UL Hospitals Group Operational Plan 2018 - HSE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

UL Hospitals
Group
Operational
Plan 2018

Contents UL Hospital Group.......................................................................................................................................... 1 UL Hospitals Group Operational Plan 2018..................................................................................................... 2 UL Hospitals Group CEO’s Priorities 2018 .................................................................................................. 3 Governance UL Hospitals............................................................................................................................... 5 2017 Activity .................................................................................................................................................. 7 Unscheduled Care ...................................................................................................................................... 7 Scheduled Care .......................................................................................................................................... 8 Section 1: Introduction and Key Reform Themes.......................................................................................... 10 Section 2: Our Population ............................................................................................................................ 12 Section 3: Building a Better Health Service .................................................................................................. 15 Section 4: Quality and Safety ....................................................................................................................... 20 Section 5: Service Delivery........................................................................................................................... 25 Section 6: Improving Value .......................................................................................................................... 35 Section 7: Finance........................................................................................................................................ 38 Section 8: Workforce .................................................................................................................................... 41 Section 9: ULHG Corporate Strategy ............................................................................................................ 46 Appendices .................................................................................................................................................. 48 Appendix 1: HR Information ....................................................................................................................... 49 Appendix 2: Scorecard and Performance Indicator Suite .............................................................................. 50 Appendix 3: Capital Infrastructure .............................................................................................................. 61

UL Hospitals Group

UL Hospital Group
University of Limerick (UL) Hospital Group is comprised of a group of six hospitals functioning collectively
as a single hospital system in the Mid-West of Ireland. The six sites include:
Ennis Hospital University Maternity Hospital Limerick
Nenagh Hospital Croom Orthopaedic Hospital
University Hospital Limerick St. John’s Hospital, Limerick
University Hospital Limerick (UHL), one of eight designated cancer centres in the country, is the Model 4
hospital for the region and has a full 24/7/365 Emergency Department and critical care service. Emergency
and complex surgeries are for the most part undertaken at UHL. The hospital is the hub for Ennis Hospital,
Nenagh Hospital and St. John’s Hospital which manage the majority of their local population through their
medical assessment units, local injury units and inpatient beds. Patients who require access to critical and
complex care are seen at University Hospital Limerick and either stabilised and transferred or admitted to
UHL as required.
Croom Hospital is the dedicated Orthopaedic hospital for adults and children in the Mid-West region whilst
also accepting the transfer of orthopaedic patients from UL hospital for post-acute care. In addition to
Orthopaedic services, Rheumatology and Pain Management services are also provided. University
Maternity Hospital Limerick (UMHL), being one of the largest maternity hospitals outside Dublin, has up to
5,000 births a year and the sole provider of obstetrical, midwifery and Level 3 Neonatal Intensive Care to
the Mid-West region.
1
UL Hospitals Group Operational Plan 2018
The 2018 Operational Plan for UL Hospitals Group sets out the type and volume of health care services to
be provided throughout the year, having regard for the available funding. Services continue to be delivered
in an environment where the population is growing, the number of people seeking to access services is
higher than ever before and where public expectations for quality services continue to increase. The
growing cost of delivering core services is such that we face a very significant financial challenge in 2018 in
maintaining the existing level of overall activity, to which we are fully committed. To this end, we are
conscious that maintaining services and driving improvements in patient safety and quality remain over-
riding priorities across the health sector, and all savings and efficiency measures will be assessed with
these priorities in mind.
For 2018, our objective is to maintain quality, deliver good outcomes and recognise that there are
opportunities, even in a constrained financial environment, to provide excellent health care services to the
population of the Mid-West of Ireland.
Risks to delivery of UL Hospitals Group Operational Plan 2018
Some risks to our ability to deliver the level and type of service include:
In the case of some services, given that the HSE is the statutory public provider and the realities
around the relatively fixed nature of certain costs, there is a requirement to respond to clinical need
even if this exceeds what can be supported by any level of realistic efficiencies coupled with the
available funding.
Delivering a volume of activity, driven by need, which is beyond funded levels.
Sustaining a level of service in areas where the nature of the response is such that activity cannot
be stopped or spend avoided, such as emergency services in our hospitals.
Progressing at scale and pace for the required transformation agenda within the funding levels
available.
Meeting the regulatory requirements in the hospital services, within the limits of the revenue and
capital available and without impacting on planned service levels.
Responding to urgent safety concerns and emergencies such as carbapenemase-producing
enterobacteriaceae (CPE). We will work with the Health Service Executive and Department of
Health to mitigate this risk, including how to manage emerging resource implications.
Meeting new drug costs.
Effectively managing our workforce including recruitment and retention of a highly skilled and
qualified workforce, required rationalisation of the use of agency personnel and staying within
our pay budget.
Working within the constraints posed by limitations to clinical, business financial and human
resource (HR) systems.
Investing in and maintaining our infrastructure, addressing critical risks resulting from ageing
medical equipment and physical infrastructure, and adhering to health and safety regulations.
2
UL Hospitals Group CEO’s Priorities 2018
No. Priority Actions Sponsor Owner Completion Date
1. ‘Governance Through Transformation’ – CEO/COO Exec Team Quarter 4
further develop Balanced Scorecards with
Directorates
Directorates and Executives incorporating
General Mangers
KPI’s and Performance monitoring - to
Head of
ensure Quality & Patient Safety.
Governance
2. HCAI- Continue best practise standards CDONM GM,CD& Quarter 1-4
with a focus on: COO/CCD DONS
- Hand Hygiene Directorates
- Dress code
- CPE
- Environmental Hygiene
3. Work with University of Limerick to CEO CAO/CCD/ Quarter 3
develop Health Sciences Academy. CDONM/
Once established progress Academic Head of Strategy
Health Science Centre.
Improve Research & Educational
Opportunities.
4. Commence Year 1 implementation of CEO Exec & Dir Quarter 1-4
Corporate Strategy 2018-2020 UL Teams
Hospitals under 4 headings;
- Clinical Transformation
- Education, Research &
Innovation
- Digital Health
- Collaboration & Alliances
5. Work with the Board of UL Hospitals and CEO Exec & Members
implement specific priorities set by Chair & of Board
Board Directors.
6. Review of Model 2 Hospitals to increase CEO Exec & Quarter 2-4
Ambulatory Care, Day Surgery and further Directorates
service provision as part of overall UL
Hospitals operational plans.
7. Implement Improvement Plans related to CEO CDONM/ Quarter 2
National Patient Experience Survey
CCD
specific to UL Hospitals
8. Commence Planning for future Health Board/ CEO Quarter 2
Service Realignment as defined in
CEO
Sláintecare Report.
3
No. Priority Actions Sponsor Owner Completion Date
9. Progress Capital Development Planning CEO COO/ Quarter 1-4
for acute bed capacity.
CDONM/
- 96 Bed Block CCD/DHR
- Elective Surgery Bed Capacity at
Croom & St John’s Hospitals.
- Critical Care Bed Capacity
Development
10. Continue to implement: CEO Executive & Quarter 1-4
Directorate Team
- National Maternity Strategy
- National Cancer Strategy
In line with UL Hospitals Service
Development.
11. Continue focus on Unscheduled Care CEO/COO Directorates Quarter 1-4
through Improvement processes,
SAFER Patient Flow Bundles &
Ambulatory Pathways at UHL.
12. Improve on Achievements with Scheduled CEO/COO Directorates Quarter 1-4
Care Waiting Lists with specific focus on
Outpatients & specific Inpatient Long
Waits.
13. Progress Value For Money processes CEO/CFO Executive & Quarter 1-4
further to ensure Financial Accountability. Directorates
Develop Value Improvement Programme
of work to achieve further efficiencies.
4
Governance UL Hospitals
The hospitals in Ireland are organised into seven Hospital Groups (HGs). Each Group Chief Executive has
full legal authority to manage the Group delegated to them under the Health Act 2004 in line with National
Service Plan (NSP) 2018 and allocated Group budgets. The UL Hospitals Group Operational Plan 2018 is
aligned with the NSP and the Acute Hospitals Division overarching Operational Plan.
The Group Chief Executives report to the National Director for Acute Services and are accountable for their
planning and performance under the Performance and Accountability Framework of the HSE. All targets
and performance criteria adopted in the service plan and the divisional Operational Plan will be reported
through this framework.
UL Hospitals is governed by a Board and an Executive Management Team led by a CEO who reports to
the Acute Hospitals Division HSE and to the Board of UL Hospitals. Our services are delivered across the
six sites under the leadership of five directorates namely, Medicine Directorate, Perioperative Directorate,
Diagnostic Directorate, Maternal and Child Health Directorate and Operational Services Directorate. Each
Directorate is led by a team of staff bringing Clinical, Managerial and Financial expertise together to provide
quality driven safe services, focused on the experience and outcomes for the patient.
5Organisational Chart
62017 Activity
Unscheduled Care
On the 29th May 2017, one of Ireland’s largest and most advanced Emergency Department opened in
University Hospital Limerick. The opening of this new ED, over three time the size of the old department,
marked a major milestone for UL Hospitals Group and has been transformational in terms of our ability to
deliver emergency care to patients in a dignified space, respecting their privacy. The new ED, includes
cutting edge diagnostics such as a unique track-mounted 128-slice CT scanner and dedicated triage and
isolation rooms. The department is laid out in pods with individual treatment rooms. There are separate
areas for major injuries, minor injuries, resuscitation and diagnostics - and a dedicated space for paediatric
patients with separate triage, waiting and treatment areas.
Whilst the new ED does not solve our problems of bed capacity or reduce the number of admitted patients
waiting on trolleys, it has greatly improved the patient experience in terms of dignity and privacy. An
Unscheduled Care Committee has been establised since the onset of the new ED with key objectives of
reviewing and improving process and patient flow issues and promoting and developing a programme of
integrated care with community services.
In addition, a new short-stay medical unit which has capacity for 17 admitted patients in the area of the old
ED opened on the 18th September 2017.
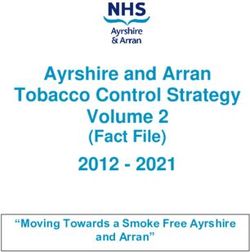
ED Presentations UHL
70,000
2017 saw nearly 68,000 presentations to the
65,000
ED. This represents an increase of 5.2% on
60,000
the previous year.
55,000
50,000
2014 2015 2016 2017
Total ED/LIU Attendance YTD Dec 2017
Local Injury Units (LIUs) account for
approximately 31% of all emergency
presentations for the Group. Attendances
11,094 UHL
to date in 2017 (December YTD) have
8,699
increased by 8.3% when compared to Ennis
the same period last year. 10,631
Nenagh
67,818
St. John's Hospital
7Scheduled Care
Inpatient Discharges
Inpatient discharges across the Group to date in 35,000
2017 (YTD December) with an outturn of nearly 30,000
52,300 have increased by over 4.1% when 25,000
compared to the same period in 2016. 20,000
15,000 2016
10,000 2017
5,000
0
Croom Ennis Nenagh St. UHL UMHL
John's
Day Cases Hospital
40,000
35,000
30,000 Day case activity has also shown a
25,000
significant growth to date, an increase of
20,000
7.3% when compared to the same period
15,000
10,000 last year (YTD December 2016).
5,000
0
Croom Ennis Nenagh St. John's UHL UMHL
Hospital Outpatient attendances year to date 2017
2016 2017 (December) across UL Hospitals Group
are standing in excess of 216,000.
OPD Attendances
Outside of the main maternity centre in Dublin, University 10,201
22,425
Croom
Maternity Hospital Limerick (UMHL) is one of the busiest 14,895
sites with over 4,400 births December year to date 2017. 10,890 Ennis
8,946 Nenagh
St. John's
Hospital
UHL
Births UMHL 2017 UMHL
450 149,455
400
350
300
250
200 388 393 410 390
371 366 364 361 374 355 346
150 309
100
50
0
July
January
Febuary
June
March
August
October
November
April
December
September
May
8Section 1: Key Reform
Themes
9Section 1: Introduction and Key Reform Themes
The HSE National Service Plan (NSP) 2018 sets out the type and volume of health and social care
services which the HSE expects to deliver over the coming year. It has regard to available funding,
planning assumptions agreed with or planned by the Department of Health (DoH) and what can be
delivered by realistic and achievable measures to improve the economy, efficiency and effectiveness of our
services during 2018. NSP 2018 provides details on the size and nature of our population, the needs of
patients and clients and how these are changing. The plan also sets out the current services that are in
place to respond to these needs, the issues and challenges with these services and the opportunities for
improvement. UL Hospitals Group, consequently will align itself to similar priorities and initiatives
throughout 2018 with the objective of maintaining the provision of a safe, quality and effective patient
centred care by recognising that there are opportunities even in times of financial constraint to provide
continuing excellent health care services.
It is however important to note that as we look to the future, it is likely to prove very challenging for health
and social care services in Ireland, including acute hospital setting such as UL Hospitals Group, to secure
the additional annual funding increases that would be required each year sufficient to allow:
(i) the existing arrangements and approaches to service delivery to expand at the pace
required necessary to respond to the increasing needs of our population; and
(ii) the population to have access to the latest models of care, evidence-based technologies,
drugs and devices.
In addition, there is a growing need to maintain or replace our current infrastructure and equipment. It will be
more important than ever that we add momentum to the good work already underway across our Hospital
Group while at the same time securing value for money, achieving maximum benefit from the available
financial, staffing and infrastructure resources.
Key reform themes
Consistent with the need to improve the health of the population, and to radically reshape where and how
services are provided, the HSE shall be pursuing four key reform themes during 2018 and beyond,
namely:
1. Improving population health.
2. Delivering care closer to home.
3. Developing specialist hospital care networks.
4. Improving quality, safety and value.
10Section 2: Our Population
11Section 2: Our Population
According to the 2016 Census, there are just over 4.7m people living in Ireland, an increase of
approximately 4% (nearly 170,000 people) since 2011. Our population is growing older, with the number of
people aged 65 years and over increasing from 11% in 2011 to 13% in 2016. The national age profile
particularly impacts on emergency services and as populations grow and age so too does the demand for
acute hospital services. Life expectancy at birth in Ireland has increased and is above the EU average of
80.6 years (Source: Eurostat). People are living longer through medical advances and technology along
with an increased knowledge and focus on health and general well-being. The greatest gains in life
expectancy have been achieved in the older age groups, reflecting decreasing mortality rates. According to
the European Commission, ageing is one of the greatest social and economic challenges for all countries
and by 2025 more than 20% of Europeans will be 65 or over with a particular rapid increase in the numbers
of those aged 80 and above. Based on 2016 CSO figures and trend analysis, forecasts tell us that the
number of people aged over 65 in Ireland will increase by a further 18% to 753,000 in the next five years
and similarly adults aged 85 years and over is projected to increase by approximately 4% annually.
Life expectancy and health status
The challenge remains to adapt health care services, settings and models of care to adequately meet the
needs of an ageing population whilst providing a safe, dignified and patient centred service at all times
within allocated budgets. In addition, chronic diseases (Cardiovascular disease, Cancer, Stroke,
Respiratory Disease and Diabetes) are on the rise with population projections indicating that by 2021 a
further 94,580 people will have at least one chronic condition (Tilda, 2010) representing a 20% increase.
However, due to heightened awareness, a strong leaning towards more active and healthy lifestyles along
with continuing focused clinical and academic research, survivorship of chronic diseases in Ireland is also
increasing which is a positive and welcome transition.
Health inequalities
The Hospital Group serves a socially diverse population including Limerick City which is the most deprived
local authority nationally with 36.8% of its inhabitants either very disadvantaged or disadvantaged (Health
Profile 2015 Limerick City). In sharp contrast to this, Limerick County is ranked as the eight most affluent
local authority area nationally with 54% of its population either being marginally above affluence or affluent
(Health Profile 2015 Limerick County).
Population Persons 2011 Persons 2016 Actual change % change
2011-2016 2011-2016
Limerick City & County 191,809 194,899 3,090 1.6%
Co. Tipperary 158,754 159,553 799 0.5%
Co. Clare 117,196 118,817 1,621 1.4%
Mid-West 467,759 473,269 5,510 1.2%
Ireland 4,588,252 4,761,865 173,613 3.8%
12There is a strong link between poverty, socio-economic status and health. In 2014, 11% of children
experienced consistent poverty (Survey in Income and Living Conditions (SILC) 2014, Central Statistics
Office (CSO)).
Life expectancy is greater for professional workers compared to the unskilled. This pattern has
increased since the 1990s (Layte R, Banks J., Socioeconomic differentials in mortality by cause of death
in the Republic of Ireland, 1984–2008; European Journal of Public Health, 2016).
Death rates are two times higher for those who only received primary education compared to those with
third level education. If economic mortality differentials were eliminated, it would mean 13.5m extra years
of life for Irish people (Burke S, Pentony S., Eliminating Health Inequalities, A Matter of Life and Death;
Think- thank for Action on Social Change, 2011).
Homeless
Nationally, latest figures indicate that over 8,000 people are homeless, with more than a third of these
being children. The total number of people homeless rose by 25% from July 2016 to July 2017
(Department of Housing, Planning and Local Government; Homeless Report, July 2017).
Travellers and Roma
The 2016 Census recorded 30,987 Travellers living in the Republic of Ireland, an increase of 5.1% from
Census 2011 (CSO, 2016). Almost three quarters of Travellers are aged 34 years or younger, while just
over 7% are 55 years and over.
The estimated Roma population is between 3,000 and 5,000 (Department of Justice, National Traveller
and Roma Inclusion Strategy 2017-2021).
Healthy Ireland Framework
Many diseases and premature deaths are preventable. Increased morbidity and mortality are strongly
related to lifestyle-based health determinants such as smoking, alcohol consumption, lack of exercise and
obesity. They are also related to inequalities in our society. The Healthy Ireland framework sets out a
comprehensive and co-ordinated plan to improve health and wellbeing over the coming years. This is
being actively implemented across all areas of the HSE.
13Section 3: Building a Better
Health Service
14Section 3: Building a Better Health Service
A key priority for the health service including UL Hospitals Group in 2018 is to develop an agreed
strategic position with the Acute Hospitals Division (AHD) and with our partners, in the interests of
building a better health service, designed to meet the needs of our population which represents higher
value care, in terms of return on the money invested in health. A number of initiatives are underway that
will lay the necessary foundations for developing a more sustainable health service into the future. A
number of these transformational programmes will continue in 2018, with a focus on:
Building a leadership culture and enabling and supporting staff to live our values and further embed
them in our working lives – Care, Compassion, Trust and Learning.
Transformation through our workforce: Health Services People Strategy 2015-2018.
Prevention through Healthy Ireland implementation and improved care management for patients
with chronic conditions.
Clinical leadership and clinical models of care, particularly care for the frail elderly and patient flow
from community services to hospitals and vice versa.
Higher rates of efficiency growth across key service areas.
Addressing serious information and knowledge management gaps in the healthcare system, and
the creation of a research and development function.
Enabling and supporting change in our delivery systems.
Care, Compassion, Trust and Learning – Our culture and our values
Within our hospital services, staff, managers, patients and service users are engaged in many formal
and informal activities to improve the way we lead and act with staff and service users to ensure that
the culture of our services is aligned with our core values. A significant challenge for all parts of
healthcare is to nurture cultures that ensure the delivery of continuously improving, high quality, safe
and compassionate healthcare. Two nationally supported approaches to building leadership capacity
and embedding values in practice will be further prioritised in 2018.
Our Patient Council, which was launched in 2016, will continue to work in partnership with UL Hospitals
Group to identify current and future opportunities to enhance the care experience for patients, families
and caregivers.
Values in Action
Values in Action is a behaviour based culture change programme designed to create better working
environments for our staff and deliver better experiences to patients and service users. It is based on
the understanding that, every day, many of our health service staff live by the core values of Care,
Compassion, Trust and Learning. Sometimes this is very visible, sometimes it is not. In June 2016 a
project team of staff from UL Hospitals Group and Mid-West Community Healthcare came together with
national colleagues to begin a journey to shape a culture where our values would become a way of life
and visible in our everyday actions and interactions. Throughout 2018, we will continue to sustain these
behaviors and values to promote a culture that we are proud of.
15UL Hospitals Group Staff Recognition Awards
The inaugural UL Hospitals Group Staff Recognition Awards were held during 2016 and this has since
become an annual event. It is seen as a welcome and important opportunity to highlight the many
achievements in the previous year, be it through excellent care, ground breaking research, innovations in
practice, more efficient ways of working, improving the patient experience and much more.
Transformation through our workforce: Health Services People Strategy 2015-2018
Through our Health Services People Strategy 2015-2018, we recognise the vital role of staff at all levels in
addressing the many challenges in delivering health services. Our commitment is to engage, develop and
value our workforce to deliver the best possible care and services to the people who depend on them. Staff
who are valued, supported in their development and treated well, improve patient care and overall
performance. Improved people management is the responsibility of all leaders, managers and staff.
Priorities in 2018 include:
Continuation of the ‘CEO Roadshows’ which allows all UL Hospitals Group an opportunity to meet
with our CEO and be updated on the progress of key priorities and initiatives.
Operationalise the Working Together for Health – A National Strategic Framework for Health and
Social Care Workforce Planning, 2017 across the health services.
Support Healthy Ireland and the Workplace Health and Wellbeing Unit to manage staff, support
services and ensure that policies and procedures are designed to enable staff to maximise their work
contributions and work life balance.
Introduce performance management systems in areas of the public health sector where these are not
already in place.
Leadership Academy
Leadership is the most influential factor in shaping organisational culture and so ensuring the necessary
leadership behaviours, strategies and qualities are developed is fundamental. 2017 marked a year that
established the Leadership Academy which was rolled out at a national level across the HSE. The
Leadership Academy is a strategic investment in developing staff at all levels so that a better, more patient-
focused, more efficient and compassionate health service can be developed. It is envisaged that in 2018 a
further two group of participants will be enrolled for both of the two flagship programmes and evaluating the
work of the Academy to ensure it is meeting its objectives.
As part of UL Hospitals Group ongoing academic relationship with the University of Limerick, a total of 30
participants from across the Group have been involved in a collaborative action based research program to
promote succession planning and leadership development. This research study takes a holistic approach to
all aspects of leadership and will continue throughout 2018.
16Healthy Ireland: Chronic disease prevention and management
The projections of future utilisation of healthcare show us that a strong and comprehensive response to
chronic diseases is required. A national policy framework and health service implementation plan is already
in place, Healthy Ireland in the Health Services - Implementation Plan 2015-2017, and the HSE has
developed an Integrated Care Programme for the Prevention and Management of Chronic Disease to
prioritise this work. Both of these will continue to be progressed in 2018.
National Clinical and Integrated Care Programmes
In 2018, the national clinical and integrated care programmes are focused on developing new integrated
care models and pathways to ensure safe, timely, efficient healthcare which is provided as close to home
as possible. The work of the national clinical programmes and integrated care programmes is
interdependent. The associated priorities and actions have been selected to generate improvements as set
out below.
Delivering care closer to home
Design new community-based models to provide improved care and outcomes for service users, close to
their home and at the lowest level of complexity that is deemed safe, and redesign care from traditional
secondary care models to community-based models.
Integrated Care Programme for Children
This programme aims to improve the way in which healthcare services are designed and delivered to
children and their families. The programme will also work with key stakeholders to design an
implementation plan for the national model of care for paediatric healthcare services, within existing
resource levels.
Integrated Care Programme for Older Persons
This programme is building on local initiatives to incrementally develop pathways for older people
across primary and secondary care, especially those with more complex care needs.
Integrated Care Programme for Patient Flow
This programme is developing a standardised approach to managing patient flow in a number of areas
including urgent and emergency care, scheduled care, outpatients and community healthcare. The
programme will develop a plan to support the reorganisation of urgent and emergency care in line with
best outcomes and the best experience for patients.
Develop Specialist Hospital Care Networks
In parallel with the requirement to shift less complex acute care from hospital to community settings, there
is a need to ensure that the secondary and tertiary care sectors are able to deliver the complex, specialised
17and emergency care that will be required by patients. The provision of integrated care is a key element of
this model of care.
Improving performance, efficiencies and effectiveness
The Performance and Accountability Framework has been enhanced in 2018 in line with new governance
arrangements and organisational changes in the HSE. It sets out the process by which the National
Divisions and Hospital Groups (including UL Hospitals Group) that performance will be managed across
Access to and Integration of services, the Quality and Safety of those services, achieving this within
specific Finance, Governance and Compliance requirements, and by effectively harnessing the efforts of
our Workforce.
Research and Development
Health research is essential to generate new knowledge to inform evidence-based practice. Knowledge
and learning are also key requirements for effective change and transition planning for the health
services in Ireland.
A research and development function nationally is being established within the health services to support
the delivery of key actions originally set out in the Action Plan for Health Research 2009-2013. The
appointment of a research and development lead is a key component of this development. The aim is to
foster a research culture within our health services by providing an enabling governance framework,
increasing the integration of research into health service delivery, strengthening research networks and
developing our research capacity.
UL Hospitals Group has forged very strong links with its academic teaching partner, the University of
Limerick. The opening of the Clinical Education and Research Centre on the main hospital campus, now
houses teaching and research facilities, a substantial lecture theatre and state of the art medical library.
This, along with other initiatives such as pioneering robotic surgery, has greatly raised the profile of UL
Hospitals Group as a centre of teaching and learning excellence. Both this local expertise and facility
have allowed such prestigious events as the 25th Anniversary Sylvester O’Halloran Scientific Symposium
to be held.
18Section 4: Quality & Safety
19Section 4: Quality and Safety
Introduction
The HSE places significant emphasis on the quality of services delivered and on the safety of those
who use them. A three-year National Safety Programme to develop and oversee the implementation of
national safety priorities and initiatives across all parts of the health system is continuing and UL
Hospitals Group will work accordingly to deliver on national patient safety priorities.
The National Patient Safety Programme
Insufficient attention to patient safety is a leading cause of harm across healthcare systems
worldwide. It impacts on health outcomes causing increased morbidity, temporary or permanent
disability and sometimes even death. The safety of patients and service users is therefore the
number one priority for the health service and UL Hospitals Group.
The National Patient Safety Programme aims to continue the work already undertaken in supporting
improvements in patient and service user safety across the entire health system to ensure changes
are integrated into the ‘business as usual’ activities of individual services.
The programme aims to:
Improve the quality of the experience of care including quality, safety and satisfaction.
Implement targeted national patient safety initiatives and improvements in the quality of services
(e.g. preventing healthcare associated infection (HCAI); use of anti-microbials and anti-microbial
resistance (AMR); addressing sepsis, falls, pressure ulcers and medication errors; clinical
handover; and recognising and responding to deteriorating patients including the use of Early
Warning Score systems.
Respond to the public health emergency by monitoring and managing CPE.
Build the capacity and capability in our services to improve quality and safety and improve
the response of the healthcare system when things go wrong.
Put in place appropriate governance for patient safety across our services.
Strengthen quality and safety assurance, including audit.
ULHG priorities 2018
Role out education and training for proactive management of Risk
Review Governance of management of incidents and role of local and group SIMT in line with new
incident framework
Implementation of new incident management framework, which involves a proportional response to
category of incident and level of harm.
Development of Clear Governance for management of HCAI
20Service user involvement and experience
A key focus will be to listen to the views and opinions of patients and service users and consider them
in how services are planned, delivered and improved. Key priorities for 2018 include:
Implement the National Patient Experience Survey in acute hospitals and maternity services (including
UL Hospitals Group).
Use the feedback received from the National Patient Experience Survey and the Patient
Narrative Project: Your Voice Matters to inform health service priorities and actions throughout
our Hospital Group.
Involve patients and family members in the design, delivery and evaluation of services through
the National Patient Forum, Patients for Patient Safety Ireland, and focus groups with the
Patient Representative Panel. ULHG will continue to work with our Patient Council.
Ensure that the information gathered through the HSE’s feedback system ‘Your Service Your
Say’, the National Appeals Service Office and the Confidential Recipient are used to inform
health service priorities and actions across our Hospital Group.
Implement the national complaints system.
ULHG priorities 2018
Patient Council meetings held - committee membership increased - Nutrition, Signage, End of Life,
Patient Flow, and Literacy.
Recruit new members for Patient Council.
UL Hospitals Group Patient and Public Participation Strategy to be launched.
Implement QIPs for National Patient Experience Survey.
Further development of patient feedback system including, web access for patients and further
development of reports.
Increase and develop Volunteer Roles.
Roll-out of education to Service Users and Staff in relation to Your Service Your Say Policy.
Improving the quality and safety of services
Improving quality and safety requires the HSE to further build the capacity and capability of frontline
services to implement the Framework for Improving Quality in our Health Service. Key priorities
nationally for 2018 which will incorporate UL Hospitals Group include:
Nationally further develop quality and safety teams across CHOs, Hospital Groups and the NAS.
Provide resources and toolkits to staff to support them in implementing the Framework for
Improving Quality in our Health Service.
Promote the continuous development of quality improvement skills amongst all staff through use of the
Improvement Knowledge and Skills Guide, 2017.
21 Deliver leadership education programmes through the Diploma in Leadership and Quality in
Healthcare for multi-disciplinary teams, and the Executive Clinical Leadership course for Clinical
Directors.
Roll out the culture of person-centredness programme across all services.
Implement quality and patient safety committees across all services to drive quality improvement
and patient safety.
Develop and use quality profiles and specialty quality programmes.
Develop the capacity and capability for staff engagement to maximise the contribution of
staff to improving quality.
Use results from the patient safety culture survey to ensure continued staff engagement in
improving quality.
ULHG priorities 2018
Development of teams for after action review.
Further support engagement with CHO with joint management of adverse events and complaints.
Quality improvement committee to continue lunch time session.
Complaint officer training and review training scheduled.
Develop Governance structures for QIPs.
Maintaining standards and minimising risk
Robust quality and patient safety systems and processes, that are an integral part of the day to day
operations of healthcare delivery, are essential to maintain standards of care, identify areas for
improvement, support learning and responses when things go wrong, and manage risk. Key priorities
nationally for 2018 include:
Support the development and implementation of National Clinical Effectiveness Committee
(NCEC) clinical guidelines and audits.
Develop a Quality Assurance Framework and further develop national clinical audits, healthcare
audits and specialty quality programmes.
Further develop the capability to report, manage, investigate, disseminate and implement learning
from safety incidents that occur.
Increase our analytical capacity to understand quality and service user safety, including
the development and use of quality profiles.
Expand the activity of the National Independent Review Panel.
Roll out assisted decision-making and open disclosure processes.
22ULHG priorities 2018
Capacity and Capability review in line with local governance process & national review
Development of multidisciplinary systems analysis framework
Development of local department reports on QPS activity
Development of risk registers to align escalation and de-escalation protocols
23Section 5: Service Delivery
24Section 5: Service Delivery
Services Provided
Acute services include emergency care, urgent care, short term stabilisation, scheduled care, trauma,
acute surgery, critical care and pre-hospital care for adults and children. The UL Hospitals Group,
continually works to improve access to scheduled and unscheduled care, ensuring quality and patient
safety within the allocated budget. Hospital Groups provide the structure to deliver an integrated
hospital network of acute care in each geographic area, the Mid-West in our case.
The hospitals have a key role in improving the health of the population by providing a range of services
from brief intervention training and self-management support, offering advice and support in staying well,
to optimising care pathways for patients admitted with exacerbations of chronic diseases, to reducing
length of stay, accelerating return to usual health and supporting an integrated approach with GPs in the
long term surveillance of patients who have had cancer. Healthy lifestyle choices are promoted across a
range of paediatric, maternity and adult services, aimed at avoidance of ill health and best management of
conditions such as asthma, COPD and diabetes.
Early detection of disease is central to optimising patient outcomes and the acute hospitals continue to
support the delivery of screening services for bowel and breast cancer and follow-up care for cervical
screening in line with the National Screening Service. The National Women and Infants’ Health
Programme (NWIHP), National Cancer Control Programme (NCCP), and the NAS work closely with the
acute hospitals and lead the strategic development of these services.
Issues and opportunities
Challenge in addressing increased demand in terms of the number of patients presenting to hospital
and the complexity of their conditions.
Lack of bed capacity. A bid to build an additional 96 bed block on the UHL site has been submitted to
the Department of Health and approval has been granted for funding of the design stage of the build.
Lack of single room availability, in particular for patients with HCAIs and when available, on discharge,
these beds must be closed for deep cleaning further impacting the patient flow.
Initiatives undertaken in UL Hospitals Group such as the LEAF project which aims at promoting
earlier discharges and saw the introduction of the Hospital Discharge Lounge which facilitates the
freeing up of beds within wards for admitted patients.
The Unscheduled Care Group and associated QIP has been established within UL Hospitals Group
to focus on the Emergency Care pathway, monitor the patient flow and work collaboratively with our
Older persons’ Services and Primary Care colleagues. A key focus in 2018 will be on improving
access to emergency care and continuing the on-going work to reduce trolley waits and improve ED
performance.
Improve access times to inpatient, day case elective procedures and outpatient consultations by
implementing waiting list action plans and following the National Treatment Purchase Fund (NTPF)
roll-out of the National Inpatient, Day Case and Planned Procedure Waiting List Management
Protocol.
25 The provision of specialist services within acute hospitals such as UL Hospitals Group remains a
priority for the HSE in terms of responding the increasing complexity of presentations and advances
in medical technology and interventions.
The National Cancer Strategy 2017-2026 was published in 2017 and support for the implementation of
its recommendations will address some of the current deficits in cancer services nationally. Details of
the NCCP’s priorities can be seen further in the plan.
Meeting increased demand for urgent colonoscopy waiting times, urgent GI endoscopy waiting times
and targeting significant reductions in overall waiting lists and efficiencies remains a key focus into
2018.
Ensuring that services for children are managed in an integrated way, including improving paediatric
access, are key challenges for acute services. The new children’s hospital, when completed, will
transform general paediatric and emergency care for children. Ensuring maximum benefit for
patients from the health service’s expenditure on medicines and allowing new effective medicines to
be adopted in the future.
Implementing priorities 2018 in line with Corporate Plan goals
Corporate Plan Goal 1: Promote health and wellbeing as part of everything we do so that people will
be healthier
Improve patient and staff health and wellbeing by implementing Healthy Ireland Plans
Priority Accountable Timeline
Develop and implement clinical guidelines for under-nutrition and an acute hospital ULHG Q1-Q4
food and nutrition policy.
Continue implementing Healthy Ireland plans in the Hospital Groups. ULHG Q1-Q4
Improve staff uptake of the flu vaccine. ULHG Q1-Q4
Prioritise the implementation of Making Every Contact Count in all care settings. ULHG Q1-Q4
Progress the implementation of the Diabetes chronic disease demonstrator ULHG Q1-Q4
Projects in the Group
Corporate Plan Goal 2: Provide fair, equitable and timely access to quality, safe health services that
people need
Increase critical care capacity
Priority Accountable Timeline
Commence monitoring of time from decision to admit to admission to Intensive ULHG Q1-Q4
Care Unit
26Improve the provision of unscheduled care
Priority Accountable Timeline
Improve pathways for care of older people living with frailty in acute hospitals in ULHG Q1-Q4
association with the Integrated Care Programme for Older Persons.
Continue to ensure that no patient remains over 24 hours in ED. ULHG Q1-Q4
Continue to implement measures to address seasonal increase and reduce ULHG Q1-Q4
delayed discharges in association with community healthcare.
Support the continued roll-out of the Integrated Care Programme for Patient Flow. ULHG Q1-Q4
Generate improved capacity by improving internal efficiencies and more ULHG Q1-Q4
appropriate bed usage by reducing length of stay, early discharge and improving
access to diagnostics.
Improve the provision of scheduled care
Priority Accountable Timeline
Continue to improve day of surgery rates and increase ambulatory services as ULHG Q1-Q4
clinically appropriate.
Monitor length of stay and opportunities for improvement using NQAIS ULHG Q1-Q4
Reduce waiting times for all patients and particularly those waiting over 15 months ULHG Q1-Q4
on outpatient and inpatient / day case waiting lists by implementing waiting list
action plans.
Develop a plan to address waiting lists challenges in Orthopaedics and ULHG Q2-Q4
Ophthalmology.
Improve efficiencies relating to inpatient and day case activity by streamlining ULHG Q1-Q4
processes and maximising capacity in acute hospitals.
Work with the NTPF to implement the National Inpatient, Day Case and Planned ULHG Q1-Q4
Procedure (IDPP) Waiting List Management Protocol.
Work with the NTPF to develop and implement a waiting list action plan for 2018. ULHG Q1-Q4
Work with the clinical programmes to complete a suite of pathways of care at ULHG Q1-Q4
condition-level, through the Outpatient Services Performance Improvement
Programme.
Implement the findings and recommendations of the NTPF special audit to drive ULHG Q1-Q4
process and performance improvement in scheduled care.
Further develop GP referral guidelines and standardised pathways, supported by ULHG Q1-Q4
efficient electronic referral systems.
Assist with the roll out the national validation project for inpatient, day case and ULHG Q1-Q4
outpatient waiting lists.
Work with National Radiology Programme to establish national vetting criteria for ULHG Q1-Q4
radiology diagnostic tests.
Continue to work with the NTPF to develop a national dataset and waiting list for ULHG Q1-Q4
CTs, MRIs and Ultrasounds
27Corporate Plan Goal 3: Foster a culture that is honest, compassionate, transparent and accountable
Ensure quality and patient safety
Priority Accountable Timeline
Facilitate initiatives which promote a culture of patient partnership including the ULHG Q1-Q4
next phase of the National Patient Experience Survey.
Monitor and control HCAIs. ULHG Q1-Q4
Continue to develop robust governance structures at hospital, group and national ULHG Q1-Q4
level to support management of HCAI / AMR.
Collate information on incidence of CPE and associated infection control measures ULHG Q1-Q4
including use of screening guidelines and appropriate accommodation of patients.
Review assessment process for National Standards for Safer Better Healthcare ULHG Q1-Q4
and develop guidance to support monitoring and compliance against same.
Enhance medicines management
Priority Accountable Timeline
Collaborate with AHD with the further enhancement medicines management, ULHG Q1-Q4
improve equitable access to medicines for patients and continue to optimise
pharmaceutical value through the Acute Hospitals Drugs Management Programme
with a focus on the use of biosimilars.
Collaborate with AHD on the implementation of the Report on the Review of ULHG Q1-Q4
Hospital Pharmacy, 2011 (McLoughlin Report) with a focus on the development of
pharmacist roles to improve and enhance medication safety, and implement HIQA
medication safety reports.
Work with AHD to advance the reimbursement of (Enzyme Replacement Therapy ULHG Q1-Q4
(ERT) through PCRS to ensure equitable access for all patients.
Contribute to the audit of Neurology Drug Use and Guidelines with particular focus ULHG Q1-Q4
on Tysabi for Multiple Sclerosis treatment
Implement Children First
Priority Accountable Timeline
Commence implementation of the Children First Act 2015 including mandatory ULHG Q1-Q4
training for staff as appropriate.
Corporate Plan Goal 4: Engage, develop and value our workforce to deliver the best possible care
and services to the people who depend on them
Support and progress the policies and initiatives of the Office of the Chief Nursing Officer, DoH and European
Directives on working hours
Priority Accountable Timeline
Extend and roll out nationally the Phase 1 Framework for Staffing and Skill Mix for ULHG Q1-Q4
Nursing in General and Specialist Medical and Surgical Care in acute hospitals
within the allocated resources as appropriate.
Implement a pilot for the Phase 2 Framework for Staffing and Skill Mix for Nursing ULHG Q1-Q4
in emergency care settings as appropriate.
28Priority Accountable Lead
Enhance the training and development of Advanced Nurse Practitioners in ULHG Q1-Q4
association with DOH and NMPDU.
Continue to improve compliance with the European Working Time Directive with ULHG Q1-Q4
particular focus on the 24 and 48 hour targets.
Corporate Plan Goal 5: Manage resources in a way that delivers best health outcomes, improves
people’s experience of using the service and demonstrates value for money
On-going monitoring and performance management of financial allocations in line with the Performance and
Accountability Framework
Priority Accountable Lead
Monitor and control hospital budgets and expenditure in line with allocations. ULHG Q1-Q4
Identify and progress realistic and achievable opportunities to improve economy ULHG Q1-Q4
efficiency and effectiveness
Secure reductions in cost and or improvements in efficiency of services currently ULHG Q1-Q4
provided
Continue the next phase of ABF including the incentivised scheme for elective ULHG Q1-Q4
laparoscopic cholecystectomy.
Ensure compliance with the memorandum of understanding between the HSE and ULHG Q1-Q4
VHI in conjunction with National Finance.
Progress implementation of the recommendations of the Patient Income Review ULHG Q1-Q4
which will focus on training, standardisation of processes and measurement of
improvements in billing and collection by hospitals.
Health and Wellbeing Services
Health and wellbeing is about helping our whole population to stay healthy and well by focusing on
prevention, health promotion and improvement, reducing health inequalities, and protecting people from
threats to their health and wellbeing.
As part of the promotion of health and wellbeing, a number of national services are provided. The
national screening service provides population-based screening programmes for BreastCheck,
CervicalCheck, Bowelscreen and Diabetic RetinaScreen. These programmes aim to reduce morbidity
and mortality in the population through early detection and treatment across the programmes.
The environmental health service protects the health of the population by taking preventative actions
and enforcing legislation in areas such as tobacco, food, alcohol, sunbeds and water fluoridation.
The health promotion and improvement service provides a range of preventative health education and
training services, focused on positively influencing the key lifestyle determinants of health such as
smoking, alcohol, sexual health, healthy eating and physical activity.
The public health service protects our population from threats to their health and wellbeing through its
provision of national immunisation and vaccination programmes, national infectious disease monitoring
and health screening.
29UL Hospitals Group published a Healthy Ireland Implementation Plan 2016-2019 in June 2016 following
staff consultations and communication roadshows. The plan has been published on the HSE and UL
Hospitals websites. Many key actions contained within the plan are in progress with some already
delivered. Examples include the formation of a group-wide flu vaccine committee which oversaw the roll
out of a peer vaccinator model. An educational module on breast-feeding was introduced for Paediatric
medical staff and several patient education events and screenings were held. One of the pillars of Health
and Wellbeing is the importance of promoting and maintaining staff health. Several physical activities
across the sites within the Group were organized along with events to highlight the significance of positive
mental health. Work will continue throughout 2018 to capitalize on the positive results already achieved in
terms of education and initiatives to further inform both patients and staff of the benefits of keeping healthy
and well.
ULHG Priorities 2018
Continue the third year of Healthy Ireland Implementation at UL Hospitals Group. Review progress
on the actions contained within the UL Hospitals Implementation Plan at Healthy Ireland Steering
committee quarterly. Support the Healthy Ireland committees on all hospital sites and ensure that
all hospital sites have an annual plan in place.
Implementing ULHG priorities 2018 in line with Corporate Plan goals
Report all progress on Healthy Ireland Implementation to the Hospital Executive Leadership Team
using Project Vision with the support of the PMO.
Progress the development of the group-wide Sports & Social Club in 2018
Continue to engage staff in resilience and stress management programmes
Work towards all hospitals sites reaching the 40% national target for uptake of flu vaccine
Communicate the launch of Making Every Contact Count training to staff on all sites and ensure
that training targets are achieved
Continue to roll out standardised measurement and documentation off BMI in all out-patient patient
records
Agree a standardised obesity care pathway for all patients identified within out-patient services in
UHL in collaboration with Mid-West Community Healthcare
Re-launch the group-wide Tobacco Free Campus policy and ensure that smoking staff are
supported to quit.
Begin a national pilot in Croom Hospital using the Work Positive screening tool for workplace
stress and agree approved actions.
Launch staff bike shelters on four hospital sites and continue to link with Limerick Smarter Travel
for active travel supports
Hold a staff summer physical activity event in collaboration with Mid-West Community Healthcare
Engage staff from across all represented cultures in the workforce with a staff multicultural
celebration event in Q1
Provide staff health screening opportunities in collaboration with the national H&WB Division and
the Irish Heart Foundation.
30Cancer Services
The population aged over 65 years is estimated to more than double in the 25 years between 2011 and
2036. This ageing of the population will drive a large increase in the number of new cancer cases, with
the number of new patients receiving chemotherapy expected to increase by between 42% and 48% in
the period from 2010 to 2025.
Services for the treatment of cancer include surgery, radiotherapy and systemic anti-cancer therapy
(SACT). The majority of, but not all, cancer surgery now takes place in the designated cancer centres,
UHL being one. As part of the new National Cancer Strategy 2017-2026, initiatives will be set up across
the continuum of care, from diagnosis and treatment, to appropriate follow-up and support, in both the
hospital and community setting across the four strategy goals:
Reduce the cancer burden through cancer prevention and early detection.
Provide optimal care in the most appropriate setting and in a timely manner.
Maximise patient involvement and quality of life, especially for those living with and beyond
cancer, through psycho-oncology services, survivorship care plans and cancer care guidelines
and initiatives.
Enable and assure change, aligned with desired outcomes.
Priorities 2018
Develop a comprehensive implementation plan for the National Cancer Strategy 2017-2026 and
continue the implementation of the strategy.
Improve the quality of cancer services through evidence-based enhancement of patient care
Develop a cancer prevention and early detection function in the NCCP.
Develop cancer survivorship and psycho-oncology services.
Support the enhancement of funding programmes for the best available cancer drug treatments, and
support hospitals in meeting the continuing burden of drug costs and in implementing quality initiatives
in cancer care.
Commence the implementation of the Medical Oncology Clinical Information System (MOCIS)
Support the development of workforce planning, in line with the National Cancer Strategy 2017-2026.
Implementing priorities 2018 in line with Corporate Plan goals
Corporate Plan Goal 1: Promote health and wellbeing as part of everything we do so that people will
be healthier
Develop cancer survivorship and psycho-oncology services
Priority Accountable Timeline
Link with other stakeholder agencies to implement survivorship model and psycho- ULHG Q3-Q4
oncology service across the cancer centres.
Develop a national implementation plan for cancer survivorship under the guidance ULHG Q4
of the NCCP.
31You can also read