The National Pharmaceutical Strategy 2016-2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The National Pharmaceutical Strategy 2016–2018

Contents
National Pharmaceutical Strategy 7. Strategy for whom?.......................15 2.4. F
ollow-up of medicines in collab-
for better use of medicines............. 3 oration between government
8. Organisation...................................16 agencies and healthcare............32
1. Why a national
pharmaceutical strategy?................ 4 9. How do we measure whether Objectives area 3
development is moving in the Economically and environmentally
2. What has the national direction of the objectives?...........17 sustainable use of medicines.......34
pharmaceutical strategy Implementation of the National 3.1. E
valuation of existing anti-
contributed to?...................................... 5 Pharmaceutical Strategy....................17 biotics for best possible use......34
3.2. Models for availability and
3. What are the great challenges Action plan 2016.................................20 responsible use of both new
in the short and long terms?........... 6 and old antibiotics of
Equal and patient-centred Objectives area 1 particular value.............................34
healthcare ................................................ 6 Effective and safe use of 3.3. E ndeavour to make it possible
Ethical challenges .................................. 6 medication............................................22 for consideration to be given
Patient groups in which use of 1.1. S
afer management of to environmental aspects in
medicines poses special risks............. 7 medicines for children.................22 the production and use of
Trend in costs .......................................... 8 1.2. V aluation of treatment efficacy medicines........................................35
Availability of medicines........................ 8 in everyday clinical practice.......22 3.4. E nvironmental assessment
E-health .................................................... 9 1.3. S tructure for documentation of non-prescription medicinal
Knowledge-based and innovative and follow-up.................................23 products..........................................36
development and promotion of 1.4. National medication list..............24 3.5. M anagement of primary-care
life science ................................................ 9 1.5. P revent prescribing of medi- medicines not included in
Long-term skills supply ......................10 cines contrary to scientific the pharmaceutical benefits
Environment..........................................10 and proven experience...............24 scheme ...........................................36
Improved follow-up of medicines....10 1.6. M ake electronic reporting
Antibiotic resistance............................10 of side effects possible................26 Further proposals being pre-
How are the challenges 1.7. Improved follow-up of pared for new activities..................39
addressed?.............................................11 pharmaceutical dosing................26 1. Shelf lives of medicines...................39
1.8. E fforts to improve patient 2. S
elf-medication with focus on
4. The vision for the national safety in generic substitution....27 non-prescription medicines.........39
pharmaceutical strategy................12 1.9. S tructured discussions on 3. C larification of the position
medication in pharmacies..........28 of regulatory approval in public
5. Objectives of the knowledge management...............39
pharmaceutical strategy................13 Objectives area 2 4. Improved use of medicines for
Effective and safe use of Accessible medicines and vulnerable groups of patients –
medicines................................................13 equal use...............................................30 the elderly and medicines.............39
Accessible medicines and 2.1. National collaboration for develop- 5. Orderly phase-out of
equal use.................................................13 ment of adaptive licensing of medicines at society level..............40
Economically and environmentally new medicines...............................30
sustainable use of medicines............13 2.2. M onitor and evaluate the Completed activities
benefit of work aimed at man- monitored under the national
6. The three perspectives of the aged national introduction of pharmaceutical strategy................41
pharmaceutical strategy................14 new medicines...............................30 Knowledge support in prescribing
2.3. Greater quality and safety medication for children......................41
at pharmacies................................32 Reason for prescribing........................41
2 The National Pharmaceutical Strategy 2016–2018
National Pharmaceutical Strategy
for better use of medicines
The Government and the Swedish there is cooperation with initiatives in
Association of Local Authorities and these areas, as well as permeating all
Regions, together with a broad set of activity under the NPS so that they
pharmaceutical actors, have agreed contribute to safe, effective and equal
to continue to build on and enhance use of medicines.
the work that has been in progress
for several years under the National As a result of the long-term collabo-
Pharmaceutical Strategy (NPS). ration platform the NPS has created
There is a consensus that the complex between the most important actors in
challenges that exist in the pharma- the pharmaceutical field, it is possible
ceutical field must be addressed jointly to bring about real improvements and
and that both a long-term and a short- attain the strategy’s long-term vision
term approach must be adopted in of Correct use of medicines to the benefit of
addressing these shortcomings. patient and society.
The strategy part of the NPS there-
fore extends over the period 2016–
2018, while the action plan is revised Gabriel Wikström
annually. As the pharmaceutical field Minister for Health Care,
has interfaces with other important Public Health and Sport
strategies and initiatives, there is also
a need for close cooperation with these Lena Micko
activities. The three perspectives in Chair, Swedish Association
the strategy – patient, innovation and of Local Authorities and Regions
e-health – have to guarantee that
The National Pharmaceutical Strategy 2016–2018 3
1. Why a national
pharmaceutical strategy?
Medicines provide great opportuni- The challenges require collaboration
ties to cure and alleviate disease, but between different parties and a strate-
also pose a number of challenges that gic approach. Since 2011 there has
must be addressed in both the short been a national pharmaceutical stra-
and long terms. One challenge is to tegy and associated action plan, aimed
make equal access to medicines pos- at addressing the challenges in the
sible for the whole population, based pharmaceutical field in both the short
on the needs of the individual person. and long terms and promoting correct
Another is to ensure environmentally use of medication. This work encom-
sustainable use of medicines. The use passes almost the entire value chain
of medicines must also be effective of medicines: from research and inno-
and safe, while the relationship be- vation to follow-up of effects in every-
tween costs of medicines and efficacy day clinical practice.
of treatment must be reasonable. The
objectively ultimately is to use med- There is a broad consensus among the
icines in as cost-effective a way as parties and stakeholders involved in
possible so that the greatest possible the strategy that intensified and last-
health can be achieved for the re- ing cooperation is required so that
sources allocated to healthcare. specific and systematic improvement
Research and development of new measures can be implemented in the
medicines is also of great significance pharmaceutical area and benefit pati-
in ensuring that we will continue to ents, the healthcare system and society.
have access to adequate treatment of The national pharmaceutical strategy
diseases and injuries in the future. is a necessary collaboration platform
on which to put this into effect.
4 The National Pharmaceutical Strategy 2016–2018
2. What has the national
pharmaceutical strategy
contributed to?
The strategy has contributed to estab- More than half of around 40 activi- Further activities that have been com-
lishing a national collaborative proce- ties in the strategy’s previous action pleted in the national pharmaceutical
dure with a clear work process. It has plans have been completed.1 Some strategy and that have contributed to
also meant that the parties involved activities have been particularly better use of medicines are the online
– the Government and the Swedish valuable as they have contributed to pharmaceutical training programmes
Association of Local Authorities and practical improvements in the area of that have been developed for home
Regions – as well as other stakehold- medicines. Examples of these are ef- help staff and doctors. In addition,
ers, the Medical Products Agency, the forts to improve pharmaceutical treat- the working group for environmental
National Board of Health and Welfare, ment of children, where the strategy indicators under the national pharma-
the Swedish Council on Health Tech- has contributed towards paediatric ceutical strategy has reported its work
nology Assessment and Assessment medicine having come closer to the on the “measurement of levels of
of Social Services, the Swedish introduction of national knowledge pharmaceuticals in the environment”.
E-health Agency, the Health and support for prescribing medication The working group has submitted
Social Care Inspectorate, the Dental for children. In addition, needs for proposals on 22 pharmaceutical
and Pharmaceutical Benefits Agency, knowledge with regard to the pharma- substances whose presence in the
the Public Health Agency of Sweden, ceutical treatment of children have aquatic environment it is relevant to
county councils, the Swedish Associ- been identified together with paediat- monitor. These substances include
ation of Health Professionals, the ric medicine, and knowledge in this anti-inflammatories, antibiotics and
Swedish Medical Association, the area has been enhanced through the endocrine disrupting substances.
Association of the Pharmaceutical preparation of, for example, treat-
Industry in Sweden and the Swedish ment recommendations.
Pharmacy Association have agreed
on what efforts must be prioritised in The process of bringing about nation-
the area of medicines to enable the al managed introduction of new pha-
vision to be put into effect. This applies rmaceutical treatments has also been
to what objectives are to be attained, pursued under the strategy. This has
what activities are to be carried out contributed, among other things, to
and how the work is to be followed Sweden being the fastest internation-
up and evaluated. Cooperation also ally to introduce new medicines for
increases knowledge and understand- hepatitis C. The effects of this work
ing of what needs exist, contributes are being evaluated at present, with
to coordinating development activity the objective of obtaining knowledge
that takes place in government agen- on whether the process has addition-
cies, county councils and organisa- ally contributed to more equal pharma-
tions and increases the interfaces for ceutical treatment.
cooperation with other initiatives
and strategies.
1
lv.se/nls
The National Pharmaceutical Strategy 2016–2018 53. What are the great challenges in
the short and long terms?
The greatest challenges for the pharma- of care actions by several different rities in healthcare) which has three
ceutical area are disparate and exist parties is also of key significance. guiding principles: the principle of
throughout the life cycle of medicines. human dignity, the principle of need
The national pharmaceutical strategy Equal care also means equal access to and solidarity and the principle of
includes activities that are to contrib- pharmaceutical treatment. One of the cost-effectiveness. The principle of
ute within a relatively foreseeable per- challenges in this area is that respon- human dignity means that everyone
iod of time to solving the problems sibility is largely shared between coun- is of equal value and has the right to
and to tackling the challenges that exist. ty councils, which may have differing care on equal terms regardless of age,
At the same time, the strategy contains priorities. Another is the way in which gender, education and social or eco-
a long-term perspective aimed at plan- the costs are to be borne in continued nomic status. In order to be able to
ning to meet future challenges. It is prin- development that provides access to prioritise on the basis of the principle
cipally initiatives requiring collabora- new, effective, but also expensive med- of human dignity, there is a need to
tion between several parties or stake- icines and more prescription medicines acquire greater knowledge and illu-
holders in the pharmaceutical area that are not covered by the pharma- strate gender-related challenges, for
that fall under the national pharma- ceutical benefits system. Equal access example, in healthcare. The principle
ceutical strategy. Some of the areas that to medicines is probably also fostered of human dignity is an overarching
require special efforts – within or out- by a pharmacy market with high avail- principle that can be said to represent
side the work on the national pharma- ability and good service throughout a framework within which decisions
ceutical strategy – are described below. the country. Pharmaceutical treatment on priority must always be made. The
that is patient-centred is also depend- other two principles are less absolute,
Equal and patient-centred ent on access to good and readily avail- in the sense that a balance should be
healthcare able information for the individual on struck between them. While the prin-
There are differences in health between medicines and how they are to be used. ciple of cost-effectiveness is concerned
different groups in society, for example with the amount of health benefit
between socio-economic groups, geo- Ethical challenges created per SEK invested, the prin-
graphical areas and genders. Equal, Priorities in healthcare in Sweden are ciple of need and solidarity indicates
accessible and patient-centred health- a key issue with ethical dimensions. that the health benefit created has to
care is an important factor in attaining It is the individual medical needs and be distributed on the basis of solidari-
greater equality in health. The care not the patient’s ability to pay or other ty, which means that priority is given
that is offered is, as far as possible, to external factors that are to dictate what to the greater need ahead of the lesser
be designed on the basis of the indi- care is to be offered. need. It is thus incompatible with the
vidual’s needs and be of equally good principle of human dignity for needs
quality regardless of the patient’s gen- More and more medicines aimed at generally to be given lower priority on
der, country of birth, age and other small groups of patients are now app- the grounds of the patient’s age, birth
similar factors. Equal care does not earing. The way in which these med- weight, lifestyle or economic circum-
always mean that the same care has to icines are managed with regard to stances. On the other hand, it is com-
be offered, but means that everyone assessing the ability of society to pay patible with the ethical principles to
has to be given the same opportunity is therefore becoming an ever more take account in the individual case of
to achieve treatment targets and good important issue. Medicines of this type circumstances that limit the benefit
health. The care also has to be carried are therefore very highly priced in rela- of the medical measures for the patient.
out in consultation with the patient tion to their benefit, which poses a cha-
and with respect for her or his right llenge from the ethical point of view. It is less likely that medicines will be
of self-determination and privacy and, developed to treat uncommon diseas-
with regard to children, in considera- Priorities in healthcare have to follow es than more common ones, and in
tion of age and maturity. Good avail- the ethical platform adopted by the addition it may be more difficult to
ability and functioning coordination Riksdag (Govt Bill 1996/97:60 Prio- carry out research on unusual con-
6 The National Pharmaceutical Strategy 2016–2018ditions because of small patient vol- properly and attention is paid to side
umes. It may therefore be reasonable effects.
for medicines for very uncommon and
severe conditions to be allowed to cost A vulnerable group, which includes
more than medicines for a more com- many elderly people, is that of multi-
mon condition but with the same morbid women and men. They are at
severity. There is, however, no guid- particular risk of being affected by
ance at present on how much such a side effects, both because they take
treatment may cost, making it very many medicines which in each indi-
difficult for the healthcare authorities vidual case can cause side effects
to allocate priorities. and because of the risks that exist
of unsuitable interactions between
Patient groups in which use of medicines. How responsibility for
medicines poses special risks and follow-up of the patient’s use of
There are groups of patients who are medicines is to be organised for these
at greater risk of being affected by un- patients, who may have many different
desirable side effects of pharmaceuti- healthcare contacts, poses a challenge.
cal treatments. These groups include
the elderly, multimorbid patients, The EU Regulation on Medicinal
children and people with mental ill- Products for Paediatric Use, the objec-
health. tive of which is to improve the health
of children by increasing research on
Among elderly women and men, it can medicines for children, has existed
be noted that physical changes due to since 2007. Pharmaceutical treatment
age and disease lead to greater sensi- of girls and boys is, however, made
tivity to medicines. Concurrent use of more difficult by a lack of medicines
many medicines is common among adapted for children, knowledge gaps
the elderly and poses an increased risk and potential safety problems. Many
of side effects and of medicines inter- present-day medicines are incomple-
acting with each other. For example, tely documented in terms of dosage,
many urgent admissions of elderly efficacy and safety for children. In
patients to hospitals are due to side eff- the absence of scientific documenta-
ects of medicines or lack of efficacy, tion, recommendations on pharma-
and a large proportion of these situ- ceutical treatment of children have to
ations are considered to be preventable. some extent been based on proven
Most side effects are not caused by experience in paediatric medicine.
directly unsuitable medicines but by There is also a shortage with regard
incorrect use of medicines that are to dosage forms and preparations
important in order to treat somatic specially suited to children, increasing
diseases in the elderly. There is there- the risk of incorrect use. The general
fore a need for healthcare providers lack of data on use of medicines in
to take measures aimed at ensuring children may also have contributed to
that the elderly patient receives the under-reporting of side effects in
correct doses, that prescribed med- children. Children may also have a
icines are compatible with each other pattern of side effects that differs
and that the treatment is followed up from that of adults.
The National Pharmaceutical Strategy 2016–2018 7Trend in costs the effects of price caps for older med- cipated. A shortage of medicines can
Pharmaceutical treatment is the most icines and factors of a one-off nature, also arise when companies stop mar-
common medical measure and is an for example decisions on the intro- keting medicines or in cases where
important aspect of healthcare. In rec- duction of medicines free of charge the medicine is not supplied to the
ent years, more than 6.3 million people for children. Swedish market at all.
in Sweden have had prescriptions filled
at pharmacies annually. In addition Many of the challenges for the future When medicines are no longer avail-
there are those patients who have re- are the present-day cost-drivers, bio- able, it poses an evident risk to patient
ceived pharmaceutical treatment in logical medicines, whose patents have safety as treatment may need to be
hospital and those who buy non-pre- expired or will soon expire. An impor- postponed or discontinued. In add-
scription medicines in a pharmacy or tant reason is that biological medicines ition, the situation may mean that the
other retail outlet. Medicines result in are often used for long-term treatment healthcare system, pharmacies and
high costs for central government and in chronic diseases and that the Med- patients may all need to spend time
county councils and for individuals. ical Products Agency deems biologi- finding alternative treatments, result-
The total costs of medicines for hu- cal medicines not to be substitutable ing in repeated contacts with the health
man use in Sweden totalled SEK 36.6 by “copies”, known as biosimilars, in service and pharmacies.
billion in 2014. Total pharmaceutical pharmacies. These factors create lock-
costs have been relatively stable as a in effects, meaning that price pressure Treatments may also be delayed and
proportion of the total healthcare becomes weak or disappears. Unlike other inconveniences may arise due
expenditure. It is notable, however, biological medicines, there has been to medicines for which there is de-
that healthcare costs as a whole have extensive pressure on prices for big- mand not being in stock in community
increased at a faster rate than the ge- selling chemical medicines that are pharmacies. When the pharmacy
neral trend in prices in Sweden in substitutable at pharmacies. The fact market was re-regulated, the circum-
recent years. The cost of pharmaceu- that biological medicines are not sub- stances for dealing with such situa-
tical benefits in 2014 totalled SEK stitutable at pharmacies makes new tions changed, partly as a result of
19.3 billion. This represents a slight demands on the Dental and Pharma- pharmacy activity now being run by
increase in comparison with 2013. ceutical Benefits Agency and county several different pharmacy compa-
councils to be able to change prescrib- nies that do not have an insight into
Forecasts for the trend in pharmaceu- ing patterns and put pressure on prices each other’s stock systems. Geograph-
tical benefit costs, however, point to and costs in these segments when bio- ical availability is also of great signifi-
a sharper increase over the next few similars are available. cance, and it can be noted that the
years. This is considered to be due to new pharmacies that have come into
more people using medicines and Availability of medicines being following re-regulation have
those who use medicines using more Inadequate access to medicines is an mostly been established in the major
medicines, as well as other factors issue that has become more topical in conurbations. A number of measures
that may have a cost-increasing or recent years, and inadequate access to have been taken in recent times to
cost-reducing effect. This applies, for various vaccines in particular has crea- increase availability and improve
example, to the introduction of new ted difficulties for those concerned. service. Mention can be made, for
and sometimes expensive medicines, There are various reasons why med- instance, of a search system for med-
expiring patents and subsequent intro- icines are not available. The most icines that has been developed by the
duction of generic medicines, reviews common is production problems at industry, and a statutory duty on
of medicines included in the pharma- the pharmaceutical company or un- pharmacies to provide information
ceutical benefits scheme by the Dental expectedly high demand, which means on where a medicine is to be found.2
and Pharmaceutical Benefits Agency, that stocks run out sooner than anti- In addition, a system of special grants
2
www.fass.se
8 The National Pharmaceutical Strategy 2016–2018for community pharmacy service in degree. An important task is to develop
sparsely populated areas has been quality registries so that they are better
introduced. There is a need to follow able to capture data on the efficacy of
up and evaluate these measures. new medicines in everyday clinical
practice. With better coordination of
E-health quality registries and opportunities
An area that offers great potential is to use other data, Sweden has potent-
e-health. New ways of offering wel- ial to become one of the world’s lead-
fare services are required in order to ing nations with regard to follow-up
meet the needs and expectations of studies of new medicines. Together
the public, patients and healthcare with a high level of basic research,
professionals. Digitisation provides this makes Sweden more attractive to
this opportunity, but success is depen- the pharmaceutical industry.
dent on long-term work on several
levels. There is a need to continue to At national level there are several
develop the coordination that takes functions that are important in enab-
place today. ling the life science sector in general
and pharmaceutical development in
Areas that need to be addressed in particular to be developed. For ex-
the future to enable to the potential ample, it is crucial that there are effic-
of digitisation to be fulfilled include ient and coordinated authorities, goal-
ensuring a basic infrastructure, stru- adapted information on regulations,
ctured healthcare documentation, coordinated registries and documen-
common prioritisation processes, coll- tation systems and an opportunity to
aboration in new groupings of parti- monitor the use of medicines. At regi-
cipants and appropriate legislation. onal and local level, the healthcare
system holds a key position in the deve-
Knowledge-based and innovative lopment of the life science sector. The
development and promotion of sector contributes to pharmaceutical
life science development in many ways. This takes
The life science sector is of great place, among other things, in parti-
significance to human health, both in cipation in clinical studies, managed
Sweden and globally. This sector is introduction of new, effective medicin-
also significant for the Swedish eco- es and participation in follow-up of
nomy, for the development of the medicines. The mutual dependency
business community and for research. between the development of new med-
Pharmaceutical development is a stra- icines through research and the use of
tegically important area of innovation, the same medicines in the healthcare-
and Sweden has strong biomedical and system is evident and must be noted.
clinical research. It is, however, im- It is thus essential that the collabora-
portant to create the necessary basis for tion in the sector between academia,
continued good development in the the healthcare system, the business
area. Our access to unique infrastruc- community and patients works.
tures with national quality registries,
biobanks and other databases and
registries must be utilised to a greater
The National Pharmaceutical Strategy 2016–2018 9Long-term skills supply affect various organisations in water if the vision of correct use of medi-
Skills supply means that the health- and soil if they escape into the environ- cines to the benefit of patient and
care system must continuously meet ment. Pharmaceutical substances can society is to be attainable. There are
both operational needs and the needs escape into the environment in three many challenges in the area of follow-
of the individual for the right skills, i.e. different ways: with the wastewater up, in particular the fact that it may
both pure manning issues and indi- from excretion by the patient, from be difficult to extract data from patient
vidual development of skills. Knowl- the manufacturing industry or from record systems on non-prescription
edge-based health and medical care is leftover medicines that are discarded medicines and the fact that present-
based on science and proven experi- in the toilet or in household refuse day quality registries only contain pha-
ence and has to be designed to meet instead of being returned to pharma- rmaceutical data to a limited extent.
the needs of patients in the best poss- cies. By far the majority of the sub-
ible way. Health and medical care being stances found in Swedish waters come Utilising and generalising the prac-
knowledge-based depends to a great from excretion by patients. In other tical results from follow-up work
extent on the skills of employees. Acc- parts of the world, for instance in done to date also poses a challenge.
ess to staff with the right skills in the India, as highlighted in several studies, New working methods probably need
right place is one of the greatest chall- there may be very large discharges of to be developed for this. Such methods
enges for health and medical care, active pharmaceutical ingredients from would create the necessary basis for
among other things in view of the manufacturing. The environmental constant improvement in the oppor-
demographic trend with a rapid in- risk assessments that have been made, tunities to follow up use of medicines
crease in the number of elderly persons such as those by Mistra Pharma3, show and their effects.
and more immigrants. The situation that some groups of substances pose
that has arisen with more people than a risk to aquatic organisms. They may Antibiotic resistance
ever seeking asylum in Sweden may also, in the longer term, cause poll- Bacteria that have developed resist-
also pose challenges for health and ution of drinking water. Mistra ance to antibiotics are a growing
medical care. Problems in the area of Pharma has also identified several public health problem. The develop-
skills supply have an impact on a large ways of improving the risk assess- ment of resistance also leads to costs
number of other areas, among which ment of medicines. Various strategies for society and the health service.
is the possibility of offering need- and methods to prevent medicines Tackling the development of resist-
adapted, safe and knowledge-based being dispersed in the environment ance at several levels is a national and
pharmaceutical treatment. Enhanced need to be developed and tested, for global challenge. Using antibiotics in
structures for knowledge management, example with regard to reduced dis- a rational way represents a challenge.
e-learning and smart decision support carding of medicines, treatment of In addition, it is important to ensure
can make medication management wastewater and reduced discharges that antibiotics of particular medical
easier for staff. throughout the life cycle of medicines. value are available for infections that
Sweden presses at the EU and inter- are difficult to treat. Diagnostics and
Environment national levels for greater considera- preventive work are important in the
Medicines in most cases contain sub- tion to be given to the environment battle against the continued develop-
stances that are biologically active. in pharmaceutical legislation, in acc- ment of resistance. Reducing the
This means that the substances can ordance with the special milestone spread of communicable diseases and
target for the environmental quality infections also reduces the need for
3
Mistra Pharma is a research programme funded objective A Non-Toxic Environment. antibiotics. Alongside efforts to main-
by Mistra 2008–2015. The main purposes are to
identify pharmaceutical substances that pose a tain the efficacy of existing antibiot-
risk in the aquatic environment and to propose
strategies for risk reduction. Mechanisms for the
Improved follow-up of medicines ics as far as possible, there is also a
development of antibiotic resistance are also stu- The use of medicines in itself and need for research aimed at the develop-
died. In addition, the programme covers a project
for process engineering development for mun-
effects of pharmaceutical treatment ment of antibiotics with new mecha-
icipal sewage treatment plants. naturally also need to be followed up nisms of action.
10 The National Pharmaceutical Strategy 2016–2018How are the challenges The Government intends to adopt a
addressed? Swedish strategy to tackle antibiotic
Outcomes in Swedish health and med- resistance. The strategy is to cover
ical care have to be world-class. To several sector areas and guide Swedish
achieve this, the area of medicines efforts nationally, in the EU and inter-
must also achieve high quality. Some nationally. The antibiotic strategy is
of the problems described above, for aimed both at giving this work a coll-
example care and availability of med- ective focus and at being used in ex-
icines sometimes being unequal, the change of experience with other
demanded digitisation at times being countries and actors.
delayed, the costs of medicines in-
creasing while the opportunities of In addition, the Government is curr-
society to finance these products are ently reviewing the formulation of
not unlimited and that the surround- future work in the area of e-health.
ing environment may sometimes be Various parties need to work together
adversely affected by pharmaceutical to exploit the potential that exists in
residues, should be addressed so that the area of e-health better. The Gov-
we can have world-class medical care ernment will continue to press for co-
and so that we achieve the vision of operation and coordination between
correct use of medicines to the benefit the efforts of the various parties
of patient and society. Sustainable involved.
solutions are needed to meet these
complex challenges. The challenges The national pharmaceutical strategy
are addressed in one way or another also creates opportunities for coope-
in the national pharmaceutical strategy, rative interfaces with parties in adjoin-
with the aim of ensuring that use of ing areas. Among other things, per-
medicines is effective, safe, accessible, spective groups will be set up that are
equal and economically and environ- to comprise representatives of author-
mentally sustainable. ities and organisations not involved in
the high-level, expert or follow-up
The challenges in the pharmaceutical groups in the national pharmaceutical
area are, however, also addressed strategy.
outside the national pharmaceutical
strategy. An example of Government
efforts is the appointment of the
special life science coordinator. The
work of the coordinator forms part
of the Government’s prioritisation of
life science, and is aimed at further
strengthening the area. Based on
Sweden’s competitive advantages and
development potential, the coordina-
tor contributes material to the Govern-
ment’s efforts to further strengthen
Sweden’s position in the area of life
science.
The National Pharmaceutical Strategy 2016–2018 114. The vision for the national pharmaceutical strategy The vision for the national pharma- ceutical strategy is Correct Use of Medicines to the Benefit of Patient and Society. The vision is formulated to safeguard the interests of both the individual patient and safety for app- ropriate use of medicines and is to focus on sustainability, care for equal health and patient safety. The concept of sustainability includes economic, social and environmental dimensions. If medicines are used correctly, they are a great asset for both patients and society: value is added throughout the care chain. Correct use of medicines means that it is both safe for patients and effec- tive: the correct medicine at the correct dose with patient-adapted information for the correct patient on each individual occasion. The goal ultimately is to use medicines in as cost-effective a way as possible from a societal perspective, in order to be able to achieve the greatest possible health for the resources allocated to medicines in Sweden. 12 The National Pharmaceutical Strategy 2016–2018
5. Objectives of the pharmaceutical
strategy
Five long-term objectives based on the • is safe, i.e. the risk of medical Economically and environmentally
principal challenges Sweden faces in injuries is low, sustainable use of medicines
the pharmaceutical area have been • provides patient benefit, i.e. the The activities in this objectives area
linked to the vision of correct use of medical outcomes are world-class are expected to contribute to use of
medicines to the benefit of patient and the benefit from use of med- medicines that:
and society: icines is high in relation to the risk • is cost-effective, i.e. entails a
to the patient and society and reasonable relationship between
1. Effective and safe use of • is knowledge-based, i.e. systematic outcome and cost,
medication knowledge and, where systematic • provides sustainable cost develop-
knowledge is lacking, clinical exper- ment and
2. Accessible medicines and equal use ience, are used in pharmaceutical • is environmentally sustainable, i.e.
treatment. leads to limited environmental
3. Economically and environmentally impact.
sustainable use of medicines. Note that the National Board of
Health and Welfare’s definition of
The objectives have been formulated effective healthcare means that the care is
on the basis of the concept of “Good designed and provided in collab-
Care” but have been adapted to reflect oration between healthcare actors
the challenges in the area of medicin- based on the severity of the condition
es. The National Board of Health and and the cost-effectiveness of the mea-
Welfare has defined Good Care as sures taken. However, the concept of
knowledge-based and appropriate, effective use of medicines does not include
safe, individually adapted, effective, cost-effectiveness, and instead means
equal and accessible healthcare. Good that the use of medicines has to be
Care is based on the intentions set out rational and knowledge-based.
in the Health and Medical Services Cost-effective use of medicines is to
Act and is a collective term that shows be found instead in the third objective
which objectives and criteria are to of the strategy, together with the objec-
serve as a guide in following up health- tive of environmentally sustainable
care processes, outcomes and costs. use of medicines.
Effective and safe use of Accessible medicines and
medicines equal use
Medicines are a great asset in creating The activities in this objectives area
health and improved quality of life. are expected to contribute to use of
However, if this is to be achieved there medicines that:
is a need for medicines to be used in a
safe way for patients and effectively. • is equal, i.e. access to pharmaceuti-
cal treatment is not influenced by
The activities in this objectives area external factors such as socio-eco-
are expected to contribute to use of nomics, gender or geography but is
medicines that: based on the medical needs of the
individual and
• ensures access to medicines at the
right time
The National Pharmaceutical Strategy 2016–2018 136. The three perspectives of the
pharmaceutical strategy
Perspectives Innovation
There are three perspectives for the Attractiveness for innovation of
strategy: patient, innovation and products and services was a separate
e-health. These perspectives have objectives area in the previous stra-
been chosen because they affect all tegy, but innovation is now raised to
the objectives areas. There are special become a perspective that should be
challenges for all three perspectives included in all objectives and strate-
that need to be addressed in collabo- gies, wherever appropriate. As a result,
ration with other strategies and initia- the concept of innovation can be
tives outside the national pharmaceu- broadened to cover different types
tical strategy. The perspectives help of initiatives that create new assets to
to link the strategy objectives and the benefit of the patient and society.
activities together with other strate- In other words, innovations are to be
gies. The perspectives have to be viewed as means of attaining the vision
considered in planning, decisions, and objectives of the strategy rather
implementation, follow-up and than being an objective in themselves.
evaluation.
E-health
Patient There are special challenges in the
The long-term objectives chosen are area of e-health. Digitisation presents
based on the National Board of great opportunities for improvements
Health and Welfare’s objectives for in health and medical care, but more
Good Care, but are adapted to the coordination and better cooperation
area of medicines and the national are required if success is to be achieved.
pharmaceutical strategy. Patients’ Efforts are needed at several levels,
involvement in their own care and and there is a need for a long-term
treatment is an essential requirement approach. To facilitate coordination
for good health and medical care. between the national pharmaceutical
This is also considered to promote strategy and other initiatives, e-health
equality between women and men in has been chosen as a perspective.
healthcare, which is an important
aspect in work on the strategy. With
regard to children and adolescents,
there may be a need to take account
of special factors in order to create
the necessary basis for involvement.
The purpose in making patient a per-
spective instead of an objective is that
the benefit for the patient should be
considered in activities under the
strategy.
14 The National Pharmaceutical Strategy 2016–20187. Strategy for whom?
The national pharmaceutical strategy
includes a broad set of stakeholders in
the pharmaceutical area. A number of
actors are involved in, or have respons-
ibility for, the various stages, from
research, manufacturing, approval,
reimbursement, prescribing, distribu-
tion and retailing to use and follow-
up of medicines. Patients and health-
care professionals are key parties
alongside the county councils, among
others. Central government has an
important role to play. In addition,
wholesalers and retailers have impor-
tant functions in distribution and
trade. In addition to this there is the
research-based and manufacturing
pharmaceutical industry and a large
number of different special interest
groups.
The national pharmaceutical strategy
covers human medicinal products,
but not medical devices and veterinary
medical products.
The National Pharmaceutical Strategy 2016–2018 158. Organisation
The national pharmaceutical strategy A new participant in the high-level tion of Local Authorities and Regions
is established by the Government and and expert groups is the Swedish and the Swedish Association of the
the Swedish Association of Local Pharmacists Association. The Pharmaceutical Industry. The group
Authorities and Regions, the parties high-level group decides annually on also serves the purpose of broadening
behind the strategy. an updated action plan. There is an collaboration between authorities and
expert group linked to the high-level organisations.
The work on the national pharma- group with a member from each
ceutical strategy is directed by a high- authority/organisation. The There is a group attached to each per-
level group chaired by the Ministry of expert group prepares proposals for spective to contribute to coordinating
Health and Social Affairs and with changes to the pharmaceutical stra- objectives and strategies with other
representatives from the Swedish tegy and associated action plan. strategies. The perspective groups are
Association of Local Authorities and to provide support throughout the
Regions, the Medical Products Agency, Work on following up the national life cycle of the activities, from plan-
the Swedish Association of Health pharmaceutical strategy is directed by ning of the activities to conclusion of
Professionals, the Swedish E-health the Centre for Rational Use of Med- the activities. The perspective groups,
Agency, the Public Health Agency of icines (CBL). A follow-up group has together with the expert group, con-
Sweden, the Health and Social Care been appointed for this task, consist- tribute horizon scanning and provide
Inspectorate, county councils and ing of representatives of the Medical proposals for activities ahead of revis-
regions, the Swedish Association of Products Agency, the National Board ion of the action plan. They are also
the Pharmaceutical Industry, the of Health and Welfare, the Dental and to provide support in the evaluation
National Board of Health and Welfare, Pharmaceutical Benefits Agency, the and follow-up of the activities. The
the Swedish Agency for Health Tech- Swedish Council on Health Techno- perspective groups have representa-
nology Assessment and Assessment logy Assessment and Assessment of tives from other ongoing relevant stra-
of Social Services, the Swedish Phar- Social Services, the Public Health tegies or initiatives that have a bear-
macy Association, the Swedish Med- Agency of Sweden, the Swedish Med- ing on the objectives and activities of
ical Association and the Dental and ical Association, the Swedish Pharma- the strategy.
Pharmaceutical Benefits Agency. cy Association, the Swedish Associa-
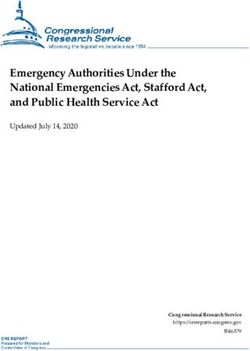
Organisation National pharmaceutical strategy
Ministry of Health and Social Affairs
Swedish Association of Local Authorities and Regions
High-level group
Centre for Rational Use of
Medicines
Perspective Perspective Perspective
Expert group Follow-up group
Patient Innovation E-health
16 The National Pharmaceutical Strategy 2016–20189. How do we measure whether
development is moving in the
direction of the objectives?
To enable it to be ensured that the ried out in structures that already exist.
activities implemented in the strategy The action plan that the high-level
contribute to the objectives of the group has produced by consensus
strategy, the activities must be follow- therefore results in government remits
ed up. Measures of progress towards for authorities, agreements between
objectives also need to be formulated. the Government and the Swedish
It may take time for an effect to be- Association of Local Authorities and
come quantitatively measurable for Regions and other commitments by
many of the activities in the strategy. parties concerned.
In many cases the measures will there-
fore be qualitative in the shorter term, The national pharmaceutical strategy
but they may be quantitative in cases is applicable over the period 2016–
where the follow-up is done over a lon- 2018, while the action plan will be
ger period. revised annually.
Implementation of the National
Pharmaceutical Strategy
Work under the national pharmaceu-
tical strategy is, as far as possible car-
The National Pharmaceutical Strategy 2016–2018 1718 The National Pharmaceutical Strategy 2016–2018
The National Pharmaceutical Strategy 2016–2018 19
Action plan 2016
Introduction The activity has a high degree
The action plan for 2016 under the of urgency
national pharmaceutical strategy con- Horizon scanning, together with the
tains three objectives areas and 18 innovation, patient and e-health per-
activities. Suggestions for activities spectives, guides what activities are
to be included in the action plan have significant and contribute to realising
been received from parties and par- the vision of Correct use of medicines to
ticipants in the national pharmaceuti- the benefit of patient and society.
cal strategy, from the previous action
plan and from the horizon scanning The activity contributes noticeably
of the former Council for Rational Use to putting into effect one or more of
of Medicines. The suggestions have the objectives areas
been processed by the expert group, • Objectives area 1: Effective and
and the high-level group has agreed safe use of medicines
what activities are to be included in
the action plan. • Objectives area 2: Accessible
medicines and equal use
The activities are aimed at addressing
several of the challenges faced in the • Objectives area 3: Economically
pharmaceutical area and, by extension, and environmentally sustainable
at contributing towards use of med- use of medicines
icines being effective, safe, accessible
and equal, as well as economically The activity has a composite set
and environmentally sustainable. of stakeholders
There is a need for several govern-
It is specific to work under the natio- ment agencies or organisations to
nal pharmaceutical strategy that it is cooperate in order to implement the
notable for collaboration between activity.
stakeholders in the pharmaceutical
area and that authorities, county coun- The activity has an
cils and other stakeholders carry out implementation plan
specific activities in accordance with There is an objective for the activity,
current action plan. The activities there is a plan for how the objective is
included in the action plan have ful- to be attained and measured and pro-
filled the following four selection posals for how the activity is to be
criteria: funded.
20 The National Pharmaceutical Strategy 2016–2018Activities in 2016 action plan
Objectives area 1 Objectives area 2 Objectives area 3
Effective and safe use Accessible medicines and Economically and environmentally
of medicines equal use sustainable use of medicines
1.1. S
afer management of medicines 2.1. N
ational collaboration for the 3.1. E
valuation of existing antibiotics
for children development of adaptive licensing for best possible use
of new medicines
1.2. V
aluation of efficacy of treatment 2.2. M
onitor and evaluate the benefit 3.2. M
odels for availability and
in everyday clinical practice of work aimed at managed national responsible use of both new and
introduction of new medicines old antibiotics of particular value
1.3. S
tructure for documentation 2.3. G
reater quality and safety at 3.3. P
romote possibility of addressing
and follow-up pharmacies environmental concerns in the
production and use of medicines
1.4. National medication list 2.4. F
ollow-up of medicines in 3.4. E
nvironmental assessment of
collaboration between govern- non-prescription medicines
ment agencies and healthcare
1.5. P
revent prescribing of medicines 3.5. M
anagement of primary-care
contrary to scientific and proven medicines not included in the
experience pharmaceutical benefits scheme
1.6. M
ake electronic reporting of
side effects possible
1.7. I mproved follow-up of
medication dosage
1.8. E
fforts to improve patient safety
in generic substitution
1.9. C
ommunity pharmacist-led
medicine management inter-
ventions
The National Pharmaceutical Strategy 2016–2018 21Objectives area 1
Effective and safe use of medication
1.1. Safer management of boys supports the development of Introduction
medicines for children more effective, safe, accessible and The purpose of the project is to im-
equal use of medicines. prove the transferability of data from
Main responsibility: Medical Products randomised clinical studies (RCTs) to
Agency Collaborating activities follow-up of the efficacy of medicines
This activity is in line with paediatric in everyday clinical practice. The pro-
Introduction legislation in the EU and is in good ject is therefore intended to create
The purpose of this activity is to bring agreement with the Medical Products better decision-support material for
about safer management of medicines Agency’s government remit “to im- decision-makers in county councils,
given to girls and boys. Children are prove knowledge of paediatric med- regions and authorities in follow-up
at greater risk of being affected by icines and their use and promote safer after the introduction of new medi-
medication-related problems as many medication management”. The activity cines. Another aim is for the project
medicines used for children are in- contributes greater knowledge to nat- to contribute to better assessments of
sufficiently documented in terms of ional knowledge support in medica- the cost-effectiveness of medicines
efficacy and safety and are not adapted tion prescriptions for children, ePed. over time and generally improve qual-
to children with regard to dose and ity in follow-up of the use of medicin-
pharmaceutical form. The safety mar- Interfaces for cooperation es in clinical practice. Improving the
gins in incorrect dosing for a young The activity involves collaboration quality and usability of data from
child are also narrower than for an with the National Board of Health clinical registries can also, in a broader
adult. Endeavouring to ensure safer and Welfare, the Health and Social perspective, bolster Sweden’s position
use of medicines for children is a cru- Care Inspectorate, the Swedish Coun- and attractiveness as a country for
cial issue of equality and patient safety. cil on Health Technology Assessment innovative development and follow-
and Assessment of Social Services, up in the pharmaceutical area.
Healthcare professions active in the the Swedish Association of Local
paediatric area have prioritised med- Authorities and Regions, the Swedish Objectives areas
ication management and children as Association of Health Professionals, Developing statistical methodology
the crucially important area in which representatives of the healthcare sys- to compare efficacy outcomes in
to produce a knowledge document. tem (doctors, nurses and pharmacists) quality registries or equivalent with
Medication management covers the and children in the capacity of patients outcomes in treatment and control
activities that form part of the patient’s and their carers. groups in randomised clinical trials
medication process, from prescribing supports the development of more
to administration of a medicine, and Implementation plan effective, safe, economically and
includes both the physical handling In May 2016, the Medical Products environmentally sustainable use of
of the medicine and transfer of infor- Agency will hold an expert meeting medicines.
mation, regardless of who manages on medication management for child-
the medicine. Information transfer to ren. A new knowledge document in Collaborating activities
children that is adapted to their age the area is expected to be ready for This activity improves the possibility
and level of maturity is also important publication in January 2017. of adaptive licensing being implement-
in this context. There is also a need to ed with more reliable data on efficacy
produce knowledge documents that and cost-effectiveness. The activity
can be used as material in the training 1.2. Valuation of treatment effi- also radically improves the prospects
of nurses, for example. cacy in everyday clinical practice of meaningful follow-up of medicines.
It ought also to be possible for the
Objectives areas Main responsibility: Swedish Council activity to provide a better basis for
The work on developing safer manage- on Technology Assessment in the pharmaceutical treatment of
ment of medicines given to girls and Health Care elderly patients.
22 The National Pharmaceutical Strategy 2016–2018Interfaces for cooperation Introduction
The project is a cooperation between The work on developing models that
the Swedish Council on Health Tech- describe processes, information flows,
nology Assessment and Assessment concepts and information structures
of Social Services, the Dental and has begun and will continue in 2016.
Pharmaceutical Benefits Agency, the The main purpose of the work is to
Medical Products Agency, the Nat- contribute to uniform structures for
ional Board of Health and Welfare, documentation and follow-up of use
the Swedish Association of Local of medicines. The models will be supp-
Authorities and Regions, Stockholm lemented by method descriptions for
County Council and other affected operational information analysis to
authorities and organisations. enable semantic interoperability, i.e.
common understanding of the terms
Implementation plan and the information descriptions that
The activity consists of two or three are used. The principal focus for 2016
sub-projects. With effect from the will be an information structure for
autumn of 2015, a systematic litera- the use of medicines in hospitals and
ture review is being conducted to take the sharing of information about
stock of current knowledge in the area. medications.
Depending on the outcome of this
study, it will be possible to develop a Objectives areas
method that could be used to assess The work on models supports the
efficacy outcomes in quality registries development of more effective and
in relation to data from previously safer use of medicines. In a broader
conducted randomised clinical trials. perspective, structured care docu-
This method will then be applied to a mentation creates the necessary basis
few suitable pilot medicines. Alterna- for work in all the objectives areas in
tively, if the literature review identi- the national pharmaceutical strategy.
fies an already established, usable
method, this will be used directly. Collaborating activities and
If the pilot tests show that the method interfaces for cooperation
provides usable results, the methodol- This work is a continuation of the
ogy can start to be used for routine activity Enable follow-up of ordered
follow-up of the clinical efficacy of medicines at an individual level l in
new medicines, for example under the previous action plan.
the processes for managed introduc-
tion and adaptive licensing. The work is expected, among other
things, to provide support in the
continued development of a national
1.3. Structure for documentation medication list. Models for prescrib-
and follow-up ing and administration can also con-
tribute to more systematic work on
Main responsibility: Swedish Associa- improved follow-up of the use of med-
tion of Local Authorities and Regions icines, among other things in Man-
aged introduction. The work as a
whole forms part of the fundamental
The National Pharmaceutical Strategy 2016–2018 23You can also read