Malaria Control and Elimination in the Western Pacific (2016-2020) - REGIONAL ACTION FRAMEWORK for
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

REGIONAL ACTION FRAMEWORK for Malaria Control and Elimination in the Western Pacific (2016–2020)


Regional Action Framework for Malaria Control and Elimination in the Western Pacific (2016–2020)

© World Health Organization 2017 ISBN 978 92 9061 815 7 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/amc/en/mediation/rules). Suggested citation. Regional action framework for malaria control and elimination in the Western Pacific: 2016- 2020. Manila, Philippines. World Health Organization Regional Office for the Western Pacific; 2017. Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. 1. Delivery of healthcare. 2. Health services. 3. Malaria – prevention and control. 4. Regional health planning. I. World Health Organization Regional Office for the Western Pacific. (NLM Classification: WC765). Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing. For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressed to Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, Fax. No. (632) 521-1036, email: wpropuballstaff@who.int Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third- party-owned component in the work rests solely with the user. General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use. For inquiries and request for WHO Western Pacific Regional Publications, please contact the Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, Fax. No. (632) 521-1036, email: wpropuballstaff@who.int

CONTENTS
Abbreviations.................................................................................................................................................. iv
Foreword............................................................................................................................................................. v
Regional Action Framework at a glance....................................................................................... vi
Executive summary.....................................................................................................................................ix
1. Background.............................................................................................................................................1
1.1 Malaria in the Western Pacific Region...........................................................................1
1.2 Challenges to malaria control and elimination in the Region..........................3
1.3 Development of the Regional Action Framework....................................................6
2. The Regional Action Framework...............................................................................................8
2.1 Vision and goals..........................................................................................................................8
2.2 Alignment with the Global Technical Strategy...........................................................8
2.3 Supporting elements............................................................................................................. 12
2.4 Priority actions.......................................................................................................................... 13
3. Strategic approaches to achieving objectives for each pillar.............................. 15
Pillar 1: Ensure universal access to malaria prevention, diagnosis
and treatment...................................................................................................................................... 15
Pillar 2: Accelerate efforts towards elimination and attainment
of malaria-free status..................................................................................................................... 20
Pillar 3: Transform malaria surveillance into a key intervention.......................... 24
4. Supporting elements .................................................................................................................... 28
Supporting element 1: Strengthening the underlying health system
and the enabling environment................................................................................................... 28
Supporting element 2: Expanding four themes of research in support
of improved service delivery and innovation...................................................................... 35
5. Measuring progress and impact............................................................................................. 38
5.1 Milestones and targets......................................................................................................... 38
5.2 Monitoring and evaluation.................................................................................................. 40
5.3 M&E framework....................................................................................................................... 42
5.4 Role of WHO in monitoring the Regional Action Framework......................... 42
6. Governance and coordination................................................................................................... 43
6.1 Regional leadership and technical support.............................................................. 43
6.2 National leadership, ownership and management............................................. 44
References...................................................................................................................................................... 46
Annex. Proposed progress indicators for the Regional Action Framework.................. 47
REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
ABBREVIATIONS
ABER annual blood examination rate
ACD active case detection
ACT artemisinin-based combination therapy
API annual parasite incidence
APLMA Asia Pacific Leaders Malaria Alliance
G6PD glucose-6-phosphate dehydrogenase
GMS Greater Mekong Subregion
GTS WHO Global Technical Strategy for Malaria 2016–2030
IEC information, education, communication
IRS indoor residual spraying
ITN insecticide-treated bed net
LLIN long-lasting insecticidal net
LSM larval source management
M&E monitoring and evaluation
MMPs mobile/migrant populations
MDA mass drug administration
MVP Malaria, other Vector-Borne and Parasitic Diseases (WHO unit)
NGO nongovernmental organization
NMCP National Malaria Control Programme
PCD passive case detection
PSM procurement and supply management
PQ primaquine
QA quality assurance
RDT rapid diagnostic test
TES therapeutic efficacy study (of antimalarial medicine)
TPR test positivity rate
UHC universal health coverage
WHO World Health Organization
WHOPES WHO Pesticide Evaluation Scheme
iv
FOREWORD
In the Western Pacific Region, malaria control efforts have been an evolving success
story. From 2009 to 2015, reported malaria deaths in the Region decreased by 85%, and
overall cases reduced by 48%. Nine out of 10 of the malaria-endemic countries in the
Region achieved the malaria targets of the Millennium Development Goals.
Building on these successes in alignment with the Sustainable Development Goals, the
regional action framework lays a foundation for accelerating progress towards malaria
elimination in the Region by 2030 – an ambitious goal endorsed by leaders across the
Region.
Despite our progress, however, malaria burden remains unacceptably high among margin-
alized population groups in many of the endemic countries of the Region. More than
70% of malaria deaths in the Region are attributable to P. falciparum. This is particularly
worrisome because of the presence of multidrug resistance in P. falciparum, especially in
remote and hard-to-reach areas of Cambodia, the Lao People’s Democratic Republic and
Viet Nam. The presence of multidrug-resistant strains of this type of malaria in areas
of the Greater Mekong Subregion reinforces the need to accelerate progress towards
elimination. Unfortunately, P. falciparum malaria is not the only challenge we face.
P. vivax and P. knowlesi strains also pose unique challenges that must be addressed by
all countries in the Region.
We can overcome these challenges and improve on the progress towards elimination.
This framework can help make that happen by helping countries build on successes and
lay the groundwork for accelerated elimination. The framework provides countries with
guidelines they need to strengthen surveillance systems and ensure access to proper
and appropriate drug treatment options. This step will further reduce mortality and
morbidity from malaria.
With the Regional Action Framework for Malaria Control and Elimination in the Westem
Pacific (2016–2020), we hope to fulfil the hopes of all those affected by malaria across
the Region for a healthier, happier and more prosperous future, free from the threat
of this deadly disease.
Shin Young-soo, MD, Ph.D.
Regional Director
vREGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
REGIONAL ACTION FRAMEWORK AT A GLANCE
OVERALL VISION: A Western Pacific Region free of malaria
GOALS: • Reduce mortality due to malaria in the Region by 50%, and morbidity
by at least 30%, by 2020, relative to 2015 baselines.
• Achieve malaria elimination in three countries by 2020.
• Establish and maintain elimination-capable surveillance systems
in the Greater Mekong Subregion by 2017, and in all countries
of the Region by 2020.
Strategic framework: pillars and objectives for 2016–2020
PILL AR 1 Universal access to malaria prevention, diagnosis and treatment
Objective 1.1 Achieve universal coverage with long-lasting insecticidal nets (LLINs)
or indoor residual spraying (IRS) for all at-risk populations no later than
2020, especially in areas of high malaria transmission.
Objective 1.2 Achieve universal access to quality-assured malaria diagnosis and
treatment no later than 2020, irrespective of household income, place
of residence or gender.
PILL AR 2 Accelerate efforts towards elimination and attainment of malaria-free status
Objective 2.1 Interrupt transmission of P. falciparum in areas of multidrug resistance,
including resistance to artemisinin-based combination therapy (ACT),
by no later than 2020.
Objective 2.2 Accelerate progress towards malaria elimination in countries aiming
for elimination by 2020.
Objective 2.3 Reduce malaria incidence in identified high-transmission areas to less
than 1 case per 1000 population-at-risk by 2020.
Objective 2.4 Define first-level subnational administrative units where malaria trans-
mission has been interrupted, and prevent the re-establishment of
malaria in those areas.
PILL AR 3 Surveillance as a key intervention
Objective 3.1 To establish elimination-capable surveillance systems (including ento-
mological surveillance) by 2017 in countries of the Greater Mekong
Subregion (GMS) and in countries aiming for elimination by 2020,
and by 2020 in all other malaria-affected countries of the Western
Pacific Region.
viSUPPORTING ELEMENTS
SUPPORTING ELEMENT 1
Strengthening the underlying health system and the enabling environment
• Strong political commitment and adequate domestic and external financial support
for malaria elimination, including ensuring the availability of sufficient, adequately
trained human resources at all levels.
• Capacity development appropriate to each country’s implementation strategy.
• Active strengthening of underlying health systems to facilitate elimination, including
increased efficiency of service delivery at the primary care level and of overall health
financing.
• Inclusion of malaria services within broader policies for delivery of health services
to meet the specific needs of mobile, migrant and hard-to-reach populations, while
also addressing gender disparities in access to services.
• Intersectoral collaboration, private sector and community involvement.
• Advocacy to support subnational political commitment for elimination efforts and
collective action.
SUPPORTING ELEMENT 2
Expanding research in support of improved service delivery and innovation
• Vector control and entomological surveillance, to better understand: the contribu-
tion of early and outdoor biting malaria vectors to malaria transmission; ecosystem
receptivity and vulnerability to malaria; how to improve the cost-effectiveness of
long-lasting insecticidal nets deployment; and the role of novel interventions.
• Case management, including approaches to: point-of-care testing for glucose-6-phos-
phate dehydrogenase deficiency; therapeutic efficacy monitoring; and the potential
role of mass drug administration.
• Social and behavioural research, including operational research, to: better define the
malaria burden among mobile/migrant and marginalized populations; help under-
stand the factors, including gender disparities, that contribute to transmission risk
among those groups; develop strategies to better manage transmission risk among
those groups; and optimize behaviour change communication.
• Health systems research and analytic work: to facilitate rapid uptake of new tools,
interventions and strategies as they are validated and strengthen, cost-effective
delivery of interventions in elimination settings.
viiREGIONAL ACTION FRAMEWORK FOR MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
PRIORITY ACTIONS
AT REGIONAL LEVEL
• Establish an elimination-capable surveillance system for malaria in all malaria-affected
countries of the Region, ensure appropriate use of data for effective targeting of
interventions, and ensure regular monitoring of their malaria situation.
• Respond aggressively to and eliminate malaria in areas with multidrug resistance –
including artemisinin-based combination therapy( ACT) resistance – in Cambodia, the
Lao People’s Democratic Republic and Viet Nam.
• Respond aggressively to and reduce transmission throughout Papua New Guinea, and
in high-transmission areas of the Lao People’s Democratic Republic, the Philippines
and Solomon Islands.
• Strengthen technical support for countries that have made significant progress
towards malaria elimination, thereby facilitating acceleration of elimination efforts
by 2020.
AT COUNTRY LEVEL
• Ensure national and subnational political commitment and sustainable domestic
funding and partnerships.
• Strengthen health system components (including surveillance, procurement and
supply management, and logistics management information systems) to maximize
efficiency through an integrated approach to facilitate universal, uninterrupted access
to quality-assured primary and preventive care for malaria.
• Use surveillance data for regular micro-stratification to better target interventions.
• Eliminate malaria in areas of multidrug resistance, including resistance to ACT.
• Address the challenges posed by P. vivax and P. knowlesi.
• Determine malaria burden among mobile/migrant and marginalized population
groups and ensure equity in access to services (including developing services tailored
to the needs of those populations).
• Achieve rapid reduction of transmission in highly endemic areas through targeted
delivery of both proven and innovative interventions.
• Ensure adequate uptake and effectiveness of interventions through sound monitoring
and evaluation.
viiiEXECUTIVE SUMMARY
Since 2000, the malaria burden in countries of the WHO Western Pacific Region
has fallen steadily in real terms, although cases reported have risen recently in
some countries, often as a result of increased case detection due to more exten-
sive roll-out of rapid diagnostic tests for malaria. Reported malaria deaths in the
Region decreased by 87% between 2000 and 2015.
The Region faces challenges on the road to malaria elimination. In particular, the epide-
miology of malaria exhibits enormous diversity, with the disease often concentrated in
remote areas and/or among highly mobile or hard-to-reach populations.
More than 70% of cases and almost all malaria deaths in the Region are due to P. falci-
parum. Resistance of P. falciparum to several antimalarial medicines, including artemisinin-
based combination therapy (ACT), has reached alarming levels in Cambodia and there
are early indications of ACT resistance in the Lao People’s Democratic Republic and
Viet Nam. Multidrug resistance is therefore both an impediment to elimination and a
reason for pursuing it.
This Regional Action Framework for Malaria Control and Elimination in the Western Pacific
(2016–2020) is guided by the WHO Global Technical Strategy for Malaria 2016–2030 (GTS)
and strongly aligned with the Strategy for Malaria Elimination in the Greater Mekong
Subregion (2015–2030). It has been developed through a series of consultations between
national malaria programmes and their partners, and WHO and individual technical
experts. Targets adopted in national malaria strategic plans and the East Asia Summit
leaders’ agreement to the goal of an Asia Pacific free of malaria by 2030 have also been
taken into consideration.
The goals of the framework are: to reduce malaria mortality in the Western Pacific
Region by 50% and morbidity by at least 30%, by 2020, relative to 2015 baselines;
achieve malaria elimination in three countries in the Region by 2020; and establish and
maintain elimination-capable surveillance systems in all malaria-affected countries of
the Western Pacific Region by 2020.
The framework is modelled on the three pillars of the GTS:
1. Universal access to malaria prevention and case management services
2. Acceleration of efforts towards elimination and attainment of malaria-free status
3. Transformation of malaria surveillance into a key intervention
ixREGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
The framework follows the parallel approach of an aggressive pursuit of burden reduc-
tion in high transmission areas and the implementation of elimination strategies, with
rigorous norms for surveillance and management in low transmission settings and in
active transmission foci.
The framework has seven objectives under the pillars (see at-a-glance summary, above).
An immediate priority is the determined reduction in malaria incidence in identified
high-transmission areas to less than 1 case per 1000 as soon as possible (in most cases,
by 2020). Consistent with the Strategy for Malaria Elimination in the Greater Mekong
Subregion (2015–2030), priority is also given to the rapid interruption of transmission
in areas affected by multidrug resistance, including resistance to ACTs. It is imperative
that efforts to address drug resistance are based on evidence, and are well coordinated
and closely monitored.
In areas and countries where transmission has been interrupted, the establishment of
elimination-ready surveillance systems will help to maintain malaria-free status and
prevent reintroduction, with a particular emphasis on strengthening preparedness and
response capacities to tackle imported malaria.
The framework highlights the need for a supportive policy environment, at both the
national and regional levels. All countries need to: ensure support from the highest level
of government to achieve effective multisectoral commitment and engagement; ensure
effective national leadership and governance, including stakeholder coordination and
expand health services to provide full access for people living or working in remote areas
including strengthening community-level services in areas with limited access to health
services in accordance with national commitments to universal health coverage (UHC).
Malaria programmes must also be supported by an adequate enabling environment that
includes stronger health systems and expanded research capability. The strengthening
of health system functions must be planned and managed effectively, including the
use of malaria related services as an entry point.
Countries must address the human resources requirements for malaria, centrally and
at all levels of the health system. They must acquire adequate financing for malaria,
but with an emphasis on the efficient use of all available health resources, especially
at the subnational level. Integrated information systems also need further investment
to ensure they are capable of delivering elimination.
xGuided by the framework, all malaria endemic countries of the Western Pacific Region
will aim for:
• a stronger health system that is able to deliver basic health services, including inter-
ventions to support malaria transmission reduction and elimination;
• universal coverage of malaria case management;
• universal coverage of appropriate vector control in transmission areas;
• full access to health and malaria services for mobile and migrant populations; and
• established and functional systems for malaria surveillance, including entomological
surveillance.
Operations will be based on a careful assessment of technical and health system factors.
In countries and subnational administrative units already reaching elimination or are
already free of malaria transmission:
• systems for adequate case-based malaria surveillance and entomological surveillance
will be established and fully functional, with mandatory notification of each case of
malaria;
• operations will be based on epidemiological investigation and classification of each
malaria case and focus;
• there will be total and effective coverage of all active foci with proven vector-control
measures based on epidemiological investigations; and
• a national malaria elimination database will be established and operational.
At the Region level, resources will be leveraged to support: training and technical
collaboration; the efficient and appropriate use of health and malaria finances; collabo-
ration in border areas; ensuring the quality of antimalarial medicines; management and
operationalization of high-priority research; monitoring and evaluation; and governance,
coordination and political commitment.
A regional mechanism to review progress under the framework will be developed to
identify lessons and experiences of mutual benefit within the Region, and to make
adjustments to regional and national strategic approaches as appropriate.
xiREGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
1. Background
1.1 Malaria in the Western Pacific Region
The World Health Organization (WHO) Western Pacific Region includes 37 countries and
areas and is home to 1.8 billion people – more than a quarter of the world’s population.
Ten of those 37 countries continue to experience malaria transmission: Cambodia, China,
the Lao People’s Democratic Republic, Malaysia, Papua New Guinea, the Philippines,
the Republic of Korea, Solomon Islands, Vanuatu and Viet Nam. Overall, approximately
735 million people are at risk of malaria, including 31 million who are at high risk.
Malaria epidemiology exhibits enormous geographical and risk group related hetero-
geneity throughout the Region – even within countries. Countries generally conform to
one of three epidemiological subgroups, based on their malaria transmission risk and
underlying social and demographic factors. Transmission is generally most intense in
the Melanesian area, mainly Papua New Guinea, some provinces of the Solomon Islands
and, to a lesser extent, Vanuatu. In the Philippines and GMS countries, transmission
is often more focal and affects ethnic minorities, migrant workers and other mobile
populations disproportionately. Three countries are approaching elimination: China,
Malaysia and the Republic of Korea.
Both P. falciparum and P. vivax are prevalent, but cases are due entirely to P. vivax in
the Republic of Korea where there is some residual local transmission. In recent years,
P. knowlesi has been recognized as the infective agent for an increasing number of
cases, especially in Malaysia.
In 2015, three countries accounted for 91% of the just over 355 000 confirmed cases
reported: Papua New Guinea (79%), Cambodia (7%) and Solomon Islands (5%). All
countries except Papua New Guinea achieved a greater than 75% decrease in the inci-
dence of microscopically confirmed cases between 2000 and 2013. The Lao People’s
Democratic Republic reported a twofold increase in cases in 2012 and 2013, but case
incidence remains less than 25% of 2000 levels.1 (1,2)
1. Unless otherwise referenced, data cited in this section were either extracted from the World Malaria
Report 2015 database maintained at the WHO Regional Office for the Western Pacific, or were reported
by national malaria programmes during the review of the Regional Action Plan for Malaria Control and
Elimination in the Western Pacific (2010–2015).
1REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
Papua New Guinea had almost a fourfold increase in confirmed cases in 2015 compared
with 2007, but this most likely reflects an increase in availability of diagnostics using
rapid diagnostic tests (RDTs). Nationally representative household surveys indicated
a drop in parasite prevalence from 12.4% to 1.8% between 2009 and 2014, while the
incidence of malaria at four sentinel surveillance sites fell from 205 per 1000 to 48 per
1000 over the same period.(3) These data are consistent with a reduction in malaria
case incidence of more than 75%.
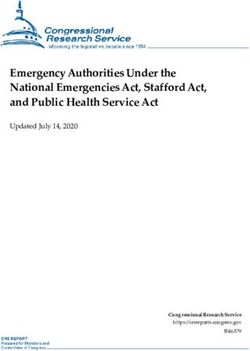
Figure 1 summarizes overall trends in reported malaria incidence for the Region as a
whole. Further detail is provided in the Annex.
FIGURE 1 Malaria caseload in the Western Pacific Region, 2000–2014
300 000
250 000
Falciparum malaria
200 000
Malaria caseload
150 000
100 000
Vivax malaria
50 000
0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2001 2012 2013 2014
Reported malaria deaths in the Region decreased by 87%, from 2360 in 2000 to 297 in
2014. Three countries accounted for 84% of all reported deaths in 2014: Papua New
Guinea (68%), and China and Solomon Islands (each 8%). Vanuatu has reported zero
deaths from malaria since 2012.
Malaysia is progressing towards elimination, reporting 5456 cases of non-zoonotic
malaria in 2007 and 1337 in 2014; less than half of cases reported in 2014 were locally
acquired – predominantly in the districts of Sabah and Sarawak.
In the Republic of Korea, which is in the elimination phase, the number of indigenous
cases was 557 in 2014. China reported just 39 indigenous cases, including 6 cases of
P. falciparum malaria and 50 cases of P. vivax in 2015, and is aiming to eliminate malaria
nationally by 2020; 97% of cases reported in 2013 and 98% in 2014 were classified as
imported.
2The Philippines is proceeding with a subnational elimination approach and by 2015, had
declared 30 of a total of 80 provinces malaria-free; the most malaria-affected provinces
– Maguindanao, Palawan and Tawi-Tawi – are subject to political instability and/or have
a substantial mobile population living in remote areas.
Figure 2 projects likely progress towards malaria elimination in countries of the Western
Pacific Region over the next 15 years, based on current trends and national strategies.
FIGURE 2 Roadmap for malaria elimination for countries of the Western Pacific Region, 2016–2030
COUNTRY 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030
Cambodia
China
Lao People’s Dem. Rep.
Malaysia
Philippines
Papua New Guinea
Republic of Korea
Solomon Islands
Vanuatu
Viet Nam
transmission reduction elimination prevention of re-introdution
1.2 Challenges to malaria control and elimination
in the Region
The major challenges to malaria control and elimination in the Region are due to the
malaria parasite and host response, population and population movement, and the
weaknesses of underlying health systems.
Challenges related to the malaria parasite and host response
Multidrug resistance of P. falciparum (including resistance to artemisinin-based combi-
nation therapy; ACT is perhaps the single greatest threat, particularly in countries of the
GMS. P. vivax parasites pose a unique set of challenges due to low density infections
and relapses.
Other technical challenges related to the host response include: individuals who remain
asymptomatic or have levels of parasitaemia that are too low to be detected using
3REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
currently available point-of-care diagnostic tools (noting also that the epidemiological
implications for transmission are not completely understood); and the lack of a diag-
nostic tool for the detection of relapse causing dormant hypnozoite parasite forms of
P. vivax in the liver.
High levels of glucose-6-phosphate dehydrogenase (G6PD) deficiency in affected popu-
lation groups can result in possible severe adverse reaction to 8-aminoquinolines, the
only class of drug available for the radical cure of P. vivax malaria.
Additionally human infection with simian malaria such as P. knowlesi presents new
challenges to malaria diagnosis, control and elimination that are unique to this Region.
Challenges related to populations
At the population level, malaria burden is often greater among mobile populations,
migrants (both within countries and between countries) and minority groups and
other hard-to-reach populations in remote areas or areas inaccessible due to conflict.
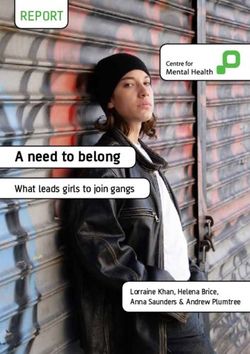
Ensuring universal access to malaria prevention interventions among high-risk popula-
tions will be a key activity for accelerating malaria elimination in the Region. Figure 3
presents World Malaria Report estimates of the proportion of high risk populations
adequately protected by vector control interventions, such as insecticide-treated bed
nets (ITNs) and indoor residual spraying (IRS).
FIGURE 3 Percentage of high-risk population in the Region protected by ITNs or IRS in 2014
Malaysia
Solomon Islands
Papua New Guinea
Vanuatu
Philippines
Lao People’s Dem. Rep.
Cambodia
China
Viet Nam
Republic of Korea
0 20 40 60 80 100
Percentage (in %) ITN IRS
Source: World Malaria Report 2015.
4Increasing numbers of workers are also travelling from countries in the Region to
malaria-endemic countries outside the Region, and add to the ongoing risk of malaria
importation.(4,5)
Health system challenges
Key health system issues hampering progress in some countries include weak surveil-
lance systems and capacity, limited human resources, insufficient funding and weak
technical capacity.
Human resources capacity needs to be strengthened and maintained until transmission
is interrupted, and possibly for some time thereafter. As malaria incidence falls to very
low levels and interventions become more focal, a more complete integration of malaria
services with broader primary and preventive care is recommended and will consider-
ably reduce the need for dedicated malaria staff. However, it will still be necessary to
retain quality technical leadership and management at national level.
Limitations in financing and technical capacity have seen a slowing of elimination efforts
and a delay in elimination time-frames in Solomon Islands and Vanuatu. In Papua New
Guinea, national revenues have been severely affected by a downturn in global oil and
natural gas prices and this will inevitably place pressure on government investment in
social sectors such as health and education.(6)
From 2008 to 2014, external donors provided about 90% of malaria financing in Melanesia
(Papua New Guinea, Solomon Islands and Vanuatu) and about 80% in GMS countries
(Cambodia, the Lao People’s Democratic Republic and Viet Nam), and the proportion
of donor financing was either steady or increasing over that period. Constrained donor
budgets following successive global economic downturns are now likely to see a reduc-
tion in donor engagement in the Region, forcing countries to identify additional sources
of domestic funds and to increase efficiencies within their health care systems. In the
Philippines, the government provides an increasing proportion of malaria funding,
currently about 50%. In China, Malaysia and the Republic of Korea, 100% of malaria
funding is from government revenues.
Other health system challenges include:
• weak commodity procurement systems and supply chain management;
• weak systems for monitoring and evaluation;
• an unregulated private health sector, which may not participate effectively in surveil-
lance systems and may allow the use of ineffective antimalarial medicines or marketing
of unregulated vector control products; and
• periodic humanitarian and environmental crises and political instability, all of which
compromise population access to health services.
5REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
1.3 Development of the Regional Action Framework
WHO Global Technical Strategy for Malaria 2016–2030
Endorsed by the World Health Assembly in May 2015, the Global Technical Strategy
for Malaria 2016–2030 (GTS) was the result of an extensive consultation process that
spanned two years. The GTS is discussed in more detail in Section 2.2, below.
The rationale for undertaking malaria elimination in the Region
Various factors have converged to create an urgent need for action to enhance, control
and, where possible, accelerate elimination of malaria from the Region. These include:
the magnitude of the threat of drug resistance; the commitment of governments; the
contribution that malaria control and elimination can make to broaden health and
development outcomes; the substantial impact and cost-effectiveness of the scaled-up
interventions currently being applied; the keen interest of partners; and the additional
momentum provided by recent scientific advances.
Also, in May 2015, the Strategy for Malaria Elimination in the Greater Mekong Subregion
(2015–2030) – aligned with the GTS – was jointly launched by the ministers of health
of GMS countries.
Malaria elimination represents a complementary approach to strengthening health
systems and promoting health security in the Region, with the potential to leverage
donor financing as disease-specific funding declines. Any delay in addressing the problem
of multidrug resistance in the GMS could lead to the emergence of untreatable falci-
parum malaria or the further geographical spread of artemisinin resistance, which would
adversely impact regional and global health security.
The Strategy for Malaria Elimination in the Greater Mekong Subregion (2015–2030)
responds to the worsening multidrug resistance situation, including resistance to ACT.
The strategy builds on the WHO recommendation that GMS countries affected by
artemisinin resistance adopt the goal of accelerated elimination of P. falciparum, to
counter the threat of multidrug resistance.
The need for a Regional Action Framework
The GTS presents a broadly inclusive approach for addressing current challenges to
malaria control and elimination at the global level, while the Strategy for Malaria Elimi-
nation in the Greater Mekong Subregion (2015–2030) addresses the needs of a sub-set
of countries with a specific threat from drug resistance.
6Each WHO region needs to adapt the approaches of the GTS along the continuum of
transmission reduction to malaria elimination to meet the specific needs of Member
States.
Process of developing the Regional Action Framework
The planning process for developing the Regional Action Framework for Malaria Control
and Elimination in the Western Pacific (2016–2020) included consultations with national
malaria programmes in all malaria endemic countries in the Region, WHO country office
malaria focal points and partners.
A regional malaria expert group convened in December 2015 to review the previous
Regional Action Plan for Malaria Control and Elimination in the Western Pacific (2010–2015)
and to identify lessons that could inform the new framework. This was followed by a
meeting of malaria programme managers in May 2016 to review and discuss a draft
version of the framework.
This framework will serve as a guide to national planning and provide countries with a
model to guide mobilization of domestic and external funding, based on WHO-endorsed
strategies adapted specifically to the needs of the Region.
7REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
2. The Regional Action Framework
2.1 Vision and goals
OVERALL VISION: A Western Pacific Region free of malaria.
ULTIMATE GOALS • Eliminate malaria in all countries in the Western Pacific
(by 2030): Region by 2030.
• Maintain malaria-free status and prevent reintroduction
in countries and areas where malaria transmission has been
interrupted.
GOALS FOR THE • Reduce mortality due to malaria in the Region by 50%, and
REGIONAL ACTION: morbidity by at least 30%, by 2020, relative to 2015 baselines.
FRAMEWORK
2016–2020 • Achieve malaria elimination in three countries by 2020.
• Establish elimination-capable surveillance systems in GMS
countries by 2017, and in all countries in the Region by 2020.
2.2 Alignment with the Global Technical Strategy
The Global Technical Strategy for Malaria 2016–2030 is based on three interlinked strategic
pillars and two supporting elements to guide global efforts towards malaria elimination
and is summarized in the box.
The Regional Action Framework for Malaria Control and Elimination in the Western Pacific
(2016–2020) follows the strategies proposed in the GTS. It adapts the three pillars and
two supporting elements of the GTS to the malaria and health system priorities of
countries in the Western Pacific Region for the first 5-year period of the GTS, 2016–2020.
It also builds on lessons learnt from the review of the previous Regional Action Plan for
Malaria Control and Elimination in the Western Pacific (2010–2015).
8VISION: A WORLD FREE OF MALARIA
Milestones Targets
GOALS
2020 2025 2030
Reduce malaria mortality rates globally
At least 40% At least 75% At least 90%
compared with 2015
Reduce malaria case incidence globally
At least 40% At least 75% At least 90%
compared with 2015
Eliminate malaria from countries
At least 10 countries At least 20 countries At least 35 countries
in which malaria was transmitted in 2015
Prevent re-establishment of malaria Re-establishment Re-establishment Re-establishment
in all countries that are malaria-free prevented prevented prevented
STRATEGIC FRAMEWORK
Comprising three major pillars, with two supporting elements
MAXIMIZE IMPACT OF TODAY’S LIFE-SAVING TOOLS
Pillar 1. Ensure universal access to malaria prevention, diagnosis and treatment
Pillar 2. Accelerate efforts towards elimination and attainment of malaria-free status
Pillar 3. Transform malaria surveillance into a core intervention
SUPPORTING ELEMENTS
1. Harnessing innovation and expanding research
– Basic research to foster innovation and the development of new and improved tools
– Implementation research to optimize impact and cost-effectiveness of existing tools and strategies
– Action to facilitate rapid uptake of new tools, interventions and strategies
2. Strengthening the enabling environment
– Strong political and financial commitments
– Multisectoral approaches, and cross-border and regional collaborations
– Stewardship of entire heath system, including the private sector, with strong regulatory support
– Capacity development for both effective programme management and research
Source: The WHO Global technical strategy for malaria 2016–2030
Principles underpinning the Regional Action Framework
The Regional Action Framework is guided by the following principles (five of which are
modelled on the GTS, with three additional principles that are specific to the Western
Pacific Region).
• All countries can accelerate efforts towards elimination through combinations of
interventions tailored to local contexts.
• Country ownership and leadership, with participation of communities, are essential
to accelerate progress through a multisectoral approach.
• Partners can maximize the use of national health systems for planning, procurement,
service delivery and reporting, and wherever possible, partner support will aim to
strengthen those national systems, rather than develop parallel mechanisms.
9REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
• A multisectoral approach includes the involvement of the private sector.
• Improved malaria case surveillance, periodic re-stratification based on the dynamics
of malaria disease burden, M&E and entomological surveillance are required to opti-
mize implementation of malaria interventions.
• Equity in access to quality assured preventive, diagnostic and curative services is
essential, especially for the most vulnerable and hard-to-reach populations.
• Malaria prevention, case management and control services will be included in all
packages of essential health services as UHC is rolled out in countries of the Region.
• Innovation in implementation approaches at the local level and the adoption of new
tools will enable countries to maximize their progress towards malaria elimination.
Adapting the three pillars of the GTS to different transmission settings
The strategic pillars of the framework are aimed at guiding regional- and country-level
actions to accelerate transmission reduction and ultimately eliminate malaria in the
regional and country contexts.
The three pillars of the GTS represent a path towards elimination – a continuum – based
on a steady transition through stronger surveillance systems and health system integra-
tion. Countries can use the strategies embedded in the GTS pillars to accelerate their
progress towards malaria elimination from any point on the continuum, whatever their
current malaria incidence or transmission intensity. As it is a continuum, there are also
natural points of strategic overlap between Pillars 1 and 2, and between Pillars 2 and 3.
PILLAR 1
Ensure universal access to malaria prevention, diagnosis and treatment
This is the starting point for countries with higher malaria incidence rates and trans-
mission intensity. Cornerstones are universal coverage of the population at risk with
appropriate vector control and other preventive interventions and effective informa-
tion on how to reduce the risk of malaria, backed up by ready access to quality-assured
diagnosis, treatment and clinical follow-up.
Pillar 1 is worded in the language of UHC.2 (7,8) In the context of UHC, “universal” does
not necessarily mean 100% population coverage with every malaria control interven-
tion (although it may, in settings of high transmission risk). Populations need access
to defined interventions – “the services they need” – which will, in turn, be defined in
2. Universal health coverage means that all people can use the promotive, preventive, curative, rehabilitative
and palliative health services they need, of sufficient quality to be effective, while also ensuring that the
use of these services does not expose the user to financial hardship (World Health Report, 2010; Bangkok
Statement: Priority Setting for UHC, 2016). A commitment to UHC is currently being adopted by most
countries of the Region.
10national malaria strategic and operational plans. This is likely to vary from population
to population according to their transmission risk, especially where the malaria epide-
miology in different parts of a country are at different stages along the continuum
towards elimination, or where there are variations in the prevalence of specific risks (e.g.
drug-resistant P. falciparum). Innovative approaches and non-traditional partnerships
may be needed to reach mobile, migrant and other hard-to-reach populations (including
ethnic minorities living in remote and/or border areas).
PILLAR 2
Accelerate efforts towards elimination and attainment of malaria-free status
This includes all of the strategic interventions that are needed as a national or subnational
malaria programme successfully reduces transmission intensity. Specific challenges
addressed during the period include: strengthening malaria surveillance and possible
transition to case-based surveillance (depending on case numbers); implementation of
universal, quality-assured parasitological diagnosis of every case; ensuring and protecting
the efficacy of specified treatment protocols; developing specific strategies for addressing
the challenge of P. vivax; and re-designing communicable disease control programmes
and related elements of the health system along more integrated (rather than disease-
specific) lines. Effective engagement with the private sector is essential.
The strategic interventions continue beyond achieving elimination and include early
detection of possible imported cases and the prevention of reintroduction in areas
where local transmission has been interrupted.
PILLAR 3
Transform malaria surveillance into a key intervention
This reflects the fundamental importance of effective surveillance to better understand
transmission dynamics in control settings and elimination settings. In control settings,
strengthened surveillance will provide for better targeting of interventions and in elimi-
nation settings will provide for responding appropriately to any cases identified. This
will contribute to better allocation of resources in an efficient and effective manner,
and will contribute to achieving accelerated reduction of malaria transmission.
Key activities under Pillar 3 can commence even while transmission intensity is relatively
high. The process defined by Pillar 3 is: a programme reorientation which includes a
11REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
transition from population-based to case-based surveillance and response (at the correct
time, which is when case numbers reach a low enough level for this to be both feasible
and efficient); management of identified or potential foci of transmission; and ensuring
rapid and timely response to identified cases.
2.3 Supporting elements
The framework has two supporting elements, aligned with the GTS but re-prioritized
to reflect and address the needs of the Western Pacific Region. Each covers a number
of key requirements for the successful acceleration of malaria transmission-reduction
and elimination in the Region.
SUPPORTING ELEMENT 1
Strengthening the underlying health system and the enabling environment
• Strong political commitment and adequate domestic and external financial support
for malaria control and elimination, including ensuring the availability of sufficient,
adequately trained human resources at all levels.
• Capacity development appropriate to each country’s implementing strategy.
• Active strengthening of underlying health systems to facilitate elimination, including
increased efficiency of service delivery at the primary care level and of health financing
overall.
• Inclusion of malaria services within broader policies for delivery of health services
to meet the specific needs of mobile, migrant and hard-to-reach populations, while
also addressing gender disparities in access to services.
• Intersectoral collaboration, private sector and community involvement.
• Advocacy to support subnational political commitment to accelerate control and
elimination efforts and collective action.
SUPPORTING ELEMENT 2
Expanding four themes of research in support of improved service delivery and innovation
• Vector control and entomological surveillance, to better understand: the contribu-
tion of early and outdoor biting malaria vectors to malaria transmission; ecosystem
receptivity and vulnerability to malaria; how to improve the cost-effectiveness of
long-lasting insecticidal net (LLIN) deployment; and the place of novel interventions.
• Case management, including approaches to: point of care testing for glucose-6-phos-
phate dehydrogenase deficiency; therapeutic efficacy monitoring in elimination
settings; and the potential role of mass drug administration.
12• Social and behavioural research, including operational research, to: better define the
malaria burden among mobile/migrant and marginalized populations; help under-
stand the factors, including gender disparities, that contribute to transmission risk
among those groups; develop strategies to better manage transmission risk among
those groups; and optimize behaviour change communication.
• Health systems research and analytic work, to facilitate rapid uptake of new tools,
interventions and strategies as they are validated, and strengthen cost effective
delivery of interventions in elimination settings.
2.4 Priority actions
This Regional Action Framework for Malaria Control and Elimination (2016–2020) aims
for an accelerated scale-up of appropriate interventions in all endemic areas, tailored
to local epidemiology and health systems.
Nevertheless, to make the best and most efficient use of available resources, there is a
need to prioritize at both regional and country levels.
Factors to be considered include the past and current intensity of transmission in an
area, the degree of resistance to different antimalarial drugs and insecticides, and the
size and mobility of affected populations. If a high-burden area is located near a low-
burden area, then early reduction of transmission in the high-burden area will likely
make it easier to achieve elimination in both.
PRIORITY ACTIONS AT REGIONAL LEVEL
• Establish an elimination-capable surveillance system for malaria in all malaria-affected
countries of the Region,3 ensure appropriate use of data for effective targeting of
interventions, and ensure regular monitoring of their malaria situation.
• Respond aggressively to malaria and eliminate in areas with multidrug resistance
(including ACT resistance) in Cambodia, the Lao People’s Democratic Republic and
Viet Nam.
• Respond aggressively to malaria and reduce transmission throughout Papua New
Guinea, and in high-transmission areas of the Lao People’s Democratic Republic, the
Philippines and Solomon Islands.
• Strengthen technical support to all countries, helping them to address the challenges
posed by P. vivax, including countries that have made significant progress towards
malaria elimination, and facilitate the acceleration of efforts to achieve elimination
by 2020.
3. This analysis should include past malaria incidence data and risk determinants related to the human host,
parasites, vectors and the environment.
13REGIONAL ACTION FRAMEWORK for MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC (2016–2020)
PRIORITY ACTIONS AT COUNTRY LEVEL
• Ensure national and subnational political commitment and sustainable domestic
funding and partnerships.
• Strengthen health system components (including surveillance, procurement and
supply management, and logistics management information systems) to maximize
efficiency through an integrated approach to facilitate universal, uninterrupted access
to quality-assured primary and preventive care for malaria.
• Use surveillance data for regular micro-stratification to better target interventions.
• Eliminate malaria in areas of multidrug resistance, including resistance to ACT.
• Address the challenges posed by P. vivax and P. knowlesi.
• Determine malaria burden among mobile/migrant and marginalized population
groups and ensure equity in access to services (including developing services tailored
to the needs of those populations).
• Achieve rapid reduction of transmission in highly endemic areas through targeted
delivery of both proven and innovative interventions.
• Ensure adequate uptake and effectiveness of interventions through sound monitoring
and evaluation.
Local analysis may identify additional priorities
This prioritization does not mean that efforts to eliminate malaria in low-transmission
areas should be put on hold, only that such efforts must not take precedence over
addressing burden reduction and major threats such as drug resistance. In most coun-
tries, certain areas should be eligible for accelerated elimination as soon as the necessary
systems have been developed. Ideally, those systems should be integrated into primary
and preventive care services, with ongoing technical oversight to ensure quality of care.
143. Strategic approaches to achieving
objectives for each pillar
PILLAR 1
Ensure universal access to malaria prevention, diagnosis and treatment
Objective 1.1: Achieve universal coverage with long-lasting insecticidal nets (LLINs)
or indoor residual spraying (IRS) for all at-risk populations no later than
2020, especially in areas of high malaria transmission.
Objective 1.2: Achieve universal access to quality-assured malaria diagnosis and treat-
ment no later than 2020, irrespective of household income, place of
residence or gender.
The WHO recommended core interventions – quality-assured vector control, chemo
prevention (where relevant), diagnostic testing and treatment – can dramatically reduce
morbidity and mortality and accelerate the progress of national malaria programmes
towards elimination. In areas of moderate-to-high transmission, ensuring universal
access of populations at risk to interventions will be a principal objective for the Region
and for national malaria programmes.
This framework recommends simultaneous implementation of two complementary
sets of key interventions:
1. Prevention strategies based on vector control and, in certain settings and in some
populations and occupational groups, administration of chemoprevention and the
use of other personal preventive measures; and
2. Universal diagnosis and prompt, effective treatment of malaria in public and private
health facilities and at the community level in high transmission settings.
Structuring national strategies and subnational programmes based on stratification of
malaria by disease burden and an analysis of access to services will enable the tailoring
of interventions to the local context and ensure efficient use of resources. 4
4. This analysis should include past malaria incidence data and risk determinants related to the human host,
parasites, vectors and the environment.
15You can also read