The Queensland Pēpi-Pod Program: A strategy to promote safe sleeping environments and reduce the risk of Sudden Unexpected Deaths in Infancy in ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Please do not remove this page The Queensland Pēpi-Pod® Program: A strategy to promote safe sleeping environments and reduce the risk of Sudden Unexpected Deaths in Infancy in Aboriginal and Torres Strait Islander communities Young, Jeanine; Cowan, Stephanie; Watson, Karen; et.al. https://research.usc.edu.au/discovery/delivery/61USC_INST:ResearchRepository/12133759420002621?l#13133759020002621 Young, Cowan, S., Watson, K., Kearney, L., & Craigie, L. (2018). The Queensland Pēpi-Pod® Program: A strategy to promote safe sleeping environments and reduce the risk of Sudden Unexpected Deaths in Infancy in Aboriginal and Torres Strait Islander communities. University of the Sunshine Coast. https://doi.org/10.25907/00011 Document Type: Published Version USC Research Bank: https://research.usc.edu.au research-repository@usc.edu.au It's your responsibility to determine if additional rights or permissions are needed for your use. Downloaded On 2022/06/20 18:41:20 +1000 Please do not remove this page
FINAL RESEARCH REPORT
for the
Department of
Child Safety, Youth & Women
Due 30th July 2018
The Queensland Pēpi-Pod® Program:
A strategy to promote safe sleeping environments and reduce
the risk of Sudden Unexpected Deaths in Infancy in Aboriginal
and Torres Strait Islander communities
Chief Investigator
Professor Jeanine Young
Co-Investigators
Mrs Stephanie Cowan
Mrs Karen Watson
Dr Lauren Kearney
Ms Leanne Craigie
Suggested Citation:
YOUNG J, COWAN S, KEARNEY L, WATSON K, CRAIGIE L. (2018) A strategy to promote safe sleeping
environments and reduce the risk of Sudden Unexpected Death in Infancy in Aboriginal and Torres Strait Islander
communities. (ID: 99489008702621) Final Implementation Project Report for the Department of Child Safety,
Youth and Women, Queensland Government. University of the Sunshine Coast, Sippy Downs, Queensland.
Available at https://doi.org/10.25907/00011
1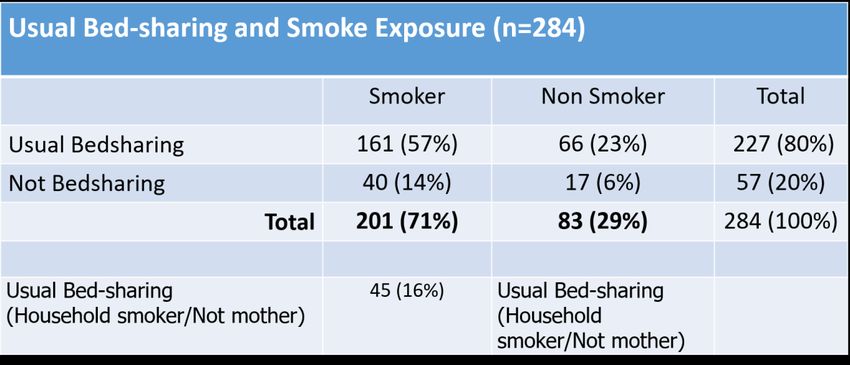
Title: The Queensland Pēpi-Pod® Program
A strategy to promote safe sleeping environments and reduce the risk of
Sudden Unexpected Deaths in Infancy in Aboriginal and Torres Strait
Islander communities
RESEARCH TEAM
Chief Investigator:
Professor Jeanine Young,
Professor, School of Nursing and Midwifery, University of the Sunshine Coast;
Member, Red Nose National Scientific Advisory Group (Chair 2008-2015)
Member, Queensland Paediatric Quality Council & Infant Mortality
Subcommittee
Member, Queensland Child Death Review Panel
Member, Australian College of Midwives Scientific Review & Advisory Group
Honorary Professor, Centre for Online Health, University of Queensland
Visiting Professor, Sunshine Coast Hospital & Health Service (HHS)
Visiting Senior Research Fellow, Children’s Health Queensland HHS
Co-Investigators (members of original project team)
Mrs Stephanie Cowan, Director, Change for Our Children, New Zealand;
Dr Lauren Kearney, Senior Research Fellow, University of the Sunshine
Coast and Sunshine Coast HHS, Queensland Health;
Mrs Karen Watson, PhD Candidate, School of Nursing, Midwifery &
Paramedicine, University of the Sunshine Coast
Ms Leanne Craigie, Indigenous Health Coordinator, Children’s Health
Queensland Hospital & Health Service
STUDY COMMENCEMENT: 16th May 2017 (as per contract signature)
(J Young notified 23 May 2017)
DISTRIBUTION TO BE COMPLETED: 30th June 2018
FINAL REPORT DUE: 30th July 2018
2
Contents
Overview: Outcomes to be reported ............................................................ 4
1. The Pēpi-Pod® Program: background and underpinning conceptual
frameworks ...................................................................................................... 4
Program Components .................................................................................. 5
Theoretical and Conceptual Framework ....................................................... 6
Ethical Principles .......................................................................................... 8
2. Data Reporting ............................................................................................. 8
3. Embedding of Program .............................................................................. 10
4. Provider Training........................................................................................ 12
5. Recommendations for risk mitigation in future programs ........................... 14
6. Pēpi-Pod® distribution with participating services .............................. 16
Priority areas for Pēpi-Pod® distribution .................................................... 16
Process for assessment and collection of data relating to family
vulnerabilities.............................................................................................. 18
Family Demographics and Risk Factors that increase risk of SUDI ........... 21
Pēpi-Pod Use ............................................................................................. 23
Interaction between smoking and bedsharing ............................................ 28
7. Program Orientation - service participation .......................................... 30
8. Distributer Survey Results ...................................................................... 32
9. Provision of relevant research outcomes. ............................................. 35
10. Budget ..................................................................................................... 35
11. Discussion................................................................................................ 36
12. Recommendations ................................................................................... 39
13. Conclusion ............................................................................................... 44
14. Reference List .......................................................................................... 45
Appendix A: Pēpi-Pod® Program Service Provider Support .......................... 48
Appendix B: Current Services ........................................................................ 50
3Overview: Outcomes to be reported
This final report for the project funding awarded by the Department of Child
Safety, Youth and Women shall include the following:
1. Overview of the Pēpi-Pod® Program and underlying theory;
2. Details of the distribution of Pēpi-Pod®’s to services sites;
3. Summary of the data returned to date for families receiving the Pēpi-
Pod®;
4. Information about Pēpi-Pod® Program education sessions, including
attendance levels, workplace and role descriptions of the attendees;
5. Recommendations for future implementation and provision of the Pēpi-
Pod® Program in Queensland.
Publications are being prepared from the original research project (conducted
during 2013-June 2017) relating to:
A forensic clinical commentary relating to role of traditional portable
sleep spaces in reducing risk of mechanical suffocation of infants;
An integrative review of in-hospital and community-based portable
infant sleep spaces;
Parent experiences of the Queensland Pēpi-Pod® Program;
Health worker perspectives of how the Pēpi-Pod® Program assisted
health promotion relating to safe sleeping and smoking reduction in
Aboriginal and Torres Strait Islander communities.
1. The Pēpi-Pod® Program: background and underpinning conceptual
frameworks
Originally developed by Ms Stephanie Cowan, Change for Our Children in
New Zealand, in response to high rates of Sudden Unexpected Deaths in
Infancy [SUDI] amongst their Māori population, the Pēpi-Pod® Program and
Wahakura Program [a woven flax infant sleep basket which is a recreation of
the traditional Māori porakaraka] (Tipene-Leach and Abel, 2010), have been
introduced as integral components of a multi-agency targeted national safe
sleep initiative. This combined initiative has been credited with contributing to
4a 29% reduction in New Zealand’s post-perinatal mortality during the period 2009-2015 (Mitchell et al., 2016). In late 2017, these targeted Programs were estimated to have contributed to a total 36% infant mortality reduction since 2009, as reported at the international conference on Baby Survival held in June 2018 (Mitchell, 2018). Randomised controlled trials of the Pēpi-Pod® portable sleep space in New Zealand have demonstrated it to be as safe as the recommended standard bassinet for infant sleep across measures of safety and stability of infant physiology (Baddock et al., 2017; Baddock et al., 2018; McIntosh et al., 2018; Tipene-Leach et al., 2018). Program Components The Pēpi-Pod® Program comprises three core components which are interlinked. These components include a portable sleep space, safe sleep education delivered by a known health care professional, and a family commitment to use the Pēpi-Pod® as intended and to share the safe sleeping messages within their social network (Cowan, 2015a). These core components are described here in more detail: 1) A Safe Sleep enabler (also referred to in the literature as a portable infant sleep space or infant safe sleep device): a safe sleep space that provides for an unobstructed infant airway, particularly in high risk environments. This sleep space consists of a polypropylene box transformed into an infant bed through the addition of culturally suitable fabric covers and a 3cm upholstery- density, fabric covered, tight fitting mattress and bedding (mattress protector, base slip-on sheet, wrap around sheet, light blanket). 2) Safe Sleep Education: which imparts practical safe infant sleeping information for families to use and adapt for their family situation. This education includes evidence-based infant settling and sleep strategies to reduce the risk of SUDI (Mitchell, et al., 2012; QH, 2008, 2012a, 2012b; Young et al., 2012) consistent with SIDS and Kids safe infant sleeping public health recommendations. This information is delivered by a health promotion officer and/or service health professional who has undertaken the Pēpi-Pod® training package and includes the safety briefing consisting of the ‘Rules of protection’ and ‘Through the Tubes’ education (Cowan et al., 2013; Cowan, 2015b). 5
3) Family commitment: participating families are asked to use the Pēpi-Pod® as intended and to make a commitment to spread safe sleeping messages about protecting babies as they sleep. Inviting families to undertake an education role through their participation in the Pēpi-Pod® Program is intended to empower, entrust and extend the influence of the Program within a family’s priority networks (Cowan et al., 2013; Young et al., 2013). Theoretical and Conceptual Framework Diffusion of Innovation theory was successfully used as an implementation strategy for the Pēpi-Pod® Program in New Zealand, as it underpins the Programs core components and supports Pēpi-Pod® Program delivery in locally relevant ways. For the Queensland implementation of the Pēpi-Pod® Program, it was recognised that consideration for the diversity that exists between, and within, Aboriginal and Torres Strait Islander communities was important. It is acknowledged that for interventions to make a difference they need to focus not only on the individual and their behaviour, but also on environmental factors that influence behaviour (Bronfenbrenner, 1979; Salm- Ward & Doering, 2014). For this reason, Socio-ecological Theory which recognises that an individual’s behaviour is influenced by a number of levels of environmental contexts, including their developmental history, informed the Queensland Pēpi-Pod® Program evaluation (Bronfenbrenner, 1979). The Socio-ecological Model also provided a framework that supported strength- based approaches and aimed to utilise the protective factors inherent to Aboriginal and Torres Strait Islander culture including extended kinship ties and community commitment, and also to prioritise the direct involvement by Indigenous peoples in co-design and development of the Program tools and materials used in the safe sleep education. The Program evaluation focused on the individual, interpersonal and community level systems (See Figure 1). 6
Figure 1: The Socio-ecological Model [SEM] was used to inform system level feedback for the Pēpi-Pod® Program evaluation (Bronfenbrenner, 1979). Individual level characteristics are those that influence behaviour such as knowledge, skills, attitudes, self-efficacy, values and goals. These also include factors such as ethnicity or economic or financial status. In this project, individual factors [Micro system level] that contribute to vulnerability [such as birth weight and gestation] and care giver and family characteristics such as bed sharing practices and knowledge about safe infant sleep, were targeted by the Pēpi-Pod® Program. Evaluation took place through participant feedback. Interpersonal level characteristics are those that relate to influence exerted by family, friends and acquaintances and the formal and social relationships that influence behaviour. In this Program, interpersonal level factors [Meso system level] included extended kinship and family members, friends, and community members. The Pēpi-Pod® program impacted the Interpersonal level through asking Program participants to spread what they learnt about safe infant sleep within their social groups. Evaluation of this aspect took place through participant feedback. Community level characteristics are those that relate to the external community and environmental factors. For this study Community level factors [Exo-system] includes elders, community leaders and local health professionals and health service providers. The Pēpi-Pod® Program impacted 7
Community levels of the Socio-ecological system through capacity building of health workers and health professionals working within service sites and utilising local models of care and health care providers and services known to families to provide the Pēpi-Pod® Program. Evaluation of this aspect of the Program took place through Health Professional feedback on the Program within their community (Bronfenbrenner, 1979; Stokols, 1996; Watson, 2018). Ethical Principles Underpinning the Pēpi-Pod® Program implementation was also the ethical considerations essential in working with Aboriginal and Torres Strait Island peoples and communities (NHMRC, 2003; Jamieson et al., 2012). Examples of how the program supported key ethical principles included: Self-determination: All participating service sites opted in to the Pēpi-Pod® Program, with the majority approaching the Project team to request to take part following word of mouth spread of information from original service sites. Respectful partnerships: participation in the Pēpi-Pod® Program builds capacity within a service site work force and ongoing support for the program has been provided by the project team. Flexibility and recognition of diversity: the Pēpi-Pod® Program has been implemented within service sites according to the model of care practised within that site, while still adhering to the core components of the Program. Support community ownership: through developing the local workforce and implementation of the Program by local and familiar health care providers, communities have developed ownership over the Pēpi-Pod® Program and services sites have embedded it into their usual service delivery. 2. Data Reporting This section will clarify the Department’s question relating to data reporting: specifically, the possibility of data reporting continuing subsequent to 30 June 2018, and if so, how this data will or could be utilised. The Pēpi-Pod® Program has been trademarked to maintain the quality and integrity of the Program. Service site staff who have collaborated with Program coordinators to deliver the Pēpi-Pod® Program within their 8
community have agreed to a) deliver the program as intended and b) to demonstrate this through the provision of a minimal dataset which relates to prioritising distribution of resources to families with known vulnerabilities and delivery of the safety briefing with parent safe sleep education. This minimal dataset is an ongoing component and expectation of both the Queensland and New Zealand national Pēpi-Pod® Programs. Change for our Children [New Zealand] in collaboration with the Queensland team, have developed an online database to capture data relating to distribution and follow-up of families with infants aged approximately 6-8 weeks, suitable for use in both New Zealand and Queensland (and other states and territories). Participating sites have been requested to contribute de-identified participant information through this online portal which is available on the paper tool distributed with each infant bedding pack, the USC website, Change for our Children website, Staff Toolkit and Program Materials. This information is provided, demonstrated and reinforced in workshops and periodic newsletters have been sent to participating sites to encourage data return. The online feedback form is available at: [https://changeforourchildrennz.sites.acclipse.com/pepi_pod_programme/data _record_nzau] This database allows agencies to monitor and evaluate their Pēpi-Pod® service by retaining with their service’s confidential paper records that contain identifying data, and only enter the de-identified information at one time point that relates to key program indicators. This functions as an in-built evaluation platform for service sites and is expected to continue. This allows us to capture information that is de-identified and able to be reported for quality assurance purposes. Provision of potentially identifiable data would require consideration of confidential storage of records, and a considerable undertaking to resource ethical and governance agreements that would be required; these conditions were discussed in early 2017 with Department staff and with USC ethics to ensure minimal data could be recorded without the necessity of multiple nongovernmental, governmental 9
and tertiary agreements in place, particularly in light of the research project being completed and the move for program integration into service delivery models, made by many participating services prior to July 2017. Although this minimal dataset is an ongoing component and expectation of the Queensland and New Zealand Pēpi-Pod® Programs, it is not enforceable at local level, and is reliant on service commitment and staffing for service documentation. Individual service deidentified data can be provided to service providers on request (if they have included their health service in the appropriate data field entry) but in a raw format that requires collation and interpretation by their own staff. The New Zealand Program aims for service providers to contribute 80-90% distribution data and 50-60% follow-up data (at 6-8 weeks) to maintain a level of consistency in reporting and recording. If the Pēpi-Pod® Program was to continue in Queensland and indeed Australia [Western Australia has commenced distribution of the Pēpi-Pod® Program through Red Nose 2017- 2018; the Victorian Council on Obstetric and Paediatric Mortality and Morbidity has recently recommended in March 2018 that the Pēpi-Pod® Program be instituted in their services for vulnerable families (Recommendation 9: Victoria State Government, 2017)], it would be strongly recommended that a dedicated officer be funded to follow-up and support services in completing minimal data requirements. 3. Embedding of Program Recommendations you have with respect to embedding the Program in existing services, having regard to feedback you may have received throughout the trial The value of the Pēpi-Pod® Program in reducing risk of adverse outcomes for vulnerable infants has been noted by the Queensland Paediatric Quality Council and the Queensland Family and Child Commission, in the most recent QFCC Annual report on Deaths of Children and Young People Queensland 2016-2017 (QFCC, 2018). The Victorian Council on Obstetric and Paediatric Mortality and Morbidity have recommended that portable sleep spaces like the Pēpi-Pod® or Wahakura be provided to families for vulnerable babies (Recommendation 9) (Victorian State Government, 2017). 10
The approach used by the project team to implement the Pēpi-Pod® Program within a service site has been successful as measured by 1) recruitment of families with identified vulnerabilities that place them at higher risk of infant death; 2) high proportion of families who stated they received the safety briefing and safe sleep messaging; 3) positive family feedback; 4) staff feedback relating to usefulness of the program as a practical safe sleeping education tool for high risk families. Recommendations for future implementation or continuing support of the Program would include appropriate resourcing to provide for ongoing program coordination in order to maintain integrity of key components and data completion; if risk assessment data reporting was considered to be a high priority. Service sites that have embedded the Pēpi-Pod® Program within their usual Maternal and Child Health Program have demonstrated positive results. An exemplary practice model is Apunipima Cape York Health Council which incorporated the Pēpi-Pod® Program into their existing Baby One Program (the original first 1000 days model in Queensland) during the original Pēpi- Pod® Program research trial in 2014-2017 (Watson, 2018). The Program continues to be delivered by Indigenous Maternal and Child Health Workers throughout the Cape supported by maternal and child health nurses and has become ‘expected and normal practice’ within a number of remote communities with the service committing to part funding of this program. Recommendation: The Pēpi-Pod® Program appears to function most effectively as part of a health focussed maternal and child health model in which safe sleeping education is provided at several timepoints during pregnancy and early infancy to provide opportunities for conversations around infant sleep environments as babies grow and develop. Another example of engaged services in regional locations would include the Royal Flying Doctors Service Cairns Base and the Ngarrama Maternity Service offered through Redcliffe Hospital where the Program is provided to families throughout the community through a Midwife and Indigenous Health Worker collaborative model within the Maternal Child Health Team. The potential to develop provider networks that include other population groups in addition to Aboriginal and Torres Strait Islander families, who 11
may be experiencing greater social vulnerability associated with increased
infant mortality, is strongly recommended as the next step. This would include
consideration for Program provision through Child Safety, Women’s Alcohol
and Drug Outpatient Services, services that provide specialist alcohol, drug or
smoking cessation programs, and community women’s refuges.
4. Provider Training
A short summary of the approach to training service providers (also provided
in the Orientation Materials Toolkit)
Pēpi-Pod® Program Orientation workshops were conducted with each
participating service, usually face to face, but also by Zoom or
Videoconference. Key content included safety briefings and ‘Rules of
protection’ which was consistent with the current Pēpi-Pod® Materials Toolkit
(Cowan, 2015), which had been adapted for use by Indigenous health
professionals and the families they care for. All health care providers who had
a current role in the provision of safe infant sleeping information to families
with young babies in these services had the opportunity to participate in the
initial workshops. Key content included:
• Safe Infant Sleeping recommendations
• Infant settling strategies and potential role of Pēpi-Pod®
• ABC responsibilities of distributors:
1. Assemble the Pēpi-Pod®
Confirm the referral meets criteria.
Take a pod, mattress, bedding package
Note the Pod ID number
Note ID on Distribution Record and Feedback Forms.
2. Brief the parent on safe use of the Pēpi-Pod®
WHY: Why we are providing Pēpi-Pod® sleep spaces
Who are the babies more vulnerable to accidental suffocation
12 How babies get oxygen, are different from adults, can suffocate
WHAT: What are its safety features and how to make up the pod
WHERE: Where must the Pēpi-Pod® sleep space be placed
Settling skills and how the Pēpi-Pod® sleep space can help
Where a Pēpi-Pod® sleep space must always be used
SUMMARY: Principles of protection for babies in Pēpi-Pod®
sleep space
Practical demonstrations: making up Pod and simulated parent
education and safety briefing and ‘Through the Tubes’ education
tool.
3. Complete the Paperwork.
Check you have transferred the sleep space ID
to all relevant forms.
Take the Distribution Record. Ask the recipient to fill out contact,
family and baby details. Complete pod details and planned date for
6-8 weeks follow-up.
Make follow‐up and feedback contacts as planned and record
answers to questions. Data forms to be kept with patient records.
Enter information from paper to online forms at USC link and/or
www.pepipod.co.nz (Cowan, 2015) following 6-8-week follow-up.
Additional safe sleeping educational support and resources for all staff who
participated was available through the Aboriginal and Torres Strait Islander
Safe Infant Sleeping (ISIS) eLearning program (Queensland Health & SIDS
and Kids, 2015). This program went live in April 2012 (available free via
internet access from http://www.sdc.qld.edu.au/courses/index) and was based
on the original Safe Infant Sleeping eLearning program launched in May
2010, which was developed to underpin the Queensland Health Safe Infant
Sleeping policy (Queensland Health, 2013). The current Queensland
government Safe Sleeping guideline was due to be updated in 2015; this has
13been brought to the attention of the Deputy Director General for Health. Red Nose is currently working with the NHMRC to develop a national Safe Sleeping Guideline (Professor Young is a member of the Red Nose NHMRC Safe Sleeping guidelines committee) and the Queensland Paediatric Quality Council has established a working group to commence update of the Queensland Health’s Safe Infant Sleeping, Co-sleeping and Bedsharing Guideline (Queensland Health, 2013). 5. Recommendations for risk mitigation in future programs The Pēpi-Pod® Program comprises three key elements essential to the integrity of the program and should continue in any service implementation (space, education, family commitment) The Safety Briefing which is embossed into the base on the Pēpi-Pod® and which is reinforced as part of parent and family education, is a core Program component and risk mitigation strategy. To date there have been no incidents reported that have related to the Pēpi- Pod® when it has been used as advised and in accordance with the safety briefing. Issues that have been identified have been potential problems associated with use of the Pēpi-Pod® around other young children, which were anticipated and addressed in the safety briefing [i.e. care with Pēpi- Pod® placement when other young children are around who could pull down or tip over the Pēpi-Pod® from a raised surface]. No adverse events have been reported. The provision of the Pēpi-Pod® sleep space being contingent on the provision of Safe Sleep education means that participants, even if they decide that the Pēpi-Pod® does not suit their situation, are still receiving dedicated one-on- one information on how to provide a safe sleep environment for their baby. Ultimately the goal is for parents to be able to provide a safe sleep environment for their baby every sleep, with or without the Pēpi-Pod®, and includes when the baby transitions from a Pēpi-Pod® to a cot or other sleep space. Evidence from the Queensland Pēpi-Pod® Trial demonstrated that participants were translating safe sleep information learnt through the Program into other sleep environments (Watson, 2018). In summary, the data reported indicates that families and carers are taking up safe sleep messages 14
in that they are positioning their baby supine to sleep (94%), utilising the Pēpi- Pod® usually or always (>70%) in the context of known risk factors; are room sharing (>90%) and creating safe sleep environments (>90%), and that families and carers are valuing the Pēpi-Pod® as indicated by their wish to retain/keep the Pēpi-Pod® for use with current or subsequent babies (>90%). Key features of the oral safety briefing that is provided to parents and families are also physically embossed into the base of the Pēpi-Pod® sleep space. This was suggested by participants in earlier Program trials and was a positive addition for Queensland service sites. With Pēpi-Pods® being passed on to other families for use, the concern was that the safety messages would be lost, however, evidence from the Queensland Pēpi-Pod® Program demonstrated that participants who shared their Pēpi-Pod® with family and other community members, were also passing on the safe sleep messages to the new family. The embossed messages served as a reminder for Pēpi- Pod® users of the safety briefing and key safe sleeping messages. Evaluation of Pēpi-Pod® Program with key outcome being infant mortality rates In order to discern the influence of the Pēpi-Pod® Program as they have in New Zealand, it would be important to consider infant mortality data both pre- and post program implementation, with a consideration for geographical location level data comparisons. An opportunity to evaluate Pēpi-Pod® Program impact on infant mortality rates in Queensland has been secured through the Queensland Paediatric Quality Council and will commence in 2019, comparing regional infant mortality rates across areas that have, or have not yet engaged in or been offered the opportunity to participate in, the Program. For future states and territories which embark on the program, there is an opportunity to more closely monitor impact on infant mortality rates through various research designs across 3-5-year periods, including cluster randomised controlled designs which would allow for a staged approach in implementation. Such an approach was beyond the current funding and timeline available in Queensland given it was a test of concept trial in the first instance and finalisation of infant mortality data collection in Queensland is frequently a 2-3-year process. Realistically, true infant mortality trends can 15
only be identified over 3-5-year periods, given the nature and duration of infant death investigations prior to infant death classifications being finalised for reporting. Now that the program has been in place in some areas for up to 4 years, it may be possible to begin to identify trends in infant mortality in Program active areas. Establish memorandums of understanding with participating organisations (similar to NZ model) to ensure: integrity of core components including delivery of safety briefing and provision of monitoring data Locally, ongoing measures and support are necessary to ensure accurate and near complete data collection and return relating to Program distribution and participant feedback, which also assists in monitoring that the Program continues to be delivered as intended for families with vulnerabilities. Development of Memorandums of Understanding with service sites would be recommended as a way of establishing mutually agreeable and achievable parameters for data return within the resources of participating organisations, as has been established in New Zealand between District Health Boards and Change for our Children, Ltd. 6. Pēpi-Pod® distribution with participating services The order for 600 Pēpi-Pod’s® was made with Change for our Children New Zealand on the 1st June 2017. From the 1st August 2017 and as at the 30th June 2018 all 600 Pēpi-Pods® had been distributed to participating maternal and child health services which provide care for Aboriginal and Torres Strait Islander families. Table 1 provides Distribution information as per location, service provider and number of Pēpi-Pods® provided. Priority areas for Pēpi-Pod® distribution Priority areas agreed by USC and the former Department of Communities, Child Safety and Disability [now DCSYW], in conjunction with Qld Health include: Mt Isa; Toowoomba and surrounding districts including residents of Cherbourg; Moreton Bay including Caboolture and Deception Bay; Townsville 16
and surrounding districts (including Palm Island); Cape York and the Torres
Strait Island, and Gold Coast and Logan district including Stradbroke Island.
Table 1 identifies the location, name and number of Pods provided to each
participating service during the funded period.
Table 1: Distribution of Pēpi-Pod’s® July 2017- June 2018.
Priority Area Service Pods
Provided
Mt Isa / Mornington Island North West HHS Qld Health MCH 50
RFDS Doomadgee 10
RFDS Mornington Island 10
Toowoomba/Cherbourg Goolburri, Toowoomba 20
Intensive Family Support Service Uniting Care 5
Cherbourg 10
Carbal, Toowoomba 5
Carbal, Warwick 10
Boomagan Caring, Toowoomba BH 5
Act for Kids, Toowoomba 5
Warwick Warwick Child Health 10
Tara Save the Children 10
Moreton Bay Ngarrama Redcliffe 15
(incl Caboolture & Deception Bay) Ngarrama Caboolture 10
Ngarrama RBWH 15
IUIH Strathpine (Caboolture/Deception Bay) 40
IUIH Woolloongabba 10
IUIH Salisbury (south Brisbane) 25
IUIH Wynnum 10
IUIH Capalaba 5
Townsville (incl Palm Island) TAIHS Townsville 20
TAIHS Palm Island 10
Cape York TSI Wuchopperen (Cairns) 35
Gurriny Yealamucka Yarrabah 5
Apunipima (Lockhart River, Hopevale, Laura, 45
Wujal Wujal)
Apunipima Aurukun 20
Apunipima Kowanyama 20
Apunipima Pormpuraaw 15
Apunipima Coen 10
Apunipima Mossman 15
Apunipima Napranum 20
Cairns and Hinterland Apunipima Cairns 10
Gold Coast & Logan IUIH Kalwun 5
(incl Stradbroke Island) Southern Qld Centre of Excellence in Aboriginal 10
& Torres Strait Islander PHC, Inala (QH)
Logan Maternity, QH 50
Kyogle Community Centre (Serving Gold Coast) 10
Sunshine Coast Direct referrals 10
NCACCH, Maroochydore 10
Total 600
17Process for assessment and collection of data relating to family vulnerabilities Data collection was scheduled to occur at the time of recruitment (1-page risk assessment conducted during the antenatal or postnatal period) and at baby age of 6-8 weeks (1-page data collection relating to safe sleep education). Identifiable data (collected with consent, family information and page 1 risk assessment) is required to enable follow-up at 6-8 weeks and is retained by the service. The follow-up is scheduled to coincide with the service visit for the postnatal check, baby check and/or immunisation to assist efficient care delivery. When both pages of the 2-page form are completed, de-identified data is then entered into the electronic database via the electronic link or sent to Chief Investigator for data entry. A detailed summary of data entered by services up until July 2018 has been provided here relating to risk factors and use of the Pod. Some missing data is apparent from incomplete data entry by staff members particularly where families may have been lost to follow-up due to disengagement with a voluntary maternal and child health service. Relevant program development activities completed relating to provision of this family information A joint ANZ data collection form has been established to ensure consistent data collection into the future that will be used to determine priority identification of families with identified needs and program integrity (i.e. delivery of the safety briefing with the Pēpi-Pod® Program dissemination through various services). This data form is included with each Pēpi-Pod® bedding pack and provides a unique identifier which allows tracking of Pēpi-Pod’s® to services and the geographical region of the family, while capturing de-identified data from families. The services may, and are encouraged to, continue to maintain their own records. 18
Data form variables captured include: antenatal and postnatal smoking, prematurity, low birth weight, Indigenous status, antenatal care engagement, maternal age, availability of a baby bed (at recruitment), and Pēpi-pod® usage and safe sleeping recommendation uptake (at 6-8 weeks). The streamlined data form has been made available via an electronic link. This can be sourced at: https://changeforourchildrennz.sites.acclipse.com/pepi_pod_programme/data _record_nzau and is linked to the USC Hub: http://www.usc.edu.au/research-and-innovation/medical-and-health- science/nurture/research-projects/the-pepi-pod-program. These links were made available to all sites via the Program documentation (and Orientation briefings). Please see Appendix 1 for Information provided via the Pēpi-Pod® Program Service Provider Support Page (available on the Change for our Children Website and USC Hub). Regular email communication with services to ensure awareness of electronic data entry has occurred to encourage data return due to low data collection/response rates captured in the on-line system as of September 2017. Refresher workshops for existing participant services and Orientation workshops for new services are provided which include the Toolkit, data collection requirements and communication strategies. A Newsletter has been re-established to increase presence and awareness and links to, data collection processes (Distributed 1st March 2018). Table 2 identifies the Hospital Health Service region where agencies operate, the agency and the number of families (n=158) whose data has been entered into the online database for each agency and region to date (as of 20th July 2018). 19
Table 2: Services returning Pēpi-Pod® Program respondent data
(July 2017- 20th July 2018, n=158)
QLD Area (HHS) Agency Number /agency Total in HHS
n %
Cairns & Hinterland Child Safety 1
Gurriny Yealamucka Health 11
Service
19 12%
Wuchopperan Health Service 7
Children’s Health University of the Sunshine Coast 1 1 0.6%
Queensland
Darling Downs Institute for Indigenous Health 2
Cherbourg 3 5 3.2%
Gold Coast Kalwun Health Service 2
Aboriginal Maternal and Infant 3 5 3.2%
Health Services Kyogle
Metro North Aboriginal and Torres Strait 2
Islander Health Service
Australian Nurse Family 3
Partnership Program
Institute for Urban Indigenous 6
Health
Ngarrama Family Community 11 22 13.9%
Service
Metro South Australian Nurse Family 3
Partnership Program
Birthing in Our Community 3
Institute for Urban Indigenous 5
Health
Logan Hospital 29
Southern QLD Centre for 1
Excellence in ATSI Primary Health
Care
Yulu Burri Ba Aboriginal 1
Corporation for Community Health
Manly 4 46 29.1%
North West Maternal Child and Youth Health 8
Service
Royal Flying Doctors Service 2
10 6.3%
Sunshine Coast Direct Referral 4
North Coast Aboriginal 4 8 5.1%
Corporation for Community Health
Torres & Cape Apunipima Cape York Health 15
Council
20Queensland Health Thursday 6
Island and Bamaga
21 13.3%
Townsville & Mackay Townsville Aboriginal and Islander 5 5 3.2%
Health Service
West Moreton Institute for Urban Indigenous 1 1 0.6%
Health
West Australia Red Nose 15 15 9.5%
158 100%
Each month, Change for our Children provides the Program team with an
electronic report of data that relates to Program distribution in Australia. As all
sites in Australia and New Zealand are now using the common data form;
some of the data included in this report may be from sites who are providing
the Program to their community that do not form part of the number purchased
by the Department of Child Safety, Youth and Women (DCSYW). The
Queensland Program team has led the educational support of additional
interstate sites as part of other funding initiatives, e.g. Red Nose and
Thursday Island Maternal and Child Health, Queensland Health. All figures
relevant to Australia have been included to provide a collective picture of
participant characteristics and Program acceptability for an Australian
population.
Family Demographics and Risk Factors that increase risk of SUDI
The risk assessment that is conducted at recruitment suggests that the Pēpi-
Pod Program is being delivered to families with identified vulnerabilities, as
intended.
All 600 Pēpi-Pod’s® had been distributed to service organisations by 20th July
2018. There were 158 entries (26.3%) in the electronic database by service
providers as at this date, of the 600 pods that were distributed. From this data
the median age of the mothers entering the Program was 24 years (range 15-
30 years; mode 30). Over one quarter of mothers had presented for antenatal
care after 20 weeks gestation (27.9%). Smoking before and during pregnancy
(60.4% & 56.7% respectively) and rates of household smoking (73.2%) were
high compared to the broader population of Queensland women who are
reported to smoke. Parental drug and/or alcohol use, noted to be problematic
particularly in terms of the associated high risk of infant mortality, was high
21compared to the general population (30.1%). Other infant vulnerabilities that
were noted included previous infant loss, maternal mental health history,
overcrowding, reduced social support and infant welfare issues. Only 57 of the
149 (38.3%) who had a response recorded in the database for the relevant
question, were reported to have a dedicated baby bed prior to being provided
with a Pēpi-Pod®. Despite the relatively low data capture, this data
demonstrates that the service providers are continuing to identify and deliver
the Pēpi-Pod’s® to families with identified risk factors which place their infant
at a higher risk of SUDI. Table 3 details the demographics and eligibility
criteria for families who received the Pēpi-Pod® Program.
Table 3: Demographic characteristics of the sample (n=158) entered into
databases (as of 20th July 2018).
N %
(in years)
Maternal AgePēpi-Pod Use
All families who received a Pēpi-Pod® also were provided with a safety
briefing, be that using a safety briefing picture card (152, 96.2%) or through a
didactic information session (6, 3.8%). Of the 158 families, follow-up was
completed for 123 families (77.8%). Of families, 39 (32%) had used the Pēpi-
Pod® for few or no sleeps in past week; 30 (24.6%) for some sleeps; 53
(43.4%) had used the Pēpi-Pod® for most or all sleeps for their baby. Babies
who were no longer using the Pēpi-Pod® or were placed in pod only
sometimes, were more likely to be older infants, aged older than 8 weeks.
Tables 4 & 5 illustrate how families used the Pēpi-Pod® and how they
perceived that the Program facilitated safe sleep.
Participants were asked to rate how the Pēpi-Pod® had supported them on
five different aspects of care using a scale from 1 being the lowest to 9 being
the highest, e.g. how well has the Pēpi-Pod® supported you with safety
(scores of six or greater were collated as strongly positive responses to the
question being asked).
Sleep for Mother
Most participants (98, 84.5% of those that responded) scored 6 or higher in
relation to the Pēpi-Pod® allowing them to sleep better. This was supported
by written comments made by participants including:
“Really useful, was able to take it with me to visit family; I felt baby was
safe in this when I had it in bed next to me. Sometimes I sleep heavily
so I had piece of mind”. P97.
Peace of mind for the carer while bed sharing was a common theme in the
written comments.
“The use of the Pēpi-Pod and education gave us peace of mind as the
baby shares a mattress on the floor with both of us and his sisters and
brother (3 other siblings)”. P153.
23Table 4: Safe sleeping practices
n %
Follow-up Yes 123 77.8
Infant age at follow-up (n=123) 0-4 wks. 14 11.4
5-8 wks. 65 52.8
>8 wks. 44 35.8
Slept in past week (n=122) Most sleeps 39 32
Some sleeps 30 24.6
Few or no sleeps 53 43.4
Would you like to keep Yes, for this baby 83 68
Pēpi-Pod®? (n=122) Yes, for next baby, share 30 24.6
with others
No please take it back 9 7.4
People spoke with about 0 14 11.5
safe sleep for babies (n=122) 1-5 68 55.7
6-10 40 32.8
Does baby sleep on back (n=122) Always 94 77.1
Usually 21 17.2
Sometimes 6 5
Never 1 0.7
Do you do a safety check to Always 110 90.9
Remove all pillows, toys, hats, Usually 9 7.4
Loose or soft items, when Sometimes 2 1.7
Baby goes to sleep? (n=121) Never 0 0
Does baby room-share with Always 113 93.4
parent? (n=121) Usually 4 3.3
Sometimes 3 2.5
Never 1 0.8
Is baby in Pēpi-Pod® when Always 59 48.7
Sleeping in or on adult bed, Usually 26 21.5
couch, makeshift bed? (n=xx) Sometimes 22 18.2
Never 14 11.6
24Table 5: Safe sleeping practices
n %
Current breastfeeding (n=122) Exclusively/fully 62 50.8
Partially 21 17.2
Sometimes 14 11.5
Not at all 15 12.3
Never 10 8.2
breastfed
Is carer receiving smoking Yes 33 27.3
Cessation support (n=121) No 39 32.2
Smoke-free 49 40.5
Scored 1-9 (9 being highest)
Has Pēpi-Pod® helped with:
Safety (n=118) Score 6-9 103 87.3
Better sleep for mother (n=116) Score 6-9 98 84.5
Convenience (n=116) Score 6-9 98 84.5
Settling (n=115) Score 6-9 82 71.3
Breastfeeding (n=108) Score 6-9 65 60.2
Breastfeeding
There were 65 (60.2% of those that responded) participants who scored the
Pēpi-Pod® as 6 or higher in relation to support for breastfeeding. One
participant identified:
“I still often bedshare in my single bed with baby as I breastfeed. Baby
did not have a bed before the Pēpi-Pod - too crowded with 5 adults and
2 other children”. P36.
“For first 6 weeks it was great but then baby was feeding lots and I
brought baby into bed and he settled better”. P37.
Convenience
There were 98 (84.5% of those that responded to the question) participants
who rated the Pēpi-Pod® as 6 or higher for convenience. Written comments
relating to this aspect of use included:
25“Our experience with the Pēpi-pod is positive and convenient for us.
I’ve been recommending it to others that think about having a baby or if
they are having a baby”. P74.
“Easier during the night. Didn't have to get up and check cot”. P48.
“I love it. It’s been the best thing for us”. P79.
Safety
Most participants (103/118, 87.3%) scored the Pēpi-Pod® 6 or higher for
safety.
“I feel the baby one is much safer when he is next to me, as I sleep
very heavily and the other children climb into my bed during the night”.
P32.
“It was great for the first 2 months especially. I would put baby down for
a nap where the sun would shine through the window and he would
also be happy to just look outside. I could take him in the Pēpi-Pod
wherever I went in the house and felt assured he was safe in it”. P103.
There have been no injuries reported during this or the original Pēpi-Pod
Program, however in three cases [out of feedback from 563 parents] parents
reported that their baby would wave their arms and bang them on the side of
the Pod. This was the reason that Pod use ceased for those participants.
“It was great straight away baby settled, as she grew she would bang
her arms on the side”. P89.
Occasionally parents have identified that they have felt their infant too cold in
the Pēpi-Pod® and preferred to bed-share for this reason.
“Mum stated baby was getting cold in the Pēpi-Pod. Would have been
ok if had been given at birth, but baby for 2 weeks got used to warmth
of mum and struggled to settle in pod.” P55.
A merino wool blanket is included in the Pēpi-Pod® bedding pack. This is light
however serves as an effective and warm insulator; in tandem with
appropriate clothing for the season the blanket should provide adequate
warmth for baby.
26The need to position the Pēpi-Pod® on a flat stable surface out of reach of
other children, along with how to make the Pod up with the bed linen for infant
sleep are instructions that are included in the safety briefing.
Settling
Out of the 115 participants who rated the Pēpi-Pod® for settling, a total of 82
(71.3%) gave a score of 6 or higher. Comments supporting the use of the Pod
for infant settling include:
“Our bed is a mattress on the floor which we share with our other kids
(2 adults, 3 siblings and baby) but now we put baby in the Pēpi-Pod
beside our mattress. Baby would have slept in our bed if we didn't have
the Pēpi-Pod. The Pēpi-Pod is very convenient when we stay at our
cousin's place. Our baby settles well in the Pod, and we feel it is very
safe and convenient to use”. P152.
“Love it, very useful. Baby unsettled so helped a lot”. P102.
Comments made by Program participants give insights into how Pēpi-Pod®
use evolved with baby’s growth and development:
“The Pēpi-Pod was awesome. We used it most sleeps during first 12
weeks - in our room and all around the house, wherever we were. As
he grew he started to try to turn over around 12 weeks so we started
using the cot and only used the Pēpi-Pod when he was in the same
room as us for day time sleeps where we could watch him”. P83.
“When baby grew out of pod around 13 weeks it was perfect to store
under change table with nappies and wash cloths; want to keep for my
next baby”. P16.
“Baby is now 4 months, getting too big for Pod. I'm her aunty. She is
sleeping back in with me in my bed now (mattress on the floor) this
week but last week I still used the pod for some night time sleeps. She
would have slept in with me if I didn't have the Pēpi-Pod. It is easier to
travel with than a cot. I bring her into bed when she needs settling. I am
more aware of safe sleeping and don't have pillows around her
anymore”. P147.
27Several participants found the Pēpi-Pod® too big for the parent’s bed, or too
hard to sleep next to. These parents also received safe sleep education and
were more aware of how to provide a safe sleep environment for their baby
even if the Pēpi-Pod® did not suit their situation and they chose not to use it.
Perhaps the most simply put message from one of the Program participants is
most apt to complete this section of the results.
“We sleep with our babies, this Pēpi-pod helps us to do it more safely”.
P95.
Interaction between smoking and bedsharing
We know that the effects that smoking during pregnancy and during early
infancy has on the developing fetus are extensive and profound and can
contribute to a number of different vulnerabilities in an infant. Shared sleep
with a smoker has been reported to increase the odds of infant death up to ten
times (Blair et al., 2014; Carpenter et al., 2013). Babies who have been
exposed to cigarette smoking during pregnancy are reported to have a
reduced response to a hypoxic episode, which may contribute to their
vulnerability to SUDI especially if they are placed in a sleeping environment
that may obstruct or compromise their airway. Most recently, a three-year
case-controlled study in New Zealand reported that infants born to mothers
who smoked during pregnancy were at six times the risk of a SUDI mortality
(Mitchell et al., 2017). Passive exposure to environmental tobacco smoke,
such as household smoking, has been identified as an independent risk factor
for SUDI including SIDS (Liebrechts-Akkermann et al., 2011). In Queensland,
67.7% of SUDI deaths in 2013 occurred in the presence of maternal and/or
household smoking (Queensland Family and Child Commission, 2018, p. 73).
Family participants who took part in the Pēpi-Pod® Program reported a very
high rate of both maternal and household smoking (56.7 % and 73.2%
respectively). Smoking cessation is difficult and smoking behaviours cannot
be changed overnight. With the provision of a sleep space for families’, infants
who may be more vulnerable due to smoke exposure can be protected from
additional challenges, particularly those associated with unsafe sleep
28environments that may increase the risk of infant airway compromise. While intention to bedshare was not a question asked on the online data forms, results from the original Pēpi-Pod® Program demonstrated that over 80% of participant families were bringing baby into the bed, and 71% of babies were reported to be sharing sleep with a smoker. Of this number 57% of these babies were placed in a Pēpi-Pod®, thereby reducing the risk associated with direct bed-sharing. It is in this way that the Pēpi-Pod Program® is breaking the smoking-bed-sharing relationship and reducing risk on any given sleep. Please see Table 6 (original study . Table 6: Interaction between Usual Bed-sharing and Infant Smoke Exposure Of the participants who did not have a baby bed at the time of recruitment, 90 (97.8%) provided details of maternal or household smoking. Intention to bed share was not explored with this participant group. From the data we can see that over 80% of infants who did not have a baby bed had the potential to be smoke exposed in their home environment. This does not take into consideration those families who did have a baby bed but for whom bedsharing was practised. Please see Table 7. 29
Table 7: No Baby bed and maternal or household smoking.
Bedsharing and Smoke Exposure (n=90)
Non- Maternal Household Any potential
Smoking Smoking smoking smoke
exposure
No baby bed at 16(17.8%) 57 (63.3%) 70 (77.8%) 75 (83.3%)
time of recruitment
7. Program Orientation - service participation
Information on attendance levels at the education sessions including the
workplace and role descriptions of the attendees was collected and will be
reported here.
Five workshops were agreed as part of the funding arrangement with
Department of Communities, Child Safety and Disability at the
commencement of the project. A total of 32 education sessions and Pēpi-
Pod® Program Orientation Competency Workshops have been conducted
during the period April 2017-May 2018 due to service requests. Please see
Table 3.
Existing services have been orientated to the new data collection process as
the Program transitions from research to service integration and new services
have participated in a Pēpi-Pod® Program Orientation and Competency
Workshop (usually 2-3 hours). Please see Appendix B for a detailed list of
services, dates, workshop locations and contact personnel. Detailed lists of
staff participants are recorded to ensure provision of Safe Sleep Champion list
back to service and to provide a Certificate of Completion for participants.
Participants to date include: nurses, midwives, paediatricians, maternal and
child health nurses, Indigenous Health Workers, and Child Safety Support
Officers. Certificates of completion have been provided to staff attending
these Orientation workshops. Table 8 provides details of the number of
workshops provided to agencies who joined with the Pēpi-Pod® Program.
30Table 8: Service Orientation Workshops: New service orientation and Existing service orientation to new documentation 31
8. Distributer Survey Results
In late July (27 July 2018) an online survey was sent to all Pēpi-Pod®
Program providers. The aim of this survey was to gain feedback about the
Program from the Health Professionals who were providing it to their
communities during the funded period 2017-2018. The survey specifically
asked for feedback relating to how much value they felt their families, and
they themselves, placed on the Pēpi-Pod® Program as a health promotion
tool.
Table 9 and 10 detail the responses to date for this survey.
This survey will remain open until October and an update of responses can be
sent on request.
Table 9: Health professional feedback: Program use and integration
Question Yes No
n (%)
Are you involved in providing 9 (100%) 0
Pēpi-Pod® Program within service
Role (n=8)
Manager 1 (12.5%)
Midwife 2 (25%)
Maternal and Child Health Nurse 2 (25%)
Indigenous Health Worker 2 (25%)
Other 1 (12.5%)
Yes No Unsure
Would your service fund Program 5 (55.6%) 0 4 (44.4%)
if not available through QH/ USC?
Has your service integrated 9 (100%) 0 0
Program into model of care?
32You can also read