The features psoriasis challenges in aesthetic care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

REVIEW Rheumatol. Forum
2023, vol. 9, No. 1, 29–35
Copyright © 2023 Via Medica
ISSN: 2720-3921, e-ISSN: 2720-3913
DOI: 10.5603/RF.2023.0006
www.journals.viamedica.pl
Tetyana Waldheim , Anna Moska-Kula, Ewa Mojs
Department of Clinical Psychology, Poznan University of Medical Sciences, Poznan, Poland
The features psoriasis challenges
in aesthetic care
and, therefore, is difficult to treat locally. Psoriasis of
ABSTRACT
the scalp is difficult to treat with local and photother-
apy, due to the need for specific hair and scalp care.
Psoriasis can affect many areas of the body, respec- Palms and soles often have particularly thick psoria-
tively; treatment should be directed to the affected sis plaques, which can interfere with the absorption
areas according to their localization. The most dif- of topical therapy and resist phototherapy. Patients
ficult in treatment and aesthetic care are considered with predominantly palmar-plantar disease often do
to be psoriasis of the nails, scalp, and palmar-plantar not respond to several treatments, and many require
localization. These areas are visible all the time and combination therapy to control the disease. Collec-
well-groomed condition is of great importance for tively, psoriasis of the nails, scalp, and palmar-plan-
women. This article is devoted to the analysis of tar psoriasis are considered complex conditions and
data on the peculiarities of care and the complexities often do not respond to standard treatment protocols
of the treatment of psoriasis of aesthetic areas. Nail and require aesthetic medicine measures.
psoriasis is difficult to treat with topical therapy since
Rheumatol. Forum 2023, vol. 9, No. 1: 29–35
the remedy must be optimized for penetration into the
nail and surrounding tissues. Part of the inflamma- KEY WORDS: nail psoriasis; head psoriasis; plaque
tion in nail disease is located deep in the nail matrix psoriasis; aesthetic medicine; phototherapy
in psoriasis etiology and the presence of which
INTRODUCTION
predisposes to the development of the dis-
Nowadays psoriasis is known as a systemic ease. In particular, the antigens HLACw6 and
immune-associated disease of a multifactorial HLADR7 are more often detected in patients
nature with a dominant role in the develop- with psoriasis. The provoking factors include
ment of genetic factors, characterized by ac- psychoemotional overstrain, chronic infec-
celerated proliferation of epidermocytes and tions, more often streptococcal, alcohol abuse,
a violation of their differentiation, immune re- and taking medications, such as lithium salts,
actions in the dermis and synovial membranes, beta-blockers, chloroquine, oral contracep-
an imbalance between pro-inflammatory and tives [2].
anti-inflammatory cytokines, chemokine, Psoriasis is often combined with systemic
which included frequent pathological changes diseases, including metabolic syndrome, dia-
in the musculoskeletal system. Psoriasis is one betes mellitus type II, coronary heart disease,
of the most common skin diseases and occurs arterial hypertension, and pathology of the
in 1–2% of the population of developed coun- hepatobiliary system.
tries [1]. The diagnosis of psoriasis is established Adres do korespondencji:
Hereditary predisposition, disorders of on the basis of the clinical picture of the dis- Anna Moska-Kula, MD
the immune, endocrine, and nervous systems, ease, the detection of symptoms of the psori- Department of Clinical Psychology,
Poznan University of Medical Sciences
and adverse effects of environmental factors atic triad, the presence of the Koebner phe-
Bukowska 70
are important in the development of psoria- nomenon in the progressive stage. In some 60–812 Poznań, Poland
sis. A number of genes have been described cases, a histological examination of the biopsy e-mail: anna_kula88@wp.pl
29
of the affected skin is carried out to confirm infiltration. The intensity is estimated from
the diagnosis. Morphological changes are 0 (absence of a sign) to 4 (maximum degree
characterized by pronounced acanthosis of of manifestation). After that, for each area,
the epidermis with a characteristic flask-like its index is determined by the formula: (ery-
expansion of the epidermal outgrowths down- thema with peeling and infiltration) × degree
wards and thinning of the epidermis above the of lesion × weight coefficient of the area. The
tips of the elongated papillae of the dermis, weight coefficient of the area corresponds
violation of keratinization processes in the to the surface area of the skin: 0.4 — legs,
form of parakeratosis and disappearance of 0.3 — trunk, 0.2 — arms, 0.1 — head. Thera-
the granular layer. During the progression of peutic tactics of management of patients with
the disease, clusters of neutrophilic leukocytes psoriasis depending on the value of the calcu-
(Munro microabcesses) are found in the stra- lated PASI:
tum corneum and in the parakeratosis zone. — intervention is required PASI > 60%;
Inflammatory infiltrates of varying degrees — intervention is recommended by PASI
of intensity from lymphocytes, histiocytes, 30–60%;
and single neutrophil leukocytes are detected — intervention is not recommended by
around the convoluted full-blooded capillar- PASI < 30%.
ies of the papillary dermis [3]. After calculating the index for each of
Psoriasis can affect many areas of the their four areas, the obtained indicators are
body and treatments should target the areas of summarized and a total PASI total index is
involvement. The main purpose of the article obtained. There is another system for evalu-
was to analyse challenged features in nail and ating the effectiveness of therapy for psoria-
scalp psoriasis in thorough aesthetic care. sis, when a decrease in the PASI index on the
background of treatment from the initial 25%
DIAGNOSTIC METHODS FOR THE DIFFERENT is regarded as ineffective, from 25 to 49% is
TYPES OF PSORIASIS a slight improvement, from 50 to 74% is an
improvement, more than 75% is a significant
The index of prevalence and severity of improvement. When analyzing the features of
psoriasis PASI (Psoriasis Area and Severity psoriasis of the nails and head, the method de-
Index) is the main tool for determining the se- scribed above was used, which also helped in
verity of psoriasis. The use of the index allows evaluating the treatment effectiveness of dif-
an objective assessment of the effectiveness of ferent psoriasis types.
the therapy and ideally should be calculated
before, during, and after the end of the course MANAGEMENT OF NAIL PSORIASIS
of therapy.
The PASI index is represented by an inte- Our investigation started with nail pso-
ger from 0 (absence of illness) to 72 (the most riasis disease because it is difficult to treat
severe course) and reflects the area of the le- with topical therapy, as the vehicle must be
sion, taking into account the intensity of mani- optimized to penetrate the nail and surround-
festations of clinical signs, such as erythema, ing tissues.
the intensity of peeling and infiltration. There Approximately 50% of psoriasis patients
are several modifications to the calculation of have some nail involvement and the life-
the PASI index, however, according to most time incidence of nail disease is estimated at
authors, the scale that takes into account the 80–90%. Nail disease may rarely be the only
three above clinical signs is considered to be manifestation of psoriasis. Nail psoriasis is
classical. associated with higher overall disease sever-
To determine the PASI index, the pa- ity and female gender. With psoriatic lesions
tient’s body is conditionally divided into four of the nail matrix, there are: leukonychia,
areas [legs — 40% of the total surface of the a symptom of a thimble, red spots in the lunu-
human skin, trunk (chest, abdomen, back) la area, and lines are characteristic horizontal
— 30% of the skin surface, arms — 20% and furrows that are the result of dystrophic de-
head — 10%]. Each of these 4 areas is evalu- struction of the nail plates. With psoriasis of
ated separately — from 0 to 6 points, depend- the nail, patients often demonstrated such nail
ing on the degree of damage. Then, for each changes: spot hemorrhages in the distal third
area, the intensity of each of the 3 clinical signs of the nail plate, subungual hyperkeratosis is
is evaluated — erythema, peeling intensity and a deformation of the nail due to keratinization
30 Rheumatology Forum 2023, vol. 9, No. 1of the nail bed, while the nail at the edge seems psoriasis may be a predictor of joint disease
to rise and thicken due to a large number of developing later in life. PsA may involve the
scales, onycholysis, the symptom of an oil stain distal interphalangeal joints and the anatomic
is thatteardrop-shaped spots of yellow-brown link between these joints and the nail unit may
color appear under the nail plate. Moreover, result in nail changes. Fingernail psoriasis, due
with psoriasis of the periarticular region, par- to its visibility and impacts on function, is more
onychia develops — inflammation of the peri- problematic for many patients compared with
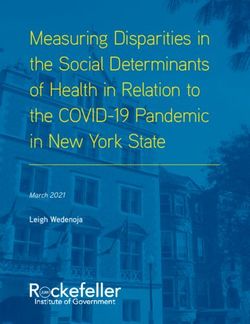
articular roller. Importantly, nail psoriasis can toenail disease [5]. The nails with psoriasis
cause significant pain, discomfort, and embar- without arthritis after treatment are demon-
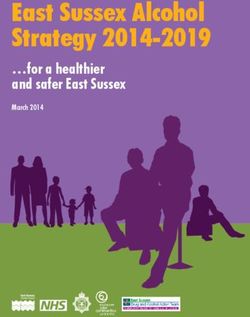
rassment, leading to impairment in quality of strated on Figure 1 and 2.
life and work function [4]. Additionally, psoriatic toenails are of-
There is a strong correlation of nail pso- ten secondarily infected with dermatophytes,
riasis and psoriatic arthritis (PsA). Psoriatic which may complicate treatment assessment.
arthritis patients have rates of nail disease as For these reasons, most studies evaluate fin-
high as 70% and there is evidence that nail gernail psoriasis alone [6].
Figure 1. Fingernail psoriasis
Figure 2. Toenail psoriasis
Tetyana Waldheim et al. The features psoriasis challenges in aesthetic care 31Clinically, nail disease has many different asis, based on published data for the treatment
presentations which depend on the location of nail psoriasis and expert opinion where data
of the inflammatory process. Nail pitting, the is lacking, has been previously published by the
most common finding in nail psoriasis, nail Medical Board of the National Psoriasis Foun-
dystrophy, and leukonychia is due to nail ma- dation and is summarized here. All psoriasis
trix involvement. patients should be evaluated for nail disease
One recent study demonstrated that nail and the extent to which their nail disease con-
clippings of clinically uninvolved nails from pa- tributes to the overall disease burden.
tients with psoriasis may show abnormalities, Nail disease should be classified as mild
thus subclinical nail disease exists. The meth- and poses no functional impact on the patient.
ods of reporting changes in nail disease within Significant or extensive nail disease has a real
clinical trials have not been standardized. The impact on daily activities, may be disfiguring,
nail psoriasis and severity index (NAPSI) was and may be associated with significant pain.
developed to measure changes in nail disease Patients with significant nail disease need
over time [7]. therapies to address their nail psoriasis. Pa-
Some studies utilize a single target nail tients with moderate to severe psoriasis and
or an overall nail severity score. Other scales significant nail disease should be treated with
have been used to measure nail involvement appropriate therapy which addresses skin and
but most of the studies reviewed herein utilize nail disease.
some form of the NAPSI. The wide variety Previous consensus guidelines for the
of objective measures used in psoriasis stud- treatment of moderate to severe psoriasis also
ies to measure nail disease and the variety of apply to the patient with nail disease. The op-
time points when the measurements are made, tions including cyclosporine, methotrexate,
make a comparison of treatment outcomes for acitretin,new low-molecular substances with
various interventions difficult. Topical agents anti-psoriasis activity and biological drugs. Bio-
are often the first-line option for treating pa- logical treatment is the most effective therapy,
tients with nail disorders. These products are options including inhibitors of TNF-a (adali-
readily available, can be cheaper, and rarely mumab, etanercept, infliximab), inhibitors of
require laboratory monitoring. Strong and interleukin 12 and 23 (ustekinumab) and new
very strong glucocorticosteroids are used in drugs — inhibitors of 17 (secukinumab, ix-
combination with keratolytic drugs, vitamin ekizumab) and new inhibitors of interleukin
A derivatives such a tazarotene, and a combi- 23 (guselkumab, tildrakizumab) [8]. Clearly,
nation of calcipotriol with betamethasone di- there is a need for more uniform reporting of
propionate [8]. The challenges to treating nail nail outcomes and the adoption of a valid met-
disease are many. The most important issues ric that is specific to nail disease [11].
are poor penetration of topical therapy into
the nail and surrounding tissue, side effects MANAGEMENT OF A SCALP PSORIASIS
and monitoring of systemic therapies, and pa-
tient adherence to therapy [9]. The second form that needs great dissua-
Topical preparations, in particular, take sion in aesthetic medicine is scalp psoriasis
several months to show efficacy and adher- because it difficult to treat. Indeed, it may re-
ence to therapy over months is challenging. spond faster than other body regions to some
In a study comparing calcipotriol twice daily biological therapies but it remains a challenge
with calcipotriol/betamethasone once daily, to obtain good results with both topical and
adherence to the twice-daily regimen was only phototherapy. While the head and neck rep-
26%. Therefore, topical therapy may not only resent about 10% of the body surface area,
be limited by penetration into the nail unit but the impact of psoriasis in this region may be
also by adherence to lengthy treatment reg- disproportionate to the area and may have
imens lasting weeks or months. Procedures social and emotional impacts on affected in-
have also been studied in the treatment of nail dividuals, especially women. Most scalp psori-
psoriasis [10]. asis is treated with topical therapies including
Phototherapy, a common treatment for shampoos, oils, foams, liquids, and gels. Over-
skin disease, in the absence of psoralen or the-counter remedies, containing tar, salicylic
a retinoid, is not likely to improve nail disease acid, zinc, and others are relatively inexpen-
and is therefore not a viable option for nail sive and widely available. Prescription topi-
psoriasis. A treatment algorithm for nail psori- cal therapy mainly involves the use of mid to
32 Rheumatology Forum 2023, vol. 9, No. 1high-potency topical steroids and topical vita- ic dermatitis can be difficult. Seborrheic der-
min D analogs [12]. matitis is characterized by a diffuse thin scale
Many larger trials for the biologics have that is localized to the hair-bearing scalp and
had measures of scalp psoriasis as secondary may involve the central face and chest [16].
endpoints. A few trials have been designed Management of scalp psoriasis included
specifically to assess scalp disease and these topical and procedural therapies. Topical ther-
will be highlighted in this chapter. Further- apies are the foundation in the management
more, scalp psoriasis provides challenges to of scalp psoriasis and are utilized by approxi-
both practitioner and patient. mately 60% of patients. These therapies have
The incidence of scalp psoriasis in pa- been formulated into shampoos, gels, foams,
tients with psoriasis is estimated between oils, and solutions. Some of these products
40 and 90 percent. In up to half of patients, pso- have been evaluated in large clinical trials.
riasis may initially present on the scalp. Some High costs limit the use of many of these
patients only have psoriasis on the scalp. The proprietary products. Initially, keratolytic drugs
scalp is characterized by the presence of the such as salicylic acid in an oil base and urea to
prominent pilosebaceous unit and has a micro- remove the scale build-up. In the next stage of
biome that differs from other skin sites. Both the therapy, treatment is used that causes the
yeast and bacteria colonize the scalp. It is im- psoriasis foci to disappear. A commonly used
portant to note that Malessazia furfur, Males- and recommended therapy for scalp psoriasis
sazia globosa, candida, and other commensal is the combination of calcipotriol with beta-
organisms are found on the scalp in significant methasone dipropionion in a gel or foam base.
numbers and may influence scalp diseases such An alternative treatment is the using of topical
as seborrhea dermatitis and psoriasis. The role glucocorticosteroids of medium and high po-
of these organisms in psoriasis is not well es- tency in the form of solutions, shampoos and
tablished but they likely play a role. Treatments foams. Shampoos with tar act as a supportive
targeting these organisms have shown some ef- treatment for psoriasis of the scalp. Biologi-
ficacy in seborrhea dermatitis [13]. cal drugs and new low-molecular substances
Recent studies have shown that the hair (apremilast and dimethyl ester of fumaric acid)
in patients with scalp psoriasis be modified by effectively reduce changes in psoriasis of the
the presence of psoriatic inflammation. Some scalp [8].
researchers evidenced that hair shafts eval- Additionally, phototherapy for scalp pso-
uated in patients with psoriasis reveal pits, riasis is limited due to hair blocking the pen-
thought to be analogous to the pitting seen in etration of the light. With widespread rashes,
nails. Additionally, recent studies evaluating the entire skin is irradiated (general photother-
the transcriptome of both scalp and body pso- apy), with limited rashes — the affected area
riasis suggest there may be differences in gene of the body (local phototherapy). In a number
activation between the scalp and body [14]. of patients, lesions on the scalp and extremi-
Scalp lesions may vary from mild, with ties regress more slowly than in other parts of
minimal erythema and scaling, to severe with the body Devices have been designed and are
thick well-defined plaques with silvery scale and available to help deliver phototherapy to the
an erythematous border. Classic scalp psoriasis scalp. These devices use fiber optics that pen-
lesions are asymmetric, sharply demarcated, etrate through the hair and deliver the pho-
covered with silvery-white or grayscale, and may totherapy, broadband or narrow-band UVB,
extend beyond scalp margins to affect the fore- directly to the scalp [17–19].
head, ear, and neck. Most patients with psoria- Another method of aesthetic medi-
sis of the face also have scalp disease [15]. cine is carboxytherapy. It is helpful in the treat-
Multiple surveys have cited itching and ment of some psoriatic lesions. It involves the
scaling as the most disturbing aspects of scalp use of purified carbon dioxide in the form of
psoriasis. This itch may be so severe that it can a subcutaneous injection. Injections are made
interfere with sleep and lead to actual hair loss using mesotherapy needles. Repeatability of
due to hair breakage and trauma. Scalp pso- treatments is important to obtain the desired
riasis is usually not associated with significant results [20].
hair loss; however, some patients may have Bearing in mind the appearance of Koe-
alopecia due to the trauma of chronic itching bner’s symptom during the active form of the
leading to hair breakage. In some cases, the disease (formation after 8–14 days of psoriatic
differentiation of scalp psoriasis and seborrhe- lesions at the site of epidermal injury), aesthet-
Tetyana Waldheim et al. The features psoriasis challenges in aesthetic care 33ic medicine treatments should be selected with outcomes. This result can only be achieved
great care [21, 22]. through a strong patient–physician relation-
There are few studies that specifically ship, with both parties committed to establish-
address the efficacy of methotrexate, cyclo- ing trust, gaining a mutual understanding of
sporine, and acitretin in scalp psoriasis. None- beliefs and expectations, and addressing chal-
theless, these therapies may be effective in lenges early [24, 25].
treating scalp disease. Appropriate monitoring
of liver function, creatinine, complete blood CONCLUSIONS
counts, triglycerides (acitretin), blood glucose
should be maintained during treatment with 1. Psoriasis affects many areas of patients’
these agents. lives. It limits their personal, social and
Before prescribing treatment to identify professional live.
contraindications, a clinical examination of 2. Biological treatment is more effective than
the patient and a complex of laboratory tests classical anti-psoriaris treatment of pa-
are carried out, including a general blood test, tients.
a general urine test, a biochemical blood test 3. Adherence is the cornerstone of disease
(including the determination of liver and kid- management, influencing disease improve-
ney function indicators), a consultation with ment, flaring, and stagnancy in dermatolo-
a therapist, an ophthalmologist, an endo- gy and across medical specialties.
crinologist, a gynecologist. According to the 4. Efforts to improve adherence may indirect-
indications, it is recommended to be examined ly reduce the overall disease burden of pso-
by other specialists [23]. riasis and other chronic conditions.
Many factors influence a patient’s de- 5. Phototherapy and carboxytherapy are most
cision to not adhere to the treatment plan or commonly used methods of aesthetic med-
discontinue a drug, some of which include icine, which are helpful in the treatment of
therapeutic inefficacy, loss of response over psoriasis symptoms.
time, poor socioeconomic status, and costs. An
individualized plan shaped to the patient’s CONFLICT OF INTEREST
goals, preferences, and disease condition
can augment adherence and improve clinical None declared.
References 1. Brownstone ND, Hong J, Mosca M, et al. Biologic treat- doi: 10.1080/09546634.2019.1687828, indexed in Pub-
ments of psoriasis: an update for the clinician. Biolo- med: 31714168.
gics. 2021; 15: 39–51, doi: 10.2147/BTT.S252578, inde- 6. Kisielnicka A, Szczerkowska-Dobosz A, Nowic-
xed in Pubmed: 33623366. ki RJ. The influence of body weight of patients with
2. Mocanu M, Toader MP, Rezus E, et al. Aspects concerning chronic plaque psoriasis on biological treatment re-
patient adherence to anti-TNFa therapy in psoriasis: A de- sponse. Postepy Dermatol Alergol. 2020; 37(2):
cade of clinical experience. Exp Ther Med. 2019; 18(6): 168–173, doi: 10.5114/ada.2020.94835, indexed in Pub-
4987–4992, doi: 10.3892/etm.2019.8008, indexed in Pub- med: 32489349.
med: 31798720. 7. van der Velden HMJ, Klaassen KMG, van de Kerkhof PCM,
3. Lin PT, Wang SH, Chi CC. Drug survival of biologics in et al. The impact of fingernail psoriasis on patients’ health-
treating psoriasis: a meta-analysis of real-world evidence. -related and disease-specific quality of life. Dermatology.
Sci Rep. 2018; 8(1): 16068, doi: 10.1038/s41598-018- 2014; 229(2): 76–82, doi: 10.1159/000360696, indexed
34293-y, indexed in Pubmed: 30375427. in Pubmed: 25171519.
4. Feldman SR, Zhang J, Martinez DJ, et al. Real-world tre- 8. Reich A, Szepietowski J, Adamski Z, et al. Psoria-
atment patterns and healthcare costs of biologics and sis. Diagnostic and therapeutic recommendations of
apremilast among patients with moderate-to-severe plaque the Polish Dermatological Society. Part II: Moderate to
psoriasis by metabolic condition status. J Dermatolog Tre- severe psoriasis. Dermatol Rev. 2018; 105: 329–357,
at. 2021; 32(2): 203–211, doi: 10.1080/09546634.2019.1 doi: 10.5114/dr.2018.77107.
698699, indexed in Pubmed: 31769703. 9. Armesto S, Esteve A, Coto-Segura P, et al. Nail psoriasis in
5. Wu B, Muser E, Teeple A, et al. Treatment adherence and individuals with psoriasis vulgaris: a study of 661 patients
persistence of five commonly prescribed medications for [article in Spanish]. Actas Dermosifiliogr. 2011; 102(5):
moderate to severe psoriasis in a U.S. commercially insu- 365–372, doi: 10.1016/j.ad.2011.02.007, indexed in Pub-
red population. J Dermatolog Treat. 2021; 32(6): 595–602, med: 21514549.
34 Rheumatology Forum 2023, vol. 9, No. 110. Werner B, Fonseca G, Seidel G. Microscopic nail clipping fin- 18. Medovic MV, Jakovljevic VLj, Zivkovic VI, et al. Psoriasis be-
dings in patients with psoriasis. Am J Dermatopathol. 2015; tween autoimmunity and oxidative stress: changes induced
37(6): 429–439, doi: 10.1097/dad.0000000000000197, by different therapeutic approaches. Oxid Med Cell Longev.
indexed in Pubmed: 25993403. 2022; 2022: 2249834, doi: 10.1155/2022/2249834, inde-
11. Radtke MA, Beikert FC, Augustin M. Nail psoriasis xed in Pubmed: 35313642.
— a treatment challenge. J Dtsch Dermatol Ges. 2013; 19. Li Y, Cao Z, Guo J, et al. Assessment of efficacy and safety
11(3): 203–220, doi: 10.1111/ddg.12054, indexed in Pub- of UV-based therapy for psoriasis: a network meta-analy-
med: 23425398. sis of randomized controlled trials. Ann Med. 2022; 54(1):
12. de Vries AC, Bogaards NA, Hooft L, et al. Interventions 159–169, doi: 10.1080/07853890.2021.2022187, inde-
for nail psoriasis. Cochrane Database Syst Rev. 2013(1): xed in Pubmed: 34989291.
CD007633, doi: 10.1002/14651858.CD007633.pub2, in- 20. Zelenková H. Carboxytherapy — a non-invasive method
dexed in Pubmed: 23440816. in aesthetic medicine and dermatology, and the combined
13. Oram Y, Akkaya AD. Treatment of nail psoriasis: common usage of carboxytherapy and PRP in the periorbital area.
concepts and new trends. Dermatol Res Pract. 2013; Glob Dermatol. 2017; 4(1), doi: 10.15761/god.1000202.
2013: 180496, doi: 10.1155/2013/180496, indexed in 21. Kamel AM, Abdelghani R. Carboxytherapy for treatment
Pubmed: 23762032. of localized chronic plaque psoriasis: Clinical and histo-
14. Langley RG, Saurat JH, Reich K, et al. Nail Psoriasis Delphi pathologic evaluation. J Cosmet Dermatol. 2018; 17(3):
Expert Panel. Recommendations for the treatment of nail 527–532, doi: 10.1111/jocd.12494, indexed in Pub-
psoriasis in patients with moderate to severe psoriasis: med: 29341446.
a dermatology expert group consensus. J Eur Acad Derma- 22. Psoriasis Treatments — National Psoriasis Foundation. https://
tol Venereol. 2012; 26(3): 373–381, doi: 10.1111/j.1468- www.psoriasis.org/about-psoriasis/treatments (5.02.2019).
-3083.2011.04349.x, indexed in Pubmed: 22151734. 23. Feldman SR, Zhang J, Martinez DJ, et al. Real-world tre-
15. Armstrong AW, Tuong W, Love TJ, et al. Treatments atment patterns and healthcare costs of biologics and
for nail psoriasis: a systematic review by the GRAPPA apremilast among patients with moderate-to-severe plaque
Nail Psoriasis Work Group. J Rheumatol. 2014; 41(11): psoriasis by metabolic condition status. J Dermatolog Tre-
2306–2314, doi: 10.3899/jrheum.140881, indexed in Pub- at. 2021; 32(2): 203–211, doi: 10.1080/09546634.2019.1
med: 25362716. 698699, indexed in Pubmed: 31769703.
16. De Simone C, Maiorino A, Tassone F, et al. Tacrolimus 0.1% 24. Wu B, Muser E, Teeple A, et al. Treatment adherence and
ointment in nail psoriasis: a randomized controlled open- persistence of five commonly prescribed medications for
-label study. J Eur Acad Dermatol Venereol. 2013; 27(8): moderate to severe psoriasis in a U.S. commercially insu-
1003–1006, doi: 10.1111/j.1468-3083.2012.04642.x, red population. J Dermatol Treat. 2021; 32(6): 595–602,
indexed in Pubmed: 22788697. doi: 10.1080/09546634.2019.1687828, indexed in Pub-
17. Armstrong AW, Siegel MP, Bagel J, et al. From the medi- med: 31714168.
cal board of the National Psoriasis Foundation: treatment 25. Bakshi H, Nagpal M, Singh M, et al. Treatment of psoriasis:
targets for plaque psoriasis. J Am Acad Dermatol. 2017; a comprehensive review of entire therapies. Curr Drug Saf.
76(2): 290–298, doi: 10.1016/j.jaad.2016.10.017, indexed 2020; 15(2): 82–104, doi: 10.2174/15748863156662001
in Pubmed: 27908543. 28095958, indexed in Pubmed: 31994468.
Tetyana Waldheim et al. The features psoriasis challenges in aesthetic care 35You can also read