THE IMPACT OF WOMEN FOR WOMEN INTERNATIONAL'S ECONOMIC AND SOCIAL EMPOWERMENT PROGRAM IN THE DEMOCRATIC REPUBLIC OF CONGO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Photo credit: Ryan Carter (2017)
THE IMPACT OF WOMEN FOR WOMEN INTERNATIONAL’S
ECONOMIC AND SOCIAL EMPOWERMENT PROGRAM IN THE
DEMOCRATIC REPUBLIC OF CONGO
SUMMARY OF FINDINGS*
Background Women for Women International’s social and economic
The Democratic Republic of Congo (DRC) has faced conflict and empowerment program:
instability for over 25 years, exacerbating poverty and gender • Increased women’s savings, assets, and access to
inequalities. Despite the abundance of valuable natural resources, credit;
DRC is one of the poorest, least-developed, and gender-inequitable • Increased women’s engagement with
places on Earth, ranking 179th out of 189 countries on both the entrepreneurial work and net earnings;
Human Development Index and Gender Inequality Index1 [1].
• Improved women’s mental health and household
Almost 70% of the population live below the international poverty
diet diversity;
line of US $1.90 a day, and over 6 million children under five suffer
from chronic malnutrition [2][3]. • Improved women’s agency, self-confidence and
Decades of conflict have claimed over 5.4 million lives and participation in household decision-making, and
displaced millions more, primarily in the eastern provinces [4]. In increased social support.
South Kivu, continued insecurity and a lack of governance have * Results are preliminary and may change after further analysis.
challenged progress, disrupted markets, and destroyed assets.
90% of informal entrepreneurs in South Kivu live below the poverty
line and the vast majority are women: women are 6.7 times more
likely than men to be “survivalist” entrepreneurs, meaning they
operate low-growth businesses [5]. women aged 15 and older is 40% compared to 17% for men [2].
Women’s vulnerability to poverty is reinforced by a complex web Women face discrimination and abuse stemming from harmful
of barriers. Women lack ownership of assets, personal income, gender norms. In South Kivu communities, patriarchal “customary”
and often do not receive inheritances. A married woman often norms take precedence over national legal protections for women.
needs her husband’s permission to work, open a bank account, Women are not supposed to speak in front of men and are seen as
obtain credit, start a business, or travel [6]. 68% of women in South second-class citizens. Conflict exacerbates these abuses and adds
Kivu did not complete primary school, and the illiteracy rate for others, including the prolific use of rape as a “weapon of war” and
the normalization of sexual violence against women (VAW) among
1 The Gender Inequality Index, calculated as part of the United Nations
Development Programme’s Human Development Report, is an index that
the civilian population [7]. Almost half of the women in South Kivu
reflects gender-based inequalities in reproductive health, empowerment, have experienced physical violence and 35% have experienced
and economic activity. sexual violence in their lifetime [2].
PROGRAM DESCRIPTION STUDY METHODS
Women for Women International (WfWI) works with the most WfWI worked with researchers at the University of Washington
marginalized women in conflict-affected countries to help them move and University of Texas at Austin and the data collection firms
from poverty and isolation to self-sufficiency and empowerment. Marakuja Kivu Research and the Innovative Hub for Research in
WfWI has been implementing its Signature Program (Figure 1), an Africa (IHfRA) to conduct a 24-month randomized control trial (RCT)
economic and social empowerment program, in North and South in four communities in South Kivu province. The primary objective of
Kivu provinces in DRC since 2004. the study was to measure the impact of WfWI’s Signature Program
on women’s livelihoods, savings and assets, social empowerment,
wellbeing, and social assets one year after program completion.
Figure 1. Women for Women International Signature Program Researchers also examined how men’s engagement activities for
male spouses, partners, and other household members impacted
women’s economic and social empowerment outcomes.
From July to September 2017, WfWI screened and recruited
2039 potential program participants in Kamanyola, Ciherano-
Luciga, Nyangezi, and Mumosho to be research respondents.2
All participants were given an explanation of the study and their
participation in the research and were told they could decline
participation or withdraw from the study at any time. Participants
provided informed consent via signature or thumb print on a paper
consent form, and then were interviewed for baseline.
Researchers assigned participants to training groups of 25 by
location, which were cluster-randomized into treatment arms. 1000
women were randomly allocated to the treatment arm, and 1039
women were allocated to the control group (Figure 2). Women in the
treatment group were further randomized into two arms: the MEP
arm, where a spouse or male family member participated in men’s
engagement programming during the trial, or the no MEP arm.
This integrated, rights-based program aims to build women’s
self-reliance in every aspect of life: economic stability, health and Figure 2. Evaluation flowchart
wellbeing, family and community participation and decision making,
and social networks. The bundled approach supports social and 2039 female respondents
completed baseline survey
economic empowerment through:
1. Foundational training in modules that include the value of
women’s work, ways to save money, ways to earn income and Randomization of groups into
study arms
improve income-generating activities, basic business skills, ways
to improve health and wellbeing, women’s rights and prevention
of VAW, strategies to make decisions and negotiate, civic action 1000 female 1039 female
respondents in respondents in
and advocacy, social networks, and safety nets; treatment arm control arm
2. Skill-building in numeracy and a chosen vocational skill (e.g.,
agriculture, sewing); 500 women randomized 500 women
to Men’s Engagement randomized to no
3. Resource provision in the form of a monthly cash stipend (US Program (MEP) arm MEP arm
$10), formal and informal savings vehicles (e.g., village savings
and loans associations (VSLAs), microfinance institutions), and
WfWI Signature Program (12 months)
referrals to health, legal, and financial services; and
4. Connections to other women through safe spaces for women
MEP with participant spouses 12 months
to learn and share together, women-led social and economic or household members
groups, and a letter exchange with international supporters. (4 months)
Over 12 months, participants are involved in two to five hours
of programming weekly, delivered to groups of 25 women in
community-based training centers. The program components are
1887 respondents completed midline survey
biweekly social empowerment training sessions (24 sessions),
weekly numeracy classes during months three and four (6 sessions), 12 months
weekly business skills training during months four through twelve
1793 respondents completed endline survey, one
(30 sessions), and intensive vocational skills sessions for months year post-graduation
seven through nine (up to 50 hours over 12 weeks). Participants also
receive training to set up their VSLAs, which then meet weekly.
WfWI also provides men’s engagement programming (MEP) to
encourage men to become active allies in support of women’s social
and economic empowerment and rights. As part of this trial, male
community leaders were trained to share knowledge and then 2 Standard eligibility criteria for participation in WfWI’s program include:
facilitated 16 weekly discussion groups with the women’s male (1) experience with war/conflict (e.g. surviving violence, being displaced);
spouses, partners, or other household members on topics including (2) social vulnerability (e.g. poorer-than-average living conditions, facing
restrictive traditional practices, or no or limited education); (3) economic
women’s economic empowerment, domestic violence, women’s vulnerability (e.g. extreme poverty, unemployment or limited to high risk or
rights, and women’s health. Couples identified by WfWI staff survivalist occupations); (4) motivation to participate in the full 12 month
members as high-risk for disputes or violence were also invited to program; and (5) ability to participate (e.g. family support, adequate health).
join one couples dialogue session, a two-hour session with up to 25 Those incapacitated because of poor mental health or very severe disability
were ineligible as they could not fully benefit from the intervention. In this
couples on topics such as roles and responsibilities in a marriage, research study, an additional criterion was that women should be aged 18 to
women’s rights (e.g., inheritance), civil registration, and making 55, and efforts were made to enroll only one household member in the trial to
commitments to reduce household conflict. address spillover concerns.
2
The 1000 treatment arm participants started the Signature Program in August and October 2017. For the 500 participants in the MEP arm,
male household members started four months of MEP part-way through the Signature Program. Control arm participants received no WfWI
intervention during the trial period and were placed on a waitlist to receive programming after the study ended.
Study participants were interviewed three times: at baseline, midline (12 months after baseline, at completion of the Signature Program),
and endline (24 months after baseline, one year after completion of the Signature Program). The endline survey had an 88% completion rate.
At each data collection point, participants completed a 90- to 120-minute survey administered in-person in Kiswahili or Mashi by trained
enumerators using the SurveyCTO platform and Android tablets. Marakuja Kivu Research led the data collection activities. In addition, 48
randomly selected individuals were interviewed in depth at endline, including 32 women who had been WfWI Signature Program participants
and 16 men who were MEP participants.
RESULTS Photo credit: Ryan Carter (2017)
Baseline findings about study population
At baseline, the average study participant was 33 years old, and the average household had 6.4 members. 67% of the study participants
were married or cohabitating with a partner. Only 14% of the study population had attained education higher than primary school, and 57%
of the survey respondents were illiterate. 41% of respondents reported that they had worked for pay, profit, or gain in the past seven days.
Across all respondents, average weekly earnings were $1.57.3 63% of women agreed that a man should have the final say on household
decisions, and 62% of respondents agreed a man could beat his wife for refusing sex.
The communities in this trial faced conflict and insecurity, market instability, and a nearby Ebola outbreak. Nearly all respondents (98%)
reported experiencing large increases in the price of daily goods in the past year. Many respondents also faced an illness of any household
member lasting over one month (75%) and unemployment of a household earner for over one month (48%). In addition, 27% of respondents
reported experiencing an incident of violence within her household and/or community in the prior 12 months. WfWI targets and serves an
extremely marginalized type of population, and these baseline figures present a consistent picture of women who are living in extreme
poverty, socially marginalized, and affected by conflict.
Study results
This section compares outcomes for the overall treatment group (both the MEP and no MEP arms together4 ) and the control group one year
after the end of the program. For each outcome with statistically significant findings, the mean or prevalence in the treatment and control
groups and the p-value of their difference are presented.5
3 All monetary results are reported in USD. The following exchange rates were used: 1600 CDF to 1 USD (2017 and 2018); 1696 CDF to 1 USD (2019).
4 Using this approach, all participants who partook in the WfWI Signature Program are included in the overall treatment group, including 500 participants in the MEP
arm and 500 participants in the no MEP arm. There were not significant differences across outcomes between the MEP and no MEP arms—the reported results are
driven by participation in the Signature Program.
5 Lower p-values indicate a higher level of confidence that the difference between the treatment and control groups is not due to chance. For example, a p-value
lower than 0.05 indicates greater than 95% confidence and is considered very strong evidence. Likewise, a p-value between 0.05 and 0.10 indicates greater than
90% confidence and is considered moderately strong evidence.
3
Women increased their income and shifted towards entrepreneurship. Women who had been through the WfWI intervention had weekly gross earnings 1.6 times higher than women in the control arm at endline ($2.75 vs. $1.70; p
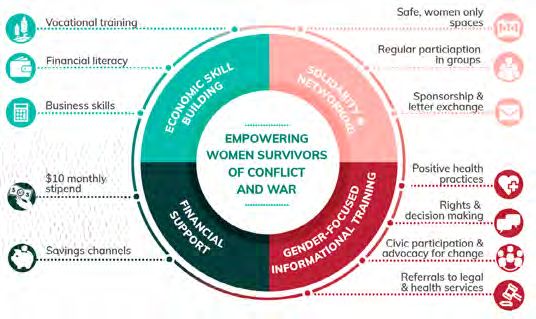
Figure 5. Percent
Figure 5. Percentofofparticipants
participants with
with any
any anxiety
anxiety Figure 6. Average
Figure 6. AverageHousehold
Household Diet
Diet Diversity
Diversity Scores
Scores (0-14)
(0-14)
diagnosis (GAD-7)
diagnosis (GAD-7)
Women’s overall gender attitudes and rates of intimate partner violence did not change in the study timeframe. More women in the
treatment arm held the attitude that women can be community leaders, compared to women in the control arm (93% vs. 84%, p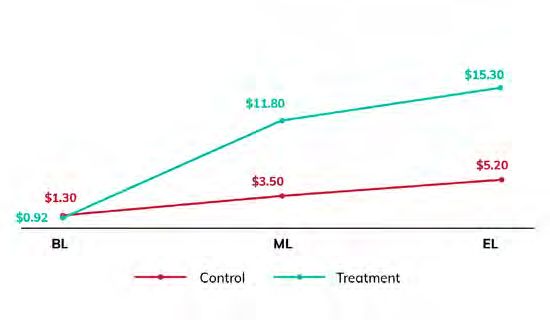
Photo credit: Ryan Carter (2017)
Study limitations
The study was conducted in a fragile setting, and there was an study demonstrate the effectiveness of an integrated approach
overall 12% attrition rate at endline, much of which was caused by even in a fragile and conflict-affected situation (FCAS) in which
participants who were ill or migrated to new locations. However, participants simultaneously faced poverty, ongoing conflict and
this rate is not significantly different between study arms: 13% instability, lack of governance and basic infrastructure, market
in the control group and 11% in the treatment group. Individuals shocks, an Ebola outbreak, and more.
in the treatment and control arms of the study lived in the same Although this study did not seek to unpack the bundled program
communities, and the research took place in communities and interrogate which components are driving which change,
with existing WfWI community advocacy activities. Therefore, WfWI believes the following integrated elements are critical to the
respondents in the control group may have been exposed to success of this approach:
elements of WfWI interventions, reducing the differences between 1. Building a women-driven program. WfWI pledges to meet
treatment arms. 67% of women in the control group reported women where they are and does so by engaging with them to
knowing someone in the WfWI Signature Program, and 12% shape programming that is based on their stated needs and
reported receiving information or lessons from WfWI program respecting the strength and resilience within them.
participants over the course of this study. 2. Laying economic foundations. Women selected for the program
For some outcomes, such as mental health and empowerment, have often missed out on formal education, so WfWI provides
Western survey tools may not have translated well to this context; training on basic foundational knowledge including numeracy,
further research is required to understand local definitions and saving money, goal-setting, and budgeting as well as vocational
manifestations of concepts such as depression, anxiety, and and business skills. In FCAS, savings and assets are essential
agency [11][12][13]. Lastly, social desirability bias, whereby both for coping with economic shocks and helping to start or
participants learn the “right” answer to questions, can manifest grow businesses. The bundled approach helps women achieve
in this type of study, particularly when questions are repeated economic self-sufficiency and withstand economic shocks.
multiple times over a long period. However, given that control
3. Integrating gender-transformative programming into poverty
group respondents were waitlisted to receive WfWI programming
alleviation efforts. Women’s poverty in FCAS is compounded
after this trial completed, it seems likely that a desire to please the
by deep-rooted gender norms that perpetrate gender
enumerator would apply equally to treatment and control groups.
discrimination. WfWI’s bundled approach supports building
Reflections on results women’s social power with training on gender equality, rights
and decisionmaking, leadership, communication, advocacy, and
This study demonstrates that an integrated social and economic health and wellness.
empowerment program can improve the wellbeing of marginalized 4. Connecting women through networks. There is power in
women in conflict-affected eastern DRC. These findings contribute women coming together to support one another. Group-based
to an extensive and growing evidence base on the success of programming and VSLAs create social support networks
“big push” bundled anti-poverty interventions such as graduation for women, reducing isolation, providing comfort and safety
approaches, especially evinced by significant and sustained in emergencies, and leading to opportunities for community
gains across a range of economic outcomes and indicators [14] engagement and collective action.
[15]. However, to date, quantitative evaluations of graduation
approaches have shown limited or mixed impacts on women’s Marginalized women are resourceful and resilient agents of
empowerment outcomes [15][16]. The results from this study change. With the right financial, technical, and social support,
demonstrate that WfWI’s combined focus on poverty alleviation women facing conflict, poverty, and oppressive gender norms can
and gender transformation leads to gains across economic and change their ways of working and earning money, improve their
social domains, including agency, participation in decision-making, health and wellbeing, increase participation in their households and
anxiety, diet diversity, and social support. The gains seen from this communities, and grow their power.
6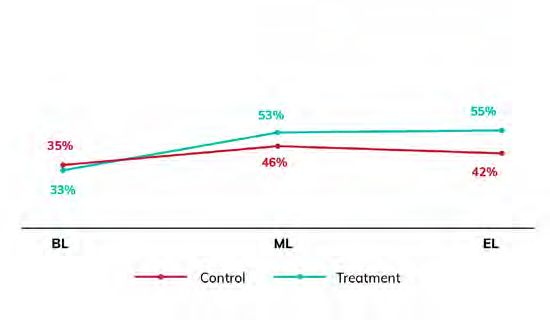
Recommendations for future programming to References
empower women
1. UNDP, “Human Development Report 2019: Beyond income, beyond averages,
This study also provides a roadmap for WfWI’s growth and for researchers, beyond today: Inequalities in human development in the 21st century,” United
practitioners, and donors in the wider development community seeking to Nations Development Programme, New York, NY, 2019.
uplift women at the intersection of conflict, poverty, and gender inequality. 2. MPSMRM, Ministère de la Sante Publique (MSP) and ICF International, “Enquête
Démographique et de Santé en République Démocratique du Congo 2013–
First, while the increase in average earnings from the WfWI Signature 2014,” Rockville, MD, 2014.
Program is substantial, it is important that programs look beyond 3. The World Bank, “Data: Democratic Republic of Congo,” 2018. [Online]. Available:
https://data.worldbank.org/country/congo-dem-rep. [Accessed 2020].
averages to identify and support women who may need an additional
4. Council on Foreign Relations, “The Eastern Congo: a CFR InfoGuide
boost to increase their earning potential. For low or moderate earners, Presentation,” 2018. [Online]. Available: https://www.cfr.org/interactives/
more individualized tracking and tailored support by staff or mentors may eastern-congo#!/?cid=soc-at-interactive-the_eastern_congo_
infoguide-121015. [Accessed 2020].
be needed [16]. Further, methodologies that capture the complexity of
5. F. M. Adoho and D. Doumbia, “Informal Sector Heterogeneity and Income
irregular or seasonal earnings data are important to employ in research Inequality: Evidence from the Democratic Republic of Congo,” Washington, DC,
that seeks to understand the realities of micro-entrepreneurs; surveys 2018.
relying on weekly or monthly recall to record the earnings of intermittent 6. L. Davis, P. Fabbri and I. M. Alphonse, “DRC Gender Country Profile, 2014,”
Swedish Embassy, DRC: Kinshasa, 2014.
or seasonal workers can narrow a study’s view of a population’s earnings
7. I. Bjorkhaud and M. Boas, “Men, women and gender-based violence in North Kivu,
potential. DRC,” Fafo, 2014.
Second, there is limited research studying links between women’s 8. K. Kroeke, R. L. Spitzer and J. B. Williams, “The PHQ-9.,” Journal of general internal
empowerment and mental health, especially in conflict settings [17]. This medicine, vol. 16, no. 9, pp. 606-613, 2001.
9. R. L. Spitzer, K. Kroenke, J. B. Williams and B. Lowe, “A brief measure for assessing
study found high rates of anxiety and depression among participants generalized axienty disorder: the GAD-7,” Archives of internal medicine, vol. 166,
and provided promising findings in the reduction of the prevalence of no. 10, pp. 1092-7, 2006.
anxiety symptoms, but not in reductions of participants with depressive 10. M. Angelucci, “Love on the rocks: Domestic violence and alcohol abuse in rural
Mexico,” The BE Journal of Economic Analysis and Policy, p1-43., 2008.
symptoms. Mental health services are extremely limited in this setting, so
11. E. E. Haroz, M. Ritchey, J. K. Bass, B. A. Kohrt, J. Augustinavicius, L. Michalopoulos,
programmers should consider a range of support strategies to promote M. D. Burkey and P. Bolton, “How is depression experienced around the world?
improved mental health and address service gaps. These include training A systematic review of qualitative literature,” Soc Sci Med, vol. 183, pp. 151-162,
2017.
staff in psychosocial support and psychological first aid, employing
12. L. J. Kirmayer, “Cultural variations in the clinical presentation of depression and
screening tools and referrals to service providers where possible, teaching anxiety: implications for diagnosis and treatment,” Journal of Clinical Psychiatry,
coping and support strategies, and leveraging targeted technical vol. 62 Suppl 13, pp. 22-28, 2001.
assistance to sensitize populations and provide services [18][19]. 13. R. Glennerster, C. Walsh and L. Diaz-Martin, “A Practical Guide to Measuring
Women’s and Girls’ Empowerment in Impact Evaluations,” JPAL, Cambridge, MA,
Third, this study showed that despite outcomes on the theorized 2018.
pathway to violence reduction being impacted [20], reported experiences 14. A. Banerjee, D. Karlan, R. Osei, C. Udry and H. Trachtman, “Unpacking a Multi-
of intimate partner violence were not reduced. The program did not set Faceted Program to Build Sustainable Income for the Very Poor.,” Innovations for
Poverty Action, New Haven, CT, 2018.
out to reduce violence in its original design, and WfWI is convinced that 15. A. Banerjee, E. Duflo, N. Goldberg, D. Karlan, R. Osei, W. Pariente, J. Shapiro, B.
intentional violence prevention programming that targets household Thuysbaert and C. Udry, “A multifaceted program causes lasting progress for the
members and community-level social norm change is needed going very poor: Evidence from six countries,” Science, vol. 348, no. 6236, p. 1260799,
2015.
forward [21]. Significant research in the last decade has been dedicated 16. S. Laszlo, “The gender transformative potential of graduation programs,”
to understanding strategies to reduce violence against women, and it Fundacion Capital, 2019.
is critical that practitioners begin to apply these tested approaches to 17. V. Baranov, S. Bhalotra, P. Biroli and J. Maselko, “Maternal Depression, Women’s
Empowerment, and Parental Investment: Evidence from a Randomized
poverty alleviation programs [22][23]. Controlled Trial,” American Economic Review, vol. 110, no. 3, pp. 824-859, 2020.
Fourth, the study finds that the examined level of men’s engagement 18. C. Lund, M. De Silva, S. Plagerson, S. Cooper, D. Chisholm, J. Das, M. Knapp and
programming was not sufficient to lead to additional average gains for V. Patel, “Poverty and mental disorders : breaking the cycle in low-income and
middle-income countries,” The Lancet, vol. 378, no. 9801, pp. 1502-1514, 2011.
women participants of WfWI’s Signature Program. Since this trial began
19. M. Kamali, M. Munyuzangabo, F. J. Siddqui, M. F. Gaffey, S. Meteke, D. Als, R.
in 2017, WfWI has improved and expanded its activities to engage P. Jain, A. Radhakrishnan, S. Shah, A. Ataullahjan and Z. A. Bhutta, “Delivering
with men, including training community and religious leaders, hosting mental health and psychosocial support interventions to women and children
in conflict settings: a systematic review,” BMJ Global Health, vol. 5, no. 3, p.
community forums, and holding men’s discussion groups, based on e002014, 2020.
global evidence for best practices in terms of types of activities, duration 20. A. M. Buller, A. Peterman, M. Ranganathan, A. Bleile, M. Hidrobo and L. Heise, “A
of engagement, topics to be covered, and frameworks to employ [24]. Mixed-Method Review of Cash Transfers and Intimate Partner violence in Low-
and Middle-Income Countries.,” The World Bank Research Observer, vol. 33, no.
More effective men’s engagement programming is required to influence 2, pp. 218-258, 2018.
women’s outcomes [25]. 21. A. Gibbs, J. Corboz, E. Chirwa, C. Mann, F. Karim, M. Shafiq, A. Mecagni, C.
Finally, the results underscore the difficulty associated with shifting MaxwellI-Jones, E. Noble and R. Jewkes, “The impacts of combined social and
economic empowerment training on intimate partner violence, depression,
deeply engrained gender attitudes, even when many other social and gender norms and livelihoods among women: an individually randomised
economic indicators showed significant improvements. Individual controlled trial and qualitative study in Afghanistan,” BMJ Global Health, vol. 16,
no. 5(3), p. e001946, 2020.
attitudes about gender are intrinsically linked to gender norms; changing
22. A. Kerr-Wilson, A. Gibbs, E. McAslan Fraser, L. Ramsoomar, A. Parke, H. M. A.
individual attitudes requires investment in shifting the beliefs, attitudes, Khuwaja and R. Jewkes, “A rigorous global evidence review of interventions to
behaviors, and norms across a community [26]. Since 2017, WfWI has prevent violence against women and girls,” What works to prevent violence and
girls global programme, Pretoria, South Africa, 2020.
increased community-oriented programming, such as training women as
23. R. Jewkes, S. Willan, L. Heise, L. Washington, N. Shai, A. Kerr-Wilson and N.
community advocates [27]. It is critical for programs seeking to empower Christofides, “Effective design and implementation elements in interventions
women to foster an enabling environment that respects women’s rights to prevent violence against women,” What Works to prevent violence against
women and girls a global program, Pretoria, South Africa, 2020.
and encourages them to raise their voices.
24. ICRW, “Gender equity and male engagement: It only works when everyone
Women in FCAS like DRC are often forgotten and risk being further plays,” International Center for Research on Women, Washington, DC., 2018.
left behind. They face multiple and intersecting barriers to their social 25. J. Vaillant, E. Koussobe, D. Roth, R. Pierotti, M. Hossain and K. L. Falb, “Engaging
and economic empowerment including extreme poverty, social exclusion men to transform inequitable gender attitudes and prevent intimate partner
violence: a cluster randomised controlled trial in North and South Kivu, Democratic
and widespread gender discrimination. Bundled approaches that aim to Republic of Congo,” BMJ Global Health, vol. 5, no. 5, p. e002223, 2020.
promote women’s social and economic inclusion must directly address 26. Community for Understanding Scale Up (CUSP), “Social Norm Change at Scale:
these barriers by integrating gender-transformative programming CUSP’s Collective Insights,” CUSP 2018 Case Study Collection, 2018.
27. Women for Women International, “Change Agents.” [Online]. Available:
into their approaches, directly investing in women’s knowledge, skills, https://www.womenforwomen.org.uk/work-we-do/our-programmes/change-
wellbeing and power and placing a strong emphasis on changing power agents. [Accessed 2020].
dynamics in the household and community. This kind of approach is
needed to ensure that women’s economic and social empowerment is
attainable and sustainable.
7
Photo credit: Ryan Carter (2017) SUGGESTED CITATION Noble, E., Ascencio, L., Wilondja, T., Mateba, A., Angelucci, M., Heath, R. (2020). The Impact of Women for Women International’s Economic and Social Empowerment Program in the Democratic Republic of Congo. Washington DC: Women for Women International. ACKNOWLEDGEMENTS The WfWI intervention trial was led by Dr. Rachel Heath, University of Washington, Dr. Manuela Angelucci, University of Texas at Austin, and Eva Noble, WfWI. The research team would like to first thank the participants of this study for sharing their time and experiences. Conducting an RCT in a conflict setting requires skill, local expertise, flexibility and creativity. For all of this and more, we thank the WfWI program implementation staff in the DRC, led by Abdoulaye Toure, Aloys Mateba, Thomas Wilondja, Ghislaine Maombi, Yvette Mudumbi, Gedeon Bamuleke, and Chantal Kizungu, and the data collection teams, Marakuja Kivu Research and Innovative Hub for Research in Africa (IHfRA), led by Adama Kabore and Aimable Amani. Last, we thank Liliana Ascencio, Anna Mecagni, Sabreen Alikhan, and all others who contributed to the analysis and write up of this project. Women for Women International works with the most marginalized women in conflict-affected countries to help them move from poverty and isolation to self-sufficiency and empowerment. WfWI has worked with over 500,000 women across eight countries since 1993. Further information about the project is available at: www.womenforwomen.org. This research was funded by the Ministry of Foreign Affairs of the Netherlands and BlackRock. The funds were managed by Women for Women International. This brief draws on the findings from this original research; however, the views expressed do not necessarily reflect the official views of the Ministry of Foreign Affairs of the Netherlands, BlackRock, University of Washington, or University of Texas at Austin.
You can also read