolution.
The results proved that many Swedish sanatoria aimed to find good environmental conditions
that supported the fresh-air treatment, in harmony with the medical theories of the times but also in areas
where they were more needed for the working force. They were hardly ever isolated or placed on high
altitude. Supplies like water and heating were generally nearby to provide the sanatoria with the
necessary resources, while other needs could be covered by the proximity to train stations or towns.
Other sanatoria were placed within cities, in search of better facilities and services, but they gave up the
benefits attributed to the clean and fresh air in the patients.
This study shows that spatial analysis has achieved a great understanding of Swedish sanatoria
from a new perspective never developed in Sweden. It has demonstrated a relationship between the
social workforce and health care, and it could have been the start of a strong investment in popular care
in Sweden that has not stopped since.
Keywords S
Sanatoria, Tuberculosis, Spatial Analysis, GIS, Hermeneutics of Space, Social Cartographies.
2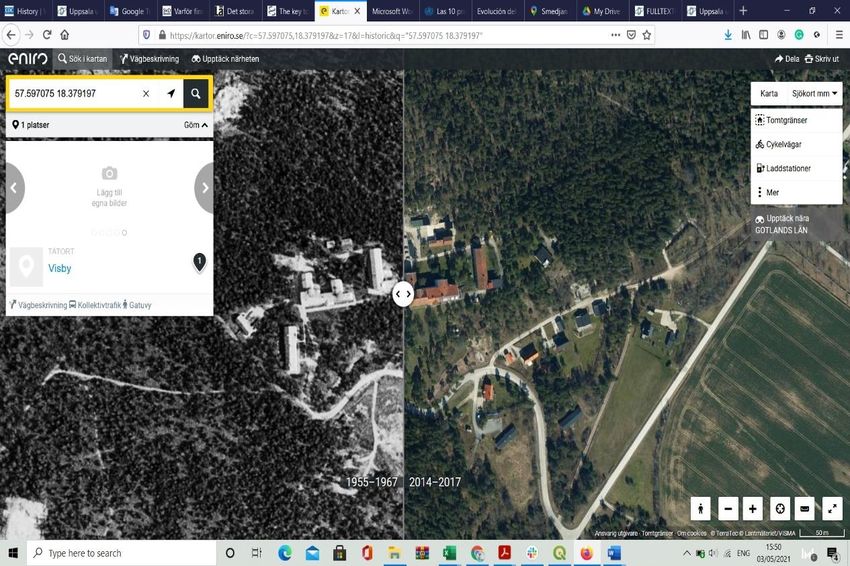
Table of Contents
1. Introduction............................................................................................................... 7
1.19 Research Questions ........................................................................................... 9
1.2 Background ....................................................................................................... 10
1.2.1 Guidelines for the construction of sanatoria in Sweden ............................. 10
1.2.2 Medicine versus sanatoria: a timetable ....................................................... 13
1.3 Literature review ............................................................................................... 15
1.3.2 Tuberculosis and sanatoria in Sweden ....................................................... 18
2. Theoretical basis ..................................................................................................... 21
2.1 Digital humanities and new cartographies. ....................................................... 22
2.2 Space and hermeneutics .................................................................................... 24
2.3 The problem of distribution and communication .............................................. 28
2.4 Space, place, landscape ..................................................................................... 29
3. Methods and Material ............................................................................................. 30
3.1 Data collection and data acquisition ................................................................. 31
3.2 Ethical considerations ....................................................................................... 33
3.3 Data visualization, spatial analysis, and GIS .................................................... 34
3.4 Spatial parameters ............................................................................................. 36
3.5 GIS and data: structures and formats ................................................................ 39
3.6 Limitations of this study.................................................................................... 42
4. Analysis and results ................................................................................................ 43
4.1 Characteristics in this spatial research .............................................................. 43
3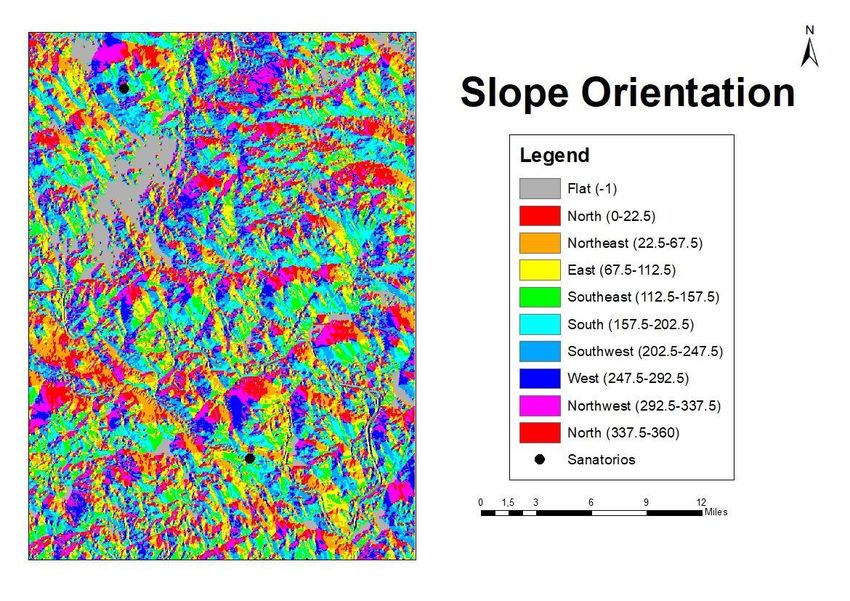
4.2 Process within GIS environment ....................................................................... 46
4.3 Results ............................................................................................................... 49
4.4 Interpretation of the results ............................................................................... 61
5.Discussion and Conclusions .................................................................................... 68
Appendix
Appendix 1………………………….………. Database for the spatial analysis
Appendix 2………...………. Last version of the database (with improvements)
Appendix 3……………..………..…………Photos: daily time at the sanatoria
Appendix 4…………………………………………….…List of collaborations
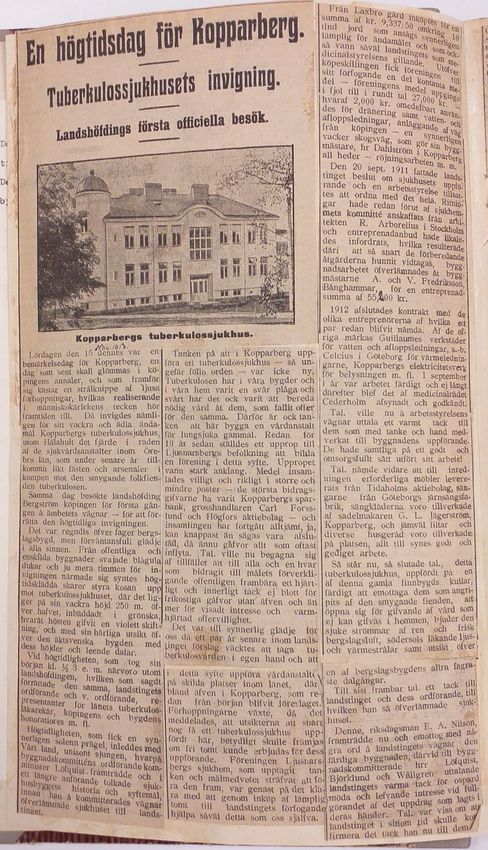
Appendix 5……………………………. News about Kopparbergs inauguration
4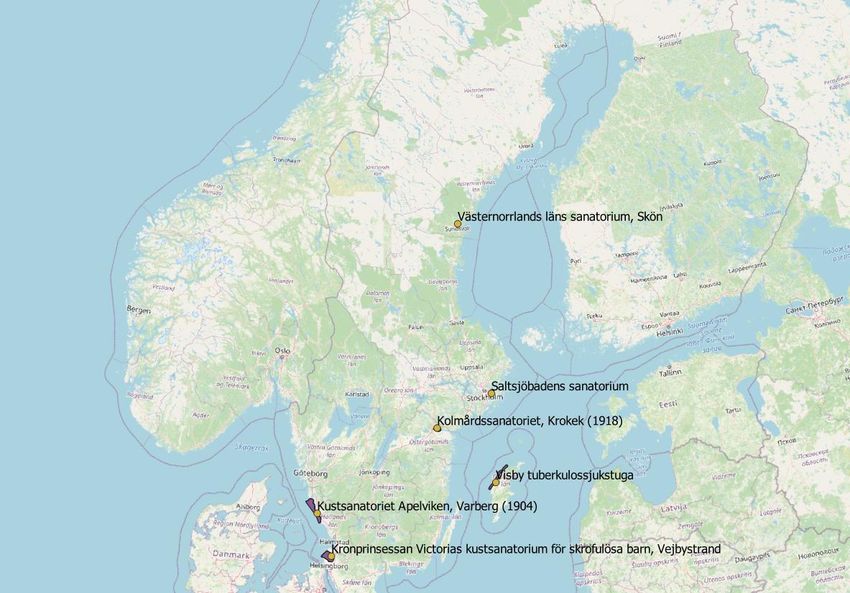
List of figures
Figure 1. Table with the Mortality in the cities because of tuberculosis, 1861-
1900. Retrieve from Puranen, 1984. Page 19.
Figure 2. Table big cities’ mortality rates in cities and countryside. Retrieve
from Puranen, 1984. P. 19.
Figure 3. Tuberculosis rate in the towns depending on their size. Retrieve from
Puranen, 1984. P. 20.
Figure 4. Dstribution of first private Swedish sanatoria. Source: E. Serrano. 20.
Figure 5. Photo of Mohed, Source: Länsmuseet Gävleborg. P. 32.
Figure 6. Distribution of the sanatoria in Sweden. Source: Elisa Serrano. P.33.
Figure 7. Image Types of vector data. Source: Elisa Serrano. P. 40.
Figure 8. Image Types of data GIS. Source: University of Sevilla. Textbook. 40
Figure 9. Old photo. Sandviken sanatorium. In author’s possession. E-mail
from Tomas Hjort to Elisa Serrano, 2021-03-06. P. 43.
Figure 10. Image. Sandviken sanatorium’s current location. In author’s
possession. E-mail from Tomas Hjort to Elisa Serrano, 2021-03-06. P. 44.
Figure 11. Ortophoto of Gotland 1960. Retrieved from GET. P.45.
Figure 12. Map of Gotland. Retrieved from OpenStreetMap. P. 45.
Figure 13. Aerial image of Gotland sanatorium, now and before. Retrieved
from Eniro.se. P. 46.
Figures 14. Map. Slope orientations in Sweden. ArcGis. General image.
Source: Elisa Serrano. P. 47.
Figure 15. Map. Slope orientations in Sweden. ArcGis. Detailed image.
Source: Elisa Serrano. P. 47.
Figure 16. Map. Sweden’s altitude and sanatoria. Qgis. Source: E. Serrano. 49.
Figure 17. Map. Regions of Sweden and distribution of the sanatoria. Qgis.
Source: Elisa Serrano. P. 50.
Figure 18. Map. Sanatoria near the sea in Sweden. Qgis. Source: E. Serrano.52.
Image 19. Photo. Firefighter station by Hålahult sanatorium. Source: Elisa
Serrano. P. 54.
Figure 20 and 21. Map. Old railways in Sweden and sanatoria’s distances.
Retrieve from: the old map of the railways comes from historiska.nu. P. 55.
Figure 22. Hålahult’s sanatorium and its own railway. Photo album of the nurse
Rut Larsson, today Regionarkivet Örebro’s property. P. 57.
Figure 23. Map. Tjärnans barnsanatorium. Retrieve from eniro.se. P. 57.
Figure 24. Photo. Adolfsbergs sanatorium today. Source: Elisa Serrano. P. 58
Figure 25. Map. Eksjö sanatorium, surrounded by forest and by the Gysjön (Gy
Lake). Retrieved from Eniro.se. P. 59.
5
Figure 26. Map. The big People’s sanatoria in Sweden. Source: Örebro’s
Länstidningen 1925, today in Örebro’s Regional Archive. P. 65.
Figure 27. Map. Tuberculosis mortality in Sweden 1911-1926. Retrieved from
Puranen, 1984. P. 66.
Figure 28. Image of metal industries in Sweden 1850 from Yngve Axelsson.
Retrieved form https://www.jernkontoret.se/sv/stalindustrin/stalindustrins-
historia/brukens-lokalisering/?fbclid=IwAR2Z-4OyXkrvgJ8mfhAZfXUSMruxlLH
sNY00z_yNHeU7RiN0SSYJLwoDXCw. P. 68
6
1. Introduction
Among all who died between 1600 and 1800 in Europe, tuberculosis was the cause in
25% of the cases (Center for disease control and prevention, 2016). Mortality by
tuberculosis grew during the 19th century because of the industrialization and the
unhealthy living conditions (Farga, 004). All around the industrialized world,
tuberculosis was out of control and it was referred to as the “white plague” (Wendel in
Farga, 2004). The discovery of the bacteria which caused the disease in 1882, by Dr.
Robert Koch, reported the tuberculosis as a contagious disease and justified the spread
of the sanatoria (Valenzuela, 1896), buildings where the infected people were isolated
and treated according to then current medical knowledge. According to Dr. Valenzuela,
two were the goals of these sanatoria: [i] isolation of the tuberculosis patients, [ii] the
recovery of the sick.
Medical theories affected decisions about where sanatoria should be built.
These theories believed in nature, fresh air, and sun as elements to help the patients
healing (Mondoni et al., 2020; Puranen, 1984; Valenzuela, 1896). It was usual to find
isolation, altitude, forest, or closeness to the sea among the elements that were
demanded for the building site (Frank, 2012; McBride, 1998). These demands were
however problematic from a social point of view, since many of those affected by
tuberculosis had no means to access them, causing increasing in the infection rates
among the poor (Martini et al., 2018; Zubiani in Almeida Gil, 2012; Lindsay, 1897).
So, the place where the sanatoria were built gives us information about the policy that
a country had in matters that influence the fight against tuberculosis.
Despite space and landscape being important elements for the treatment in the
sanatoria they brought complications in the executions, extra cost, and difficulties for
the potential patients of benefiting. Therefore, the purpose of this study is to analyze
the places where the Swedish sanatoria were built, in order to find out how these
elements were balanced overall. The spatial parameters analyzed in this thesis are the
following: [i] distribution, [ii] altitude, [iii] orientation, [iv] proximity to the sea, [v]
proximity to lakes or rivers, [vi] proximity to train stations, [vii] proximity to forests,
[viii] proximity to towns and hospitals, [ix] proximity to industries. These nine
parameters have been considered important by personal observation.
The scope of analysis is Sweden. The Swedish sanitarium movement was easier
to chart because of the time I have lived in Sweden, with access to archives and people
interested in the subject. I was able to visit some of them and, furthermore, I believe
that Sweden needed further studies in the field of sanatoria research. I was very
surprised by the great constructive activity of sanatoria that had taken place in Sweden
7
- Sweden had more than a hundred sanatoria while Spain, for example, with a bigger
population, had only 66 in 1935 (García Librero, 2018) -, and I could not find a
satisfactory explanation.
A lot has been said about the link of space, landscape, treatment, and sanatoria.
Authors like Deborah McBride (1988), Rebecca Le Get (2019), Dave Lüthi (2005),
etc., have based their theories about tuberculosis sanatoria on the importance of the
location and the landscape. All around the world sanatoria have been approached from
their placement, and location and treatment have been linked many times during their
study (Gilbert and Ellis, 2011; Droulia and Tsiros, 2017; Järnfeldt-Carlsson, 1988;
Paniagua Capparrós in Ruiloba Quecedo, 2014). This approach to the Swedish
sanatoria has not previously been significant and the research on sanatoria in Sweden
lacks a general consideration of their locations. This link is however a main component
in the fight against tuberculosis all around the world and this study aims to fill the lack
of spatial analysis in Swedish sanatoria by analyzing location, altitude, landscape, and
other spatial components related to the space and place where they were built. The
development of spatial analysis in Swedish sanatoria was expected to add insights to
Sweden's anti-tuberculosis plan and shed light on the general history of the industrial
revolution, revealing new dynamics from a social health perspective. I am referring to
investment in health and social power in the fight against tuberculosis, bearing in mind
that social progress usually comes from tension, peaceful or not, between social forces
and governing forces (Marx, 1848).
This study brings the spatial analysis to the front of the sanatoria’s study as a
consequence of the industrial revolution in Sweden. It is also innovative in the tools
that executed the analysis as it is grounded on GIS technology. GIS offers the tools to
approach sanatoria in a way that has not been done before, while georeferencing the
sanatoria and overlapping layers with different geography content that gives exact
knowledge of their position in the space. It provides a digitalization of real space that
leads to a cartography of the sanatoria and creates a new method of analysis that could
be applied to study other groups of sanatoria. It is a methodology that consists of
mapping first and then to add spatial information of the places of enquiry to analyze
the interesting parameters over the map, generating an enriched cartography that could
be named social cartography because of the social meaning existing in it. For similar
studies, I would like to call the attention on the considerable work in localizing the
buildings/sanatoria, because these buildings might have disappeared and because the
spaces might have remarkably changed, what makes the task of creating new spatial
data more difficult.
The cartography of the sanatoria is essential if we want to do further analysis. I
have found several difficulties due to the number of sanatoria that have disappeared.
8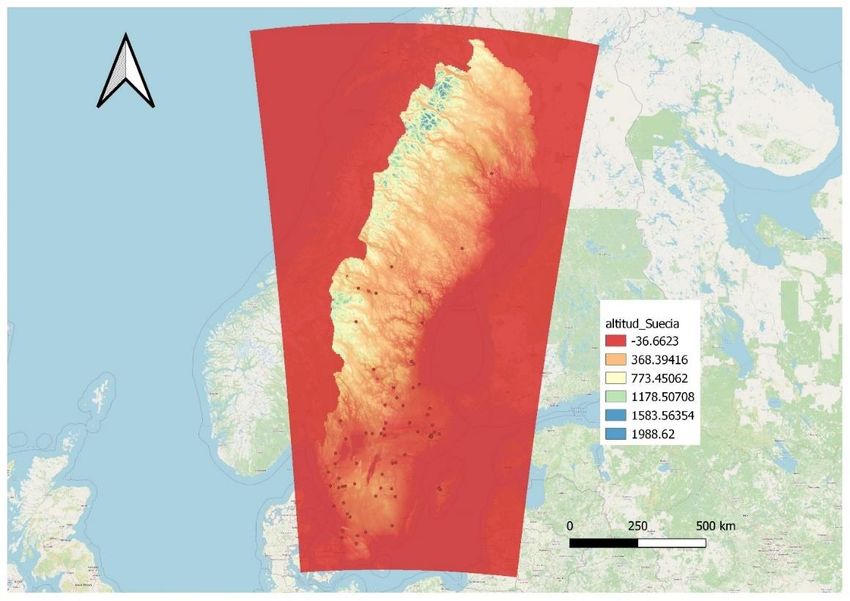
To get locations, I used different means: [i] contact archives, libraries, and museums,
[ii] check a posted list on Wikipedia and corroborating the coordinates on Google
Maps, [iii] traveling to the area and asking the people there, [iv] searching manually on
Google Maps environment. At a first stage, this search gave me a total of 68
coordinates. Within them, I consider a possible error of 3 locations at the most, but,
even when error exists, results would not be affected by them. Because of time
limitations, I needed to start the processing of the data with the 68 sanatoria instead of
continuing the enlargement of my data collection. Few other sanatoria’s locations came
after, together with other interesting information. It generated two different databases:
[i] the first database employed in the analysis (appendix 1), [ii] the final database with
all the information I could collect and which I attached for future research (appendix
2).
Considering this thesis aims to analyze the different spatial elements involved
in the sanatoria movement and interpret them in light of the historical context, spatial
hermeneutics has been considered the most appropriate philosophical lens were to
frame the subject. Hermeneutics of space leads to problematization of space as a
production of humanity (Lefevbre in Grantton, 2017) and its cartography as the
interpretation of humanity’s activity (Ángel Pérez, 2011). Space and its components
will be read as if they were text, considering the context and the agents involved in the
aim of searching for meaning and hidden patterns.
Space is the core of this project that aims to take part of the spatial turn in
history, mixing geographic features and tools in the study of history. I followed the line
of Graves who argued the possibility to create cartographies, not as flat representations
of spatial elements, or mere copies of reality, but as social constructions that revealed
complex dynamics behind (Graves and Teulié, 2017). That is exactly what I aim to do
here.
1.1 Research Questions
This paper wants to respond to the following questions:
How can Swedish sanatoria be described in relation to their spatial characteristics?
What was the spatial distribution and possibilities of communication of the sanatoria
in Sweden?
What characteristics do the landscapes of the sanatoria share and why these
landscapes were the favorite for sanatorium constructions?
9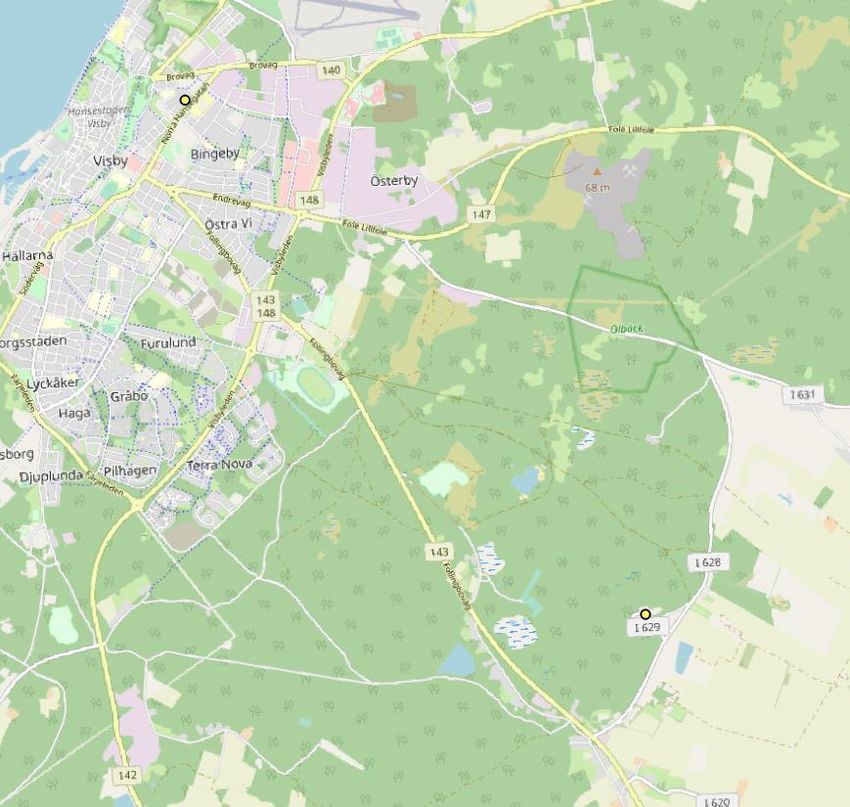
1.2 Background
A book titled “Tuberkulossjukhus: deras planläggning och uppförande : betänkande
och förslag med program, ritningar, kostnadsberäkningar och driftkalkyler” was
published in Stockholm in 1906, and it provided the official advise for the sanatoriaum
constructions that would come after. It was the main official study about construction
recommendations when building sanatoria and makes clear the concerned about the
location of the sanatoria and the complexity involved in the decisions taken about the
building sites. Due to its importance for the subject and for being considered the best
background, I explicitly address it below.
1.2.1 Guidelines for the construction of sanatoria in Sweden
In 1906, the Committee against Tuberculosis published a guideline for the construction
of sanatoria valuing the already existing buildings and describing the elements
considered useful within them. It turned out to be a very interesting document that
valued the sanatoria and their characteristics if these contributed to a successful fight
against tuberculosis. It is also a very international compendium of valuable practices
to fight tuberculosis as it brings examples that cross the Swedish borders, aiming to
analyze what was being done in other countries.
“Till styrelsen för svenska nationalföreningen mot tuberkulos har
lämnat i uppdrag dels att utreda i vad mån olika tuberkulosanstalter i
vårt land kunna sammanföras sinsemellan eller med andra
sjukvårdsinrättningar, dels att utarbeta förslag till ritningar, program och
kostnads förslag för uppförande av enklare vårdanstalter för
tuberkelsjuka.
För fullgörande av detta uppdrag hava kommitterade såväl samarbetat
in pleno som överlämnat åt särskilda subkommittér och enskilda
kommitterade att utreda vissa detaljer i den åt dem anförtrodda
utredningen.
Kommitterade have uppdelat sitt betänkande i tvenne
huvudavdelningar. Den förra omfallar dels frågan om kombination av
tuberkulossjukhus med andra sjukvårdsantalter, dels ett allmänt hållet
program för enklare tuberkulosantalter. Den andra avdelningen utföres
av speciella program, ritningar m. m. för några större och mindre
tuberkulossjukhus.
10Såsom resultat av sitt arbete få kommitterade härmed vördsamt
överlämna hosföljande skrivelse jämte bilagor” (Wawrinsky et al.,
1906)
This is the beginning of the book “Tuberkulossjukhus : deras planläggning och
uppförande : betänkande och förslag med program, ritningar, kostnadsberäkningar och
driftkalkyler”, signed by R. A. Wawrinsky, Carl Dahlborg, Hugo Hammarskjöld, R.
von Post, E. Stenhammar, Anna Westman. This introduction is providing interesting
information to understand the situation before the increase in the number of buildings
that came after 1910. The second decade of the 20th century became the most prolific
construction period.
Among the authors of the official guidelines, see above, one finds E.
Stenhammar’s name. He was the only architect within the group, and he was an
experienced hospital architect who participated in the design of St Göran Hospital in
Stockholm (1906) and the sanatorium in Kolmården (1918). The existence of an
architect who specialized in hospitals is an important fact that shows the evolution of
the medical science towards hygienic conditions and points out the concerns in the
building of healthy hospitals to fight the infections and pandemics. At this point, it is
interesting to remember how unhealthy hospitals in the 19th century were, a topic that
will be considered later.
This introduction of the guidelines presents the state’s concern about expenses
in sanatoria’s maintenance. The topic will be treated in that book as a need to reduce
costs. We should think of the impact of an ideal sanatoria from the economical
perspective: a building constructed in nature and far away from other people’s living,
if possible, on top a hill to get altitude. This means the availability of train services in
the nearby area, which involves tracks and stations. Also, roads from these stations to
the building. They needed water and a sewage system for dirty water. This became
more expensive to build the further the building was from the existing infrastructure.
Food was one of the pillars in the treatment. Guidelines said food had to be
healthy and abundant. This made it important to have access to food distribution or
even to food growing in gardens and farms, turning the cost of food into high expenses.
Being an independent sanatorium far from everything would necessitate hiring several
professionals that would work and live in the place and had no chance to cover other
hospitals. In the light of this analysis, it is understandable the intention of the
government to establish a net that merged different healthcare institutions and allowed
to save money.
The economic situation in Sweden mirrors well the experts’ opinions about the
sanatoria. Sweden was a poor country with increasing factory development but very
low social investment (Kuuse and Dahlin, 2005). The need of workers was high due to
11the growing industrialization, but the taxes were not sufficient to grant their good
health. In the light of the historical context, it is understandable the publication of
official guidelines advising to be pragmatic when building the sanatoria.
The board of the Swedish Committee against tuberculosis was committed to
design plans and proposals for future constructions based on the experience of the
previous sanatoria. This was an engaging task as the experience of previous
constructions was not limited to the Swedish borders, but other countries’ experiences
were taken as examples. Some of the conclusions addressed by the experts in the
guidelines are addressed below.
1. Isolation: the board asserted the inconvenience of keeping the tuberculosis
patients together with other patients, arguing the contagious character of the
tuberculosis. This fits with the discovering of tuberculosis’ bacteria made years earlier
by Dr. Robert Koch, that changed the situation completely as tuberculosis was taken
as a hereditary disease, among other misconceptions. Besides the convenience of
separating tuberculosis patients, they also agreed in the need to leave sanatoria open
for those patients with chances to survive, consequently the board advised that those
with a very severe condition were kept at their homes. This removes the idea of
sanatoria as isolation places and underlines their goals as treatment and healing places.
2. Education was an essential part of the treatment, digging into the hygienic
practices of the patients looking for a continuity of these habits after they left the
sanatoria. Fresh air, proper food, exercise, open spaces, and ventilation were the basic
elements within the education received. A critical approach to this educative program
points out the suitability of non-urban locations because it helped to value hygiene and
the ventilation of the lungs by resting and exercising in the fresh air and in clean
environments, while food or other needs could be distributed from other places or being
grown at the sanatoria.
3. Forests were desired in the proximity of the buildings, preferably pines,
where the sun had long exposure and there were shadows to get protection when
needed. These spaces were modified to create paths for nice walks. Due to the weakness
of the patients, these paths should be easy to walk, flat and comfortable.
4. They would be cheaper if combined with other hospital institutions than if
they are put out by themselves. It was pointed out a possibility to have the sanatoria
within the hospital if the hospital had not much traffic and a park nearby. If the area of
the hospital fulfilled the requirements of a sanatoria, then it would be beneficial to share
doctors, nurses, and other staff. “Be careful to let the best become an enemy of the
good.: if it is good enough, even though it is not the best, it can work”. If there were
resources, it was best to build them in the countryside and be self-sufficient. But the
economical aspect played a big role and it could be wise not to skip the possibilities to
12combine the sanatoria with other hospitals. Besides, it was difficult for the countryside
sanatoria in terms of salaries, as the number of patients could vary but the employer
had a regular staff to pay.
To conclude, the ideal location, according to the guidelines is this: Countryside,
on a hill’s slope to the south with protection against the wind of the north. High and
dry terrain with access to good water. Not close to big roads, not close to railways or
factories. Not a windy or cold position. It is important to think on how fragile these
patients were and how bad the wind was for the breath. It was important for them to
feel they could be outside as much as possible to feel better. A good rule according to
the Committee was to limit the number of patients, no more than 100. “Having too
many patients is not good”. Rooms should have lights and bright colors and should also
face south to get better climate conditions. The committee admits the possibility of
using old buildings by fixing regular houses into tuberculosis hospitals.
1.2.2 Medicine versus sanatoria: a timetable
I consider it important to have a space that deals with the medical theories referring
tuberculosis which existed from 1890 until 1940. 1890 is set as the beginning of the
period of analysis because it is near the year of construction of the first sanatoria in
Sweden. 1940 is the end of my approach to the medical theories about tuberculosis as
it is the moment that sanatoria started to be unoccupied. As scientific knowledge related
to tuberculosis increased, the treatments applied to heal the tuberculosis changed and
therefore sanatoria, that were very linked to the treatment process could also be affected
by science’s evolution. Doctors were very involved in the sanatoria since before their
construction, by applying their knowledge to the general plan, so it might be possible
that the history of sanatoria construction mirrors this evolution of the medical theories.
The following information contains important dates and important events to
consider when assessing the space where the sanatoria were located. It aims to be a
reminder for the reader about how medical science evolved and changed the perception
of the sanatoria.
1804: Laennec found out that the tuberculosis caused caves in the lungs
(Roguin, 2006).
1836: George Bodington, English pulmologist, established the first European
sanatoria in Birmingham, which model did not succeed but had an impact in the
consideration of special buildings to treat tuberculosis (Cyriax, 1941).
1854: The construction of the first sanatoria in Silesia. The doctor Herman
Brehmer started a treatment based on his belief in altitude, fresh air, sun exposure,
exercise, and abundant food as supportive elements in healing. He based this treatment
on his own experience from when he got tuberculosis himself but got better during his
13trip to Himalaya. His student, Peter Dettweiler, would continue this treatment but
would change the exercise by long time resting in horizontal position and in outdoor
space.
1870: Doctors became aware of the benefits of ultraviolet light against bacteria,
boosting the long-time exposition to the sun (heliotherapy). The northern countries in
Europe applied artificial light treatments during the winter (Mondini et al 2017)
1874: Dr. Dettweiler, patient and student to Dr Brehmer, opens the first
sanatoria for people without economic resources and commits the treatment of
tuberculosis with the therapy of lying down and protected by a roof which will prevail.
This sanatorium was in Falkenstein.
1882: discovering the tuberculosis bacillus by Dr. Robert Koch: the beginning
of the end in the perception of tuberculosis as a hereditary disease and the beginning
of the end of tuberculosis itself.
1887: The first known sanatoria is opened in Sweden. It was a private premise
located in Gothenburg which goal was to attend women from that area with no means,
although the attention could be extended to other women from other areas.
1891: Dr Torkel Horney opens Mörsil sanatorium, introducing Sweden into the
German sanatoria-movement by establishing the fresh air treatment and the laying
resting time as the main path to follow. Torkel Horney had worked in Germany, where
he got in contact with the Berhmen's and Dettweiler's medical theories about
tuberculosis treatment.
1899: Dr von Unterberger called attention to the lack of results in the traditional
sanatoria treatment during the Conference on Tuberculosis in Berlin, opening the field
to new alternatives to consider such as putting the sanatoria in or closer to the towns
(Eylers 2014)
1900: Hålahults sanatorium opens as the first Jubileum-sanatorium with the
funds from Oscar II's anniversary foundation. It was the first of a series of sanatoria
paid with royal money that enlarged the number of beds available due to the
construction of big and well-equipped sanatoria. After Hålahults sanatorium, Hässleby
and Österåsens sanatoria were built in 1901, and Spenshults sanatorium in 1913.
1904: The National Association Against Tuberculosis was created, resulting in
an efficient tool to get funds necessary to promote new sanatoria and support the
existing ones, and to support the knowledge and education in tuberculosis’ matters.
1921: Due to a general debate about how efficient the sanatoriaum therapy was,
a study in 4.067 patients was done comparing people treated in sanatoria with people
treated at home. Sanatoria treatment resulted in higher rates of healing (Lissant Cox,
1923).
1921: the vaccine against the tuberculosis is discovered. The cases of
14tuberculosis decreased widely in the world.
1944: the antibiotic streptomycin was successfully applied in the treatment
against tuberculosis. Sanatoria start to disappear or to change their uses.
1.3 Literature review
1.3.1 The history of tuberculosis and sanatoria
This project roots in the tuberculosis disease that overwhelmed the world parallel to
the industrial revolution during the 19th century and the first half of the 20th century.
Although tuberculosis is estimated to have been with us for at least 10000 years (Pérez
Cruz et al., 2009), it was the pollution and bad-living conditions intrinsic to the factory
work and the growing of population in the cities that prepared the perfect field to spread
the bacteria. This caused the construction of special buildings focused on the control
of the disease. These were called sanatoria and followed construction guidelines that
will be analyzed in this paper, which aim is to study the locations of these sanatoria in
Sweden and the reasons that explain their locations.
In this anti-tuberculosis fight, countries took different paths and decisions. I
would like to point out two of the most surprising practices. In the middle ages, France
thought that the king had the power to help in the healing of the sick by touching their
heads (Pérez Cruz et al., 2009) A different perspective was seen in Spain, a country
that started to suspect the contagious character of tuberculosis early on. It is possible
to read early laws concerning hygiene in the cities in the 18th century, which
commanded the destruction of all the belongings of the person if he or she had died out
of tuberculosis (Jori, 2012).
The lack of knowledge about the disease helped a lot in the spreading of the
disease. The World had to wait until 1882 to know that the real cause was a bacteria,
the tuberculosis-bacillus discovered by doctor Robert Koch. This revolutionized the
fight against tuberculosis by adding isolation of the sick and novel hygienic practices
to the treatment. Until this moment, treatments were based on old-fashioned erroneous
ideas as for example a suspected inherited condition or genetic predisposition
(Carbonetti, 2008; Puranen 1984). Because of these wrong conceptions, infected
people lived with healthy people who would easily end up contaminated, a situation
made worse by the lack of hygiene and the unhealthy share of space.
Tuberculosis, however, affected all sorts of social classes, from homeless to
kings, and had a strong impact on the society. To be famous or rich could help to live
in healthy conditions, but even a short time contact with the bacteria could be fatal.
Anne, Charlotte and Emily Brontë, Chopin, Eugene Delacroix, George Orwell, Antón
15Chéjov, all died of tuberculosis, depriving society of their late works. Alfonso XII king
of Spain died out of tuberculosis; many historians think he got infected during one of
his visits to prostitutes (Queralt, 2018). Despite having all the commodities, the only
way to be safe was isolation. Under these circumstances, the big investments in fighting
tuberculosis that were made in the second half of the 19th century are understandable,
when social rights became to be considered.
The treatment against tuberculosis has passed through different moments based
on the scientific knowledge available, though it is in 1882 when we can see a real break
with old-fashioned ideas. Even before the discovery of the bacteria, experts suspected
the importance of clean air and a good diet (Frank, 2012; Pérez Cruz et al., 2009),
treatments that can be tracked back until the Roman Times. That is why infected people
left the big cities in hope of healing. This created a health-tourism where people from
different social and economic conditions spent long periods of time in natural
landscapes breathing clean and fresh air. People who belonged to high social class
rented houses or spent these periods in hotels as the one in Mörsil, while others with
fewer resources could settle in tents, as Gilbert and Ellis reported to happen in New
México and Arizona (2011). But the discovery of the contagious character of the
disease led to the sanatorium movement which attempted to contain the spread of
tuberculosis by removing the sick from society and confining them in sanatoria
(Carbonetti, 2008).
These sanatoria proliferated all over the world because of the need to control
the pandemic. Patients’ staying time varied a lot from a few months up to years
(Wallstedt and Maeurer, 2015). It is difficult to imagine how this long stay affected
those living there emotionally, although there are few examples of real cases where
real patients have written about their sanatoria-time. An example is the text by
Raymond Hurt that reproduces parts of a female patient's diary during her recovery
time in the sanatoria (2004). She described the atmosphere of fear and fight surrounded
by a strict daily schedule in what consisted of treatment against tuberculosis.
Testimonies as hers are very valuable today to construct an understanding of the time
in the sanatoria, where people, completely isolated from society, lived under strict rules
to promote healing. There are also plenty of photos, where it is possible to see smiling
patients, engaged in conversations, walks, readings or even costume parties (see
appendix 3) The number of patients was large, and it explains the diversity of feelings.
The growing body of knowledge about tuberculosis affected the treatments
available. In 1854, the German doctor Hermann Brehmer opened one of the first
European sanatoria at Görbersdorf in Silesia, built at a height of 569 meters to develop
what was called the “hygienic-dietetic treatment”. He thought this treatment allowed
to heal tuberculosis in a high percent when it was applied at the beginning of the
16infection, helped by long time stay in sanatoria built in high altitude, as that air was the
best in his consideration and helped in the cleaning of the lungs due to the lower air
pressure (Eylers, 2014). His patients were prescribed the following activities: exercise,
resting, clean and abundant air, high protein, and varied food and, heliotherapy
(consisted in direct exposure of the body to sunlight). From this experience, other
sanatoria were in high altitudes. Thalassotherapy was also recommended (therapies
based on sea water’s benefits and the sea environment in general), and when possible,
sanatoria were built by the sea to enjoy the benefits (Pérez Cruz et al., 2009). It had a
lot to do with the lack of proper ventilation and sanitation in times when hospitals were
pointed out as dangerous places for the patients due to the uncontrolled infections
within their walls (Turnes, 2009).
Brehmer advised exercise as a main activity during treatment. Peter Dettweiler,
changed this perspective by advising passive-resting therapy and built a sanatorium in
1874 near Frankfurt. Dettweiler, who also had been a patient to Brehmer, did two
revolutionary changes in his sanatoria: [i] he changed the exercise therapy to a
horizontal position resting therapy, as this position was supposed to help the lungs in
the breathing, [ii] his sanatoria was orientated to people with no means, creating
opportunities of healing to the poor and calling the attention on a social need (Eylers,
2014 and Ruiloba, 2014). His horizontal position resting therapy succeeded, and the
buildings were planned with long open galleries for the purpose of enabling the patients
to rest in open air, becoming one of the most common features of the sanatoria.
From the beginning of the sanatoria movement, many of them aimed to be
constructed in natural areas which would be positive for the healing of the patient. This
must be approached from two different perspectives. First, the belief in fresh air as a
tool for healing. Second, the patients’ long stay in the sanatoria, which made the
thinking of surroundings and projecting of beautiful views in the shape of gardens and
nature an important part of the building itself. It is therefore interesting to approach the
buildings from a spatial perspective to know more about the reasons that guided the
decision of their final location. These treatments could not be scientifically proved,
although they decreased the number of deaths (Lissant Cox, 2006). Today we know
they were indirectly efficient as they improved the patient’s defenses, preparing the
body for a better fight against the bacteria by promoting ventilation (Díez Ruiz-
Navarro, 2021).
In Germany, new knowledge according to Eyler (2014) gave way to critical
positions towards the suitability of locating sanatoria in natural isolated spaces and
allowed a net of sanatoria with locations based on other criteria such as population
distribution, creating a sanatoria network that covered the country from a more social
fair perspective.
17The 20th century would bring the biggest improvements in the treatment of
tuberculosis that would finally take the sanatoria institutions to an end in the second
half of the century. The vaccination against tuberculosis was fully ready in 1921, and
1944 brought the streptomycin, the only efficient treatment against the bacteria. 1944
was the year when an infected woman was successfully treated with antibiotics and
completely cured for the first time in history, making the sanatoria’s therapy
unnecessary. However, the mycobacterium tuberculosis has not disappeared, and it
remains one of the main causes of death in the world (WHO, 2020)
1.3.2 Tuberculosis and sanatoria in Sweden
Tuberculosis mortality increased in Sweden together with the industrialization of the
country, which in Sweden happened around 1870 (Puranen). But from the 1880 it is
possible to see a decrease in tuberculosis urban mortality in statistics. Statistics also
showed that tuberculosis’ mortality was higher in the cities than in smaller towns until
1900, when tuberculosis mortality rates quickly decreased among the urban population
which led cities to have a lower tuberculosis mortality than the rural populations in
1930 (Sundbärg in Puranen).
In the tables below it is possible to see [i] the evolution of mortality and lung
mortality in urban and rural areas compared with each other.
Figure 1. Sundbärg, G in Puranen, 1984
Tabell 27. Big cities’ mortality rates compared to the countryside. Countryside = 100.
År Index År Index
1816-40 155 1871-80 139
181841-50 146 1881-90 121
1851-60 150 1891-00 108
1861-70 135
Figure 2: Table big cities’ mortality rates in cities and countryside. Source: Runborg, C. &
Sundbärg, G., (1905), in Puranen 1984
Swedish industrialization had strong rural character because of the iron industry but
also paper or wood industries. This caused the rural population around these industries
to grow, and it might explain the high tuberculosis mortality in the rural areas.
Sweden opened its first sanatoria in 1887, a small private sanatorium in
Gothenburg (Hulter Åsberg, 2021), and the second and more embedded into the
European movement at Mörsil in 1891 (Åman, 1976) and, immediately after, other
sanatoria were built. They were not built in the most populated or affected areas as
could be Stockholm or Malmö. Big cities had the highest incidence of tuberculosis at
the time and were therefore in big need of help. In the table below it is possible to read
how the tuberculosis affected the towns depending on their size.
Figura 3. Runborg,C. and Sundbärg, G., in Puranen, 1984
Little has been written about the reasons that motivated the constructions of the
sanatoria in their final emplacement. For example, Mörsil’s sanatoria was built by Jon
Jonsson Mankel and his relative Dr Torkel Horney. The latter had visited sanatoria in
Germany and Switzerland and wanted to bring the model and the sanatoria’s therapy
to Sweden, in an area in Jämtland where they could reproduce the German treatment.
Shortly after, a second sanatoria was built in Ryd because of the existence of water
enriched in iron, which was thought to be efficient against tuberculosis. Patients drank
19and took showers with metal-rich water (Fredriksson, 2013). This suggest to me that
these first Swedish sanatoria were linked to the spatial environment where they were
built.
The first sanatorias built in Sweden were private buildings built by companies
or private entities (Järnfeldt-Carlsson, 1988), and all of them had a low capacity of
attention due to their small size. This represented an insufficient capacity to deal with
the number of infections in the country and great inequality, since people with means
could travel to other countries to be treated, but the average citizen could not. Besides,
people with no means had few chances to travel to the first sanatoria as they were not
in the cities and it was necessary to travel, generally by train. In the map below it is
possible to get an idea of the distribution of these first private Swedish sanatoria.
Figure 4. Source: Elisa Serrano
In 1904 the National Assembly against Tuberculosis was founded, providing Sweden
with an official governmental body to fight tuberculosis. This meant more investments
in the construction of sanatoria that was reinforced with another law against
tuberculosis in 1938 (Fredriksson, 2013). There are, however, two earlier examples of
public institutions against tuberculosis in Sweden established in cities, one in
Stockholm, the Paviljong för bröstsjuka at Sabbatsbergs sjukhus in Stockholm, housing
32 patients, built in 1899; and a few years after, Akademiska Sjukhuset in Uppsala.
They were real sanatoria, but they belonged to public health care institutions (Åman,
201976).
The beginning of the 20th century meant an explosion of sanatoria in Sweden.
Among the first are the sanatoria that are called the “Jubileums-sanatorierna”, three
public sanatoria that were built with the money gathered for the king Oscar II in
celebration of his 25 years anniversary as king of Sweden. After, and with the support
of the National Assembly against Tuberculosis, a lot of new buildings were made or
reused as tuberculosis sanatoria, possibly as many as roughly one hundred that gave
service until the tuberculosis was defeated.
Apart from the sanatorium, other interesting entities existed in Sweden to fight
tuberculosis. These entities were smaller places where patients did not live but attended
during the day, many times within the cities, where people got education and
knowledge to fight tuberculosis. The experience was taken from London and Germany,
where the development of small dispensaries had supported the sanatoria easing their
workload and developing education and assistance practices (Wawrinsky at al 1906).
The dispensaries were a cheap and easy means to support the sick or people around,
giving education to prevent the infection and stimulating the medical support with the
sufferer at home.
2. Theoretical basis
The theories behind this project are diverse, covering different thematic areas: [i]
digital humanities as an efficient approach to the means of the cartography of the
sanatoria and, [ii] hermeneutics of space, understood as a modern wave of the
hermeneutics affected by the “spatial turn” in humanities and social sciences that focus
the efforts in understanding the problematic in perception and interpretation of space.
These theories merge here to provide deep and strong roots to the spatial study of the
sanatoria. As an epilogue to the section, I will try to mirror my thoughts about the
terminology implied that covers the geographical concepts “space”, “place”, and
“landscape”, to avoid misconceptions and give a theoretical perspective to the diversity
of the contemporary scientific terminology.
212.1 Digital humanities and new cartographies.
Digital humanities (Dh) is “anything that combines digital work of any sort with
humanities work of any sort” (Golumbia 2013, p.1) According to this definition, it is
possible to frame this project under the spirit of the digital humanities, mainly grounded
in the use of geography information system’s technologies. This is, however, not the
only digital work existing in the different steps of work. It contains other digital tasks
such as online searching, digital archive consultation, and collaborative participation.
However, would this project be considered as a digital humanities’ work by everyone?
The answer is complex, and I try to explain why below.
As Svensson addressed (2009), the object of study in the first wave of the Dh
was text, resulting in a very specific area of research. These two legs of the humanities
computing, [i] new computer tools, [ii] text-based studies, were soon enriched with
other elements together with the evolution of the field. New topics, new tools, and new
perspectives. After this first wave that started around 1950, Dh evolved pushed by a
growing interest towards the behavior online (Berry, 2011), changing completely the
perspective of some “modern” digital humanists.
Different visions of the field have made it difficult to define the discipline,
although today many are claiming to keep an inclusive perception where both the
technological part and the new behaviors are given room: “Only if you care more about
boundaries than results would you want to try to distinguish whether these people are
or are not DH, rather than looking at the results they produce” (Golumbia, 2013)
A pillar of the Dh that is being successfully applied in new ways of research is
the quantitative approach to the studied topic. What does a quantitative perspective
include? I would say that it includes all sorts of elements that can be measured. This
way, it is possible to point out two different methodological theories traditionally
known as qualitative and quantitative. The differences between these two traditional
types of research are several: [i] the type of data used in the project, [ii] tools applied
to collect data, [iii] the type of analysis, [iv] the organization of the data (Ángel Pérez
2011). Ángel Pérez also states that the quantitative or qualitative character of the data
is, however, not what defines a research as positivist but the insistence in regularities
that deny singularities. Gadamer went further and said that validity criterion does not
rely on methods (Gadamer 1960), leaving the field based on quantitative research open
to reflection and interpretation.
By bringing positivism to the stage, I aim to unlink this thesis from it, as it could
be understood as positivist due to the results provided in long list of facts. Research
that follows a positivist approach to knowledge basing the truth on the number of
feasible data, does not develop a deep interpretation of facts or context, but remains in
the explanation of data (Pérez Villamar, 2015) According to the positivist perspective,
22only the objects as mathematical and logical source of data are means to reach the truth
(Adler, 1964 in Villamar 2015, Landeros-Olvera et al 2009). In response, philosophy
provided other methodological streams at the end of the 19th century and beginning of
the 20th (Pérez Vilamar, 2015).
One of the movements against positivism was hermeneutics, which has a
special weight in this project as it sets the basis of its theoretical understanding and the
problematization, due to the force that interpretation and comprehension of data have
in its basis (Herrera and Ángel Pérez, 2011). An interpretative character has been
applied in religious texts since the Middle Ages (López, 2018). In the spirits of the Age
of Enlightenment, the German philosopher Friedrich Schleiermacher (1768-1834),
considered by many as the father of the modern hermeneutics (Echeverría, 1997;
Coreth 1972), took hermeneutics out of the religion’s field, enriching the interpretation
with reasons out of God’s making. He addressed the need to know the author and the
movement or group behind the author to completely understand the message (of a text),
as an attempt to build a critical system to reach a real understanding. The reception of
the information is no longer sufficient, but the interpretation according to the context
is necessary. From Heidegger, interpretation is seen as an ontological part of human
beings (Angel Perez and Herrera, 2011). Interpretation becomes an ontological skill,
not a process, and it is innate to human beings. It happens in the frame of existence
where people first comprehend the world and, based on a comprehension manipulated
by their position in the world, can interpret it (Whitney, 2011). Gadamer continued the
development of the hermeneutics. He wrote his major work in 1960, Truth and Method
where he constructed a critique against the method. Methods must be tools to reach
the truth, not paths to strictly follow. I consider this essential in this thesis where the
main method is not unique, and other ways of analysis have been used to unveil the
truth.
Late hermeneutics philosophers have focused their interest on interpretation as
a way of understanding social phenomena (Herrera, 2009). It was the case of Gadamer
or Heidegger, and other social philosophers in the second half of the 20th century.
Within the social sciences methods supporting a hermeneutical approach it is possible
to find social cartography, a mapping method that aims to interpret a territory (Ángel
Pérez, 2011). Social cartography does not copy the land but interprets the existing
elements on the space, where space must be read and interpreted as if it was text, a
metaphorical but also illustrative glance to social cartographies that transforms space
into text, the traditional object of the hermeneutics, and leads to a new theoretical
stream that will be approached in the upcoming section: the hermeneutics of space.
232.2 Space and hermeneutics
History has traditionally been the study of men in their time, as time is an element that
changes men’s goals and determines their position in the world (Izuzquiza, 2004).
Space, however, changes men as much as time and it is an existing element in each
historical moment. There is no time without space although traditional history narrative
has insisted on organizing history according to a taxonomy based on years and
centuries. This way, the author C. Castoriadis identified the character of being as the
character of time (2002). This started to change about thirty years ago, with a “spatial
turn” within humanities and social sciences (Graves and Teulié, 2017) M. Foucault
affirmed that time is presented as a dimension of space (1999), removing the
independent existence of time, that, as it has been addressed above in Castoriadis,
remains in some. Due to this opening in the perspective, humanists broke the borders
of their discipline and entered areas traditionally belonging to geographers.
Historiography did experience the “spatial turn” long ago. In 1849, the British
historian Thomas Babington Macaulay wrote “Could the England of 1685 be, by some
magical process, set before our eyes, we should not know one landscape in a hundred
or one building in ten thousand [...] The country gentleman would not recognize his
own fields. The inhabitant of the town would not recognize his own street […]”
(Babington Macaulay in Guldi 2011). He was considering the changeable character of
space as a need to study from his discipline. This spatial perspective did not succeed
and remained a secondary approach until recent times.
Changes continued in the history studies as a continuous effort to keep history
into the scientific discipline and went through important shifts across the 20th century.
An important milestone in the field is the Annales School where historians became
aware of the historiography as an interpretative act (Sanchez Delagado 1993). Soon
after, there was an agreement in the interpretative character existing when approaching
historical narratives (White, 1973; Carr, 1961). This makes History a discipline very
influenced by hermeneutics, understood as the philosophy that searches the real
meanings hidden behind the different channels of communication.
It is here, in the conjunction of space and its interpretation, where the
hermeneutics of space happens, and space is understood as a production (Lefebvre in
Grantton 2017), i.e., if space is a channel for history communication is because it can
be the result of men’s activity. There are dynamics that exist behind the space and that
stamp their own history on the territory and landscape (Ángel Pérez 2011). These
dynamics have different origins, as might it be a wish (of beauty in the landscape), the
war (and its power of destruction), a pandemic (and its need for hospitals). Men have
the skills to modify the territory, and the cartography of these changes is the
interpretation of the activity of men, involving interpretation as a need to comprehend,
24You can also read