Operating Plan 2017-18 - 2018/19 Refresh - Version: Date: 1.0 15th June 2018 - NHS Corby CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Operating Plan 2017-18 - 2018/19 Refresh Version: 1.0 Date: 15th June 2018
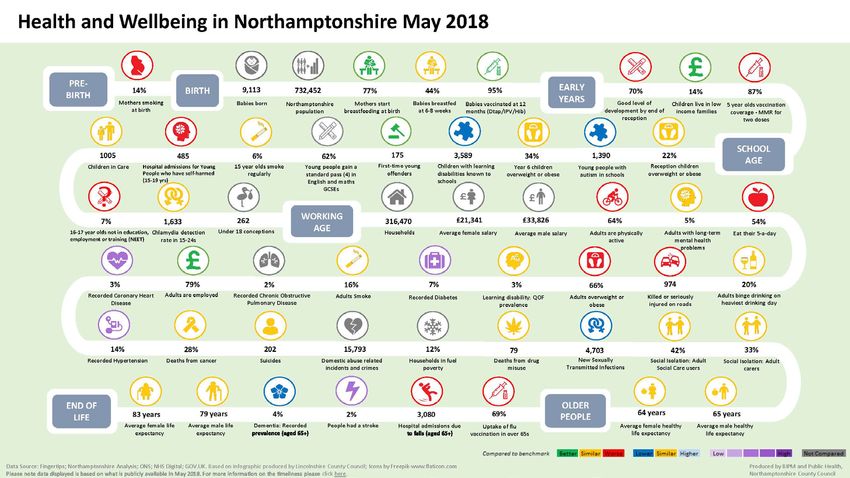
Table of Contents
1. Introduction .............................................................................................................. 1
Aim of the Operational Plan ............................................................................................... 1
2. National Context & Policy .......................................................................................... 2
3. Local Context & Policy ............................................................................................... 5
Nene and Corby CCGs ......................................................................................................... 5
Our Population.................................................................................................................... 5
Who We Buy Our Healthcare Services From ...................................................................... 9
Local Operating Context ..................................................................................................... 9
CCGs’ Joint Management.................................................................................................. 10
CCGs’ Joint Corporate Objectives ..................................................................................... 11
Joint Commissioning Intentions ....................................................................................... 11
Our Future Vision for Integrated Care .............................................................................. 12
Our Commissioning Approach .......................................................................................... 12
Delivery Plans for 2018/19 ............................................................................................... 14
4. Northamptonshire Health & Care Partnership .......................................................... 18
Northamptonshire Health & Care Partnership Structure................................................. 19
Programme Plan .................................................................. Error! Bookmark not defined.
New Models of Care : Workstream Definition Document Objectives ............................. 20
5. Finance .................................................................................................................... 22
Introduction ...................................................................................................................... 22
Overall CCG Financial Management ................................................................................. 22
Planning Assumptions....................................................................................................... 22
CCG Revised Control Totals and Business Rules for 2018/19........................................... 23
Contracts ........................................................................................................................... 24
Financial Plans................................................................................................................... 25
Key Financial Risks ............................................................................................................ 27
QIPP .................................................................................................................................. 27
Approach to Efficiency ...................................................................................................... 27
Expenditure in 2018/19 .................................................................................................... 28
Health System Balance ..................................................................................................... 29
6. Strategic Commissioning & Framework .................................................................... 31
How is Strategic Commissioning Different? ..................................................................... 31
i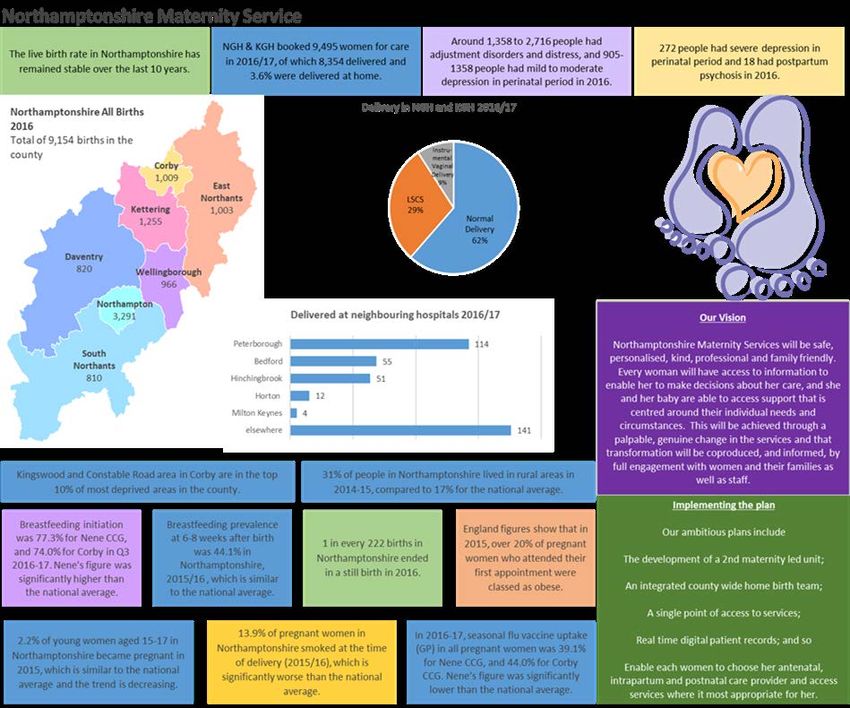
7. Delivering our Contractual Position.......................................................................... 32
2017/19 Contracts ............................................................................................................ 32
Contract Variations for STP Priority Transformation Schemes ........................................ 32
Contract Values................................................................................................................. 32
Readmissions/Marginal Rate Emergency Tariff (MRET)................................................... 32
8. Prevention & Self-Management ....................................... Error! Bookmark not defined.
9. Primary Care............................................................................................................ 35
Re-Provision of Corby Urgent Care Centre ....................................................................... 36
10. Urgent & Emergency Care ........................................................................................ 37
Intermediate Care ............................................................................................................. 39
What are we doing in support of NHS England’s 2018/19 deliverables? Error! Bookmark
not defined.
11. Planned Care (including Maternity) .......................................................................... 41
Planned Care ..................................................................................................................... 41
Maternity .......................................................................................................................... 43
What are we doing in support of NHS England’s 2018/19 deliverables? ........................ 44
12. Cancer ..................................................................................................................... 45
13. NHS Continuing Healthcare ...................................................................................... 48
CHC Transformation: Applying New Models .................................................................... 50
14. Mental Health ......................................................................................................... 51
National Challenge ............................................................................................................ 51
Northamptonshire Position - Adult and Older People ..................................................... 52
Future in Mind - the Children and Young People’s Mental Health Transformation Plan 53
Local Delivery Priorities .................................................................................................... 53
15. Learning Disabilities ................................................................................................. 55
The Local Approach .......................................................................................................... 55
.......................................................................................................................................... 55
Our Local Evaluation ......................................................................................................... 55
Local Delivery Priorities .................................................................................................... 56
What are we doing in support of NHS England’s 2018/19 deliverables? ........................ 57
16. Services for Children and Young People ................................................................... 59
18. Services for People in the Last Years of Life .............................................................. 64
ii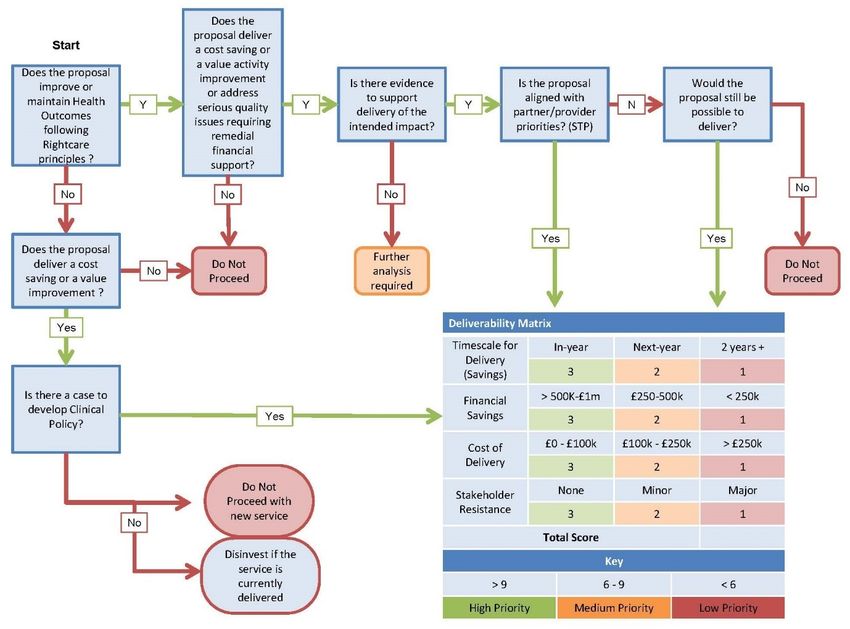
19. Delivering Quality Care ............................................................................................ 66
Quality Priorities ............................................................................................................... 66
CQC Inspection Updates ................................................................................................... 68
Quality Improvement (QI) ................................................................................................ 70
APPENDIX A – PERFORMANCE STANDARDS ............................ Error! Bookmark not defined.
iii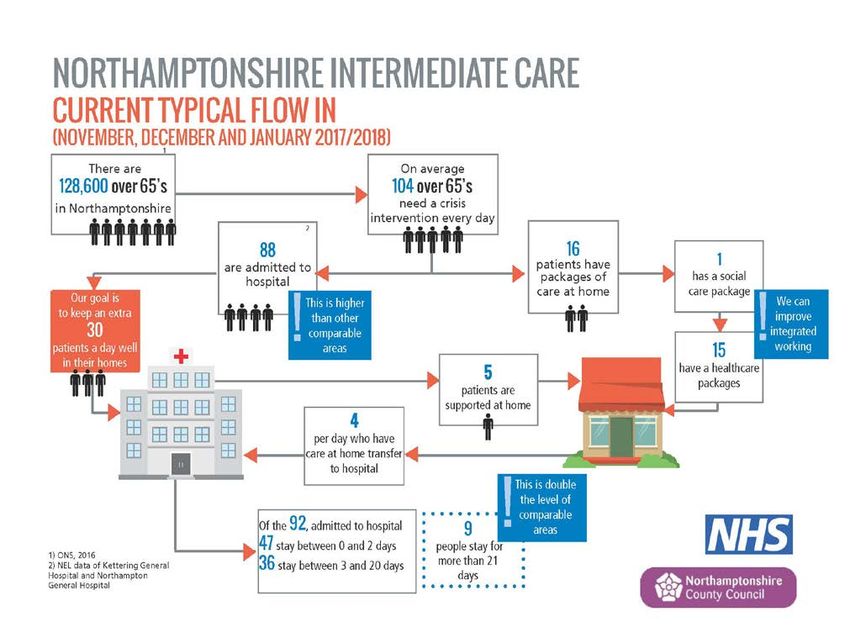
1. Introduction
Last year, Nene and Corby CCGs developed their first jointly approved Operating Plan for the
period 2017/18 – 2018/19. This document represents a refresh of that plan for 2018/19 in
the context of the latest planning guidance from NHS England 1 and the plans developed by
the Northamptonshire Health and Care Partnership (previously known as the
Northamptonshire Sustainability & Transformation Partnership).
During this period, the local health and social care system has undergone structural and
organisational changes as it continues to find ways to achieve clinical, operational and
financial sustainability in the face of ongoing challenges around increasing demand for care
and services.
Partners across Northamptonshire continue to work together, predominantly through the
Northamptonshire Health and Care Partnership. Whilst Nene and Corby CCGs have
produced this Operating Plan, it is aligned with the strategic aims and objectives of the
wider system, whilst ensuring CCGs’ efforts continue to focus on those priority areas that
will deliver quality, performance and financial efficiencies, and to ensure we meet our NHS
constitutional standards.
Aim of the Operational Plan
This document sets out the on-going plan for the delivery of health and care in
Northamptonshire in 2018/19. The plan supports the wider Northamptonshire’s Health and
Care Partnership’s proposals as we enter year 3 of the national 5-year plan; the NHS
constitution; and the NHS Mandate.
1
https://www.england.nhs.uk/wp-content/uploads/2018/02/planning-guidance-18-19.pdf
-1-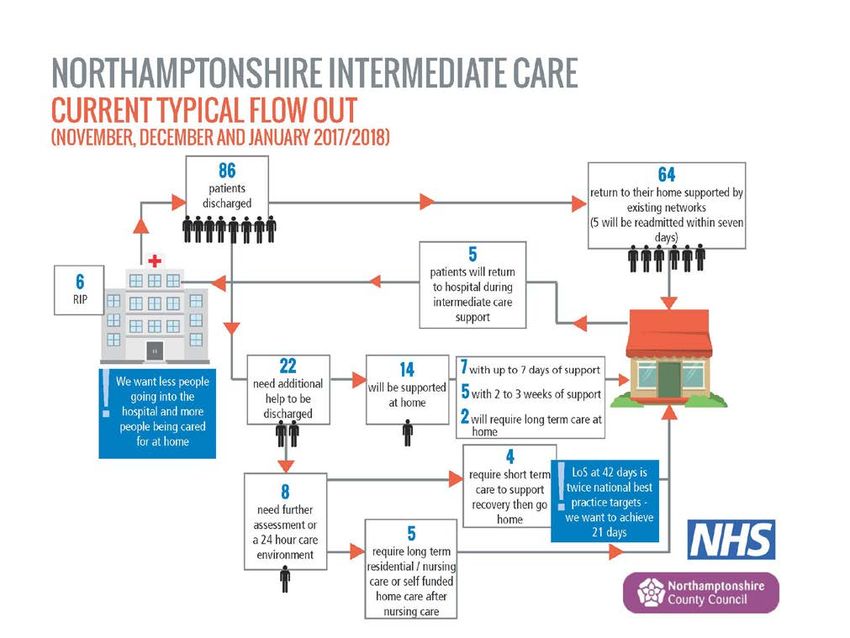
2. National Context & Policy
Significant challenges continue to exist both nationally and locally for the present and future
delivery of healthcare services. These include an expanding and ageing population; evolving
healthcare needs to address lifestyle behaviors; increasing numbers of people attending
A&E Departments; medically fit patients not able to leave hospital due to lack of post-
discharge support (i.e. Delayed Transfers of Care – DTOCs); all set against a backdrop of
rising costs and workforce challenges.
Each health system is required to meet those challenges, and the “must dos” as mandated
by the Government and in support of NHS England’s 2 objectives.
In the 2018/19 planning guidance, NHS England set out 9 “must dos” for 2017-19, a
summary of which can be found below:
Table 1. 2017/18 and 2018/19 “Must Dos”
2017/18 and 2018/19 National “Must Dos”
1. STPs
• Implement agreed STP milestones so systems are on track for full achievements by 2020/21;
• Achieve agreed trajectories against the STP core metrics set for 2017-19.
2. Finance
• Deliver individual CCG and NHS provider organisational control totals and achieve local system
financial control totals;
• Implement local STP plans and achieve local targets to moderate demand growth and increase
provider efficiencies;
• Demand reduction measures;
• Provider efficiency measures.
3. Primary Care
• Ensure the sustainability of general practice in your area by implementing the General Practice
Forward View;
• Ensure local investment meets or exceeds minimum required levels;
• Tackle workforce and workload issues;
• By no later than March 2019, extend and improve access in line with requirements for new
national funding;
• Support general practice at scale, the expansion of MCPs or PACS, and enable and fund primary
care to play its part in fully implementing the forthcoming framework for improving health in care
homes.
4. Urgent & Emergency Care
• Deliver the four-hour A&E standard, and standards for ambulance response times including
through implementing the five elements of the A&E Improvement Plan;
• By November 2017, meet the four priority standards for seven-day hospital services for all urgent
network specialist services;
• Implement the Urgent and Emergency Care Review;
• Deliver a reduction in the proportion of ambulance 999 calls that result in avoidable transportation
2
NHS England is an executive non-departmental public body (NDPB) of the Department of Health that
oversees the budget, planning, delivery and day-to-day operation of the commissioning side of the NHS in
England, as set out in the Health and Social Care Act 2012.
-2-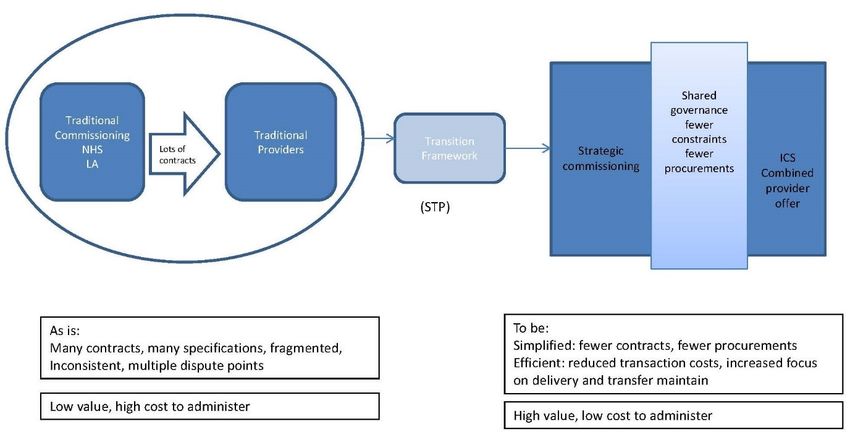
2017/18 and 2018/19 National “Must Dos”
to an A&E department;
• Initiate cross-system approach to prepare for forthcoming waiting time standard for urgent care
for those in a mental health crisis.
5. Referral to Treatment Times & Elective Care
• Deliver the NHS Constitution standard that more than 92% of patients on non-emergency
pathways wait no more than 18 weeks from referral to treatment (RTT);
• Deliver patient choice of first outpatient appointment, and achieve 100% of use of e-referrals by no
later than April 2018 in line with the 2017/18 CQUIN and payment changes from October 2018;
• Streamline elective care pathways, including through outpatient redesign and avoiding
unnecessary follow-ups;
• Implement the national maternity services review, Better Births, through local maternity systems.
6. Cancer
• Through Cancer Alliances and the National Cancer Vanguard, implement the cancer taskforce
report;
• Deliver the NHS Constitution 62-day cancer standard;
• Make progress in improving one-year survival rates by delivering a year-on-year improvement in
the proportion of cancers diagnosed at stage one and stage two; and reducing the proportion of
cancers diagnosed following an emergency admission;
• Ensure stratified follow up pathways for breast cancer patients are rolled out and prepare to roll
out for other cancer types;
• Ensure all elements of the Recovery Package are commissioned.
7. Mental Health
• Deliver in full the implementation plan for the Mental Health Five Year Forward View for all ages;
• Ensure delivery of the mental health access and quality standards including 24/7 access to
community crisis resolution teams and home treatment teams and mental health liaison services in
acute hospitals;
• Increase baseline spend on mental health to deliver the Mental Health Investment Standard.
• Maintain a dementia diagnosis rate of at least two thirds of estimated local prevalence, and have
due regard to the forthcoming NHS implementation guidance on dementia focusing on post-
diagnostic care and support; and
• Eliminate out of area placements for non-specialist acute care by 2020/21.
8. People with Learning Disabilities
• Deliver Transforming Care Partnership plans with local government partners, enhancing
community provision for people with learning disabilities and/or autism;
• Reduce inpatient bed capacity by March 2019 to 10-15 in CCG-commissioned beds per million
population, and 20-25 in NHS England-commissioned beds per million population;
• Improve access to healthcare for people with learning disability so that by 2020, 75% of people on
a GP register are receiving an annual health check;
• Reduce premature mortality by improving access to health services, education and training of staff,
and by making necessary reasonable adjustments for people with a learning disability and/or
autism;
• Eliminate out of area placements for non-specialist acute care by 2020/21.
9. Improving Quality in Organisations
• All organisations should implement plans to improve quality of care, particularly for organisations
in special measures;
• Drawing on the National Quality Board’s resources, measure and improve efficient use of staffing
resources to ensure safe, sustainable and productive services;
• Participate in the annual publication of findings from reviews of deaths, to include the annual
publication of avoidable death rates, and actions they have taken to reduce deaths related to
problems in healthcare.
-3-
NHS England’s Five Year Forward View notes that "The traditional divide between primary
care, community services, and hospitals – largely unaltered since the birth of the NHS – is
increasingly a barrier to the personalised and coordinated health services patients need.
Long term conditions are now a central task of the NHS; caring for these needs requires a
partnership with patients over the long term rather than providing single, unconnected
'episodes' of care. Increasingly we need to manage systems – networks of care – not just
organisations. Out-of-hospital care needs to become a much larger part of what the NHS
does and services need to be integrated around the patient".
The strategic aim set out by NHS England is to make “the biggest national move to
integrated care of any major western country”. The planning guidance for 2018/19 clearly
states that local health and care systems are expected to:
• Ensure a system-wide approach to operating plans that aligns with key assumptions
between providers and commissioners;
• Work with local clinical leaders to implement service improvements that require system-
wide effort;
• Identify system-wide efficiency opportunities; and
• Take further steps to enhance the capability of the system including stronger
governance and aligned decision making.
-4-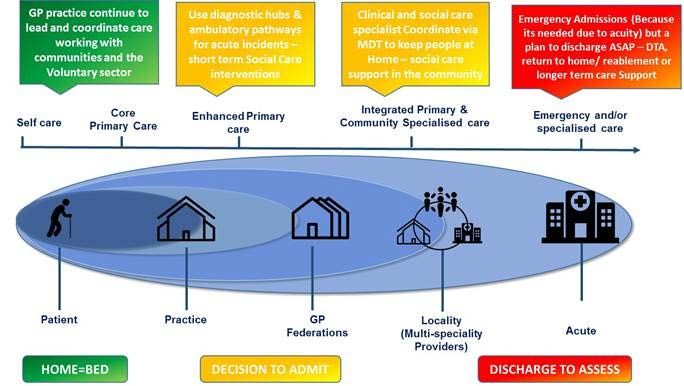
3. Local Context & Policy
Nene and Corby CCGs
NHS Nene CCG is responsible for commissioning (planning and buying) most health services
for a large area across Daventry, Northampton, Wellingborough, Kettering, East
Northamptonshire and South Northamptonshire, covering a population of circa 662,000
people.
NHS Corby CCG is responsible for commissioning most health services for Corby which has a
registered population of around 78,785 patients and which is growing rapidly, with 10,000
patients registered to Corby practices from outside the boundaries of Corby.
There are a total of 70 GP practices operating under both CCGs (Nene – 65; and Corby – 5);
3 GP Federations; and 1 Super-Practice.
Our Population
Northamptonshire as a whole has a population of
733,128 3 residing in mixed rural and urban areas
covering 2,364 km2, which is both growing and
ageing. The county has experienced significant
growth in recent decades, resulting in a 9.1%
increase in the last 10 years, in comparison to an
England average of 7.6%, with this trend set to
continue. The growth in Corby’s population has
been noticeably exponential, seeing a 22% in the
last 13 years (from 54,900 to 66,900). This is in part
due to a building programme which saw nearly ten
thousand new homes being built during 2011-17,
and this growth rate is set to continue with an
additional new 11,000 projected new residents
expected by 2020.
The health of people in Northamptonshire is varied compared with the England average.
About 16% (22,800) of children live in low income families across the county (20% in Corby
specifically), and whilst life expectancy for both men and women is similar to the England
average and expected to increase, health inequalities show that life expectancy is 8.8 years
lower for men and 7.0 years lower for women in the most deprived areas of
Northamptonshire than in the least deprived areas. Again, these figures are worse for
Corby, rising to 11.2 years lower for men and 10.8 years lower for women.
18.3% (1,299) of year 6 children across Northamptonshire are classified as obese, which is
better than the average for England. Estimated levels of adult excess weight are worse than
3
ONS 2016 mid-year estimates
-5-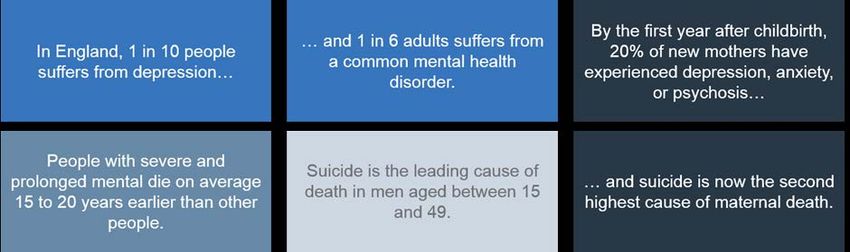
the England average, as is the rate of people killed and seriously injured on roads.
The rate of alcohol-related harm hospital stays for adults is 682, representing 4,715 stays
per year, which is higher than the average for England. The rate of self-harm hospital stays
is also worse (255), and rates of smoking related deaths is 281 per 100,000 population,
representing 1,038 deaths per year.
There has been a declining rate of mortality across Northamptonshire. Changes to the
under 75 mortality rates for cancer have decreased significantly from 151.3 per 100,000
population in 2009-11, to 136.0 per 100,000 population in 2013-15; and mortality rates
from “preventable” causes is similar to the England average (183.7 per 100,000 compared
to 184.5 for England in 2013-15).
Northamptonshire has high rates of common mental health issues such as anxiety and
depression, which is expected to increase over the next five years, compounded by levels of
homelessness and alcohol use. The numbers of patients living with dementia reflects the
England average, with over 10,000 people over the age of 65 expected to have the condition
by 2020.
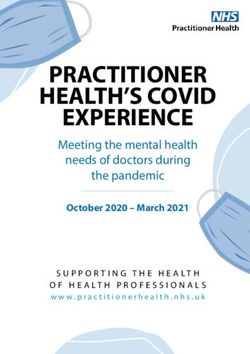
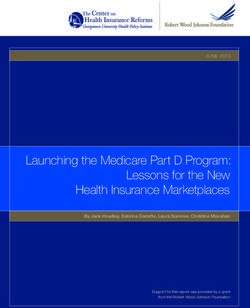
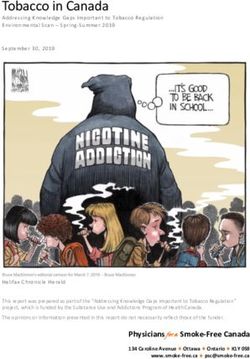
Two snapshots of the Northamptonshire population and its health can be found below:
Figure 1. Northamptonshire Health Profile, 2017
-6--7-
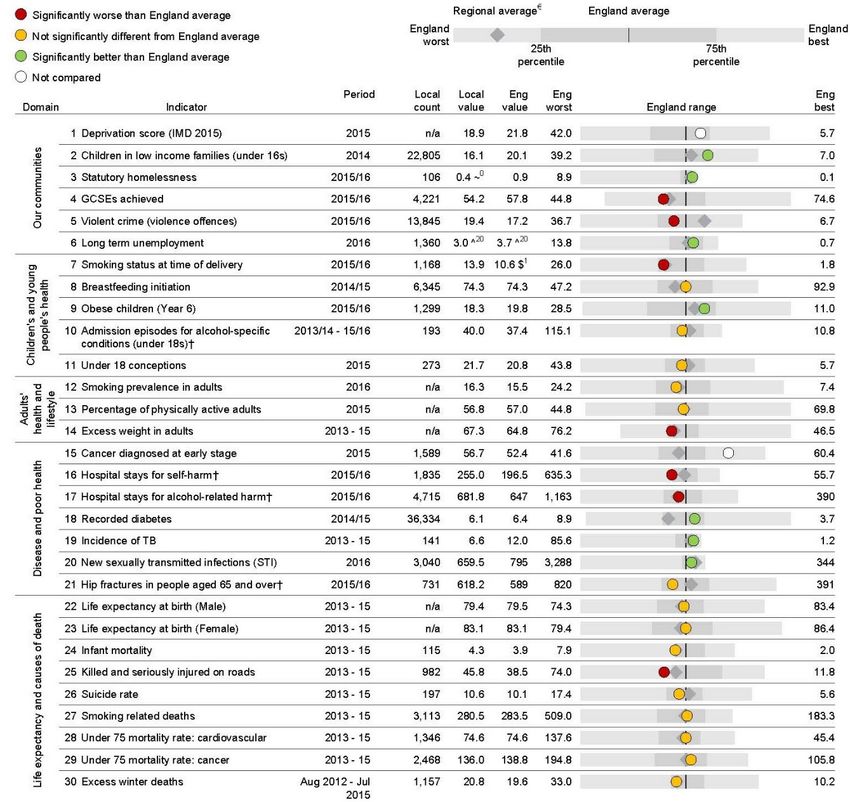
Figure 2. Health & Well-Being in Northamptonshire (May 2018)
-8-Who We Buy Our Healthcare Services From
We buy our health services from a range of providers (any organisation commissioned to supply a
health or care-based service) including acute hospital trusts; mental and community health trusts;
GP practices, super-practice and federations; voluntary and third sector organisations; social work;
home support; health visiting and district nursing.
Some of our main providers are listed below:
• Northampton General Hospital NHS Trust (NGH) and Kettering General Hospital NHS
Foundation Trust (KGH) are the main providers of acute care for Northamptonshire;
• Northamptonshire Healthcare NHS Foundation Trust (NHFT) provides the majority of our
community and mental health services;
• East Midlands Ambulance Service;
+
• Lakeside for the Corby Urgent Care Centre;
• Other hospitals in nearby counties; independent sector providers; social care providers;
community healthcare and voluntary sector organisations to give patients the opportunity to
choose their preferred provider;
• For Nene, there are three GP Federations formed by the 65 member practices: GP Alliance
(who operate in Northampton); 3 Sixty Care (who operate in the north of the county), and PML-
DocMed (who operate in the south). In addition to this, Corby CCG has a Super-Practice
(Lakeside Healthcare).
Local Operating Context
There continue to be a range of local critical operating factors within Northamptonshire that
impact on the delivery of health and care services in the county, and drives the changes needed to
make sure we can deliver the highest quality of care for all whilst making most appropriate use of
resources to improve the health and well-being of our growing and ageing population, at a time of
continuing rises in demand but within limited resources.
One of the biggest challenges that has arisen relates to the well publicised changes to local
Government in Northamptonshire. Following a review of its finances, the Secretary of State for the
Department of Health and Social Care, appointed two commissioners to dissolve Northamptonshire
County Council, and to create a new authority or authorities by 2020. Options being considered as
part of a formal consultation exercise, include an option for 2 unitary organisations.
Business as usual is supported by the new commissioners, enabling good relationships to continue
to exist between health and local government. Whilst the situation inevitably gives rise to
challenges and risks to funding, the system will endeavor to use this opportunity to look at new
ways of commissioning health and care services.
Other key factors for the local system include:
• Quality, safety and minimizing harm
o The healthcare system has not been able to meet and maintain core constitutional
-9-standards in relation to A&E, RTT and cancer;
o Where organisations are in turnaround, the financial impact can often be significant;
o Care Quality Commission (CQC) reports highlight areas that require improvement;
o Agency rates are high leading to some of the highest agency spend levels in England for
some organisations
• Infrastructure and estate
o The local model for community services continues to have a high bed base and high
overheads;
o Some local estate is ageing and may not be suitable for the provision of modern healthcare
services;
o Long term Private Finance Initiative (PFI) contracts within the care sector are inflexible and
less able to move at a pace to meet changing patterns of demand;
o New contractual models are required to drive different outcomes [from the estate];
o Intermediate Care Team (ICT) arrangements are a barrier to delivery
• Integration and models of care delivery
o Having been recognised as having the most financially challenged Local Authority in the
country, the county is undergoing wide changes at Local Government level (as detailed
above) which provides its own challenges on its ability to deliver change through enabling
frameworks such as Better Care Fund (BCF);
o Integration of health and care remains limited, impacting on patient flow, process
challenges and risk.
Our key local challenges continue to be:
• Lifestyle and well-being issues that drive people into the health system, in particular due to
respiratory conditions, circulation issues, cancer and mental health;
• Population demographics, needs and personal preferences are changing but our services are
not yet aligned to these;
• Demand pressures and lack of resources in out-of-hospital settings means that too many
people are being admitted to hospital bed-based services;
• Despite some areas of improvement since last year, our patients are continuing to experience
poor access and quality of care from some of our local providers, as reflected in poor
performances against Accident & Emergency 4-hour wait standard; Referral to Treatment (RTT)
waiting times; East Midlands Ambulance Service (EMAS) response and handover times; and
cancer waits;
• We continue to have workforce shortages and key skills gaps affecting our ability to provide the
quality of service are patients require to keep them well, and increasing the cost of delivering
services.
CCGs’ Joint Management
During 2017/18, NHS Nene and Corby CCGs came together to further strengthen their joint working
by establishing a single joint management team, whilst continuing to be two separate statutory
bodies.
The key changes made include:
• Joint Committees - Joint Finance Committee; Joint (new) Strategic
- 10 -Commissioning Committee
• Committees in Common - Patient & Public Assurance Committee;
Remuneration Committee; Audit Committee
• Joint Appointments - Joint Accountable Officer; Joint Chief Finance
Officer; Joint Secondary Care Officer; Joint
Medical Director with responsibilities for quality &
safety
The following will not change:
• Each CCG will retain their respective Governing Bodies; their separate statutory accountabilities
for assurance; and their member-elected clinical roles;
• The approach to commissioning will remain clinically led and informed; and
• The principle that individual communities and membership voices are heard in any new
arrangements, is enshrined.
The CCGs will use this opportunity to improve working and communication links between
Committees and groups; improve reporting and feedback mechanisms (internally and externally)
including a robust communications & engagement plan; strengthened oversight and delivery of
plans; and strengthened risk assessment and management of respective duties.
CCGs’ Joint Corporate Objectives
Both CCGs’ joint corporate objectives for 2018/19 are:
• Quallity – we will improve quality within all providers to ensure services are safe, efficient and
effective;
• Transformation – we will create the environment to enable the commissioning and delivery of
high quality services to reduce health inequalities and improve health outcomes and resilient
communities;
• Commission sustainable services – we will ensure the development of seamless transition
between providers where patients need the support or intervention of primary care; community
care; secondary care; social services; or the voluntary sector, within available resources,
ensuring high quality provision and best value for money;
• Engagement – we will engage patients, public, members and partner organisations to ensure
that services are delivered at the right time, in the right place and to the highest quality;
• Workforce and culture – we will develop and support a motivated workforce equipped with the
required capabilities, culture and competencies to meet the evolving needs of primary care, and
the progression towards a strategic commissioning function;
• Accountability – we will be truly accountable to our population and have appropriate
arrangements in place to discharge our functions effectively, efficiently and economically, and in
accordance with the statutory framework and best practice principles of good governance and
transparency.
Joint Commissioning Intentions
This plan supports the joint Nene and Corby CCGs Commissioning Intentions document, published
in 2017. Our Commissioning Intentions set out the changes and improvements expected across
- 11 -pathways of care, mapped to the following settings of care:
• Prevention & self-management;
• Primary care;
• Enhanced primary and community care;
• Intermediate care; and
• Acute care.
Our Future Vision for Integrated Care
With the support of our local partners, and in support of the national direction of travel and our
commissioning intentions, we will work towards delivering an integrated model of care:
Figure 3. Integrated Care
/
Super Practices
Our Commissioning Approach
NHS RightCare Opportunities
The CCGs will continue to use NHS England’s RightCare data to help underpin and support the
commissioning of services moving forward, making the NHS’s valuable resources go as far as
possible whilst improving patient outcome as much as possible. NHS RightCare provides data on
local health economies spend data, patient admissions and prescribing data, alongside other
evidence. It helps to shine a light on variation and performance, and by doing so, helping to
identify opportunities for local improvements.
This year, NHS RightCare’s data pack for Northamptonshire identifies some potential early
opportunities for discussion and prioritisation:
• Non Elective Care
o Respiratory – opportunities to improve COPD and asthma management in primary and
- 12 -community care, as well as smoking prevalence conditions;
o Problems of circulation (CVD) – CHD (from early detection of hypertension to cholesterol
management and optimising prescribing); stroke (AF management and optimising anti-
coagulant prescribing); diabetes (continuing the work already undertaken in primary and
acute care to optimise patient care);
o Trauma & injuries – particularly for frailty patients, dementia, osteoperosis and fragility
fractures (mainly hip);
o Neurology, genitourinary; and gastrointestinal – will require further local interpretation to
identify potential opportunities.
• Elective Care
o MSK provides an opportunity to further improve pathways, with the MSK Referral
Management Service which began piloting during Q4 2017/18, to be evaluated in light of
NHS RightCare data;
o Prescribing – MSK and other prescribing opportunities will be looked at further locally to
see if these present further opportunities.
Value Based Conversations & Decisions
As commissioners, it is imperative that getting as much value out of limited resources is at the
heart of our decision-making process when looking at the care needed to most improve our
population’s outcomes.
It is imperative that we explain the value for money that is expected to be delivered in all our
decisions. The CCGs will increasingly need to find ways to balance activity, finance and non-activity
based risks, and to demonstrate value for money whilst adhering to the NHS Constitution and NHS
England’s mandate. Where this cannot be demonstrated, remedial action plans will be developed.
Below is an example of a decision tree which will be used to support future decision-making:
Figure 4. Decision Making Tree for Investment Decisions
- 13 -We are committed to continuing to work with our local providers and would like them to be the
providers of choice – to do this, we need different conversations and a different contract approach.
Our intention is to move towards risk/gain share agreements that work to help best meet patients’
needs to the quality standards required. We want an open book approach to maintain ongoing
investments and to meet strategic drivers.
Service Development Improvement Plans (SDIPs) will be applied to known areas of
productivity/cost challenge, and agreement sought to adhere to findings. We will also seek
agreement and resolution to competitive dialogue discussions, and to share issues at a senior level
over the life of contracts.
Strategic Commissioning
Using the above intelligence to help identify our opportunities, the CCGs will take a strategic
commissioning approach to the planning and buying of health services, by looking at whole
populations (either geographical or by conditions) to help maximise the value of what we’re able to
deliver within our allocated funding.
Strategic commissioning involves identifying the needs of individuals and communities, enabling
health and care systems to decide what will best address those needs and working together with
agencies to put the right services and support in place.
More details about the CCGs’ strategic commissioning framework can be found at Chapter 6.
Delivery Plans for 2018/19
As the CCGs work ever more closely with each other, there will be clear oversight and monitoring
- 14 -of delivery programmes for each area of work.
The key programmes of work are outlined below, and the background to each of these can be
found in more detail in the subsequent chapters.
Table 2. CCG Delivery Plans – 2018/19
No. Deliverable By When Lead(s) / SRO
Primary Care
1. Completion of pilot for online consultations and creation
Q2
of roll out plan
2. Completion of resilience programme with E. Northants
Q2
cluster
3. Commissioning of extended GP access to cover 100% of
Q3
the population
4. Commissioning of GP out of hours service to cover 100%
Q4
of the population
5. Successful IR bid and creation of associated work
Q2
programme
6. Creation of primary care home development plan for all
local primary care homes/practice clusters (to include all Q4
practices)
7. Completion of GPGV Development for Practice Manager
Q4
Training throughout 2018/19
8. Estates review to support STP work programme:-
• Recruitment of Health Planner to support Estates
Planning for the county Q2
• Workstream 1 – Production of an STP Capital and
Estates Programme Q2
• Workstream 2 – Community Hospital Review Q3
• Workstream 3 – Planning for Population Growth Q4
Modelling
Urgent & Emergency Care
1. System recommendation for addressing demand and
Qtr 1
capacity
2. Development of a robust demand and capacity plan
3. Implementation of approvals process for schemes
addressing non-elective admissions
Planned Care
1. Referral Management System – monitor MSK RMS and D Sandhu / A Ali
Qtrs 1 & 2
review C Williams
2. Ophthalmology – work with system on NHS England High D Sandhu / S
Impact Intervention Qtrs 1 & 2 Gadhia
C Williams
3. Stroke – oversee safe transition of all acute stroke D Sandhu / A Ali
Qtrs 1 & 2
services to NGH C Williams
4. Community elective services – agree scope and procure Qtrs 1-4 L Riddaway / A Ali
- 15 -No. Deliverable By When Lead(s) / SRO
new services & S Gadhia
C Williams
5. Respiratory – delivery of RightCare identified L Riddaway / J
opportunities Qtrs 1-4 Findlay
C Williams
6. Diabetes – monitor and review impact of interim funding S Barnes / Y Javaid
Qtrs 1 & 2
C Williams
7. Circulation – delivery of RightCare identified S Barnes / Y Javaid
Qtrs 1-4
opportunities C Williams
Maternity
1. Priority workstream – Continuity of Carer; Initial work Qtr 2 Helen Adams
scope agreed and modelling started Alison Kemp
2. Priority Workstream – Community Hubs; First hub in Qtr 2 Helen Adams
place. Second hub development under discussion Alison Kemp
3. Priority Workstream – IT/Digital; Engaged with STP IT Qtr 2 Helen Adams
workstream; IT plan in development Alison Kemp
4. Priority Workstream – Mobilisation of Specialist Qtr 1 Helen Adams
Community Perinatal Mental Health Service Alison Kemp
5. Priority Workstream – Collaborative working; Starting to Qtr 4 Helen Adams
plan and deploy work force across the county Alison Kemp
6. Rebranding Maternity voices partnership – ‘Maternity Qtr 2 Helen Adams
Northants’ User/Professional Group transformation Alison Kemp
Cancer
1. Implement Faecel Immunochemical Testing (FIT) for Q3 L Dunkley
bowel cancer in Primary Care C Williams
FIT testing is a new method of collecting stool samples as
a diagnostic tool for symptomatic, low risk patients, and
provides a means of risk stratifying patients with
symptoms indicative of colorectal cancer as it detects
microscopic amounts of blood in faeces that would not
be detectable with the human eye
2. Implement elements of the National Optimal Lung Q4 L Dunkley
Pathway (NOLP) C Williams
The NOLP is a more efficient pathway with faster access
to diagnosis and treatment
3. Implement the RAPID Prostate pathway in two phases: L Dunkley
• Phase 1 mpMRI Q2 C Williams
• Phase 2 one-stop clinics to be implemented
following completion of Nottingham pilot and
evaluation (anticipate 19/20)
The RAPID pathway is a streamlined, evidence based,
fast access, one-stop imaging diagnostic pathway for
men suspected of having prostate cancer
4. Implement stratified follow up for: L Dunkley
• Breast cancer Q3 C Williams
- 16 -No. Deliverable By When Lead(s) / SRO
• Colorectal cancer Q4
Continue to deliver stratified follow up for:
• Prostate cancer Q1
Stratified pathways tailored to individual needs, offer
huge benefits to patients and the service. They will
improve the quality of life for people following
treatment for cancer through addressing their needs,
and help them to return to living their lives as positively,
healthily and quickly as possible
5. Deliver the elements of the Recovery Package for people L Dunkley
living with cancer: C Williams
• Holistic Needs Assessments Q3
• Treatment Summaries Q3
• Health & Wellbeing events Q2
• Cancer Care Reviews in Primary Care Q4
The four main interventions of the Recovery Package
listed above form part of an overall support and self-
management package for people affected by cancer
Quality
1. Improve shared learning from Serious Incidents and Qtr 2 Alison Jamson /
Serious Case Reviews Matthew Davies
2. Develop countywide Quality Improvement Strategy Qtr 3 Alison Jamson /
Matthew Davies
3. Deliver priorities set within quality strategy through Qtr 4 Alison Jamson /
team work plan Matthew Davies
4. Ensure quality standards included in all procurements, Qtr 2 Alison Jamson /
commissioning plans Matthew Davies
5. Ensure quality and safeguarding involvement in STP Qtr 2 Alison Jamson /
workstreams Matthew Davies
- 17 -4. Northamptonshire Health & Care Partnership
The Northamptonshire Health & Care Partnership (NHCP) (previously known as the Sustainability &
Transformation Partnership or ‘STP’) enters its third years of partnership working across the
statutory agencies within the Northamptonshire health and social care system, together with
representatives of primary care:
Table 3. Northamptonshire STP Partners
Northamptonshire STP Partners
NHS Corby CCG Northamptonshire City Council
Kettering General Hospital NHS Foundation Trust Northamptonshire Healthcare NHS Foundation
Trust
NHS Nene CCG The Local Medical Committee
Northampton General Hospital NHS Trust GP Federations / Superpractice
The refreshed planning guidance for 2018/19 makes it clear that system partnership arrangements
will in due course be replaced by Integrated Care Systems. The creation of the Northamptonshire
Health and Care Partnership is a key milestone on the road to the creation of an Integrated Care
System locally. Integrated Care Systems are key to sustainable improvement in health and care
through:
• The creation of robust cross-organisational arrangements to tackle the systemic challenges
facing the NHS;
• Population health management;
• Delivering more care through redesigned community and home based services; and
• Collective responsibility for financial and operational performance and health outcomes.
The Partnership seeks to work together to build on local best practice and in shaping a collective
approach to delivering health and care - now and for the future - to ensure local care is sustainable
and represents both the national priorities and the needs of our local community.
In working together to deliver the objectives of the Five Year Forward View, Five Year Forward Next
Steps and now Refreshing NHS Plans for 2018/19 guidance, the NHCP is seeking to deliver the
following objectives:
• People live longer, healthier lives;
• People live in strong and resilient families and communities;
• People have improved mental health and wellbeing;
• People can access care and support closer to home, when needed;
• Children start life healthy and stay healthy;
• Health inequalities are reduced; and
• A stronger economy and healthier workforce.
In support of this, the partnership underwent a re-set in 2017/18. This was done in line with the
updated national priorities and following the review of our local priorities, to help now focus on the
- 18 -NHCP’s priority workstreams, i.e. the most important areas for us to work together where we know
we can make a difference to improve outcomes for those we care for and be more sustainable.
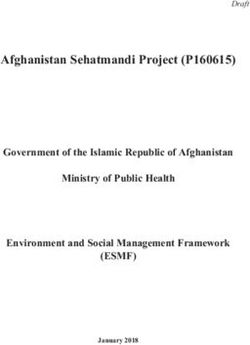
Northamptonshire Health & Care Partnership Structure
The overarching NHCP is now structured as follows:
Figure 5. Northamptonshire Health and Care Partnership Organogram
Organogram
Statutory Boards/Governing
Health and Wellbeing Board Bodies
Northamptonshire STP/ACS
Partnership Board
Collaborative
Advisory Advisory
Stakeholder Forum
Strategic Executive
Strategic Finance Group Clinical Advisory Group
STP Lead & Workstream SROs
DSU Support
includes
communication
function
Commissioning LDR Primary, Community
Urgent and Emergency
Development and Social Care
Care
Unified Acute Model Workforce
Mental Health Cancer
Accountable Care Modelling/Business
System Intelligence Health and Wellbeing Learning Difficulties
Estates
Maternity Children & Young
SYSTEM People
DEVELOPMENT SYSTEM ENABLERS
NEW CARE MODELS
Integrated Care Board/Better Care Fund
The Northamptonshire HCP comprises three portfolios - New Care Models; System Development;
and System Enablers, each of which has a series of workstreams:
Table 4. New Models of Care Workstreams
Group A Group B
Urgent and Emergency Care
Children & Young People
Primary / Community / Social Care
Maternity
(including Intermediate Care)
Health & Well-Being
Cancer
Learning Difficulties
Mental Health
Table 5. System Development & System Enabler Workstreams
System Development Enablers
- 19 -Local Digital Roadmap
Commissioning Development
Workforce
Unified Acute Model
Modelling/Business Intelligence
Accountable Care System
Estates
Each workstream is led by a SRO who is responsible for developing Workstream Definition
Documents (WDDs) setting out:
• The purpose and objectives of the workstream
• A vision statement summarising the desired future state
• Outputs, outcomes and benefits
• Scope
• Workstream management, organisation and resources
• The projects comprising the workstream
• A plan for the workstream and its constituent projects
• Controls and reporting arrangements
• Key risks and issues
• Stakeholders and how they are involved.
These WDDs remain work in progress subject to a process of continuous updating. Nevertheless,
they represent ‘statements of intent’ on the part of the local health and social care system.
New Models of Care : Workstream Definition Document Objectives
Whilst the WDDs remain works in progress, set out below is a high-level summary of what each
workstream within the New Models of Care portfolio will focus on in 2018/19:
Group A
• Urgent and emergency care
o Roll out of proactive care projects: clinical advice hub, respiratory pathways, dementia and
delirium pathway, frailty pathway
o Roll out of flow projects: ambulatory care pathways, GP led primary care assessment, multi-
disciplinary discharge planning, NWB pathway, MH Core 24, discharge to assess
• Primary/ community/ social care (including intermediate care)
o Development of an integrated model of primary, community and social care (inc.
intermediate care)
o Development of a strategic outline case for review/ approval by the Partnership Board
o Identification of implementation projects
• Cancer
o Roll out of early detection projects
o Roll out of pathways and performance projects
o Roll out of living with cancer projects
• Mental health
o A clear and agreed outcomes framework
o A set of co-produced and prioritised metrics
- 20 -o A model of care (inc. transitions through to last years of life)
o A delivery plan
o A contractual framework supporting frontline innovation
Group B
• Children and young people
o Roll out of project on services for children and young people with disabilities and complex
conditions
o Roll out of project on consistent service provision and streamlined care pathways
o Roll out of project on mental health services
o Roll out of project on early intervention services
o Roll out of project on improving outcomes for children in care.
• Maternity services
o Roll out of Better Births: LMS transformation plan
• Health and wellbeing
o Roll out of building resilient communities project
o Roll out of social prescribing project
o Rollout of prevention at scale project
o Roll out of clinical preventative services project.
The learning disability WDD will be produced in Q1 18/19.
- 21 -5. Finance
Introduction
NHS Corby CCG and NHS Nene CCG both have a strong history of delivering on their financial
targets despite working in a financially challenged health economy. The control totals across both
CCGs are forecast to be delivered again in 2017/18. This is against a backdrop of growing financial
pressures in the following areas:
• The cost of acute activity;
• Significant national increases in the cost of GP Prescribing; and
• Growth rates in Continuing Healthcare packages.
These pressures have been mitigated in year by underspends in other areas alongside the release
of contingencies and reserves. Most of these underspends and reserves are non-recurrent. Both
CCG’s have held the nationally required 0.5% risk reserve in 2017/18.
Nene CCG and Corby CCG are together the two CCG’s with the largest Distance from Target in the
Central Midlands area with -3.13% and -3.08% respectively. The average Distance from Target for
the Central Midlands area is -1.55% and the Midlands & East area is -1.56%:
Table 6. Distance from Target
Distance from Target %
North 1.59%
Midlands & East (1.56%)
London 1.50%
South East (1.22%)
South West (0.57%)
England 0.0%
Overall CCG Financial Management
The two CCGs will be working under a combined leadership team in 2018/19. The new leadership
arrangement across the two CCGs will allow us to drive efficiency and focus on commissioning that
is truly integrated around the needs of local people, in line with the expectations of the NHS Five
Year Forward View.
This new arrangement will help us harness the benefits of greater collaboration across the whole
health and social care system with CCGs, NHS organisations, local authorities and the voluntary
sector, in line with the Northamptonshire Sustainability and Transformation Partnership (STP)
footprint. The CCGs will remain autonomous constituted bodies with their own clinical
membership committed to the areas they serve but both organisations have agreed to work under
one management team to achieve the organisation control totals going forward into 2018/19.
Planning Assumptions
- 22 -The 2018/19 financial plan has been designed using a combination of national and local planning
assumptions. The key assumptions are as follows:
• Growth rates for secondary care activity have been applied that exceed the minimum national
expectations:
Table 7. Secondary Care Growth Rates
Activity %
GP Referrals 0.80%
Other Referrals 4.60%
st
1 Outpatient Appointments 6.40%
Follow-Up Outpatient Appointments 4.10%
Elective Day Cases 4.20%
Elective Ordinary Cases 0.3%
A&E Attendances 1.10%
Non-Elective 0+ Length of Stay 5.6%
Non-Elective 1+ Length of Stay 0.90%
• Growth in secondary care (non-specialist) drugs expenditure is covered through the tariff uplift;
• For primary care prescribing, growth is offset by efficiencies, guidance on reforms to drugs
prescribed over the counter and the ending of the cost pressure accruing from generic drugs in
short supply;
• Investments are included that as a minimum comply with the levels required in the GP Forward
View;
• The plan has taken into account the cost impact of changes within Healthcare Resource Group
(HRG) 4+ and the Identification Rules (IR) changes for Specialist Services;
• Allocations cover the additional costs to CCGs accruing from the delegation of Primary Care IT
Enabling Services;
• CCG Quality Premiums will be restructured in 2018/19 to provide an increased focus on non-
elective demand management (emergency admission avoidance);
• Commissioning for Quality and Innovation (CQUIN) performance thresholds will be updated for
flu vaccinations, sepsis, and reducing the use of antibiotics. For 2018/19 the 0.5% risk reserve
CQUIN will be withdrawn with the allocation added to the engagement CQUIN. Also the safe
discharge indicator for hospital providers will be withdrawn in 2018/19 with the funds spread
across the other CQUIN indicators, with this concession made as there are incentives to support
effective discharges elsewhere and to reduce financial pressures on providers; and
• The current prescribing cost pressures accruing from the generic drugs in short supply will not
continue into the next financial year at the same level.
Nene CCG & Corby CCG have been given control totals of breakeven for the 2018/19 financial year.
CCG Revised Control Totals and Business Rules for 2018/19
Whilst developing the financial plan, the CCG has adhered to NHS England business rules as
detailed in the planning guidance. The business rules and how they have been applied to the plan
- 23 -are reflected in the table below:
Table 8. NHS England Business Rules
CCG Financial Business Rules 2018/19 CCG Position 2018/19
CCGs should hold a 0.5% uncommitted The financial plan includes a 0.5%
general contingency at the start of the year to contingency at the start of the financial year
manage their in-year pressures and risks
CCGs have to plan for in-year breakeven The financial plan is based on an in-year
adjusted for draw up/(draw down) breakeven position
Mental Health Investment Standard The financial plan demonstrates compliance
with the mental health investment standard
Contracts
The CCG’s signed two-year contracts with the three main providers within the county at the
beginning of 2017/18. Contract variations will update the second year values in line with required
changes for activity trends and contractual adjustments for 2018/19.
- 24 -Financial Plans
An Income and Expenditure summary for each CCG is detailed below:
Table 9. Nene CCG Income & Expenditure
NENE CCG £000 £000 £000 £000 £000
Income 2017/18 Unmitigated QIPP QIPP Non-
2018/19
2018/19 Recurrent Recurrent
Recurrent 790,858 815,849 815,849
Non-Recurrent 2,511 515 515
Total In-Year Allocation 793,369 816,364 0 0 816,364
Expenditure
Acute 441,542 475,663 (4,911) (11,780) 459,972
Mental Health 82,061 84,929 (135) 84,794
Community 70,348 70,679 70,679
Continuing Care 49,939 53,581 (2,385) 51,197
Primary Care 114,618 113,511 (2,830) 110,681
Other Programme 22,266 30,104 (300) (7,659) 22,145
Primary Care Co-Commissioning 0 0 0
Total Programme Costs 780,773 828,468 (10,561) (19,439) 798,468
Running Costs 12,482 13,814 13,814
Contingency 0 4,082 4,082
Total Costs 793,255 846,361 (10,561) (19,439) 816,364
GAP 114 (30,000) 0
Efficiency – Nene CCG
Local Tariff £9.8m 33%
Arrangement
QIPP Schemes £12.5m 41%
Investments held £7.7m 26%
£30m 100%
- 25 -£ 000 £ 000 £ 000 £ 000 £ 000
CORBY CCG
Unmitig QIPP
QIPP
Income 2017/18 ated Non- 2018/19
Recurrent
2018/19 Recurrent
Recurrent 107,625 111,942 111,942
Non-Recurrent (94) 96 96
Total In-Year Allocation 107,531 112,038 0 0 112,038
Expenditure
Acute 59,026 60,921 (1,858) 59,063
Mental Health 9,747 9,535 (14) 9,521
Community 8,977 9,553 (8) 9,545
Continuing Care 4,618 5,691 (313) (600) 4,778
Primary Care 13,364 13,607 (260) (81) 13,266
Other Programme 288 4,052 (766) 3,287
Primary Care Co-Commissioning 9,943 10,452 10,452
Total Programme Costs 105,963 113,812 (2,453) (1,447) 109,912
Running Costs 1,549 1,565 1,565
Contingency 0 561 561
Total Costs 107,512 115,938 (2,453) (1,447) 112,038
Table 10. Corby CCG Income & Expenditure
- 26 -GAP 19 (3,900) 0
Efficiency - Corby CCG
QIPP Schemes £3.1m 79%
Investments held £0.8m 21%
£3.9m 100%
Key Financial Risks
The financial plan includes funding for a number of anticipated cost pressures. However, there are
significant risks to delivery of the financial control totals in the following areas:
• Referral To Treatment (RTT) waiting list backlogs which are currently being assessed in
conjunction with the local providers. If capacity exists to deal with this work, it could result in a
significant non-recurrent cost pressure;
• Delivery of a significant QIPP programme;
• Constraining acute activity & cost growth within the contracted financial envelope;
• The impact on Health Budgets resulting from the financial position of the Local Authority.
QIPP
The CCG’s have a combined QIPP target of £33.9m (Nene CCG £30m, Corby CCG £3.9m). The
commissioners have identified schemes that address £25.4m of the gap, leaving £8.5m to be
covered by withholding investments until further schemes are fully developed. £13m (38%) of the
identified schemes are recurrent schemes.
Approach to Efficiency
The CCGs are using the concepts and ideas from NHS RightCare, the Menu of Opportunities, the
NHCP and local initiatives to design the transformation required to meet the financial challenge.
The CCGs have implemented a gateway process to enable each programme to manage its own
pipeline with a review required at each gateway. Gateways 1-3 ensure scarce resource (staff time
and funding) is prioritised for the schemes that represent the best combination of benefit and risk.
Gateways 4-5 ensure maximum value is secured from the CCGs’ investment of staff time and
funding.
The gateways are shown below:
Figure 6. CCG Gateway Process
- 27 -You can also read