"TRIPLE NEGATIVO" - Foro de Debate en Oncologia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

“TRIPLE NEGATIVO” Emilio Alba UGCI Oncología Hospital Universitario Regional y Virgen de la Victoria Facultad de Medicina Málaga IBIMA
ÍNDICE DE LA PRESENTACIÓN • Introducción • Tratamiento adyuvante • Tratamiento neoadyuvante • Enfermedad metastásica • Clasificación genómica/molecular • Conclusiones y perspectivas

Epidemiology of basal-like breast cancer,
Millikan et al., Breast Cancer Research and Treatment, 2008
(PMID:17578664)
Luminal A Basal-like
N=796 N=225
Menarche < 13 1.1 (0.9-1.3) 1.4 (1.1-1.9)
Adjusted ORs
(95% CI) > 3 children 0.7 (0.5-0.9) 1.9 (1.1-3.3)
N = 1424 cases
and
2022 controls First birth < 26 0.7 (0.5-0.9) 1.9 (1.2-3.2)
Breastfeeding > 4m 0.9 (0.7-1.1) 0.7 (0.4-0.9)
Parity > 3 and
0.7 (0.5-0.9) 1.9 (1.1-3.3)
No breastfeeding
Waist:Hip > 0.84 1.5 (1.1-1.9) 2.3 (1.4-3.6)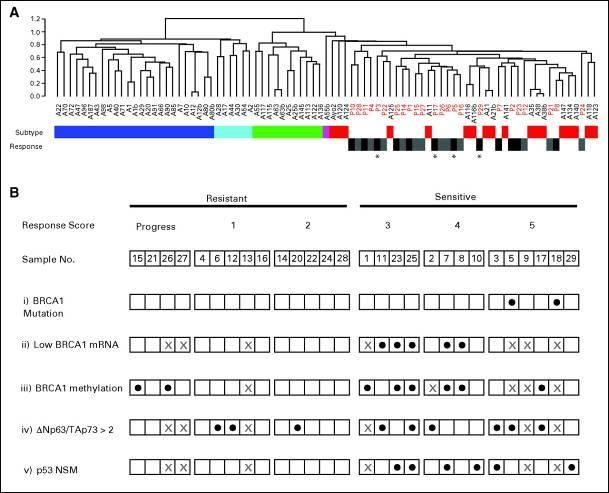
BBC Clinical Characteristics
Population-based study of 496 incident breast cancers 1992-6:
Basal-like HER2+/ER- Luminal A Luminal B P-value
(n=100) (n=33) (n=255) (n=77)
Stage
I 24% 28% 44% 39% 0.06
II 62% 53% 47% 54%
III-IV 13% 19% 9% 6%
Lymph node + 41% 56% 34% 47% 0.04
Invasive ductal 84% 94% 70% 79%
Triple negative/basal-like breast cancer:
Biologic features
• Miscelaneous disease
• Basal-like: entirely different from other breast cancers:
High proliferation index (↑Ki-67)
High prevalence of p53 mutations (>80%)
Genomic instability, abnormal DNA repair
High rate of mutations over time:
• adquired resistance to chemotherapy after exposition
• large variety of different gene mutations
Evidence of BRCA-1 dysfunction even in sporadic tumors
Lack of clear drugable targets so far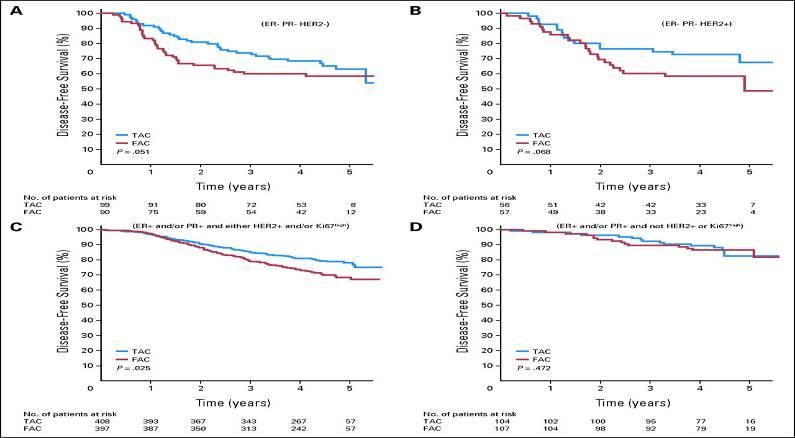
TNBC is a heterogeneous disease
• Invasive Ductal Carcinoma NOS, high grade
• Invasive Lobular Carcinoma high grade, pleomorphic
Poor
prognosis
• High grade (oat-cell) neuroendocrine
• Metaplastic, high grade
• Myoepithelial carcinoma
• Medullary
• Apocrine
• Adenoid-cystic
• Metaplastic, low grade
Good
prognosis
Modified from Viale, G
Triple negative and basal-like tumors

Frequencies of subtypes across studies
Cheang, M et al, ASCO 2012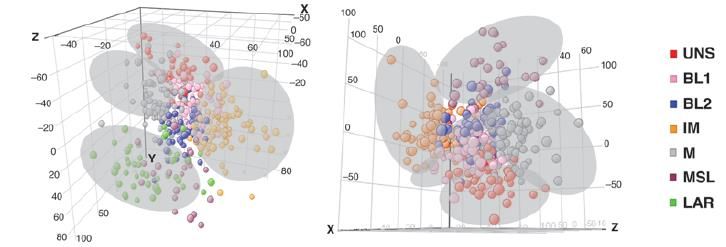
IHC Features of Basal-like versus Non-Basal-like
Breast Cancers
Basal-like Non-Basal-like P value
ER 14% 78% --
ErbB2 0% 26% --
CK 5/6 62% 14% --
C-KIT 29% 11%
MA.5 DFS
100
80
Patients (%)
60 CEF
40 CMF
20 P = .005
0
0 5 10
Yrs
No. at CEF 351 212 84
Risk: CMF 359 193 80
Levine MN, et al. J Clin Oncol. 2005;23:5166-5170.BCIRG 001: DFS WITH FAC (—) O TAC (—) ACCORDING TO INTRINSIC
SUBTYPE
Copyright © American Society of Clinical Oncology
Hugh, J. et al. J Clin Oncol; 27:1168-1176 2009CALGB 9344 (AC VS ACPACLITAXEL)
Hayes et al. N Engl J Med. 2007;357:1496.La proliferación es importante aun en el basal-like
Prat A. BJC 2014Final OS (secondary endpoint)
1.0
0.8
Estimated probability
0.6 CT CT + BEV
(N=1290) (N=1301)
Events, n (%) 149 (11.6) 144 (11.1)
0.4 3-year OS rate, % 91.5 92.4
(95% CI) (89.9‒93.1) (90.9‒93.9)
5-year OS rate, % 87.7 87.9
0.2 (95% CI) (85.7‒89.6) (86.0‒89.8)
Stratified hazard ratio 0.93
(95% CI) (0.74‒1.17)
Log-rank p-value 0.5247
0
0 6 12 18 24 30 36 42 48 54 60 66 72 78
No. at risk: Time (months)
CT + BEV 1301 1264 1238 1205 1165 1122 1084 1053 1004 876
495 141 42 0
CT 1290 1248 1217 1175 1133 1089 1053 1019 976 862
511 122 41 0
OS = overall survivalPathologic complete response to neoadjuvant
chemotherapy differs by subtype
T-FAC1 AC-T2
(N=82) (n=107)
Luminal A/B 2/30 (7%) 4/62 (7%)
Normal-like 0/10 (0) NA
HER2+/ER- 9/20 (45%) 4/11 (36%)
Basal-like 10/22 (45%) 9/34 (26%)
PRegimen No. pts No. of pCRs % pCRs CMF 14 1 7 AC 23 5 22 FAC 28 6 21 AT 25 2 8 Cisplatin 12 10 83
pCR rate: 22%
Predictors of response to cisplatin therapy in triple-
negative/basal-like tumors
Copyright © American Society of Clinical Oncology
Silver, D. P. et al. J Clin Oncol; 28:1145-1153 2010pCR and platinum salts in TNBC
Predictors of general chemotherapy sensitivity (both arms combined) in
GEICAM2006 within tumors that are PAM50 Basal-like
Gene Ontology TermspCR in Stratified in Subgroups
Neoadjuvant trials: PCR rates WITH BEVACIZUMAB +
CHEMOTHERAPY in TNBC subgroups
Patients (%)
Von Minckwitz et al. NEJM 2012; Bear et al. NEJM 2012Carboplatin vs Docetaxel in Advanced TNBC or BRCA1/2+ BC
(TNT): ORR
90 Carboplatin
Docetaxel
Response at Cycle 3 or 6 (%)
80
Crossover P = .03
70 68.0%
60
50 P = .44 P = .16
40 35.6% 36.6%
31.4% P = .73 33.3%
30 28.1%
22.8% 25.6%
20
10
0
All Pts C→D D→C BRCA1/2 No BRCA1/2
(n = 376) Crossover* Mutation Mutation
(All pts; n = 182) (n = 43) (n = 273)
*Excludes those with no first progression or not starting crossover treatment.
Tutt A, et al. SABCS 2014. Abstract S3-01.Phase I Trial of Olaparib in Patients with Solid Tumors
• Escalation and expansion phase, n = 60
• Recommended phase II dose: 400 mg PO BID
• Toxicities
– Nausea (32%), fatigue (30%), vomiting (20%), taste alteration (13%), anorexia (12%), anemia
(5%)
• Clinical activity = 12/19 patients with BRCA mutations
Tumor BRCA No. of pts Response
Breast 2 2 1 CR, 1 SD
Ovarian 1 or 2 8 8 PRs
Fallopian tube 1 1 PR
Prostate 2 1 PR
Fong PC et al. N Engl J Med 2009; 361:123-134Olaparib in BRCA-deficient Metastatic Breast Cancer: Results
Best percent change from
Median 3 prior lines of therapy baseline in target lesions by
genotype
ITT cohort 400 mg BID 100 mg BID
N = 27 N = 27
ORR 11 (41%) 6 (22%)
CR 1 (4%) 0
PR 10 (37%) 6 (22%)
Median PFS 5.7 mo 3.8 mo
(4.6-7.4) (1.9 – 5.6)
Tutt A et al. J Clin Oncol 2009;27(18S):803s (abstr CRA501)Phase I: Olaparib + Paclitaxel in 1st and 2nd line MBC BKG: Olaparib single agent activity in BRCA 1/2 mutated MBC Olaparib + paclitaxel, N=19, 70% 1st line, unselected for BRCA mutations 33-40% RR; no CRs Median PFS: 5.2-6.3 months Hematologic toxicity high, requires G-CSF Dose reductions common Unclear whether combination be taken forward
Pembrolizumab in Advanced TNBC (KEYNOTE-012): Tumor
Regression
Change From Baseline in Sum of Longest
100 Confirmed CR (nodal disease)
80 Confirmed PR
Diameter of Target Lesion (%)
SD
60 PD
40
20
0
-20
-40
-60
-80
-100 Individual Evaluable Pts (n = 23)
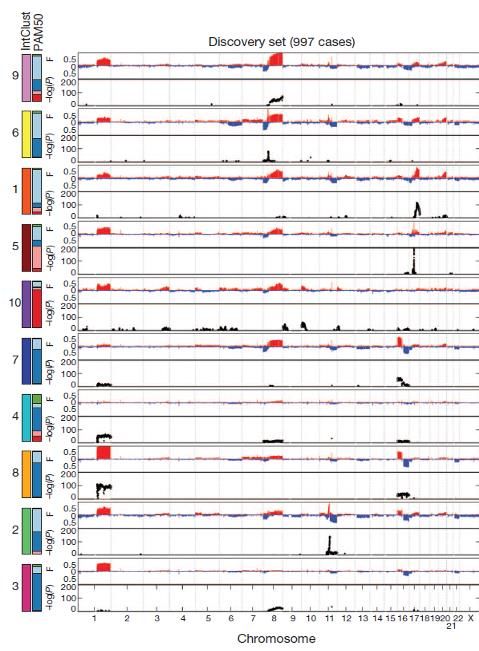
Nanda R, et al. SABCS 2014. Abstract S1-09.The genomic and
transcriptomic
architecture of 2,000
breast tumors reveals LumB
novel subgroups.
Curtis et al., Nature 2012
(PMID 22522925)
HER2E
Basal-like
LumA
LumA
(1q/16q)Identification of human triple-negative breast cancer subtypes and
preclinical models for selection of targeted therapies
• In silico analysis (21 breast cancer data sets in public genomic libraries)
• Gene expression profiles identified 587 TNBC cases
• Cluster analysis identified 6 TNBC subtypes displaying unique GE and ontologies, including 2
basal-like (BL1 and BL2), an immunomodulatory (IM), a mesenchymal (M), a mesenchymal
stem–like (MSL), and a luminal androgen receptor (LAR) subtype.
Lehmann BD et al, J Clin Invest. 2011;121:2750–2767.Heterogeneities in the Nomenclature and
Classification of TNBC
BRCA1 mutant
Immune system
and BRCAness
TNBC
ER-negative
PgR-negative
Basal-like EGFR and
HER2-negative
tumors cytokeratins
Claudin-low Different histologic
subtype subtypes
Metzger-Filho O, et al. J Clin Oncol. 2012;30:1879-1887 Lehman J Clin Invest 2010Targeting Heterogeneity of TNBC
Lehmann et al, JCI 2011
Multiple potential targets?
• Basal-like 1 and 2 – DNA damage response genes, growth factor paths (EGFR)
• Immunomodulatory - Immune approaches?
• Mesenchymal and mesenchymal / stem cell – PI3K/mTOR pathway
• LAR – androgen receptor signalingRESULTADOS
RESULTADOS
PAM50 (Nanostring nCounter) y Array HTA2.0 (Affymetrix)
PAM50 Subtipos de Lehmann
90
90 pacientes
pacientesRESULTADOS
RCp población estudio vs RCp Subtipos de Lehmann
Subtipos de Lehmann
100
90
80
70
Pacientes
60
50
Si RCp
40
30 No RCp
20
10
0
BL1 BL2 IM LAR M MSL
• Consiguen RCp el 30% de las • Pacientes BL1 consiguen un 50% de RCp
pacientes con CMTN mientras que las pacientes LAR consiguen
un 11% (p>0,05)San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center – Dec. 4-8, 2012
Approach
Profiling of triple-negative breast cancers after neoadjuvant
chemotherapy identifies targetable molecular alterations in the
treatment-refractory residual disease
Median Min Max
114clinically-defined
114 clinically-definedTNBC
TNBC
patients with RD after NAC Age 48 24 78
patients with RD after NAC
N %
Stage IIa 3 3%
IIb 5 5%
IIIa 13 12%
IIIb 77 69%
IIIc 10 9%
Nanostring digital
Immunohistochemistry
Immunohistochemistry Ki67, Nanostring digital expression NA 3 3%
expression analysis
Ki67, ER, PR, HER2, AR Taxane Yes 55 50%
ER, Pr, HER2, AR 112/114 analysis450
450genes
genes 89/114
112/114 No 53 48%
89/114
NA 3 3%
Menopause Pre 55 50%
Next generation sequencing
Next 182 oncogenes
generation and
sequencing
Post 53 48%
tumor suppressors NA 3 3%
182 oncogenes and tumor
81/114 Node status Pos 70 63%
suppressors 81/114
Neg 37 33%
NA 4 4%
This presentation is the intellectual property of the authors/presenters. Contact them at carlos.arteaga@vanderbilt.edu for
permission to reprint and/or distribute Balko et al. SABCS 2012Clinically Targetable Pathways in refractory TNBC
Balko et al. SABCS 2012CONCLUSIONES • El cáncer de mama triple negativo es una enfermedad heterogénea (basal-like+otros) • La quimioterapia es el tratamiento de elección. No está claro si hay un tratamiento superior a otros • Las sales de platino parecen ser mas eficaces en el subgrupo con mutación (o inactivación ) de BRCA • Los inhibidores de PARP son eficaces en el subgrupo con mutaciones de BRCA • La subclasificación genómica podría identificar nuevos tratamientos basados en el conocimiento de la biología del tumor
You can also read

















































