THE RESULTS OF A SURVEY TO UNDERSTAND THE BLOOD SUPPLY SYSTEMS IN WESTERN EUROPEAN COUNTRIES - Rijksoverheid
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

REPORT TO
THE NETHERLANDS
MINISTRY OF HEALTH, WELFARE, AND SPORT
PHARMACEUTICAL AFFAIRS AND MEDICAL TECHNOLOGY
ON
THE RESULTS OF A SURVEY TO UNDERSTAND
THE BLOOD SUPPLY SYSTEMS IN
WESTERN EUROPEAN COUNTRIES
Conducted under Public Service Contracts ARVODI-2016
Contract number 201700274.003.001
February 2018 Revision
TABLE OF CONTENTS
Executive Summary ......................................................................................................................2
Chapter 1. Introduction and Terms of Reference ....................................................................4
Chapter 2. The Survey ...................................................................................................................6
Survey design – who, what, how; collaboration with EBA
Blood Supply Organizations surveyed
Response to Survey
Chapter 3. Structure of Report.....................................................................................................8
Chapters, charts (maps), and what is covered by the text
Chapter 4. Blood Supply Systems.................................................................................................9
Summary of results – charts with commentary, question by question
Other key points
Chapter 5. Blood Components for Transfusion ........................................................................17
Summary of results – charts with commentary, question by question
Other key points
Chapter 6. Plasma for PDMPs ....................................................................................................26
Summary of results – charts with commentary, question by question
Other key points
Chapter 7. Conclusions................................................................................................................44
Responders and Non-Responders
Recent Dynamic Changes
How the Netherlands/Sanquin Fits In
Appendices
A. Sample Questionnaire ........................................................................................................47
B. Brief Summary of Responding Countries and Their Blood Systems ................................56
C. Individual Responses to Supplementary Questions ...........................................................81
D. Malta Responses ................................................................................................................87
E. Abbreviations Used ............................................................................................................88
F. Acknowledgements ............................................................................................................90
G. About the Authors ..............................................................................................................91
1
EXECUTIVE SUMMARY
A survey was designed by the Dutch Ministry of Health to better understand the blood
supply systems in Western European countries. This includes how the blood supply is regulated
in other countries and how this differs from the situation in the Netherlands.
The survey was developed for online response, and tested, refined, and the results
analysed by a contract supplier. It was sent to 30 countries within Europe, all members of, or an
observer to, the European Blood Alliance. These 30 countries have an estimated 2018 population
of 470 million.
A total of 22 countries responded for a response rate of 73%. These 22 responders have a
population of about 392 million, or 83% of the total. The responders included 20 countries that
are members of the European Union and two that also follow the EU Directives for blood and
plasma products.
Overall, the results of the survey were largely self-explanatory and met the expectations
of the researchers.
The majority of Western European blood systems are operated by the government, either
locally or nationally. This reflects the way healthcare is also largely delivered in these countries.
Where the government does not operate the blood system, and with very few exceptions, private
not-for-profit organizations, such as Red Cross and the Dutch supplier (Sanquin), operate the
blood systems.
Other major findings from the survey are as follows:
- Aside from compliance with European Union Blood Directive and country-specific
regulations for the manufacture of blood components and plasma derivatives, with which
all responders comply, the majority of EBA countries responding also have laws
regarding self-sufficiency in providing an adequate supply of blood components for
transfusion. With the exception of plasma for transfusion, all but one responding country
were self-sufficient for the major blood components, that is red blood cells and platelet
concentrates.
- In the majority of responding countries, the government specifies which and what type of
organizations can collect and process blood for transfusion, including regulating prices
and donor compensation. Most countries also restrict from which organizations hospitals
can acquire blood components needed for patients. The majority of these countries also
do not regulate blood components as “medicinal products.”
- The situation with plasma-derived medicinal products (PDMP) has been evolving. Unlike
for blood components for transfusion, the majority of countries have no laws pertaining
2
to self-sufficiency for patient needs for PDMP, and indeed are not self-sufficient. The
majority of countries do regulate the collection and processing of plasma as a starting
material for PDMP, although most do not have fractionation facilities for manufacturing
PDMP. Most governments do not regulate the prices of PDMP.
- In all situations, Sanquin is in the majority of responders or a sizable minority. Indeed,
Sanquin is only an outlier in two very specific situations: 1) it is the only non-Red Cross,
non-governmental, not-for profit sole supplier of blood components for transfusion, and
2) it is the only country to use its own plasma as the only source of solvent-detergent
treated plasma.
3
1. Introduction and Terms of Reference
In the Netherlands, the responsibility for an effective and adequate blood supply system
lies with the Minister of Health (MoH) and is regulated in the Blood Supply Act
(http://wetten.overheid.nl/BWBR0009079).
According to this act, the MoH appoints a single organization, called the Blood Supply
Organization (BSO), for the implementation of the Blood Supply Act. According to this act, the
specific tasks of the BSO include:
- To estimate yearly the medical need of whole blood, plasma, semi-finished blood
products, and blood products.
- To collect whole blood and source plasma1 in the Netherlands.
- To prepare (semi-finished) blood products from the collected person, whole blood and
source plasma, as well as storage, packing, labelling, transporting, and delivery of these
products.
The blood products can be divided in two categories: blood components for transfusion
and plasma derivatives.
Blood components: in the Netherlands, the Minister of Health has appointed Sanquin
Blood Supply Foundation as the BSO. Sanquin is, in accordance of the Blood Supply Act, the
sole organization responsible for the collection of whole blood and plasma in the Netherlands. In
the interest of an effective and adequate provision, hospitals in the Netherlands are obliged to
purchase blood components for transfusion from Sanquin and are prohibited to purchase blood
components from other parties or countries.
Plasma derivatives: in the Netherlands, plasma derivatives are produced by Sanquin
Plasma Products BV, a subsidiary company of Sanquin Blood Supply Foundation. In case of the
plasma derivatives, the Dutch Medicines Act (http://wetten.overheid.nl/BWBR0007867) is also
applicable for the quality, safety, and marketing authorization of these products. In contrast to
blood components, there are multiple providers for plasma derivatives in the Netherlands. Based
on the Blood Supply Act, Sanquin (and since April 2015, the subsidiary company of Sanquin,
Sanquin Plasma Products BV) must first offer the plasma derivatives, produced from Dutch
plasma, to the Dutch market. Only in case of surplus is Sanquin Plasma Products BV allowed to
offer its products to other countries.
Also based on the Blood Supply Act, Sanquin must annually submit its policy plan and
budget to the MoH for approval. This approval influences in an indirect way the price level of
the blood components for transfusion (exclusively delivered by Sanquin). For the production of
plasma derivatives Sanquin Plasma Products BV purchase whole blood plasma and source
plasma from Sanquin Blood Supply Foundation. In the interest of a level playing field, the MoH
1
Source plasma refers to plasma obtained by a plasmapheresis
4
determines the price of this plasma. The price is based on the price of plasma on the European
market.
Survey: The MoH developed a series of questions for a survey to understand the blood
supply systems in Western European countries. This includes how the blood supply is regulated
in other countries and how this differs from the situation in the Netherlands. Further, it is
relevant to understand the role and the position of the government in the blood supply system.
By means of a limited bidding procedure, the MoH awarded this contract to a supplier
(the two authors noted in Appendix G) with proven experience with the European blood systems
and in the area of marketing research.
The supplier, in turn, enlisted the assistance of the European Blood Alliance (EBA), an
association of not-for-profit BSOs, with 26 members plus an observer, throughout the European
Union and European Free Trade Association (EFTA) states, including the four countries within
the United Kingdom. Serbia is the observer for a total of 30 countries. EBA agreed to promote
participation in the survey with its members and observer.
5
2. The Survey
Survey design – who, what, how; collaboration with EBA
The original survey questions from the Ministry of Health (MoH) were refined and
clarified through a series of discussions between the suppliers, MoH, Sanquin, and staff of the
European Blood Alliance (EBA). EBA is an association of not-for-profit Blood Supply
Organizations, with 26 members, plus one observer, throughout the European Union and
European Free Trade Association (EFTA) states.
Once all parties were satisfied with the content, the questions were loaded on to the
SurveyGizmo (Bolder, CO) online platform using logic to determine whether subquestions
needed to be responded to based on the answer to a previous question.
The suppliers then tested the survey among three prospective recipients. All found the
survey easy to follow, although clarification was required for several questions. A full text copy
of the final electronic survey used is shown is Appendix A.
EBA staff then emailed the link to the survey to all its members and observer, including
the four countries within its UK member. EBA followed up three times with non-responders
before closing the survey at the end of August 2017. The suppliers used various tools provided
through SurveyGizmo to compile and analyse the results.
Blood Supply Organizations surveyed
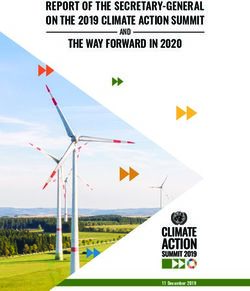
The attached map, which was open-sourced on the internet, shows the responding
countries. Unfortunately, we could find no open source map showing Malta. Their answers are
included in the survey analysis provided in Chapters 4, 5, and 6, as well as listed entirely in
Appendix D. Also, we could not separate on the map N Ireland, which did not respond to the
survey, from the other three UK countries (England, Scotland, and Wales), which did respond.
In all, the survey link was sent to the 30 countries within the EBA of which 22 responded
for a 73% response rate. SurveyGizmo calculated that the average time to complete the survey
was 22 minutes. In addition, and under Chapter 7, Conclusions, we note how two of the larger
non-responders (Austria and Spain) generally might have responded, that is, to which other
countries they are similar in structure.
6
RESPONSE TO SURVEY
ANSWERED THE SURVEY SURVEY NOT RETURNED
1. The Netherlands 12. Lithuania 23. Austria
2. Belgium 13. Malta 24. Croatia
3. Denmark 14. Portugal 25. Estonia
4. Finland 15. Romania 26. Hungary
5. France 16. Serbia 27. Luxembourg
6. Germany 17. Slovenia 28. Northern Ireland
7. Greece 18. Sweden 29. Norway
8. Iceland 19. Switzerland 30. Spain
9. Ireland 20. England
10. Italy 21. Scotland
11. Latvia 22. Wales
7
3. Structure of Report
This report is broken down into an executive summary, plus seven chapters and seven
appendices.
Most important are Chapters 4, 5, and 6, which summarize and analyse the results on a
strictly factual basis in accordance with the terms of reference and scope of the project, as
delineated by the MoH. The charts (mostly maps) vividly show the results, and any commentary
is based on factual findings by the suppliers.
Any interpretation of the findings or context of the issues covered in the survey is left to
Chapter 7, Conclusions.
In addition, Appendix B includes a brief description of the demographics, economy, and
healthcare and blood systems for the 22 responders, as well as for the two largest non-responders
(Austria and Spain).
8
SURVEY OF EUROPEAN BSOs
CHAPTER 4: THE BLOOD SUPPLY SYSTEM
Question 1. Does government have any legal responsibility for a self-sufficient, safe or
effective blood supply? (Self-sufficient means that the organisation(s) supplying the blood -
estion 1 Does the Government have legal responsibility for a self-sufficient,
hereafter called the blood service organisation(s) or BSO(s) - can independently meet the
saf
effective
medical need of blood components bloodinsupply?
for transfusion its country.)
YES NO
18 respondents, including the Netherlands, answered YES to this question. The 4 who
responded NO were Finland, France, Latvia, and Lithuania.
There were 15 responses to the supplementary request: If YES, please outline briefly
the government’s responsibilities (Include any references to related legislation, regulation,
a national blood policy, etc.). Respondents made reference to legislation bringing the EU Blood
Directives into national law; governmental responsibility for funding blood services; and
legislation specifically setting up a national organisation, reporting to the government, and
responsibility for the provision of the blood service.
9SURVEY OF EUROPEAN BSOs
QuestionQuestion
2 Does the national
2. Does nationallawlaw outline
outline specific specific responsibilities
responsibilities for the
to the BSO(s) (rather than BSO(s)?
those responsibilities otherwise delegated by a government agency)?
YES NO
21 respondents answered this question. 14, including the Netherlands, responded YES
and 7 responded NO. The NOs were Finland, Ireland, Latvia, Lithuania, Malta, Sweden, and
Switzerland. 3 respondents, Finland, Latvia, and Lithuania, answered NO to both questions 1 and
2.
There were 12 responses to the supplementary request, if YES, please outline briefly the
BSO(s)’s legal responsibilities (Include any references to related legislation, regulation, a
national blood policy, etc.). These largely consist of detailed requirements for blood collection,
testing, processing, storage, and distribution of blood, often with specific reference to the EU
blood directives.
10SURVEY OF EUROPEAN BSOs
Question 3 Is the collection of whole blood regulated by the government?
Question 3. Is the collection of whole blood regulated by the government?
YES NO
18 respondents, including the Netherlands, answered YES to this question and 4 (Finland,
Ireland, Sweden, and Wales) answered NO. Of the 4 NOs, only Wales answered YES to question
2. Finland answered NO to all of the first 3 questions.
11Question 4. How many BSOs are allowed to collect whole blood (including plasma for
transfusion) in the country?
1 (10 respondents) 2 – 5 (5 respondents) 6 or more (7 respondents)
Netherlands Belgium - 4 Germany - 15+
Finland Denmark - 5 Greece - 100
Iceland France - 2 Italy - 283
Ireland Lithuania - 3 Portugal - 31
Latvia Slovenia – 3 Romania - 41
Malta Serbia - 47
Switzerland Sweden - variable
England (see analysis next question)
Scotland
Wales
12Question 5. Which types of BSOs (that is, government agencies or companies) are allowed
to collect whole blood?
16 respondents answered that only government-owned BSOs were allowed to collect
whole blood. 4 respondents (the Netherlands, Belgium, Finland, and Switzerland) answered that
only a privately-owned not-for-profit BSO was allowed to collect whole blood. 2 respondents
(Germany and Sweden) answered that any type of BSO (government-owned, privately-owned
not-for-profit, privately-owned for-profit) was permitted to collect whole blood.
The 10 respondents who said that only 1 BSO was allowed to collect whole blood
included the 3 privately-owned not-for-profits (Netherlands, Finland, and Switzerland). The
other 7 were government-owned BSOs.
The 5 BSOs in Denmark are owned by the 5 Regions in mainland Denmark.
The 2 BSOs in France are both government-owned (Etablissement Français du Sang or
EFS and the Army Blood Centre).
13The BSOs in Germany include the regional Red Cross centres (collecting about 70% of
the whole blood supply); the community/university-owned centres (about 15%); and the
privately-owned for-profit centres (about 15%).
The 100 centres in Greece include 96 hospital blood centres and 4 blood establishments.
There are plans to rationalise the provision.
The two Red Cross BSOs in Belgium provide over 95% of the blood supply with
hospitals (mostly government and private not-for-profit) providing the rest.
The 283 BSOs in Italy are run by government-owned hospitals.
In Portugal, 3 IPST (Instituto Português do Sangue e de Transplantação) public blood
centres collect 60% of whole blood, and the remaining 40% is collected by public blood services
in hospitals.
In Serbia, there are 3 major blood transfusion institutes and 44 hospital blood banks.
In Sweden, there is no set number of BSOs as the county councils/regions decide how
they want BSOs to be organized. The candidate BSO must have a license by the competent
authorities by law and regulations.
14SURVEY OF EUROPEAN BSOs
on 6: Are whole blood donors allowed compensation more than their e
Question 6. Are whole blood donors allowed to receive more compensation than their
(paid
expenses (such as for travelling or donations‘)?
for consuming meals that are related to the donation)
made by the donor, that is, ‘paid donations’?
YES NO
2 respondents answered YES to this question: Germany and Latvia. They then responded
to question 7.
15Question 7. If there are ‘paid donations’, are there also unpaid whole blood donations?
Both Germany and Latvia replied YES to this question.
Question 8. Are there any political or social indications for changes to the present
arrangements for collecting whole blood?
Only Switzerland replied YES to this question.
In response to the supplementary question, if YES, what changes may occur?
Switzerland responded:
Better definition of the (Red Cross) mandate.
Better description of voluntary, non-remunerated blood donation (VNRBD) in the
law.
16CHAPTER 5: BLOOD COMPONENTS FOR TRANSFUSION
Question 9. Is blood for transfusion regarded as a Medicinal Product?
15 respondents, including the Netherlands, answered NO to this question. All these 15
answered YES to the supplementary question: if NO, is there a separate ‘blood law’ that
includes the requirements in the EU Directives?
17Question 10. Is plasma for transfusion regarded as a medicinal product? (Please note that
for this question and Q.18., "plasma for transfusion" only includes the following blood
components: Plasma, Fresh Frozen; Plasma, Fresh Frozen, Pathogen Reduced;
Cryoprecipitate; and Plasma, Fresh Frozen, Cryoprecipitate Depleted, as defined in
the European Pharmacopeia.)
The same 15 respondents, including the Netherlands, who answered NO to question 9,
answered NO to question 10. In both cases, the remaining 7 respondents answered YES.
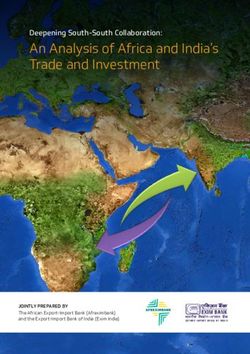
18Question 11. Are the blood components for transfusion processed in the country?
All 22 respondents answered YES to this question.
19We then asked: if YES, which types of BSOs are processing these blood components?
Gov: government
PFP: private for-profit
PNFP: private not-for-profit
N/A: not answered
The Netherlands was 1 of 3 respondents to report privately-owned not-for-profit BSO(s)
as the sole source of supply. The other 2 are Finland and Switzerland. Germany reported that part
of their supply came from privately-owned for-profit organizations. Sweden’s blood supply is
hospital-based, both government and private for-profit.
20Question 12. Are blood components processed outside the country?
2 respondents – the Netherlands and Portugal - reported that some blood components
were processed outside the country and returned for use, in both cases, plasma for transfusion.
21Question 13. Is the country self-sufficient for its blood components for transfusion?
2 respondents reported that they were not self-sufficient for blood components for
transfusion, Greece and Ireland. Greece reported that they obtain supplies from the Swiss Red
Cross; Ireland reported that they source plasma from Austria because of variant Creutzfeldt-
Jacob Disease (vCJD) risk.
22Question 14. Are there any specific legal obligations for the delivery or processing of blood
components for transfusion?
19 respondents, including the Netherlands, answered YES to this question. Three
countries, Finland, Lithuania, and Serbia, answered NO.
23Question 15. Are hospitals allowed to purchase blood component for transfusion from
other parties or (European) countries?
5 respondents, France, Germany, Malta, Switzerland, and Wales answered YES to this
question. (Note: Malta does not appear on this map; Wales cannot be shown separately from the
rest of the UK.)
24We then asked 2 supplementary questions, if YES, from whom? And, if ‘YES’, are there any
conditions and rules that must be met?
France reported that some plasma for transfusion is bought from Octapharma; Germany
and Malta reported that theoretically hospitals could purchase from any suppliers who complied
with national laws and regulations; Switzerland reported that hospitals could purchase from any
supplier using voluntary non-remunerated donors, but in practice none did; and Wales reported
that hospitals could purchase from other parties, but, as the Welsh National Blood service is an
integral part of the Welsh National Health Service, none do.
Question 16. Are there any political or social indications for changes?
Only Greece responded YES to this question. In response to the supplementary question,
if YES, what changes may occur? Greece reported:
We are further centralizing collection, testing, processing, and distribution into 4 BE
(Blood Establishments). The Hellenic National Blood Transfusion Centre plans to
undertake the responsibility of blood collection from the Hospital Transfusion Services.
This project is expected to ensure better functioning of the whole system and blood
sufficiency. (Greece has a very high index of donations per 1,000 inhabitants.) This will
give us the opportunity to stop red blood cell imports.
25CHAPTER 6: PLASMA COLLECTION FOR PLASMA-DERIVED MEDICINAL
PRODUCTS (PDMPs)
Note: Romania did not answer any of the questions in this section of the survey. They are
shown as ‘N/A’ (Not Answered) and coloured light green on all the maps. Other respondents
also omitted some questions in this part of the survey and are also marked ‘N/A’ (light green),
where appropriate. With the exception of question 25, which required responses only from the 2
respondents who answered YES to question 24, and question 29a, which required response only
from the 15 respondents who answered NO to question 29, all the questions were answered by at
least 17 of our 22 respondents. Most were answered by 19 or more.
This chapter covers both plasma collected by plasmapheresis, also known as ‘Source
Plasma’, and plasma derived from whole blood collections, also known as ‘Recovered Plasma’.
‘Plasma derivatives’ are also known as ‘plasma protein products’ or ‘plasma-derived medicinal
products’ or PDMPs, and include products such as clotting factor and albumin concentrates, as
well as intravenous immune globulin or IVIG and other immune globulins.
The chapter falls into 2 parts. The first part, comprising questions 17 - 26 inclusive, deals
with the legal framework and arrangements for the collection of plasma for the manufacture of
PDMPs. The second, comprising questions 27 - 34 inclusive, deals with the legal framework for
the actual PDMPs and the manufacturing and distribution arrangements.
26Question 17. Government Responsibilities: Does government have any legal responsibility
for a self-sufficient*, safe or effective supply of plasma for plasma derivatives/PDMP?
(*Self-sufficient means that the BSO or BSOs can independently meet the medical need for
plasma derivatives in their country.)
6 respondents (Ireland, Belgium, Germany, Slovenia, Italy, and Portugal) answered YES
to this question and 15, including the Netherlands, answered NO.
All of the respondents who answered YES, except Italy, replied to our supplementary
request, if YES, please outline briefly their government’s responsibilities (include any
references to related legislation, regulation, a national policy for plasma derivatives, etc.). The
responses referenced national laws translating relevant EU Directives into national law and, in
the case of the Portuguese, the national Strategic Programme for Plasma Fractionation 2015-
2019.
27Question 18. Does national law give specific responsibilities to the BSO (rather than
responsibilities delegated by the government)?
6 respondents, including the Netherlands, answered YES to this question and 14
answered NO. Other countries who answered with YES are: Belgium, Germany, France,
Slovenia, and Italy. Denmark and Romania did not answer the question.
28Question 19. Is the collection of plasma for the manufacture of plasma derivatives
regulated by the government?
13 respondents, including the Netherlands, answered YES to this question and 6
answered NO. The countries which answered NO are Iceland, Ireland, Finland, Latvia,
Lithuania, and Malta. Denmark, Romania, and Wales in the UK did not answer this question.
10 of the respondents who answered YES to this question replied to our supplementary
request, if YES, please outline briefly what is regulated by the government. Respondents
from the UK noted that plasma for fractionation is not collected there because of the vCJD risk,
and that the regulator (Medicines & Healthcare Products Regulatory Agency or MHRA) has to
be assured of the quality of plasma imported for fractionation. Other respondents noted that the
requirements for plasma were similar to those for other blood components. The response from
the Netherlands noted that the government regulates the amount of plasma that can be collected.
29Question 20. Are organizations allowed to collect plasma in your country for the
manufacture of plasma derivatives?
9 respondents answered YES to this question and 12, including the Netherlands,
answered NO. The 9 countries that responded YES are Iceland, Sweden, Denmark, Germany,
Switzerland, Italy, Latvia, Lithuania, and Malta.
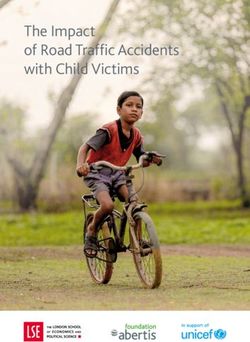
30Question 21. Does the government determine the price for selling of plasma for
manufacture of plasma derivatives?
5 respondents, including the Netherlands, answered YES to this question and 14
answered NO. The other 4 countries that responded YES are Sweden, Denmark, France, and
Slovenia. Portugal, Romania, and Scotland did not answer this question.
31Question 22. Which types of organizations are allowed to collect plasma for the
manufacture of plasma derivatives?
Gov: government
PNFP: private and not-for-profit
PFP: private and for-profit
N/A: not answered
10 respondents answered that only government-owned BSOs were allowed to collect
plasma for the manufacture of PDMPs. Two respondents (Sweden and Switzerland) reported that
government-owned and privately-owned, both not-for-profit and for-profit organisations were
allowed to collect plasma for the manufacture of PDMPs. The Netherlands responded that only
the privately-owned not-for-profit BSO was allowed to collect plasma for the manufacture of
PDMPs. Germany responded that both privately-owned not-for-profit and privately-owned for-
profit organisations were allowed to collect plasma for the manufacture of PDMPs. Belgium,
Finland, France, Malta, Romania, and the 3 respondents in the UK (where collection of plasma
for manufacture of PDMPs is not permitted) did not answer this question.
32Question 23. Does your country have priority for the use of plasma derivatives
manufactured from plasma collected in your country?
7 respondents answered YES to this question and 12, including the Netherlands,
answered NO. The 7 countries that answered YES are Denmark, France, Italy, France, Slovenia,
Serbia, and Latvia. Romania, and England and Scotland from the UK (where collection of
plasma for manufacture of PDMPs is not permitted) did not answer this question.
33Question 24. Are plasma donors allowed to receive more compensation than their expenses
(such as for travelling or for consuming meals that are related to the donation) made by the
donor - ‘paid donations’?
2 respondents, Germany and Latvia, answered YES to this question. 17, including the
Netherlands, answered NO. Romania, and England and Scotland from the UK (where collection
of plasma for manufacture of PDMPs is not permitted) did not answer this question.
In response to our supplementary question, if YES, is this compensation regulated by
the government? Germany responded YES and Latvia did not answer. In response to our
34further supplementary, if YES, what aspects are regulated? Germany answered, “Not more
than €25 per donation as a lump sum for time and travel expenses”.
Question 25. If there are ‘paid donations’ of plasma for the manufacture of plasma
derivatives, are there also unpaid donations of plasma for the manufacture of plasma
derivatives?
Both Germany and Latvia answered YES to this question. In response to our
supplementary question, if YES, which organizations are taking care of these collections?
Germany answered the Red Cross (less than 5% of the total plasma collected); and Latvia, the
State Blood Donor Centre.
Question 26. Are there any political or social indications for changes to the present
arrangements for collecting plasma for the manufacture of plasma derivatives?
Belgium answered YES to this question, reporting that the Belgian government was
tendering for plasma. 20 respondents, including the Netherlands, answered NO. Romania did not
answer this question.
35THE FINAL QUESTIONS CONCERN PLASMA DERIVATIVES, THAT IS PDMPs,
SUCH AS IVIG, ALBUMIN, AND CLOTTING FACTOR CONCENTRATES.
Question 27. Are plasma derivatives regarded as Medicinal Products?
All 21 respondents to this question, including the Netherlands, answered YES.
Question 28. Is there a plasma derivative manufacturing facility in the country?
9 respondents, including the Netherlands, replied YES to this question and 12 NO. The
map below combines these answers with our supplementary question, if ‘YES’, which type of
organisations are manufacturing plasma derivatives?
Gov: government
PFP: private and for-profit
N/A: not answered
5 respondents (Belgium, Germany, Sweden, Switzerland, and England) answered
privately-owned for-profit organisations; Serbia replied a government-owned organisation;
France replied government-owned and privately-owned for-profit organisations; and Netherlands
replied a privately-owned not-for-profit organisation. Italy did not respond to this supplementary
question; however, the fractionator, Kedrion, is private and for-profit.
36Question 29. Is your country self-sufficient in collecting plasma for the manufacturing and
supply of plasma derivatives?
4 respondents, including the Netherlands, responded YES to this question. 15 replied NO.
Denmark, Romania, and Wales did not reply.
37Question 29a. If ‘NO’, does your country obtain plasma for the manufacturing and supply
of plasma derivatives from other countries to obtain the balance of its supply?
13 of the 15 respondents who answered NO to question 29 answered our supplementary
question. Italy and Portugal did not. The other N/As shown on the map either answered YES to
question 29 or did not answer it.
Of the 13 respondents, 6 said YES. 7 (including Malta, and Scotland in the UK) said NO.
The 6 countries that answered YES were Belgium, England, Greece, Lithuania, Sweden, and
Switzerland.
38Question 30. Is the country self-sufficient for the manufacturing and supply of plasma
derivatives?
4 respondents, including the Netherlands, answered YES to this question. The other 3
countries that answered YES are Ireland, France, and Latvia. 14 answered NO. 4 (Italy,
Romania, and England and Wales in the UK) did not answer the question.
13 of the NOs answered the supplementary question, if NO, from where does the
country obtain the balance of its supply? Answers indicated that the sources were international
pharmaceutical companies who supply the finished products. Belgium was the NO that did not
answer this supplementary question.
39Question 31. Who distributes plasma derivatives to hospitals, clinics, or pharmacies?
21 respondents answered this question. Respondents were offered 3 alternatives: regional
or national BSOs; manufacturers; and other types of organisation (these were mainly
pharmacies).
Two countries (the Netherlands and Finland), replied that the BSO and manufacturers
were the distributors. One country (Slovenia) said the BSO and another type of organisation; 3
(Latvia, and Scotland and Wales in the UK) said only the BSO; 6 (including England in the UK)
said only the manufacturers; 2 (France and Germany) said the manufacturers and another type of
organisation; and 7 only other types of organisations.
40Question 32. Are there any specific legal obligations for the delivery or production of
plasma derivatives?
11 respondents, including the Netherlands, answered YES to this question. 8 answered
NO. The 8 countries that answered NO are Finland, Germany, Iceland, Ireland, Latvia,
Lithuania, Malta, and Serbia. 3 (Denmark, Romania, and Wales in the UK) did not answer this
question.
8 of those who responded YES answered our supplementary question, if YES, what are
these obligations and who is involved in them? Answers included relevant legislation,
including traceability requirements, and Good Manufacturing Practice (GMP). Belgium, Italy,
and Switzerland did not answer the supplementary question.
41Question 33. Does the government make a requirement for emergency supplies of plasma
derivatives?
5 respondents (Belgium, Greece, Slovenia, and Scotland and Wales in the UK) answered
YES to this question. 12 respondents, including the Netherlands (and England in the UK),
answered NO. Germany, Portugal, Romania, Sweden, and Switzerland did not answer this
question.
3 of those who responded YES (Greece, Scotland and Slovenia) answered our
supplementary question, if ‘YES’, which plasma derivatives are involved and in what
quantities? Greece and Slovenia said IVIG; Scotland said all PDMPs. In all 3 countries, the
Ministry of Health was involved in funding the emergency supply and the BSO was involved in
its storage and distribution.
42Q.34. Are there any political or social indications for changes?
18 respondents, including the Netherlands, replied NO to this question. 4 respondents
(Greece, Portugal, Romania and Sweden) did not answer this question.
437. Conclusions
Responders and Non-Responders
All the members and observer of EBA, a total of 30 countries (including the 4 countries
that make up the single EU Member State, the United Kingdom) were invited to respond to the
survey. A total of 22 European countries responded for a response rate of 73%. This included 20
countries that are members of the European Union (including three countries - England, Scotland
and Wales - within the United Kingdom). The two responding countries not members of the EU,
Iceland (a member of the European Free Trade Association and European Single Market) and
Switzerland (a member of the European Single Market), follow the EU Directives (regulations),
including for blood and plasma products. The 30 countries surveyed have an estimated 2018
population of 470 million. The 22 responding countries have an estimated population of 392
million, or 83% of those surveyed.
Seventeen of the responding countries are considered traditionally part of Western
Europe, while five (Latvia, Lithuania, Romania, Serbia, and Slovenia) were part of what was
once considered Eastern Europe.
Eight of those invited did not respond to the survey: Austria, Croatia, Estonia, Hungary,
Luxembourg, Northern Ireland, Norway, and Spain. Of note are the two larger EU countries
(Austria and Spain), which did not respond to the survey despite several attempts by EBA.
Information about how these two countries blood systems are organized are contain in Appendix
B.
Overall, the results of the survey are largely self-explanatory and met the expectations of
the researchers. The majority of European blood systems are operated by the government, either
locally or nationally. This reflects the way healthcare is also largely delivered in these countries.
Increasingly since the 1980s, blood processing and testing has been consolidated into larger
blood centres and/or hospitals. This consolidation has occurred more slowly in countries where
there is greater regional autonomy in healthcare, such as in Spain, Italy, Switzerland, and the
Nordic countries (Denmark, Iceland, Norway, and Sweden).
Recent Dynamic Changes
Of note, despite the free movement of goods and services between and among both EU
and Council of Europe countries, blood collected for transfusion within a country nearly always
stays within a country. This is partly because, even without a government mandate, most
countries are self-sufficient for blood components. Indeed, only Greece imports non-plasma
components.
Hospitals in most of the countries responding to the survey are not allowed to obtain
blood components processed in other countries. Even where it is allowed (France, Germany,
44Switzerland, and Austria), the practice is rare. Because of the large variation in pricing blood
components from country to country, it was thought that the sameness in quality due to EU
regulations coupled with pressure on hospitals to reduce costs, could open the markets for blood
components between EU countries. However, since the great recession of 2008, emphasis within
hospitals has been to use less blood under the belief that blood was overused. There is also the
issue of volunteer donors (VNRD) wishing to assure local needs are met first and foremost.
While studies from the US show donors are willing to support patients in need anywhere,
assuring local supply is a major motivation for repeat donors.
The situation regarding plasma derivatives (PDMP) has evolved much faster than any
changes in blood components for transfusion. This is reflected in the mixed responses to the
survey and reflects multiple factors. The HIV transmission tragedy in the 1980s among people
with haemophilia forced many countries with national plasma fractionation facilities to rethink
their model. The vCJD crisis in the UK, Ireland, and Portugal changed the world view of using
European plasma, and the dynamics of using plasma for transfusion.
In addition, the change to recombinant anti-haemophilic factor in high-income countries,
and major swings in plasma supply and PDMP demand since the late 1990s, has resulted in
government-owned PDMP plants to privatize, close or otherwise disassociate from the national
blood system in Belgium, England, Finland, France, Germany, Scotland, Switzerland, and
others.
HIV and other infectious diseases changed how plasma for transfusion has been used.
Many countries have seen huge declines in use, whereas even where used, there has been a
switch to products perceived to be safer, such as methylene blue-treated and solvent detergent-
treated (SD) plasma. The latter product is provided primarily by Octapharma and to a lesser
extent by Kedrion. SD plasma is the only plasma product provided in Austria, Finland, and the
Netherlands and has largely replaced use of plasma for transfusion in other European countries.
How the Netherlands/Sanquin Fit In
The survey results show that Sanquin and the Dutch government are largely in concert
with their EU counterparts when it comes to blood regulation and supply of blood components
for transfusion. For nearly every question, Sanquin’s response is either in the majority of fellow
EU blood services or in a sizable minority.
Sanquin is an outlier in that it uses only Dutch plasma for its SD plasma supply. It is also
in a small minority of being a private not-for-profit blood supplier, along with the Red Cross
societies in Belgium, Finland, Germany, and Switzerland.
Sanquin owns the last or one of the last remaining not-for-profit (non-governmental)
PDMP manufacturing facility in Europe, although under a planned reorganization, the plant
would become a for-profit subsidiary of a Sanquin holding company. (Less than 25 years ago,
45PDMP production in Europe was largely by national not-for-profit or government-owned
facilities. Today, the field is dominated by for-profit entities.) The Netherlands is one of the few
European countries mostly self-sufficient for PDMP, a situation that has benefits for assuring
product availability, and whereby finances largely stay within the country.
As a national blood supplier, Sanquin is most similar to the blood programmes of the UK
and France, and to a somewhat lesser extent to Italy, Germany, and Finland. Dutch regulation is
also similar to that of most of the larger EU countries with regard to blood components and
PDMP.
46Appendix A
Survey of Western European Blood and Plasma Services
Dear Blood Service Operator
Sanquin, the national blood supplier to the Netherlands, is undergoing a structural reorganization.
Because the reorganization requires amendment to Dutch national legislation, the Ministry of Health,
Welfare and Sports (MHWS) approached Sanquin about gathering information on how the blood systems
are organized and regulated in other Western European countries. Sanquin and the MHWS agreed that
such a survey should be conducted by an outside entity.
Based on similar efforts and expertise, I was awarded the contract by the MHWS. Many of you knew me
as the CEO of America's Blood Centers for nearly 29 years, and as an observer to the board of the
European Blood Alliance (EBA) for 12 years. Your colleague, Martin Gorham, former CEO of NHS
Blood and Transplant and former President of EBA, graciously agreed to assist me in conducting and
analysing the survey data, and providing the final report to the MHWS. A copy of that final report will
also be provided to all responders of the survey.
In addition, both Sanquin and the EBA endorse this survey and encourage your participation.
Please note that the final report will identify responses only by country. The names of those providing
information through this survey will NOT be included in the report and will be kept confidential by
Martin and me.
The survey, of course, is in English. While most of the questions should be easy to answer, you may be
unclear how to answer a question as you try to complete it. There are two ways to get clarifications. First,
you can call or email me (+1 202 468 6548; jmacpherson1948@gmail.com) or Martin (+44 7711 447
265; martin.gorham@yahoo.co.uk). Or, you can just leave the question blank. In many cases, we will be
contacting you for a brief follow up phone interview to be sure we understand the information you
provided.
While some of the questions may not apply to your organization (such as those regarding plasma
derivatives or PDMP), we are asking you to complete the survey as it applies to your country. Again,
when in doubt, you can leave the question blank and we will follow up with you.
In addition, if you have concerns about the proprietary or competitive nature of any of the responses, just
provide rough estimates of the information, as publicly may be known, or just leave the question blank.
Please respond by 31 July 2017.
Thank you so much for your help with this. We know your time is valuable and hope the final report will
be useful to you.
Jim MacPherson
1) This first set of questions concerns Government Responsibilities
Q.1. Does government have any legal responsibility for a self-sufficient, safe or effective blood supply?
47(Self-sufficient means that the organisation(s) supplying the blood - hereafter called the blood service
organisation(s) or BSO(s) - can independently meet the medical need of blood components for transfusion
in its country.)
( ) Yes
( ) No
2) If ‘YES’, please outline briefly the government’s responsibilities (Include any references to related
legislation, regulation, a national blood policy, etc.).
____________________________________________
3) Q2. Does national law outline specific responsibilities to the BSO(s) (rather than those responsibilities
otherwise delegated by a government agency)?
( ) Yes
( ) No
4) If ‘YES’, please outline briefly the BSO(s)’s legal responsibilities (Include any references to related
legislation, regulation, a national blood policy, etc.).
____________________________________________
5) Q.3. Is the collection of whole blood regulated by the government?
( ) Yes
( ) No
6) Q.4. How many BSOs are allowed to collect whole blood (including plasma for transfusion) in the
country?
____________________________________________
7) Q.5. Which types of BSOs (that is, government agencies or companies) are allowed to collect whole
blood:
[ ] Government owned?
[ ] Privately owned, not-for-profit?
[ ] Privately owned, for-profit?
8) If there is more than one BSO collecting whole blood in the country, please specify roughly what
percentage of the blood supply each BSO type collects. (For example, government owned = 50%;
privately owned, not-for-profit = 30%; privately owned, for-profit = 20%.)
____________________________________________
9) Q.6. Are whole blood donors allowed to receive more compensation than their expenses (such as for
travelling or for consuming meals that are related to the donation) made by the donor, that is, ‘paid
donations’?
( ) Yes
( ) No
4810) If ‘YES’, is this compensation regulated by the government?
( ) Yes
( ) No
11) If ‘YES’, what aspects are regulated?
____________________________________________
12) Q.7. If there are ‘paid donations’, are there also unpaid whole blood donations?
( ) Yes
( ) No
13) If ‘YES’, which BSOs are taking care of these collections?
____________________________________________
14) Q.8. Are there any political or social indications for changes to the present arrangements for
collecting whole blood?
( ) Yes
( ) No
15) If ‘YES’, what changes may occur?
____________________________________________
16) This next set of questions concerns Blood Components for Transfusion
Q.9. Is blood for transfusion regarded as a Medicinal Product?
( ) Yes
( ) No
17) If ‘NO’, is there a separate ‘blood law’ that includes the requirements in the EU Directives?
( ) Yes
( ) No
18) Q.10. Is plasma for transfusion regarded as a medicinal product? (Please note that for this question
and Q.18., "plasma for transfusion" only includes the following blood components: Plasma, Fresh
Frozen; Plasma, Fresh Frozen, Pathogen Reduced; Cryoprecipitate; and Plasma, Fresh Frozen,
Cryoprecipitate Depleted, as defined in the European Pharmacopea.)
( ) Yes
( ) No
19) Q.11. Are the blood components for transfusion processed in the country?
( ) Yes
( ) No
20) If ‘YES’, which types of BSOs are processing these blood components:
49[ ] (i) Government owned?
[ ] (ii) Privately owned, not-for-profit?
[ ] (iii) Privately owned, for-profit?
21) If there is more than one BSO processing blood components for transfusion in the country, please
specify roughly what percentage of the component supply each agency/ company provides. (Processing
includes manufacture, testing, storage and distribution.)
____________________________________________
22) Q.12. Are blood components processed outside the country (check if "Yes"):
[ ] Red Cells
[ ] Plasma for transfusion
23) Q.13. Is the country self-sufficient for its blood components for transfusion?
( ) Yes
( ) No
24) If ‘NO’, from where does the country obtain the balance of its supply (please give the name of the
agency/company; whether it is government owned; privately owned, not-for-profit; or privately owned,
for-profit; and the country in which it is based).
____________________________________________
25) Q.14. Are there any specific legal obligations for the delivery or processing of blood components for
transfusion?
( ) Yes
( ) No
26) If ‘YES’, what are these obligations and who is involved in them?
____________________________________________
27) Q.15. Are hospitals allowed to purchase blood component for transfusion from other parties or
(European) countries?
( ) Yes
( ) No
28) If ‘YES’, from whom?
____________________________________________
29) If ‘YES’, are there any conditions and rules that must be met?
( ) Yes
( ) No
30) If ‘YES’, please specify:
____________________________________________
5031) Q.16. Are there any political or social indications for changes?
( ) Yes
( ) No
32) If ‘YES’, what changes may occur?
____________________________________________
33) The next set of questions concern Plasma Collection for the Manufacture of Plasma Derivatives
(Note: This includes both plasma collected by apheresis, also known as “Source Plasma”, and plasma
derived from whole blood collections, also known as “Recovered Plasma.” In addition, the “plasma
derivatives” are also known as “plasma protein products” or "plasma-derived medicinal products" or
PDMP, and include products such as clotting factor and albumin concentrates, as well as intravenous
immune globulin or IVIG and other immune globulins.)
Q.17. Government Responsibilities
Does government have any legal responsibility for a self-sufficient*, safe or effective supply of plasma
for plasma derivatives/PDMP?
(*Self-sufficient means that the BSO(s) can independently meet the medical need for plasma derivatives
in its country.)
( ) Yes
( ) No
34) If ‘YES’, please outline briefly the government’s responsibilities (include any references to related
legislation, regulation, a national policy for plasma derivatives, etc.).
____________________________________________
35) Q.18. Does national law give specific responsibilities to the BSO (rather than responsibilities
delegated by the government)?
( ) Yes
( ) No
36) If ‘YES’, please outline briefly the BSO(s)’s legal responsibilities (include any references to related
legislation, regulation, a national policy for plasma derivatives, etc.).
____________________________________________
37) Q.19. Is the collection of plasma for the manufacture of plasma derivatives regulated by the
government?
( ) Yes
( ) No
38) If ‘YES’, please outline briefly what is regulated by the government.
____________________________________________
5139) Q.20. Are organizations allowed to collect plasma in your country for the manufacture of plasma
derivatives?
( ) Yes
( ) No
40) If ‘YES’, how many organizations collect plasma for the manufacture of plasma derivatives?
_________________________________________________
41) Q.21. Does the government determine the price for selling of plasma for manufacture of plasma
derivatives?
( ) Yes
( ) No
42) Q.22. Which type of organisations are allowed to collect plasma for the manufacture of plasma
derivatives (check, as applies):
[ ] Government owned
[ ] Privately owned, not-for-profit?
[ ] Privately owned, for-profit?
43) If there is more than one type of organization collecting plasma for the manufacture of plasma
derivatives in the country, please specify roughly what percentage of the plasma supply from your
country each organization collects. (For example, government owned = 50%; privately owned, not-for-
profit = 30%; privately owned, for-profit = 20%.)
____________________________________________
44) Q.23. Does your country have priority for the use of plasma derivatives manufactured from plasma
collected in your country?
( ) Yes
( ) No
45) Q.24. Are plasma donors allowed to receive more compensation than their expenses (such as for
travelling or for consuming meals that are related to the donation) made by the donor - ‘paid donations’?
( ) Yes
( ) No
46) If ‘YES’, is this compensation regulated by the government?
( ) Yes
( ) No
47) If ‘YES’, what aspects are regulated (please specify)?
____________________________________________
48) Q.25. If there are ‘paid donations’ of plasma for the manufacture of plasma derivatives, are there also
unpaid donations of plasma for the manufacture of plasma derivatives?
52( ) Yes
( ) No
49) If ‘YES’, which organizations are taking care of these collections?
____________________________________________
50) Q.26. Are there any political or social indications for changes to the present arrangements for
collecting plasma for the manufacture of plasma derivatives?
( ) Yes
( ) No
51) If ‘YES’, what changes may occur?
____________________________________________
52) The final questions concern Plasma Derivatives, that is PDMP, such as IVIG, albumin, clotting factor
concentrates.
Q.27. Are plasma derivatives regarded as Medicinal Products?
( ) Yes
( ) No
53) If ‘NO’, are plasma derivatives covered by a ‘blood law’ that includes the requirements in the EU
Directives?
( ) Yes
( ) No
54) Q.28. Is there a plasma derivative manufacturing facility in the country?
( ) Yes
( ) No
55) If ‘YES’, which type of organisations are manufacturing plasma derivatives (check as applies):
[ ] Government owned?
[ ] Privately owned, not-for-profit?
[ ] Privately owned, for-profit?
56) If there is more than one manufacturer of plasma derivatives in the country, please specify roughly
what percentage of the plasma derivative supply each type of manufacturer provides. (For example,
government owned = 50%; privately owned, not-for-profit = 30%; privately owned, for-profit = 20%.)
Also, please specify for type of manufacturer whether they use recovered plasma or source plasma or
both.
___________________________________________
57) Q.29. Is your country self-sufficient in collecting plasma for the manufacturing and supply of plasma
derivatives?
53( ) Yes
( ) No
58) If ‘NO’, does your country obtain plasma for the manufacturing and supply of plasma derivatives
from other countries to obtain the balance of its supply?
( ) Yes
( ) No
59) Q.30. Is the country self-sufficient for the manufacturing and supply of plasma derivatives?
( ) Yes
( ) No
60) If ‘NO’, from where does the country obtain the balance of its supply?
____________________________________________
61) Q.31. Who distributes plasma derivatives to hospitals, clinics or pharmacies (check as applies):
[ ] The national or regional blood service?
[ ] The manufacturer (if this is not the blood service)?
[ ] Some other organisation?
62) If some other organisation(s), please specify which ones.
____________________________________________
63) Q.32. Are there any specific legal obligations for the delivery or production of plasma derivatives?
( ) Yes
( ) No
64) If ‘YES’, what are these obligations and who is involved in them?
____________________________________________
65) Q.33. Does the government make a requirement for emergency supplies of plasma derivatives?
( ) Yes
( ) No
66) If ‘YES’, which plasma derivatives are involved and in what quantities?
____________________________________________
67) How and by whom is the continued existence of emergency supplies funded?
____________________________________________
68) If ‘YES’, by whom is it held?
____________________________________________
69) Q.34. Are there any political or social indications for changes?
54You can also read