Influence of Folic Acid on Postprandial Endothelial Dysfunction
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Influence of Folic Acid on Postprandial
Endothelial Dysfunction
Hanneke W. Wilmink, Erik S.G. Stroes, Willem D. Erkelens, Wim B. Gerritsen, Robert Wever,
Jan-Dirk Banga, Ton J. Rabelink
Abstract—Triglyceride-rich lipoproteins that circulate postprandially are increasingly being recognized as potentially athero-
genic. These particles also have been shown to cause endothelial dysfunction. We recently demonstrated that acute parenteral
administration of folic acid restores endothelial function in vivo in patients with increased LDL cholesterol levels. In vitro data
suggested that this effect could be mediated by a reduction of radical stress. In the present study, therefore, we evaluated the
effect of an acute oral fat load on both endothelial function and oxygen radical production. Next, we studied whether 2 weeks
of pretreatment with 10 mg folic acid PO could prevent these fat-induced changes. We conducted a prospective, randomized,
placebo-controlled study to evaluate the effect of oral folic acid administration (10 mg/d for 2 weeks) on basal endothelial
function as well as endothelial function on an acute fat load in 20 healthy volunteers 18 to 33 years old. Endothelial function
was assessed as flow-mediated dilatation (FMD). Endothelium-independent dilatation was measured after sublingual
nitroglycerin spray. Oxygen radical stress was assessed by measurement of the urinary excretion of the stable radical-damage
end product malondialdehyde. During administration of placebo, FMD decreased significantly after an acute oral fat load, with
a median from 10.6% (8.3% to 12.2%) to 5.8% (3.0% to 10.2%), P,0.05. During folic acid administration, FMD was
unaffected by a fat load, with a median from 9.6% (7.1% to 12.8%) to 9.9% (7.5% to 14.1%), P5NS. The increase in
malondialdehyde excretion in the urine after fat loading was also prevented during folic acid administration (absolute increase
after an acute fat load during placebo, 0.1160.1 mmol/L versus folic acid, 0.0260.1 mmol/L, P,0.05). The response to the
endothelium-independent vasodilator nitroglycerin remained unaltered throughout the study. Pretreatment with oral folic acid
prevents the lipid-induced decrease in FMD as well as the lipid-induced increase in urinary radical-damage end products.
Because these observations were made in healthy volunteers with normal folate and homocysteine levels, it is suggested that
a higher folate intake in the general population may have vasculoprotective effects. (Arterioscler Thromb Vasc Biol.
2000;20:185-188.)
Key Words: endothelial function n malondialdehyde n triglyceride-rich lipoproteins n folic acid
T riglyceride-rich lipoproteins have been shown to stimu-
late atherogenesis in both humans and animal models.1–3
In recent observations, these lipid particles could also ad-
In the present study, we evaluated the effect of postprandial
lipemia on endothelial function, assessed as flow-mediated
dilation (FMD), and radical stress, measured as the excretion of
versely affect the antiatherosclerotic properties of the endo- oxidative-damage end products in the urine before and after fat
thelium, mainly by interfering with the L-arginine–NO path- loading. Using a randomized, placebo-controlled crossover
way.4 – 6 Even a transient increase in triglyceride-rich study design, we subsequently tested whether 2 weeks of oral
lipoproteins may alter vascular functions, such as endotheli- pretreatment with folic acid can prevent the lipid-induced
um-dependent vasodilatation.7 changes in endothelial function and/or redox dysregulation.
We have recently demonstrated that acute parenteral ad- Because the studies were carried out in healthy volunteers with
ministration of the active form of folic acid, normal folate and homocysteine levels, the observations made in
5-methyltetrahydrofolate (5-MTHF), restores endothelial our study may give an indication of the vasculoprotective effect
function in patients with familial hyperlipidemia character- of dietary folate intake in the general population.
ized by increased LDL cholesterol levels.8 In these patients,
decreased NO bioavailability may relate to both decreased Methods
production and increased degradation of NO. In in vitro
Subjects
studies, 5-MTHF was able to scavenge oxygen radicals,8 Twenty healthy volunteers 18 to 33 years old participated. All
suggesting that 5-MTHF in vivo may improve NO availabil- individuals were normotensive (systolic blood pressure
ity by preventing NO degradation by oxygen radicals. ,160 mm Hg and diastolic blood pressure ,90 mm Hg) and had no
Received March 29, 1999; revision accepted July 9, 1999.
From the Divisions of Internal Medicine (H.W.M., W.D.E., J.-D.B.) and Nephrology and Hypertension (E.S.G.S., T.J.R.), University Hospital Utrecht;
the Department of Clinical Chemistry, Sint Antonius Hospital Nieuwegein (W.B.G.); and the Department of Clinical Chemistry, University Hospital
Utrecht (R.W.).
Correspondence to Prof Dr T.J. Rabelink, Department of Nephrology and Vascular Medicine, F 03.226, University Hospital Utrecht, Heidelberglaan
100, 3584 CX Utrecht, Netherlands. E-mail t.rabelink@digd.azu.nl
© 2000 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org
Downloaded from http://atvb.ahajournals.org/
185 by guest on November 8, 2015186 Arterioscler Thromb Vasc Biol. January 2000
history of cardiovascular disease or family history of premature TABLE 1. Characteristics of the Study Group Before an Oral
vascular disease. All subjects had normal plasma folate (.6.8 Fat Load After Placebo and Folic Acid Treatment
nmol/L) and homocysteine (,15.5 mmol/L) concentrations. Fasting
triglyceride and cholesterol concentrations were ,2.0 mmol/L and Placebo Folic Acid
4.5 mmol/L, respectively. The subjects did not use medication. The Participants, n 20 20
study was approved by the Medical Ethics Committee of the
University Hospital Utrecht, and written informed consent was Age, y 23 (3.4)
obtained from all participants. Male sex, % 50
Smoking, % 20 20
Study Design 2
Body mass index, kg/m 22.8 (2.6) 21.9 (2.7)
A randomized, double-blind, placebo-controlled crossover trial was
performed comparing 10 mg folic acid PO versus placebo. A dose of Systolic blood pressure, mm Hg 135 (14.8) 137 (14.1)
10 mg folic acid was chosen to reach optimal folic acid saturation Diastolic blood pressure, mm Hg 69 (8.8) 69 (9.2)
during a relatively short (2 weeks) protocol. All subjects were
Folate, nmol/L 13.7 (3.9) 701 (207.4)*
randomly assigned to receive either oral folic acid or placebo
treatment for 2 weeks, followed by the forearm vasomotion study. Homocysteine, mmol/L 7.2 (2.1) 5.0 (0.7)*
After an 8-week washout period, subjects were crossed over to MDA, mmol/L 0.12 (0.10) 0.18 (0.12)
placebo or folic acid, respectively, for another 2 weeks, again
followed by the second vasomotion study. The dosage of folic acid Vessel size, mm 4.0 (0.5) 4.1 (0.4)
was estimated to cause increments in plasma folate similar to those FMD, % 10.6 (8.3–12.2) 9.6 (7.1–12.8)
previously observed with acute infusion of 5-MTHF.8 The vasomo- NTG, % 19.7 (15.6–24.9) 16.8 (10.4–22.8)
tion study consisted of assessment of FMD and nitroglycerin-
induced vasodilation (see below) before and after a standard oral fat Values are percentages, means, or medians, with SD or 25th–75th
load. The fat load consisted of 50 g fat (in the form of whipped percentile in parentheses.
cream, 40% fat) per square meter body surface.9 *P,0.05 vs placebo.
All subjects refrained from drinking caffeine-containing beverages,
smoking, and eating for 12 hours before the vasomotion studies. At each
expressed as median (25th to 75th percentile), and statistical tests on
visit, blood samples were drawn for laboratory determinations of
ranks were used. Differences in FMD at baseline between the treatment
triglycerides, total cholesterol, HDL cholesterol, folate, and homocys-
teine concentrations before and 4 hours after an oral fat load. At each periods were tested with a 1-way repeated-measures ANOVA on ranks.
visit, urine was collected before the oral fat load and 3 to 6 hours after Differences in FMD before and after lipid load within 1 treatment
the oral fat load for determination of excretion of the stable oxidative- session were tested with the Wilcoxon signed rank test. If variance ratios
damage end product malondialdehyde (MDA). reached statistical significance, differences were analyzed with the
Student-Newman-Keuls test for a value of P,0.05.
Lipid changes before and after lipid load and between treatment
Forearm Vasomotion Study groups were tested by paired-samples t test with Bonferroni
The ultrasound measurements were performed at the elbow of the correction.
right arm, with the subject in the supine position, with a vessel MDA is presented as mean6SD. Comparisons between groups
wall–movement system (Wall Track System, Pie Medical), which were made by repeated-measures ANOVA and Student’s t test.
consists of an ultrasound imager with a 7.5-MHz linear array Differences between changes in FMD and MDA before and after
transducer connected to a data acquisition system and a personal lipid load between the placebo and folic acid treatment sessions were
computer.10 In short, an optimal 2D B-mode image of the brachial
tested with 1-way repeated-measures ANOVA.
artery was obtained. An M-line perpendicular to the vessel was
Correlation testing was performed by linear regression. Differ-
selected. Next, the ultrasound system was switched to M-mode, after
ences were considered significant at a value of P,0.05.
which the storage of data was begun. The vessel-movement detector
system registered end-diastolic vessel diameter repeatedly during a
period of 5 to 6 cardiac cycles. This procedure was performed 3 Results
times. The measurements were averaged to provide a baseline The characteristics of the study group before an oral fat load
diameter measurement. after either placebo or folic acid treatment are given in Table
By inflation of a blood pressure cuff for 4 minutes at a pressure of 1. There were no statistically significant differences between
100 mm Hg above the systolic blood pressure, ischemia was applied
to the forearm distal to the location of the transducer. Ultrasonogra-
baseline parameters during the placebo and folic acid treat-
phy continued for 3 minutes after cuff release, with measurements at ment periods, ie, lipid parameters (Table 2), basal arterial
30-second intervals. The widest lumen diameter was taken as a diameter, and basal FMD and NTG.
measure for maximal diameter. After 10 minutes of rest, allowing the During placebo therapy, fat loading induced an increase in
artery to return to its baseline diameter, sublingual nitroglycerin triglyceride levels, whereas the other lipid parameters re-
spray was administered as an endothelium-independent dilator.
Measurements were obtained for another 5 minutes at 1-minute mained unaltered (Table 2). FMD was impaired after the fat
intervals. load (Figure). FMD decreased from a median of 10.6% (8.3%
FMD and nitroglycerin-induced dilatation (NTG) were expressed to 12.2%) to 5.8% (3.0% to 10.2%), P,0.05, whereas NTG
as a percentage change relative to baseline diameter. remained unaffected (preprandial NTG, 19.7% [15.6% to
24.9%]; postprandial NTG, 18.0% [13.3% to 21.6%],
Laboratory Determinations
P5NS). Urinary MDA concentration in the urine (expressed
High-performance liquid chromatographic analysis was used to
measure MDA in urine, as described previously.11 A good reproduc- as the ratio of the urinary creatinine), a stable oxygen
ibility of the method was found, with an intrarun coefficient of radical– damage end product, also demonstrated a significant
variation of 3.1% for MDA and a detection limit of 0.2 mmol/L.11 increase on fat loading (baseline MDA, 0.1260.10 mmol/L;
The measurement of MDA in urine shows an excellent resolution, after fat load, 0.2260.12 mmol/L, P,0.05). Values are
and the component is easy to identify.
summarized in Table 3.
Statistical Analysis During folic acid therapy, plasma levels of folate increased
Group values are expressed as mean6SD. Because of failure of the significantly, from 13.7 nmol/L before to 701.0 nmol/L after
normality test for FMD data andDownloaded fromand
NTG data, FMD http://atvb.ahajournals.org/
NTG values are by guest
treatment on November
(P,0.05). 8, 2015 levels decreased during folic
HomocysteineWilmink et al Folic Acid and Endothelial Function 187
TABLE 2. Preprandial and Postprandial Lipid Values During Placebo and Folic
Acid Treatment
Cholesterol, mmol/L HDL, mmol/L Triglyceride, mmol/L
Placebo Folic Acid Placebo Folic Acid Placebo Folic Acid
Preprandial 4.4 (0.7) 4.4 (0.7) 1.4 (0.3) 1.5 (0.3) 1.0 (0.4) 1.1 (0.5)
Postprandial 4.4 (0.7) 4.5 (0.7) 1.4 (0.3) 1.5 (0.2) 1.8 (0.8)* 1.8 (0.8)*
Values are means with SDs in parentheses.
*P,0.05 vs preprandial values.
acid treatment (Table 1; P,0.05). Preprandial FMD was com- vessel size (P50.87), FMD (P50.17), NTG (P50.10), MDA
parable to preprandial FMD during placebo, 10.6% (8.3% to (P50.22), and homocysteine (P50.99).
12.2%) versus 9.6% (7.1% to 12.8%) after folic acid treatment.
The basal excretion of MDA was also comparable to placebo Discussion
therapy (0.1260.10 versus 0.1860.13 mmol/L, P5NS, placebo In the present study, we demonstrate that an acute fat load is
versus folic acid treatment) (Table 3). Whereas the rise in associated with increased excretion of oxidative end products
triglyceride levels after fat load was unaffected by folic acid in the urine of healthy volunteers. Acute fat loading also
therapy (Table 2), the impairment in FMD was completely causes a sharp decrease in FMD. Both increased radical
prevented (Table 3). Accordingly, the change in FMD (differ- damage and impaired FMD can be prevented by oral pretreat-
ment with folic acid.
ence between preprandial and postprandial) was significantly
Evidence has accumulated that triglyceride-rich lipoproteins
different between placebo and folic acid treatment (Figure). The
play an important role in the atherogenic process. Accordingly,
increase in urinary MDA concentration was also annihilated by
the impaired remnant clearance in, eg, diabetes, familial com-
folic acid therapy (Table 3). Again, the change in MDA
bined hyperlipidemia, and renal insufficiency has been put
(difference between preprandial and postprandial) was signifi-
forward as an important risk factor for future cardiovascular
cantly different during placebo and folic acid treatment (placebo, disease.3,5 In support of this hypothesis, it has been shown in
0.1160.10 versus folic acid, 0.0160.08, P,0.01). The response both in vivo and in vitro studies that remnant lipoproteins are
to the endothelium-independent vasodilator nitroglycerin re- associated with impaired endothelium-derived NO activity,4,6,7
mained unaffected (Table 3). which is a key to the antiatherosclerotic properties of the
By using an independent t test, we tested whether there was endothelium.12 In the present study, we also demonstrate a
any carryover effect of folic acid after an 8-week washout consistent decrease in FMD on lipid loading.
period. There was no significant difference in the sum of Previous studies have shown that NO is the main determi-
responses of subjects receiving placebo followed by folic acid nant for FMD.13 Triglyceride-rich lipoproteins may impair
compared with the sum of responses of subjects receiving FMD by compromising production of NO as well as increas-
folic acid followed by placebo. This test was performed for ing degradation of NO by, eg, oxygen radicals.14,15 Using a
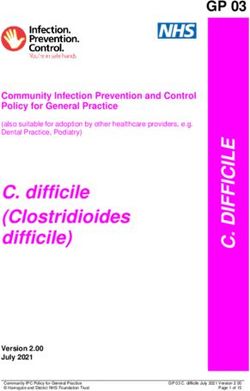
Change in postprandial FMD compared
with preprandial FMD during placebo
and folic acid treatment. The bars repre-
sent means with SEMs. First bar shows
change in FMD (postprandial minus pre-
prandial) during placebo. Second bar
shows change in FMD (postprandial
minus preprandial) during folic acid treat-
ment. *P,0.05, change in FMD during
placebo compared with folic acid
treatment.
Downloaded from http://atvb.ahajournals.org/ by guest on November 8, 2015188 Arterioscler Thromb Vasc Biol. January 2000
TABLE 3. Brachial Artery Responses and MDA Concentrations diabetes and familial combined hyperlipidemia. It is also of
After an Oral Fat Load Preceded by Placebo and Folic interest that higher dietary folate intake apparently may also
Acid Treatment protect healthy humans from daily fat-associated endothelial
Time, h insults. This may imply that in the general population as well,
a higher folate intake may be vasculoprotective.
0 4
FMD, % Acknowledgments
Placebo 10.6 (8.3–12.2) 5.8 (3.0–10.2)* E. Stroes was supported by a fellowship from the Dutch Heart
Foundation. We thank Michel Hijmering for expert technical advice.
Folic acid 9.6 (7.1–12.8) 9.9 (7.5–14.1)
NTG, % References
Placebo 19.7 (15.6–24.9) 18.0 (13.3–21.6) 1. Bradley WA, Gianturco SH. Triglyceride-rich lipoproteins and athero-
Folic acid 16.8 (10.4–22.8) 16.9 (15.2–20.8) sclerosis: pathophysiological considerations. J Intern Med Suppl. 1994;
736:33–39.
MDA, mmol/L 2. Karpe F, Hamsten A. Postprandial lipoprotein metabolism and athero-
Placebo 0.12 (0.10) 0.22 (0.12)† sclerosis. Curr Opin Lipidol. 1995;6:123–129.
3. Hodis HN, Mack WJ. Triglyceride-rich lipoproteins and progression of
Folic acid 0.18 (0.13) 0.2 (0.13) atherosclerosis. Eur Heart J. 1998;19:A40 –A44.
Values are means or medians with SD or 25th–75th percentile in parenthe- 4. Grieve DJ, Avella MA, Elliott J, Botham KM. The influence of chylo-
ses. micron remnants on endothelial function in the isolated perfused rat aorta.
*P,0.05 vs preprandial values. Atherosclerosis. 1998;139:273–281.
†P,0.05 vs preprandial values. 5. Karpe F, Steiner G, Uffelman K, Olivecrona T, Hamsten A. Postprandial
lipoproteins and progression of coronary atherosclerosis. Atherosclerosis.
1994;106:83–97.
stable isotope technique, we recently demonstrated that 6. Kugiyama K, Hideki D, Motoyama T, Soejima H, Misimu K, Kawano H,
(whole-body) NO production was unimpaired in hypercho- Nakagama O, Yoshimura M, Ogawa H, Matsumura T, Sugiyama M,
Nakano T, Nakajima K, Yasue H. Association of remnant lipoprotein
lesterolemic patients.14 In line with this, in vitro studies have
levels with impairment of endothelium-dependent vasomotor function in
shown that oxidative inactivation of NO is predominant in human coronary arteries. Circulation. 1998;97:2519 –2526.
hyperlipidemia.15,16 Our present data extrapolate this concept 7. Plotnick GD, Corretti M, Vogel RA. Effect of antioxidant vitamins on the
to the postprandial state in healthy volunteers. transient impairment of endothelium-dependent brachial artery vasoac-
tivity following a single high-fat meal. JAMA. 1997;278:1682–1686.
Oral supplementation of folic acid completely prevents the
8. Verhaar MC, Wever R, Kastelein J, van Dam T, Koomans H, Rabelink TJ.
increase in oxygen radical stress and the impairment in FMD 5-Methyltetrahydrofolate, the active form of folic acid, restores endothelial
after an acute fat load. The mechanism by which folic acid function in familial hypercholesterolemia. Circulation. 1998;97:237–241.
exerts beneficial effects on redox state and endothelial func- 9. Castro Cabezas M, de Bruin TW, Westerveld HE, Meijer E, Erkelens W.
Delayed chylomicron remnant clearance in subjects with heterozygous
tion simultaneously after an acute fat load can be explained in familial hypercholesterolaemia. J Intern Med. 1998;244:299 –307.
several ways, as follows. 10. Wilmink H, Banga JD, Hijmering M, Erkelens W, Stroes E, Rabelink T.
Folic acid may increase NO production by NO synthase. Effect of angiotensin-converting enzyme inhibition and angiotensin II
Folic acid has been suggested to increase endogenous regen- type 1 receptor antagonism on postprandial endothelial function. J Am
Coll Cardiol. 1999;34:140 –145.
eration of tetrahydrobiopterin, an essential cofactor for NO
8
11. Gerritsen WB, Aarts LP, Morshuis WJ, Haas FJ. Indices of oxidative
synthase.17 Such an effect of folate may result in decreased stress in urine of patients undergoing coronary artery bypass grafting. Eur
2
NO synthase– dependent O2 formation as well as increased J Clin Chem Clin Biochem. 1997;35:737–742.
NO production (Reference 18; E.S.G.S, unpublished obser- 12. Anggard E. Nitric oxide: mediator, murderer, and medicine. Lancet.
1994;343:1199 –1206.
vations). Alternatively, as folate is reduced by the gastroin- 13. Joannides R, Haefeli WE, Linder L, Richard V, Bakkali EH, Thuillez C,
testinal tract into 5-MTHF, endothelial uptake of 5-MTHF Luscher TF. Nitric oxide is responsible for flow-dependent dilatation of
(which can reduce the oxidative defense mechanisms into an human peripheral conduit arteries in vivo. Circulation. 1995;91:1314–1319.
active oxidant state by donating electrons) may improve the 14. Wever R, Stroes E, Rabelink TJ. Nitric oxide and hypercholesterolemia: a matter
of oxidation and reduction? Atherosclerosis. 1998;137(suppl):S51–S60.
endothelial redox state. In general, folic acid has been shown 15. Ohara Y, Peterson TE, Harrison DG. Hypercholesterolemia increases
to possess direct scavenging effects in vitro.8 endothelial superoxide anion production. J Clin Invest. 1993;91:
Finally, the well-known homocysteine-lowering effect of 2546 –2551.
folic acid could contribute to improvements of endothelial 16. Anderson RA, Evans LM, Elli GR, Jackson SK, Lewis MJ, Rees A,
Fronnaux MP. Postprandial lipaemia is associated with increased free
dysfunction. 19,20 However, in the present study, this mecha- radicals and deterioration in endothelial function in non-insulin dependent
nism probably cannot explain the observed effects on endo- diabetes. Eur Heart J. 1998;A3305. Abstract.
thelial function, because the folic acid–induced decrease in 17. Wever R, van Dam T, van Rijn H, de Groot P, Rabelink TJ. Tetrahydro-
biopterin regulates superoxide and nitric oxide generation by recombinant
homocysteine concentrations was not associated with
endothelial nitric oxide synthase. Biochem Biophys Res Commun. 1997;
changes in baseline FMD. 237:340 –344.
In conclusion, our data indicate that oral treatment with 18. Stroes ES, Hijmering M, van Zandvoort M, Wever R, Rabelink TJ, van
folic acid restores endothelial dysfunction and abolishes the Faassen EE. Origin of superoxide production by endothelial nitric oxide
synthase. FEBS Lett. 1998;438:161–164.
increase in radical-damage end products induced by triglyc-
19. Pancharuniti N, Lewis CA, Sauberlich HE, Perkins LL, Go RC, Alvarez
eride-rich lipoproteins. In combination, these data imply that JO, Macaluso M, Acton RT, Copeland RB, Cousins A, et al. Plasma
folic acid enhances NO bioavailability through inhibition of homocyst(e)ine, folate, and vitamin B-12 concentrations and risk for
lipid-induced oxygen radical stress. These data underscore a early-onset coronary artery disease. Am J Clin Nutr. 1994;59:940 –948.
20. Van den Berg M, Boers GH, Franken DG, Blom HJ, Van Kamp GJ,
potential beneficial effect of folic acid supplementation for Jakobs C, Rauwerda JA, Kluft C, Stehouwert CD. Hyperhomocys-
cardiovascular prevention strategies, especially in patients teinaemia and endothelial dysfunction in young patients with peripheral
with an impaired cholesterol remnant clearance,
Downloaded such as in
from http://atvb.ahajournals.org/ by guest
arterial on November
occlusive 8, J2015
disease. Eur Clin Invest. 1995;25:176 –181.Influence of Folic Acid on Postprandial Endothelial Dysfunction
Hanneke W. Wilmink, Erik S. G. Stroes, Willem D. Erkelens, Wim B. Gerritsen, Robert Wever,
Jan-Dirk Banga and Ton J. Rabelink
Arterioscler Thromb Vasc Biol. 2000;20:185-188
doi: 10.1161/01.ATV.20.1.185
Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272
Greenville Avenue, Dallas, TX 75231
Copyright © 2000 American Heart Association, Inc. All rights reserved.
Print ISSN: 1079-5642. Online ISSN: 1524-4636
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://atvb.ahajournals.org/content/20/1/185
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the
Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of the Web
page under Services. Further information about this process is available in the Permissions and Rights
Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online
at:
http://atvb.ahajournals.org//subscriptions/
Downloaded from http://atvb.ahajournals.org/ by guest on November 8, 2015You can also read