Trichotillomania and excoriation disorder: Primary care implications
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

lolostock
Trichotillomania and excoriation
disorder: Primary care implications
Abstract: Trichotillomania and excoriation disorder are two psychiatric conditions that have
similar origins to obsessive compulsive disorder. Both can cause patients significant distress
and lead to medical consequences. It is important that primary care NPs identify and refer
these individuals for psychiatric treatment.
By Debra A. Scrandis, PhD, CRNP-PMH, CRNP-F, and Ana C. Duarte, PhD, CRNP-PMH
bsessive compulsive disorder (OCD), seen in OCD, while at its essence suggests an anxiety dis-
O both medical and psychiatric realms, is com-
posed of two distinct types of symptoms.
order, is listed in the Diagnostic and Statistical Manual
of Mental Disorders, Fifth Edition (DSM-5) as its own
Obsessions are thoughts that are recurrent and intru- separate disorder due to the specific neurobiological
sive in individuals with the disorder. Compulsions are factors involved in its presentation. Two distinct disor-
actions taken to gain relief from the obsessive thoughts. ders falling under the OCD umbrella are trichotillo-
In combination, the disorder can be debilitating as the mania (TTM—hair pulling) and excoriation disorder
individual continues to have thoughts and a need to (skin picking). The former is specific to hair, while the
act on these thoughts repetitively. latter is specific to skin. Root causes of both are the
Keywords: excoriation disorder, obsessive compulsive disorder, psychiatric conditions, trichotillomania
www.tnpj.com The Nurse Practitioner • August 2021 51
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.Trichotillomania and excoriation disorder: Primary care implications
same, but the symptoms present in different locations pubic and perirectal regions.1,5 Skin picking usually
on the body.1 They are both considered under the um- involves the face, but can also include fingers, arms,
brella of body-focused repetitive behaviors. DSM-5 torso, legs, back, and pubic area.7 Behaviors in skin
criteria for TTM include recurrent pulling out of one’s picking include scratching, rubbing, removing skin
hair resulting in hair loss, while excoriation disorder parts, and pinching using finger nails, fingers, and/or
includes recurrent skin picking resulting in skin lesions. teeth.7 Inanimate objects such as pins, tweezers, and
Both disorders include the criteria of repeated attempts scissors may also be used in repetitive skin picking be-
to decrease or stop these behaviors.1 Individuals may haviors.7 Individuals with either or both disorders spend
perform these behaviors to help them manage their a significant amount of time doing these behaviors
anxiety, stress, or boredom.2,3 Etiologies are not known, similar to OCD. These behaviors can lead to medical
but there may be genetic and environmental problems, such as irreversible hair loss, skin lesions,
components.4 keloids, and infections.5
The following scenarios depict actual cases seen in While these disorders are relatively rare, they
clinical practice. may present with more frequency in the context of
• J.T. is a 30-year-old female who picks at the skin on increased anxiety resulting from the COVID-19 pan-
her fingers and scalp and is unable to stop these demic.8 Presentation of symptoms may first occur in
behaviors. She is experiencing hair loss on her head medical practices, where prompt identification and
and excoriations on her fingers, which she finds referral will result in appropriate treatment.
distressing and worries that other people will notice
these signs. She finds that her finger picking has ■ Neurobiology
increased more recently with her plan to move to a Excoriation disorder and TTM have similar structural
new home. and functional brain changes as OCD. Brain changes
• B.C. is a 17-year-old female with an anxiety disorder. in OCD involve the decision-making functions of the
She reports a strong urge to pull the hair on her scalporbitofrontal cortices and the movement-related
and pubic area, which provides relief for her anxiety. functions of the basal ganglia. Reportedly, there are
She is distressed by this behavior and wishes she had also reductions in cortical thickness in the parietal
the ability to stop. and temporal lobes, which are responsible for so-
matosensory and auditory func-
tions, respectively. These brain
Excoriation disorder and TTM have similar changes may contribute to de-
structural and functional brain changes creased control of habit formation
as OCD. for which the basal ganglia are
responsible.9
Changes are also seen in corti-
The prevalence of these disorders is up to 2% co-striato-thalamo-cortical (CSTC) neurocircuitry,
for TTM and 2% to 5% for excoriation disorder.5,6 which is involved in the expression of compulsive
One study reported that both disorders occur three behaviors.10 The CSTC circuit also plays an important
times more in females than males and adolescence as role in reward processing, habit formation, and motor
the average time of onset, although it also can begin control. In addition, it contributes to the awareness
in childhood.5 Comorbidities can include personality and recognition of significant behavioral stimuli, as
disorders, major depressive disorder, generalized anxi- well as regulation of goal-directed behavior. All of
ety disorder, and OCD.7 Body dysmorphic disorder these attributes of the CSTC neurocircuitry suggest
can also coexist in these individuals. Individuals may that it is an important area to target in the treatment
be conscious or unconscious of the repetitive of TTM and excoriation disorder, as it has been hy-
behaviors. pothesized that skin picking/hair pulling is a problem
Locations of hair pulling and skin picking vary. Hair with motor inhibition.10 Functional imaging in pa-
pulling can occur in any location where there is hair tients with OCD shows CSTC hypoactivation during
growth, most commonly the scalp, eyebrows, and eye tasks requiring inhibitory control, and a reduction in
lashes.1,5 Less common areas include axilla, face, and functional connectivity between inhibitory control
52 The Nurse Practitioner • Vol. 46, No. 8 www.tnpj.com
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.Trichotillomania and excoriation disorder: Primary care implications
and focus during cognitive tasks.9 Functional MRI
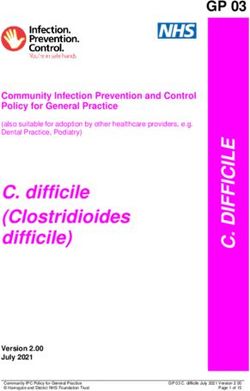
also suggests an increase in glutamate in the CSTC Common medication classes that can
circuit. Glutamate is the body’s main excitatory neu- contribute to hair loss
rotransmitter and is abundant in the central nervous Acne medications with Hormone replacement
system, making it a novel treatment target.11 vitamin A therapy
Sleep quality is a novel treatment target that is Amphetamines NSAIDs
implicated in both TTM and excoriation disorder, but Antibiotics and antifungals Oral contraceptives
the effects of poor-quality sleep are noted in the sever- Anticoagulants Parkinson disease
ity of hair pulling yet not skin picking. This suggests medications (levodopa)
the involvement of separate brain mechanisms in the Antihypertensives (ACEIs, SSRIs (paroxetine,
relationship of sleep to each disorder.12 Other emerg- beta-blockers, diuretics) sertraline, fluoxetine)
ing targets include inflammation and the immune Antiepileptic medications Steroids
system and the endocannabinoid system (ECS).13-15 (valproic acid)
ECS receptors are located in the same areas of the Chemotherapy Thyroid medications
brain involved in OCD, suggesting a link between the Cholesterol-lowering agents
ECS and OCD neural circuits. The function of the (clofibrate, gemfibrozil)
ECS is largely in maintaining homeostasis. It is also ACEI, angiotensin-converting enzyme inhibitor; SSRIs, selective serotonin
reuptake inhibitors; NSAIDs, nonsteroidal anti-inflammatory drugs
involved in immune function, reaction to stress, sleep, Adapted from www.medicalnewstoday.com/articles/326955
pain, rewarding, and arousal.15 The ECS prevents
increases in neuronal activation within the central
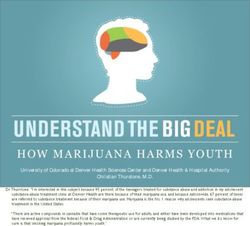
nervous system, thus producing calming and restful Common medication classes that can
contribute to allergic reactions and/or pruritus
effects.13-15
Antiarrhythmic medications Corticosteroids
■ Assessment Antibiotics Diabetes medications
The NP may find signs of hair loss or cutaneous lesions
Antiepileptic drugs Monoclonal antibody
on the skin during a physical exam or episodic visit. If therapy
there are signs or the patient presents with the complaint Antihypertensives Opioids
of hair pulling or skin picking, a thorough hair and skin ASA, NSAIDs Statins
assessment would be appropriate. The NP should look
Chemotherapy Thyroid medications
for cutaneous lesions and hair loss such as decreased
ASA, aspirin; NSAIDs, nonsteroidal anti-inflammatory drugs
hair density or patches of alopecia.5 In hair pulling, there Adapted from Reich A, Ständer S, Szepietowski JC. Drug-induced pruritus: a
are typically broken hair shafts of different lengths and review. Acta Derm Venereol. 2009;89(3):236-244. doi:10.2340/00015555-0650.
the alopecia may not show any scarring.5
It is important to rule out medical conditions, sub- and abscesses. Individuals with substance use may pick
stance use, and medications as the cause of these behav- or rub their skin due to restlessness, pruritus, or crawling
iors (see Common medication classes that can contribute sensations. Opioid withdrawal with symptoms including
to hair loss and Common medication classes that can con- agitation and piloerection can lead individuals to pick or
tribute to allergic reactions and/or pruritus). Actual hair rub their skin.16 Delusions of parasitosis, a relatively rare
loss from medical conditions, such as thyroid disease, condition in which the individual believes he or she has
hormone changes in the postpartum or perimenopausal insects or other organisms embedded in the skin with-
periods, alopecia, and tinea capitis, may be considered out any evidence of infestation, is another differential
as possible differential diagnosis for TTM. For excoria- diagnosis that may involve pruritus and excoriations.17
tion disorder, scabies, systemic pruritus, and acne may A psychiatric evaluation is appropriate for this suspected
be considered as differential diagnoses.7 Other disorders diagnosis.
that may involve skin picking include atopic dermatitis, Screening for underlying anxiety and depression
seasonal or environmental allergic reactions, contact would also be prudent using the Patient Health Ques-
dermatitis, basal cell carcinoma, and actinic keratosis. tionnaire 9 (PHQ-9) and the Generalized Anxiety
Substance use, such as use of heroin and methamphet- Disorder 7 (GAD-7) questionnaire, since these dis-
amine, can cause damage to the skin due to needle marks orders are frequently comorbid with TTM and
www.tnpj.com The Nurse Practitioner • August 2021 53
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.Trichotillomania and excoriation disorder: Primary care implications
excoriation disorder. Because poor sleep quality is It is important to note that there are no FDA-
typically present in both TTM and excoriation dis- approved medications for TTM or excoriation dis-
order, it is also wise to do a sleep assessment on in- order. As far as pharmacologic options, underlying
dividuals presenting with symptoms of either. 13 comorbidities need to be considered in deciding
treatment. More studies have been conducted on
■ Management TTM than excoriation disorder. One meta-analysis
The course of the disease for TTM and excoriation on TTM found that clomipramine, N-acetylcysteine,
disorder can vary but tends to be chronic and difficult and olanzapine had significant benefits compared with
to treat.5 Individuals may be hesitant or embarrassed placebo.19 A systematic review and meta-analysis on
to share their hair pulling and skin picking behaviors. treatment options found some evidence for the use
When communicating with these individuals, it is of SSRIs (fluoxetine, citalopram, escitalopram, fluvox-
important to acknowledge their distress and not mini- amine, and sertraline) in the treatment of excoriation
mize it. The use of alopecia medications would not be disorder, while other studies found little efficacy or
useful since hair pulling will continue without psychi- significant findings in TTM.4,10,18,19 The evidence for
atric interventions. Skin excoriations should be treated lamotrigine has been mixed.4 One meta-analysis found
for secondary infections if present, and if needed the large treatment effects for lamotrigine and SSRIs in
patient can be referred to dermatology. excoriation disorder and made the recommendation
There is evidence to support the use of cognitive that individuals seeking treatment for this disorder
behavioral therapy and habit reversal therapy and both may experience significant benefits regardless of treat-
might be the best initial treatment for excoriation dis- ment modality.18 As with anxiety disorders, SSRI doses
order and TTM.18,19 Cognitive behavioral therapy in- for OCD may need to be at higher levels than those
volves learning about unhealthy patterns of thoughts prescribed for major depression, which may relate to
that impact psychologic problems and behaviors. It has TTM and excoriation disorder.
Although excoriation disorder
Self-care methods to decrease the frequency and TTM are two distinct conditions,
of hair pulling and skin picking can include reviews of the literature largely yield
support for some of the same treat-
wearing hats or head wraps when appropriate ments that would target OCD be-
and keeping nails short or manicured. cause of their shared etiologies. In
addition to serotonergic agents, phar-
been found to be effective in treating anxiety disorders, macotherapies may include medications that target
excoriation disorder, and TTM. Habit reversal therapy N-methyl-d-aspartate and dopamine.11
includes training the patient on other behaviors that Glutamate studies are promising but not conclusive
are not compatible with hair pulling or skin picking, at present. Glutamate modulation in the CSTC can
identifying settings or activities that increase hair pull- potentially be treated with noninvasive and invasive
ing/skin picking (such as touching face or head) and procedures. Transcranial magnetic stimulation is a
altering activities to avoid these pulling/picking situa- noninvasive procedure, while surgical ablation and
tions, and conducting positive self-care at pulling and deep brain stimulation are invasive, of which only the
picking sites.20 Therefore, it would be important to latter is reversible. Modulation approaches can target
provide a therapy referral for these individuals. areas of interest in OCD, likewise they can help to
Self-care methods to decrease the frequency of hair further identify affected regions for more precise and
pulling and skin picking can include wearing hats or effective therapies.11
head wraps when appropriate and keeping nails short In light of anecdotal reports of OCD symptom
or manicured. For individuals with underlying anxiety relief by patients who use cannabis, the ECS is another
disorders, other methods for anxiety relief include area worthy of study as a target for novel treatments.
meditation, mindfulness, relaxation therapy, and ex- Recent research in the use of cannabidiol for issues
ercise. Recognizing stressful situations and using stress such as anxiety and fear response, in addition to FDA
balls where the hands are busy may decrease hair pull- approval for two rare epilepsies of childhood, bode
ing and skin picking. well for continued research in this area.15
54 The Nurse Practitioner • Vol. 46, No. 8 www.tnpj.com
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.Trichotillomania and excoriation disorder: Primary care implications
A few small studies have found immunologic dif- REFERENCES
ferences between adults with OCD and healthy controls, 1. American Psychiatric Association. Diagnostic and Statistical Manual of
Mental Disorders: DSM 5. 5th ed. 2013.
which suggests an immune system role in OCD. The 2. Graham R, Soares NS. What are the DSM-5 diagnostic criteria for exco-
antibiotic minocycline and cyclooxygenase-2 (COX-2) riation (skin-picking) disorder? Medscape. 2018. www.medscape.com/
answers/1122042-169038/what-are-the-dsm-5-diagnostic-criteria-for-
inhibitors have provided some relief from obsessional excoriation-skin-picking-disorder.
symptoms in studies. Also, probiotics, which aim to 3. Elson DM. Trichotillomania. Medscape. 2019. https://emedicine.medscape.
com/article/1071854-overview#a3.
decrease inflammation, have recently become a treat-
4. Sani G, Gualtieri I, Paolini M, et al. Drug treatment of trichotillomania
ment of interest for this new target. Additional research (hair-pulling disorder), excoriation (skin-picking) disorder, and nail-biting
is needed in this area both to understand the mecha- (onychophagia). Curr Neuropharmacol. 2019;17(8):775-786.
5. Jones G, Keuthen N, Greenberg E. Assessment and treatment of trichotil-
nisms and to develop treatments.13,14 lomania (hair pulling disorder) and excoriation (skin picking) disorder.
More than 100 therapeutic trials for OCD and Clin Dermatol. 2018;36(6):728-736.
6. Grant JE, Chamberlain SR. Prevalence of skin picking (excoriation) disorder.
related conditions are currently ongoing worldwide, J Psychiatr Res. 2020;130:57-60.
mostly in the areas of neuromodulation and psycho- 7. Torales J, Díaz NR, Barrios I, et al. Psychodermatology of skin picking (exco-
therapy. Approximately 20% of these trials are in- riation disorder): a comprehensive review. Dermatol Ther. 2020;33(4):e13661.
8. Pathoulas JT, Olson SJ, Idnani A, Farah RS, Hordinsky MK, Widge AS.
vestigating new pharmacologic therapies targeting Cross-sectional survey examining skin picking and hair pulling disorders
glutamate and the immune system. Additionally, novel during the COVID-19 pandemic. J Am Acad Dermatol. 2021;84(3):771-773.
9. Grant JE, Chamberlain SR. Exploring the neurobiology of OCD: clinical
therapies such as psychedelics, catechol-o-methyl- implications. Psychiatr Times. 2020;2020.
transferase inhibitors, and endocannabinoid modula- 10. Fineberg NA, Apergis-Schoute AM, Vaghi MM, et al. Mapping compulsiv-
tors are being studied. In addition to new medication ity in the DSM-5 obsessive compulsive and related disorders: cognitive
domains, neural circuitry, and treatment. Int J Neuropsychopharmacol. 2018;
options, authors of one review recommend that 21(1):42-58.
continued studies narrow focus even further, toward 11. Goodman WK, Storch EA, Sheth SA. Harmonizing the neurobiology and
treatment of obsessive-compulsive disorder. Am J Psychiatry. 2021;178(1)
biomarkers for more personalized and effective :17-29. doi:10.1176/appi.ajp.2020.20111601.
treatment.13 12. Cavic E, Valle S, Chamberlain SR, Grant JE. Sleep quality and its clinical
associations in trichotillomania and skin picking disorder. Compr Psychiatry.
Overall, there is no single-line treatment for TTM or 2021;105:152221.
excoriation disorder. Though some of these new treat- 13. Grassi G, Cecchelli C, Vignozzi L, Pacini S. Investigational and experimental
drugs to treat obsessive-compulsive disorder. J Exp Pharmacol. 2021;12:695-706.
ments are promising for OCD, and possibly TTM and
14. Marazziti D, Mucci F, Fontenelle LF. Immune system and obsessive-compulsive
excoriation disorder, it is still prudent to refer patients disorder. Psychoneuroendocrinology. 2018;93:39-44.
to a psychiatric specialist to ensure best outcomes. 15. Kayser RR, Snorrason I, Haney M, Lee FS, Simpson HB. The endocan-
nabinoid system: a new treatment target for obsessive compulsive disorder?
Cannabis Cannabinoid Res. 2019;4(2):77-87.
■ Conclusion 16. Lipman ZM, Yosipovitch G. Substance use disorders and chronic itch. J Am
Acad Dermatol. 2021;84(1):148-155.
J.T. is unable to take SSRIs due to elevated hepatic
17. Ansari MN, Bragg BN. Delusions of parasitosis. In: StatPearls. Treasure
enzymes and presented with a rash with lamotrigine. Island, FL: StatPearls Publishing; 2020. www.ncbi.nlm.nih.gov/books/
NBK541021/.
She currently gets manicures and found her picking
18. Selles RR, McGuire JF, Small BJ, Storch EA. A systematic review and meta-
decreased once she relocated to the new home. She is analysis of psychiatric treatments for excoriation (skin-picking) disorder.
currently receiving cognitive behavioral therapy. Gen Hosp Psychiatry. 2016;41:29-37.
19. Farhat LC, Olfson E, Nasir M, et al. Pharmacological and behavioral treat-
B.C. was prescribed an SSRI for her anxiety with ment for trichotillomania: an updated systematic review with meta-analysis.
minimal improvement in her hair pulling. She received Depress Anxiety. 2020;37(8):715-727.
20. Himle JA, Bybee D, O’Donnell LA, et al. Awareness enhancing and monitor-
a referral for habit reversal therapy and was advised to ing device plus habit reversal in the treatment of trichotillomania: an open
work on methods such as exercise and nutrition to feasibility trial. J Obsessive Compuls Relat Disord. 2018;16:14-20.
improve her anxiety.
TTM and excoriation disorder can have a detri- Debra A. Scrandis is an associate professor at the University of Maryland School
mental impact on patients. It is important for primary of Nursing, Baltimore, Md.
care NPs to identify these disorders, as well as allow
individuals to share their distress and refer them to Ana C. Duarte is an assistant professor at the University of Maryland School of
Nursing, Baltimore, Md.
mental health providers, such as psychiatric mental
health NPs and therapists. Several self-care techniques, The authors and planners have disclosed no potential conflicts of interests,
such as exercise, can be recommended for patients financial or otherwise.
empowering them to take some control over these
symptoms. DOI-10.1097/01.NPR.0000753840.44209.51
www.tnpj.com The Nurse Practitioner • August 2021 55
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.You can also read