THIS IS LONG-TERM CARE 2018 - Ontario Long Term Care Association
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

THIS IS LONG-TERM CARE 2018

It’s natural to want to stay in our own homes as we age, but that
isn’t possible for everyone. Many people, particularly those with
dementia, will eventually need a level of support and supervision
that family, friends, and home care can no longer provide.
Ontario’s long-term care homes provide support to more than
100,000 people and their families every year. Homes offer 24/7
nursing care and supervision, support with daily activities, and
a safe, caring environment, helping people live comfortably and
with dignity.
Who lives in long-term care?
Seniors whose dementia In one-third of residents, stage in the progression of
has progressed to the this impairment is severe.1 their conditions, when their
middle or advanced stages In recent years the Ontario health is more likely to be
are the core population in government has been unstable, they are more
long-term care homes. Two investing more funds in physically frail, and their
out of three (64%) residents home care and aging- care is more complex.
9
have been diagnosed with at-home strategies. New In particular, an increasing
OUT OF 10 Alzheimer’s disease or residents to long-term number of residents are
RESIDENTS another dementia. Overall, care must now have “high” admitted to long-term care
90% of residents in long- or “very high” physical at a later stage of their
HAVE COGNITIVE term care have some form and cognitive challenges dementia, with increasing
IMPAIRMENT of cognitive impairment, in order to qualify for needs for support with daily
not solely from dementia admission. This means that activities.
but from other causes such people are now coming to
as stroke and memory loss. long-term care at a later
Higher needs, more care
The Ontario Long Term described as borderline years ago. At the same
Care Association analyzed or mildly impaired time, the number of long-
data over the last five years, (7% decrease).1, 2 term care residents who can
from 2011-12 to 2016-17. There have also been carry out daily activities
During that short time, steady year-over-year without assistance has
there has been a steady dropped by half, from
1 in 3 increase in the number
increases in the number of
people who need extensive approximately 6% to 3%.1, 2
of new residents with
HAVE SEVERE moderate and moderately
or complete support with These increasing high
everyday activities such as needs have significant
COGNITIVE severe cognitive getting dressed or feeding implications for the support
impairment (6% increase),
IMPAIRMENT with a corresponding
themselves. Today, 85% of that residents need, and
long-term care residents the additional staffing and
decrease in the number need extensive or complete funding that homes require
of new residents who don’t help with daily activities, to provide this support.
have cognitive impairment, compared to 77% just five
or whose function is
2 This is Long-Term Care 2018
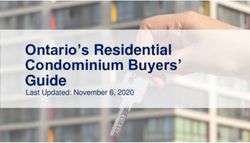
2016-17 85%
2015-16 83%
2014-15 82%
2013-14 81%
2012-13 79%
2011-12 77%
More residents need extensive
or complete support
Over the last five years alone, the proportion of residents who need
extensive or complete support with daily activities such as eating and
getting dressed has increased by more than 7%, from approximately 77%
to 85%. Data source: Canadian Institute for Health Information, Continuing
Care Reporting System (CCRS 2011-2012 to CCRS 2016-2017).
A changing culture
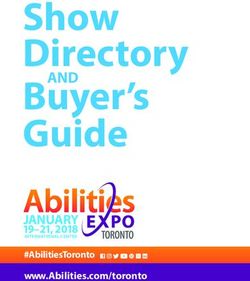
6%
INCREASE
6%
INCREASE
8%
INCREASE
9%
INCREASE
12%
INCREASE
At the same time that the are provided through a
DRESSING PERSONAL TRANSFER TOILET BED population is changing, sensitive understanding of
HYGIENE USE MOBILITY so too is the culture of each resident’s individual
long-term care. Like many needs and preferences.
More residents need support
other areas of health care, Even when someone has
with important daily activities
long-term care was built advanced dementia, long-
The majority of residents in long-term care need help with daily activities on what is often called term care homes provide
such as getting dressed, getting out of bed, and toileting. This figure an “institutional” model, a life of purpose and
shows the rise over a five-year period in resident needs for physical focused primarily on connection, as the stories
assistance from one or more staff with these activities. The increased providing physical and in this report illustrate.
needs for support are accompanied by a need for more staff time, skills, medical care. This is Long Term Care is
and resources to provide care. Data source: RAI-MDS 2011-12 to 2016-17,
That is changing rapidly. designed to provide readers
Ontario Ministry of Health and Long-Term Care, Intellihealth Ontario.
Caring for medical and with a better understanding
physical needs is still very of what homes do, the
important, but homes people they serve, and
are shifting to a resident- some context behind the
1 in 3
centred or relationship- headlines.
centred approach, where
care and quality of life
RESIDENTS ARE HIGHLY
OR COMPLETELY
DEPENDENT ON STAFF
This is Long-Term Care 2018 3
A caring community
A movement to holistic, person-centred care has been
rapidly evolving over the last decade, changing the
way we think of disabilities and dementia, as well as what
“The change we are experiencing is a
change in the culture of LTC; a sweeping,
we expect from services such as hospitals, home care, cleansing movement that embraces
and long-term care homes. As a society, we have been person-centred care. The picture of
redefining what good care means for those with
dementia, and what people really need. living life in LTC is changing to a full
In person-centred care, the focus is on the person’s recognition of the wholeness of each
preferences and their emotional and social needs, person, even those living with severe
in addition to physical and health care needs. This is cognitive or physical changes. Teamwork
a movement away from caring for residents according
to set schedules and routines, to caring for residents is flourishing, empathy is growing, a social
according to their lifetime practices, habits, and model of living is sweeping over our LTC
preferences — even if those can be hard to decipher homes, replacing the institutional model
in the face of advanced dementia.
of care that has existed for decades. Great
work is being done across our province!”
What does resident-centred care look like? – Dee Lender, Executive Director, Ontario Association
Hush, no rush of Residents’ Councils
Bloomington Cove, a residents according to
Sienna Senior Living home, their lifetime practices Staff continuously try DementiAbility program,
was the Ontario Long and habits. new programs and care which has rolled out across
Term Care Association’s techniques that improve all Jarlette homes.
Residents are offered each resident’s quality
Resident-Centred Home choices of meals, clothes, The program teaches staff
of the Year in 2016. In this of life. Craniosacral techniques for engaging
programs, and bathing. treatments have led to a
specialty home, every A Hush, No Rush care residents with dementia
resident has a diagnosis reduction of antipsychotic and introducing activities
philosophy reminds medications and have
of dementia. staff to adjust the way that leverage their abilities,
improved speech, appetite, passions, and curiosities.
Bloomington Cove has they approach residents, and sleep. Doll therapy
moved away from caring programs, and physical The idea is that by keeping
is a particular source of residents active and
for residents according space. This includes comfort for residents who
to staff schedules and supporting natural engaged, they have a richer
have difficulty falling quality of life and fewer
routines to caring for wake-up times. asleep, and for those who challenging behaviours
experience continuous that are often a side effect
pacing as a result of their of dementia.
disease; sitting with dolls
provides them with rest and
reduces the risk of falls. The “We had one resident who
home also uses a technique was often agitated. We
called Gentle Persuasive learned that she always
Approach to respond cooked and made sure
respectfully and skilfully to everyone else was taken
the challenging behaviours care of before eating. So
that can accompany we got her involved in
dementia. escorting residents into
the dining room, clearing
Focusing on abilities tables, and helping staff
Leacock Care Centre, get dinner ready. She
a Jarlette Health Services enjoys the activity and
home, received the you could see it gave her
Ontario Long Term Care a sense of purpose. She’s
Association’s Quality also a great help to staff in
Improvement Innovation the dining room!”
of the Year Award in – Leacock Care Centre staff
2017 for its use of the
4 This is Long-Term Care 2018
78,872 BEDS
FOR LONG-STAY
RESIDENTS
Living and working together 80,000 STAFF
Dedicated staff in long- Some homes are also
term care homes provide experimenting with the use “As a young nurse,
daily care and supervision of staff such as porters and when I found long- What about
when someone’s needs have health care aides to support term care, I knew I was more staff?
become too great to be resident care, but these home. It’s a community:
cared for at home by family positions are not currently you build relationships In late 2017, the
and community supports. eligible for funding from with residents and provincial government
the government. families that just committed to an
While the most visible staff aren’t possible in other additional 15 million
at a home are registered Residents' Council settings.” – Candace care hours per year for
nurses, registered practical Chartier, RN, CEO, long-term care, to bring
nurses, and personal Each home has a Residents’
Ontario Long Term the provincial average
support workers (PSWs) Council, which has powers
Care Association for resident care to four
who provide the daily under the Long Term Care
hours a day. This is good
health care and support, Homes Act to approve
cognitive impairment can news but a tall challenge,
there are many other people certain decisions in the
no longer make decisions as there is currently a
involved in each resident’s home (such as the menu),
about their care, and a recognized workforce
care and support. Each provide the resident’s
family member or friend shortage in both long-
home has a medical director perspective and advice to
serves as the "substitute term care and home care.
along with other health the home’s leadership, and
professionals and support help to support resident- decision maker" who is The Association believes
staff in areas including centred care. regularly consulted by the that this new funding
pharmacy, dietary, long-term care home about commitment also needs
Families and volunteers the resident’s treatment to be accompanied by
physiotherapy, occupational
therapy, recreation therapy/ Families are not just and quality of life. Each changes to the Long
resident engagement, visitors; they are a crucial home's Family Council Term Care Homes Act
social work, housekeeping, part of the care team. The is also empowered by the that currently puts tight
maintenance, and majority of people with Act to advise the home restrictions on the type
administration. moderate to severe about meeting the needs of staff and roles of staff
of residents. — restrictions that don’t
Volunteers also support exist for staff in home
“Long-term care homes do an amazing job. Your first- care, for example. Long-
line health care workers, the PSWs, are jewels. There individual residents and
programs that enrich the term care needs more
aren’t enough of them, and they don’t get rewarded flexibility to be able to
enough, but they still have the drive to come into life of the home.
provide the care that
work every day and deal with me with empathy, which residents need.
impresses me.” – Bill Jarvis, long-term care resident and
OLTCA Lifetime Achievement Award recipient 2017
This is Long-Term Care 2018 5
2 OUT OF 3
LONG-TERM CARE
RESIDENTS
HAVE DEMENTIA
The specialty of dementia care
Physical space
A lzheimer’s disease and other dementias
are complex, progressive, and
ultimately fatal conditions. When families
Providing personal care and medical
treatments requires a specialized approach
because dementia is often accompanied by
matters
The design of a home’s
can no longer manage to care for their challenging behavioural symptoms, also environment is important
loved ones at home, long-term care homes called responsive behaviours (see more for improved privacy,
offer the support and services they need, about behavioural symptoms on page 8). dignity, and quality of life.
along with expertise in dementia and When people with dementia don’t Nearly half of Ontario’s
end-of-life care. understand what is happening, they may long-term care homes
The general perception of dementia is react negatively when staff approach are due for significant
that it primarily involves memory loss to help with daily activities or medical renovation or rebuild
and confusion. What’s not well understood treatment. They may refuse verbally or in order to meet current
is that as the brain deteriorates because physically to have a bath, to eat a meal, design standards that
of the dementia, the organs that it directs or to have a dressing changed. Even include more private rooms
will deteriorate as well. As the disease something as simple as hair combing and more lounges, wider
progresses into middle and later stages — or a fingernail trim can be confusing or hallways, and smaller, more
which is usually when most people come frightening, triggering angry or fearful intimate dining rooms in
to long-term care — they have lost responses, including physical aggression. every resident area.
the ability to speak or understand Caring for someone with dementia requires The right design can also
speech, to accurately interpret what’s a compassionate understanding of the help to reduce dementia-
happening around them, and to care for many different ways that the disease can related behaviours. Resident
themselves. For example, they may no affect each individual, and experimenting altercations are more likely
longer recognize that they need to eat, with behavioural management strategies in older homes, where
or what utensils are for. that soothe the resident’s symptoms, four-bed rooms, crowded
People in these stages of the disease improve his or her quality of life, and allow hallways, and limited
need extensive or complete help with staff to provide care. lounge space create an
daily activities such as personal hygiene, environment that lacks
toileting, and eating. The vast majority privacy and is too close
of people also have two or more health for comfort.
conditions that require treatments and The provincial government
medications. is providing a capital
redevelopment program to
help older homes redevelop,
“Roughly 70% of people who live with dementia will eventually live but there are still a number
at the end of their lives in a long-term care home, because of barriers, including
of the nature of the disease. Long-term care is an excellent setting insufficient construction
funding and excessive
for palliative care for people with dementia, while of course municipal development
understanding that people are still living life to the fullest.” charges, that are making
– Mary Schulz, Director, Education at Alzheimer Society of Canada it difficult for all homes
to participate.
6 This is Long-Term Care 2018
Making connections
Behavioural Supports Ontario (BSO) Long-term care homes care for the physical, medical,
Some excellent behavioural management social, spiritual, and emotional needs of their residents.
programs have been implemented in recent years People who have dementia have all these needs, but they
that are helping to reduce behavioural symptoms may need help in tapping into the activities, memories,
and improve residents’ quality of life. Homes have and relationships that provide them with a sense of
been using a variety of strategies with success. purpose and meaning.
One of the biggest contributors to homes’ ability
Long-term care homes use a variety of therapies
to implement behaviour management strategies is
including personalized music, art, and animals to help
a provincial program called Behavioural Supports
improve mood, reduce pain, and reduce dementia-related
Ontario, because it is accompanied by the funding
behaviours. These activities create moments of pleasure
to hire and train specialized staff teams.
for people with dementia, and treasured moments of
BSO rolled out in 2012 in a limited number of connection with their families and staff.
homes, and has been shown to be effective in
But it’s not just these
supporting the shift to a behaviour management
therapies that are making a
approach and in reducing severely aggressive
difference. Many residents
behaviour, antipsychotic use, and restraint use.3
were accustomed to an
In the 2017 provincial budget, the government active life with multiple
committed to fund BSO teams in each of the responsibilities. It can give
province’s 625 long-term care homes. them a sense of renewed
These teams are critically needed. Frontline staff purpose to work alongside
are juggling the needs of many residents and most staff to help set the table,
need to continuously increase their knowledge sweep the floor, fold towels,
of how to manage challenging behaviours. BSO and water plants. Homes
teams are their support system — they provide report that involving
education about dementia, problem-solve and residents in meaningful
suggest strategies, and help to create a culture activities typically reduces
where all staff are focusing on making each day responsive behaviours and
better for every resident. allows staff to form closer
relationships.
Sensitive care, successful care
Having a blood test can Maintaining good accustomed to being in at bathtime are given a
be upsetting for people with nutrition and hydration charge in a health care personalized playlist on
dementia if someone simply can be challenging, as environment. The staff headsets about 20 minutes
shows up to take blood. One people with dementia can gave her a clipboard and before bathtime and during
home has incorporated doll lose interest in eating a checklist, include her the bath if needed. Familiar
therapy for their residents and drinking. It can take in their home’s nursing music is known to be
to help ease this stress. some creativity. One home meetings, and speak to her pleasurable and calming
About 20 minutes before discovered that one of their as a former nurse manager for people with dementia.
the blood test, staff bring residents used to love Coca when they are providing her Each of these examples
in a doll and involve the Cola, and found he will take care. These are familiar and comes from a home with
resident in talking about chocolate nutritional drinks comforting activities that a Behavioural Supports
it. Then they explain the if they call them his Coke. make her feel in control, Ontario team as part of
blood test is coming, and A resident who was a and her resistance to care their staff. Research shows
ask the resident to show former nurse manager has stopped. that staff in homes with BSO
the baby how to be brave. would become agitated and Many people with teams feel significantly more
Many residents did this yell at staff when they tried dementia are resistant to supported and capable of
for their own children, and to provide her care. After having a bath because they developing solutions that
it taps into that memory. observing her behaviour don’t like to be wet, or they help their residents and
Mechanical pets are equally and talking to her family, don’t understand what is reduce behaviours
effective for some people. they concluded she was happening. In one home, in the home.3
reacting because she was residents who struggle
This is Long-Term Care 2018 7
Long-term care homes prefer to call these reactions
“responsive behaviours” because the person is responding
to a trigger in their environment. Very little of this is true
aggression; the behaviour is unfortunately mislabelled
by the national reporting system that provides statistics.
Aggression implies malicious intent, and this is rarely
the case.
Behaviour management approaches work well in reducing
the frustration and irritation level of individuals as well
as the overall level of resident-on-resident tension in
a home. This involves finding ways to engage people
with dementia in productive activities that tap into their
pleasurable memories, current abilities, and sense of
Understanding aggressive behaviour self. Homes also create activities to diffuse common “hot
spots” for resident altercations, such as mealtimes. As
I n the course of their disease, 80% of residents will exhibit
behavioural symptoms of dementia, such as pacing and
wandering, repetitive questioning or actions, uninhibited
mentioned earlier, long-term care homes need Behavioural
Supports Ontario teams in every home in order to support
their work in this area.
behaviour (including sexual), and irritability. 4 These
behaviours can unfortunately aggravate and intrude on
“When George first arrived, he would yell at residents
the space of other residents. As dementia destroys social
and staff and raise his fist. He’s a big man and that was
skills and the ability to manage emotions, residents
intimidating. We learned from his family that he had
may react reflexively by hitting, or by using angry and
been a real doer, someone who liked to tinker about in
accusatory responses.
the garage. So we built him a cart full of tools and things
The vast majority of altercations between residents to tinker with, all attached to the cart with sturdy chains
with dementia are minor and result from the belief that so they don’t pose a threat to anyone else. We also gave
someone is intruding on their space or behaving in a George the job of sweeping the floor in the dining room
way that frustrates or angers them. Sometimes the cause after meals with our staff. He’s a man who needs to be
makes sense to us, as when another resident wanders busy and by having these jobs to do, it has significantly
into their room and rummages in their dresser; many reduced his anger and frustration.” – BSO team member
times it does not.
A word about abuse
No abuse of a resident is The definition has a very All incidents, even when According to a report by
ever acceptable. Long-term low threshold. For example, staff are uncertain, are Ontario's Auditor General,
care homes have a zero- if a resident with dementia documented and reported only a small number of
tolerance approach to this swatted away another to the Ministry of Health reported incidents that
very serious issue. resident's hand when they and Long-Term Care for required inspections were
When the current Long- both reached for something follow up. considered a “high risk”
Term Care Homes Act at the dinner table, homes More serious incidents concern by the Ministry.5
came into force in 2010, must report this as abuse. certainly do occur and these Any incidents of suspected
it introduced very specific From a staff perspective, examples are not intended or confirmed abuse are
definitions of physical, behaviour and language to minimize the importance taken extremely seriously
verbal, and sexual that might have been of zero-tolerance reporting, by long-term care homes.
abuse, along with new acceptable a generation ago, but they do illustrate the
requirements for reporting such as calling a resident types of behaviour that the
and managing any “dearie”, is now considered public might be surprised to
suspected incident. disrespectful and requires find classified as “abuse”.
reporting as verbal abuse.
8 This is Long-Term Care 2018
Not suitable for Responding to concerns
long-term care
In early 2018, CBC aired a misleading series on resident-on-resident violence in long-term
Residents who are known care. The thoughtful response below was written by Dr. William Reichman, President and CEO
to have severe violent of Baycrest Health Sciences and former president of the American Association for Geriatric
tendencies do not respond Psychiatry. Excerpted and reprinted with permission.
to behaviour management
strategies, and they require Dementia is among the most devastating Occasionally this aggression can be
the care of a psycho- health conditions associated with growing predicted and prevented, but often it is
geriatrician and/or 1 to 1 older, with Alzheimer’s disease being the remarkably impulsive and occurs very
supervision to keep other most prevalent cause. Over the past suddenly. At present, we do not have
residents and staff safe. several decades, as the ability of families medications that adequately prevent
In several tragic cases, to cope with the many stresses of aggression without also so thoroughly
people who were extremely dementia caregiving have mounted, tranquilizing individuals that they
violent were suffering from long-term care facilities in Ontario and cannot safely move about, communicate,
a severe psychiatric illness across the world have become the places or meaningfully engage in social,
or had a history of physical we look to in order to best meet the needs recreational or other activities that
or sexual violence — of affected patients and to give their support quality of life.
sometimes in combination families respite. This is hard, grinding As a society we have rightly chosen to
with dementia. Long-term work as patients with dementia need avoid limiting the freedom of movement
care is not a suitable place assistance in nearly all activities that of affected patients living in long-term
for people with severe the rest of us might effortlessly take care homes — we do not think it is morally
psychiatric conditions for granted. right to physically restrain or lock up
or a history of violence, Along with the cognitive deficits of in seclusion our loved ones who are
who need specialized care dementia, in which patients are forgetful, suffering from terrible brain diseases that
where they are not among have difficulty communicating, cannot cause them to behave in ways they would
frail and vulnerable elders. adequately organize themselves or likely never choose.
When homes are informed problem-solve effectively, nearly all Some believe that more staffing would
of a prospective resident get confused navigating familiar solve the issue of assaultive behaviour.
with severe psychiatric surroundings. At mid to later stages The reality is that we have very limited
illness or a history of of severity, these individuals need help useful data to tell us the extent to which
violence, they are currently dressing, bathing, eating and having increased staffing levels for dementia care
not allowed by legislation their daily care needs met. would reduce the occurrence of resident-
to refuse them. This needs While the work is demanding of all of us to-resident violence and by what amount.
to change. who have dedicated our careers to this We do know it would likely be impossible
field, it is also immensely rewarding and to completely eliminate the risk if patients
of great benefit to families — that is why with dementia continue to live together
we do it. in congregate care settings, such as the
One of the greatest challenges in caring contemporary long-term care home.
for patients with dementia is that the The CBC Marketplace episode titled
disorder often results in changes in Crying Out For Care, which first aired
behaviour and emotional control. This is on January 26, 2018, highlights a serious
very troublesome and has to be addressed public health challenge that will grow in
when patients are cared for in their own importance as the global population ages.
homes by family members as well as by We want to talk about this issue, but it
staff in long-term care facilities. People must be in a responsible, thoughtful way
46% of residents affected with dementia can get easily
excited or upset, be verbally abusive to
that informs the public. As a society, as
well as focusing on care, we must also
exhibit some level of others, resist care, are suspicious, and at focus public efforts on brain health and
times, might engage in violent behaviour. invest resources into the prevention,
aggressive behaviour diagnosis and treatment of brain diseases
related to their like Alzheimer’s. Eradicating these
threats to our well-being should be a
cognitive impairment major priority.
or mental health
condition
This is Long-Term Care 2018 9
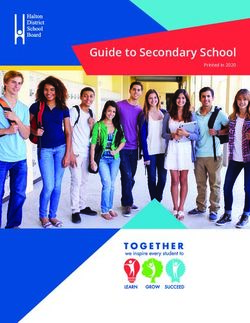
OUTSTANDING Committed to quality of care
RESULTS OVER
JUST FIVE YEARS S ince 2012, thanks to a new national reporting system, all long-term care homes in
Ontario have been able to track the care they are providing. This new data provides
homes with invaluable information about the quality of care they provide, and how they
compare to other homes. It helps staff to identify where they can improve quality of care,
and helps residents and families to see how their home is performing in key areas.
Recent data analysis shows that over the last five years, homes have made great strides
in improving care outcomes for their residents. In particular, they have made outstanding
improvements in reducing the use of restraints, pain management, and reducing
Restraint use has antipsychotic medications.1,2
dropped by more
than half
2016-17
2015-16
Increase in quality
Nearly 40% fewer
residents are 2012-13 2013-14 2014-15
being prescribed
antipsychotics
Quality improvement at a glance
This graph shows the outstanding work that homes have accomplished in improving quality of care across all
50% fewer residents areas since 2012, when the data was available to help guide their efforts.
are experiencing pain The blue bar represents a composite score for the nine areas of care (indicators) that are tracked and reported
publicly: antipsychotics, experiencing pain and worsening pain, restraint use, depression, wounds (pressure ulcers),
falls, and physical functioning (both improving and worsening).6
90% OF Long-term care homes do well on inspections
LONG-TERM Long-term care home Homes take this However, at a 2018 meeting
CARE HOMES DO operators adhere to commitment seriously. on workforce challenges
Ontario’s Long Term Ministry findings show in long-term care, many
WELL ON THEIR Care Homes Act, widely that the vast majority of participants identified
INSPECTIONS considered one of the homes (90%) do well on the inspection process as
toughest pieces of nursing their inspections.7 highly demoralizing for
home legislation in the world. Staff are proud of the their teams. They stressed
Homes are inspected care they provide, that inspections need to
annually by the Ministry the relationships they move away from a punitive
of Health and Long-Term build with residents, approach to a focus on
Care against more than and the work they do supporting staff with
600 regulations — to meet the stringent quality improvement.
with more than 1,000 requirements of the Act.
requirements — that look at
everything from cleanliness
to resident safety.
10 This is Long-Term Care 2018A closer look at antipsychotics
The understanding of dementia, and how to provide
appropriate care, has undergone a significant evolution
in the last decade. Many residents come to long-term care
on an antipsychotic medication that was prescribed in the
hospital or community. Until recently, it was believed that
they would need to stay on that medication permanently.
There is now greater understanding that dementia
symptoms wax and wane over time, and someone who
needed an antipsychotic to manage symptoms at one stage
of the disease may not need it later. Antipsychotics still
have an important role in reducing major symptoms for
some residents, such as severe
aggression or paranoia, so the
focus in homes is on ensuring
that antipsychotics are used
appropriately, not eliminated
entirely. The goal is to ensure
antipsychotics are prescribed
for the right symptoms, at the
right dose, and only for as long
as needed.
The importance of innovation
Over the next 20 years it is The Ontario Long Term
anticipated that there will Care Association is also
be twice as many seniors leading a major project to
over the age of 75 and, by implement standardized
extension, a growth in the clinical guidelines in all
number who need long-term long-term care homes Clinical Support Tools
care and other supports. (see Clinical Support Tools Long-term care staff would benefit from having
Even with the recent this page), researching standardized, evidence-based guidelines and protocols
announcement of another different models of that are written specifically by people who know long-term
30,000 long-term care beds residential care for seniors care — practical documents that address the real-world
over the next decade, there (see LTC Plus, page 14), environment of long-term care.
will not be enough capacity and leading a Strategic
to meet all of these needs. Innovation Council of Last year, the Ontario Long Term Care Association
government, academics, started an innovative project to develop these Clinical
The way to meet the future Support Tools. Ontario’s Ministry of Health and Long-
needs of Ontario’s seniors and educational partners
to generate actionable Term Care has provided significant project funding and
is by evolving our current the first phase of the project is underway. Guidelines are
ways of doing business, recommendations to
accelerate innovation in being developed for diabetes, dementia, incontinence,
and taking action now. wound care, end-of-life care, chronic obstructive
Long-term care homes are long-term care and the
broader health sector. pulmonary disease (COPD), and seasonal influenza/
actively driving innovation respiratory virus prevention.
by leading and partnering Two major challenges with
to design and test new innovation in long-term Long-term care homes have been quick to sign on to
tools and technologies care are the Long Term Care participate. They are committed to quality improvement,
to improve quality of care Homes Act and the current and eager for tools and support that are tailored specifically
and quality of life and funding model, as both for the unique needs of long-term care residents.
reduce administrative are very restrictive and
tasks for staff, allowing make it difficult for homes
them to spend more time to try new ways of doing
on resident care. things. The Ontario Long
Term Care Association has
raised this concern with
the government.
This is Long-Term Care 2018 11The need for long-term care
Long-term care is in high demand. As of October 2017,
there were nearly 34,000 people waiting for a bed. The
wait lists have been growing at an astounding rate in the
last two years alone (see below). The average wait time for
placement is now 143 days. 8
625 homes are licensed In late 2017, the Ontario government announced that it
would be funding 30,000 more long-term care beds over
and approved to operate in Ontario the next decade, with 5,000 of those in the next four years.
58% of homes are privately owned Growth in wait list for long-term care
24% are non-profit/charitable
The wait list for Ontario long-term care is growing rapidly by approximately
15% a year. Source: Long-Term Care Home System Reports, Ontario
16% are municipal
Ministry of Health and Long-Term Care, October 2017.
2% other
35K
33,775
30,326
78,872 “long stay” beds provide
30K
permanent, residential care 25,530
to more than 100,000
25K
23,018
people each year
20K
SOURCE: Long-Term Care Home System Reports, Ontario Ministry 2015
01-15 02-15 03-15 04-15 05-15 06-15 07-15 08-15 09-15 10-15 11-15 12-15 2016
01-16 02-16 03-16 04-16 05-16 06-16 07-16 08-16 09-16 10-16 11-16 12-16 2017
01-17 02-17 03-17 04-17 05-17 06-17 07-17 08-17 09-17 10-17
of Health and Long-Term Care, October 2017.
Rebuilding and expanding long-term care
In addition to new beds, and rural communities. this funding has not been commitment of added
there is a significant These communities often sufficient for many homes capacity will help support
program underway have limited home care or to participate, particularly this goal.
to renovate or rebuild retirement home options, for small homes and those The Association has
approximately 300 older and are typically the only found in urban areas, also requested improved
homes — almost half of place where frail seniors which lack available and/or construction funding, a
the system’s supply. can receive support, close affordable land to build on. reduction or elimination
These homes need to to home and families. In its 2018 pre-budget of municipal development
be upgraded to current The government currently submission (More charges, the creation
design standards such provides all long-term Care. Better Care), the of an urban homes
as sprinklers in resident care homes in need of Ontario Long Term Care strategy, and a small
rooms, on-site generators, redevelopment with Association asked the homes retention strategy
and more spacious and construction funding based province for added capacity, reinforced by additional
private accommodations on a “per resident, per day” focused specifically on operating funding. These
for residents. model, similar to the way “topping up” redevelopment additional measures
More than 40% of all long- it funds operations. This projects to avoid the need to be included in
term care homes are small, approach provides equal need for amalgamation, the government’s capital
with 96 or fewer beds, funding for all homes to particularly in more redevelopment program
and nearly half of these participate, regardless of rural and remote areas. in order to support broader
homes are located in small home location. However, The government’s recent participation.
12 This is Long-Term Care 2018Daily rate set by government
that residents pay the
home for “room and board”
(accommodation and food)
Basic:
$59.82
Semi-Private:
$68.02–$72.12
Private:
$78.27–$85.45
SOURCE: LTC Home Accommodation
Charges Bulletin, Ontario Ministry of Health
and Long-Term Care, May 2017.
How long-term care works PROVINCIAL
FUNDING FOR
In Ontario, long-term care is regulated and funded by the provincial LONG-TERM CARE,
government. Government agencies called Local Health Integration 2017
Networks (LHINs) do the assessments to determine who is eligible
to be admitted to long-term care, and they manage the wait lists.
Long-term care homes in Ontario are owned and operated by a variety
$4.1 billion
of different operators including individuals, family-owned businesses, (7.7% of overall health budget)
Approximately $96.26 per
private corporations, publicly traded companies, non-profits and charities,
and municipal governments (municipalities are required by legislation
to operate at least one long-term care home). There’s a wide range in how resident, per day for nursing and
they function: some long-term care homes are part of large corporations,
while others are stand-alone independents. personal care such as assistance
Each home owner/operator is granted a licence to operate by the with personal hygiene, bathing,
government, which then provides funding for the staff and supplies eating, and toileting
to provide nursing and personal care, resident programs and support
services, and raw food (used to make meals). Homes are required to $11.82 per resident, per day for
follow the requirements of the Long Term Care Homes Act, and are
inspected annually to ensure that they are complying with the more specialized therapies, recreational
than 600 regulations. programs, and support services
Residents are required to pay a copayment that ranges between
approximately $1,800 and $2,600 a month, depending on whether $9 per resident, per day for raw
accommodation is a basic, semi-private, or private room. In essence, this food (ingredients used to prepare
resident copayment covers their “room and board”. The government sets
the rate, while offering subsidies to those who can’t afford the copayment. meals, including nutritional
This payment for resident accommodation is what long-term care homes supplements)
use to pay expenses such as non-care staff, utilities, and mortgages as well
SOURCES: 2017 Ontario Budget; 2017 Long-Term Care
as expenses that support infection control, regular building maintenance, Home Level-of-Care Per Diem Funding Summary,
and major capital repairs (such as a roof or heating system). Ontario Ministry of Health and Long-Term Care.
This is Long-Term Care 2018 13POST-ACUTE SPECIALIZED THE HUB CONTINUUM DESIGNATED
CARE CARE OF CARE ASSISTED
LIVING
Looking to the future
How does our health care system need to evolve to meet the needs of seniors?
At the moment there is only one type of long-term care home in Ontario, providing 24-hour
personal and nursing care for a population with advanced physical and cognitive decline.
There are regulations, admission criteria, and funding models that currently affect the kinds
of residents that long-term care homes are able to accept. But with flexibility and innovation,
long-term care could offer so much more.
In 2011, an expert panel made a number of key recommendations about expanding the
current model of care to a number of different options. These models of care build on current
long-term care homes and their expertise to provide a broader range of services to Ontario’s
seniors. Many of the models have been applied in the United States and other jurisdictions,
and some components have been implemented on a small scale in some Ontario homes. The
expert panel believed these models could be expanded more broadly in Ontario. Doing this
would improve the options currently available to provide care to seniors and free up much-
needed beds within existing long-term care homes.
Called Long Term Care Plus, these models of care could offer so much more than the
traditional long-term care model that is currently funded in the province. Each model
of Long Term Care Plus may require additional staff, equipment and training, a different
mix of staff, or changes to the physical environment. The Ontario Long Term Care
Association is currently researching these models of care and identifying the legislative,
regulatory, and policy changes that would be required to allow seniors in Ontario flexibility
in the care they need.
14 This is Long-Term Care 2018About the Ontario
References Long Term Care Association
1. Canadian Institute for Health Information
(2017). Continuing Care Reporting System:
Profile of Residents in Continuing Care
Facilities 2016-2017. Ottawa: CIHI.
2. Canadian Institute for Health Information
(2012). Continuing Care Reporting System:
Profile of Residents in Continuing Care
Facilities, 2011-2012. Ottawa: CIHI.
3. Grouchy M., Cooper N., Wong T. (2017).
Implementation of Behavioural Supports
Ontario (BSO): An evaluation of three
models of care. Healthcare Quarterly,
19(4) January 2017: 39-73.
4. Ballard C. (2008). Int Rev of Psychiatry.
Vol 20, Issue 4: 296-404.
5. Office of the Auditor General of Ontario.
(2015). Annual Report 2015. Toronto:
Queen's Printer for Ontario.
6. Wilkinson A., Haroun V., Cooper N.,
Wong T., & Chignell M. (2018). Developing
a Composite Quality Score to Support
Performance Improvement in Long Term
The Ontario Long Term Care Association
Care. Poster presentation at the Canadian
Association for Health Services and is the largest association of long-term
Policy Research (CAHSPR), May 29-31, care providers in Canada and the only
Montreal, QC.
association that represents the full mix
7. Office of the Auditor General of Ontario. of long-term care operators — private,
(2017). Annual Report 2015, Vol 2: Follow-up
Reports on 2015 Annual Report. Toronto: not-for-profit, charitable, and municipal.
Queen's Printer for Ontario.
The Association represents nearly 70%
8. Ontario Ministry of Health and Long-Term
Care, Long-Term Care System Reports, of Ontario’s long-term care homes,
October 2017. located in communities across the
province. Our members provide care
and accommodation services to more
than 70,000 residents annually.
Photo credits
The Association would like to thank the residents For more information,
and staff of Kensington Health, the O'Neill please contact info@oltca.com
Centre, Schlegel Villages, Woodingford Lodge,
Tilbury Manor and Trinity Village for the photos
used in this report.425 University Avenue, Suite 500 Toronto, Ontario M5G 1T6 Tel: 647-256-3490 info@oltca.com www.oltca.com This is Long-Term Care 2018 April 2018 With the exception of those portions of this document for which a specific prohibition or limitation against copying appears, the balance of this document may be produced, reproduced and published in its entirety, in any form, including in electronic form, for educational or non-commercial purposes, without requiring the consent or permission of the Ontario Long Term Care Association, provided that an appropriate credit or citation appears in the copied work as follows: Ontario Long Term Care Association. (2018). This is Long-Term Care 2018. Toronto, Ontario: Ontario Long Term Care Association. © 2018 Ontario Long Term Care Association The Association would like to thank our Corporate Alliance Partners for their sponsorship of this report.
You can also read