Management of Complex Cases - Grand Rounds from HSS | Rheumatology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Management of Complex Cases
Grand Rounds from HSS | Rheumatology
November 2021 The Art and Science
Volume 10 Issue 2
of Rheumatology
HSS Authors Karmela Kim Chan, MD
Anne R. Bass, MD
Attending Physician
It is my honor to serve as editor of this issue of Grand Rounds from HSS: Management of
Professor of Clinical Medicine
Complex Cases focused on rheumatology. We at HSS take pride in our thoughtful and
Weill Cornell Medicine
thorough approach to caring for patients, and we are excited to share with you lessons we
David R. Fernandez, MD, PhD have learned in 4 cases involving complex rheumatologic conditions.
Assistant Attending Physician
Assistant Professor of Medicine One principle encountered in medical training is that when a diagnosis is elusive, consider
Weill Cornell Medicine the triad of pathologies of malignancy, infection, or rheumatic disease. The cases in this
issue confirm that there is a good reason this heuristic endures.
Roberto A. Garcia, MD
Associate Attending Pathologist Case 1 from Kevin Yip, MD, and Anne R. Bass, MD, suggests that in a patient with a
Associate Professor of Clinical previously treated hepatitis B virus infection, vaccination against SARS-CoV-2 may have
Pathology and Laboratory activated the immune system in an unexpected way. Case 2 from Diane Zisa, MD,
Medicine Roberto A. Garcia, MD, and Susan M. Goodman, MD, demonstrates the challenge of
Weill Cornell Medicine identifying new-onset inflammatory arthritis after total joint arthroplasty. Case 3 from
David R. Fernandez, MD, PhD, details the diagnostic curveballs encountered in a patient
Susan M. Goodman, MD
with proximal muscle weakness, rash, and nailfold capillary changes. Finally, Case 4 from
Attending Physician
Lauren Robinson, MD, and Sarah Taber, MD, presents a 2-year-old boy with macrophage
Professor of Clinical Medicine
Weill Cornell Medicine activation syndrome, whose underlying diagnosis of Kikuchi–Fujimoto disease was revealed
several years later.
Lauren Robinson, MD
Rheumatology Fellow I hope you find the cases in this issue as stimulating as I did. These cases show the
complexities and uncertainties that rheumatologists face routinely as we practice this art
Sarah Faith Taber, MD form we call medicine. As ever, we welcome your feedback, at complexcases@hss.edu.
Assistant Attending Physician
Assistant Professor of Pediatrics
Weill Cornell Medicine
In This Issue
Kevin Yip, MD
Rheumatology Fellow Case 1
Recurrent Leukocytoclastic Vasculitis Following
Diane Zisa, MD mRNA COVID-19 Vaccination in a 76-Year-Old Woman
Rheumatology Fellow
with Previously Treated Hepatitis B Virus Infection
Case 2
Incident Rheumatoid Arthritis in a 64-Year-Old
Woman with a Prosthetic Joint
Case 3
An Overlap of Drug-Induced Subacute Cutaneous
Lupus Erythematosus and Dermatomyositis in an
80-Year-Old Woman
Case 4
Kikuchi–Fujimoto Disease in a 6-Year-Old Boy with
a History of Macrophage Activation Syndrome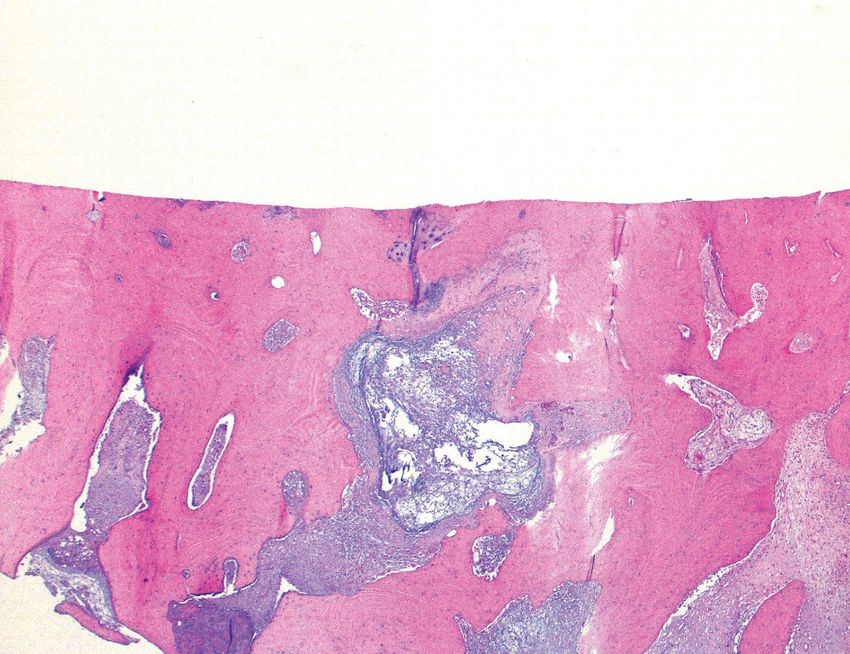
Case 1: Recurrent Leukocytoclastic Vasculitis Following
mRNA COVID-19 Vaccination in a 76-Year-Old Woman with
Previously Treated Hepatitis B Virus Infection
Discussion COVID-19 vaccination This patient also experienced elevated
Case presented by:
is recommended for people with liver enzymes and a high international
Kevin Yip, MD autoimmune and inflammatory normalized ratio (INR). We hypothesize
Rheumatology Fellow rheumatologic diseases, even though it several possible explanations. First, the
may increase the risk of disease flares vaccine may have caused autoimmunity
in some patients [2]. A few cases of LCV directed against the SARS-CoV-2 spike
occuring after COVID-19 vaccination have protein–expressing liver cells; a study in
Anne R. Bass, MD been reported: 1 patient had psoriatic mice showed that after mRNA vaccination
Attending Physician arthritis and 2 were otherwise healthy there was uptake of mRNA-containing
Professor of Clinical Medicine [3-5]; we believe we are the first to lipid nanoparticles and protein translation
Weill Cornell Medicine describe LCV recurrence along with HBV in the liver [10]. Second, the vaccine may
reactivation after COVID-19 vaccination. have led directly to HBV reactivation
and acute hepatitis through an unknown
Expert position papers from the EASL
Case Report The coronavirus disease mechanism. Third, the vaccine may have
(European Association for the Study of
2019 (COVID-19) messenger RNA induced only LCV, and the elevated liver
the Liver) [6] and the AASLD (American
(mRNA) vaccines have proven largely enzymes could have developed due to
Association for the Study of Liver
safe and highly effective in preventing stopping the tenofovir for several days.
Diseases) [7] note that patients with
hospitalizations and deaths from infection chronic liver disease are at high risk for The Pfizer-BioNTech COVID-19 vaccine
with severe acute respiratory syndrome COVID-19 sequalae and recommend phase 2/3 trial enrolled 43,448
coronavirus 2 (SARS-CoV-2) [1]. In early COVID-19 vaccines for this population individuals; of those in the vaccine arm,
2021 we treated a 76-year-old woman (although patients with significant liver 125 had mild liver disease and 1 had
with chronic hepatitis B virus (HBV) disease were excluded from licensing moderate or severe liver disease [1].
infection who developed a recurrence of trials). Some evidence suggests that Although the phase 1/2 trials excluded
leukocytoclastic vasculitis (LCV) within patients with chronic liver disease mount a those with known HBV infection, such
days of receiving her first dose of the weaker vaccine response to the influenza, patients were eligible for the phase 2/3
Pfizer-BioNTech mRNA COVID-19 vaccine. Streptococcus pneumoniae, and hepatitis trial if they were negative for hepatitis
The patient was diagnosed with HBV A and B virus vaccines [6]. B e antigen (HBeAg), had persistently
in 1994 when she presented with normal alanine aminotransferase and
Our patient’s clinical picture was
hepatocellular carcinoma. She was started aspartate transaminase (ALT and AST)
consistent with a reactivation of HBV
on lamivudine but in 2002 developed levels, and had a serum HBV DNA level
infection, manifesting as LCV and
lamivudine resistance and LCV requiring of less than 2000 IU/mL. US Food and
compromised liver function. Her LCV had
corticosteroids. Adefovir and azathioprine Drug Administration documents from the
been quiescent for more than 10 years on
were added in 2004, but in 2008, after Vaccines and Related Biological Products
tenofovir, and her HBV viral load was nil
developing adefovir resistance, she was Advisory Committee show no increase
15 months prior to receiving the vaccine.
switched to tenofovir, with suppression of of hepatic enzymes in the vaccinated
While we cannot establish causation, the
HBV and resolution of LCV. Corticosteroids group [11]. Still, our case suggests that
timing of the rash suggests a possible
and azathioprine were discontinued, and in in patients with chronic HBV infection
relationship between COVID-19 mRNA
2019 her HBV viral load was undetectable. it may be prudent to check the HBV
vaccination and HBV recrudescence and
viral load and liver enzyme levels before
In late 2020 the patient received her LCV recurrence. Tenofovir was held for
COVID-19 vaccination and maintain HBV
first dose of the COVID-19 mRNA several days after vaccination, but it was
control and continue antiviral agents after
vaccination. ■
vaccine; 5 days later she developed a not a likely cause of this degree of HBV
purpuric rash on her legs (Fig. 1), and her reactivation.
dermatologist diagnosed LCV. The day LCV in patients with HBV can be due to Image on page 3
the rash appeared her internist instructed either HBV-containing immune complexes Table and references on page 4
her to discontinue tenofovir, but it was or cryoglobulinemia [8]. Both mechanisms
resumed 3 days later. Laboratory test lead to complement activation and
results revealed markedly elevated liver hypocomplementemia. Although the
enzymes, coagulopathy, active HBV, and patient twice had negative cryoglobulin
profound hypocomplementemia (see test results, high titer rheumatoid factor
Table 1 on page 4). The patient improved and profound hypocomplementemia could
with prednisone 40 mg, but LCV recurred suggest cryoglobulinemia [9]. While there
when this dose was tapered. Her HBV viral currently are no studies or case reports
load declined and LCV improved, but mild to support the hypothesis, we believe the
symptoms persisted several months post- vaccine could have led to HBV reactivation
vaccination. and in turn to recurrent immune-complex-
mediated LCV.
2 | Management of Complex Cases
November 2021 | Volume 10 Issue 2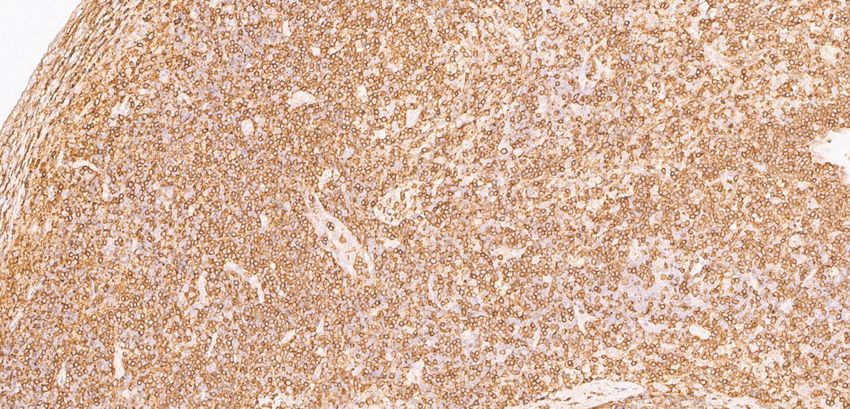
Case 1: Recurrent Leukocytoclastic Vasculitis Following mRNA COVID-19 Vaccination in a 76-Year-Old Woman with Previously
Treated Hepatitis B Virus Infection Case Images
Figure 1
A purpuric rash over the patient’s right calf,
characteristic of leukocytoclastic vasculitis.
3 | Management of Complex Cases
November 2021 | Volume 10 Issue 2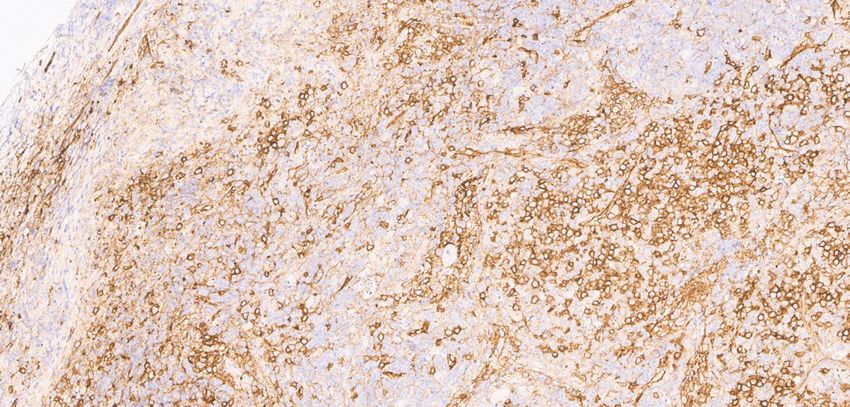
Case 1: Recurrent Leukocytoclastic Vasculitis Following mRNA COVID-19 Vaccination in a 76-Year-Old Woman with Previously
Treated Hepatitis B Virus Infection Table and references
Table 1
Timeline and laboratory results, before and after first dose of the Pfizer-BioNTech mRNA COVID-19 vaccine
16 5 weeks 20 days Day 0: Day 4 Day 9 Day 13 Day 21 Day 27 Day 39 Day 55 Day 71
months prior to prior to COVID-19
prior to vaccine vaccine vaccine
vaccine
Clinical event LCV onset LCV LCV LCV LCV LCV flare LCV LCV
ongoing ongoing worse fading, ongoing improved
no new
lesions
Tenofovir 300 300 300 300 Withheld Resumed 300 300 300 300 300 300
(mg/day) 300
Prednisone 40 60 40 2.5 ->10 10 10
(mg/day)
Alkaline 66 71 99 247 245 118 168 188 177 188
phosphatase
(IU/L)
Aspartate 29 28 335 495 85 45 58 40 58
transaminase
(IU/L)
Alanine 21 11 13 260 314 56 56 39 56
aminotransferase
(IU/L)
INR 1.0 1.08 1.1 6 1.1 0.6 1.02
Complement 3 100 91.2 67 69 76 67.1
(mg/dL)
Complement 4 22 16.5
Case 2: Incident Rheumatoid Arthritis in a 64-Year-Old
Woman with a Prosthetic Joint
Focal granulation tissue with loss of the We know of no other reported cases of
Case presented by:
synovial lining layer and increased numbers incident RA in a prosthetic joint. This
Diane Zisa, MD of superficial neutrophils were suggestive case illustrates the ambiguity that often
Rheumatology Fellow but not diagnostic of infection (Fig. 1D). confronts rheumatologists. Tools to
Review of the histopathology from the differentiate an inflammatory arthritis
initial surgery confirmed degenerative joint flare from PJI are needed to avoid the
disease without inflammatory features morbidity and expense associated with
and moderate calcium pyrophosphate delay in making a definitive diagnosis and
Roberto A. Garcia, MD deposition (Fig. 2A, 2B). treating PJI. At HSS, research is under
Associate Attending Pathologist
Associate Professor of Clinical way to investigate serum and synovial
Additional serologic testing revealed a high-
Pathology and Laboratory biomarkers and next-generation microbial
titer rheumatoid factor (RF) of 168.3 IU/mL
Medicine sequencing in arthroplasty patients with
and an anticyclic citrullinated peptide (anti-
Weill Cornell Medicine and without inflammatory arthritis to help
CCP) antibody level of more than 250 units,
diagnose PJI expeditiously in patients with
inflammatory arthritis. ■
Susan M. Goodman, MD with persistent elevations in ESR and CRP. A
Attending Physician rheumatology review of her history revealed
Professor of Clinical Medicine no symptoms suggestive of inflammatory Images on pages 6–8
Weill Cornell Medicine joint disease. However, based on serology
and histopathology results and subsequent
swelling of several metacarpophalangeal REFERENCES:
and proximal interphalangeal joints, RA 1. Premkumar A, Morse K, Levack AE, Bostrom
Case Report A 64-year-old woman was diagnosed. Antibiotics were stopped MP, Carli AV. Periprosthetic joint infection
presented 16 months after bilateral total 4 weeks after surgery and methotrexate in patients with inflammatory joint disease:
knee arthroplasty (TKA) with acute pain was begun. She has had a partial response prevention and diagnosis. Curr Rheumatol
and swelling in her left knee that began to antirheumatic therapy, and her regimen Rep. 2018;20(11):68.
during exercise and worsened; she also is being adjusted to achieve better control.
developed fatigue and malaise. X-rays 2. Mirza SZ, Richardson SS, Kahlenberg CA,
Discussion It is challenging to differentiate et al. Diagnosing prosthetic joint infections
demonstrated a well-fixed TKA in good
PJI from a flare of inflammatory arthritis, in patients with inflammatory arthritis: a
position. Laboratory test results revealed
given the overlapping clinical and laboratory systematic literature review. J Arthroplasty.
an erythrocyte sedimentation rate (ESR) 2019;34(5):10321036.e2.
of 128 mm/hr and a C-reactive protein criteria for each diagnosis, especially
(CRP) level of 5.8 mg/dL, mild anemia when definitive microbiologic data are not 3. Goodman S, Kapadia M, Miller A, et al.
available [1,2,3]. Furthermore, patients with Clinical features of prosthetic joint infections
and thrombocytosis, and a normal white
rheumatoid arthritis are at increased risk for in patients with rheumatic diseases vs
blood cell (WBC) count. Aspiration of
PJI and may have more frequent culture- osteoarthritis [abstract]. Arthritis Rheumatol.
the left knee yielded opaque fluid with an 2019; 71 (suppl 10). Presented at: 2019 ACR/
elevated WBC count of 17,457/µL (89% negative infections [3]. Following any
ARP Annual Meeting; November 8-13, 2019;
neutrophils) and a negative Gram stain arthroplasty, elevated serum inflammatory Atlanta, GA.
without crystals. markers and synovial fluid leukocyte levels
are always concerning for PJI. Microbiology
Acute periprosthetic joint infection (PJI) results can take time; because a delay in
was the presumed diagnosis, prompting diagnosis may worsen outcomes, surgery
urgent irrigation and debridement of should be performed promptly.
the left knee with a liner exchange.
Aspiration of her asymptomatic right The patient’s initial monoarticular
knee was also performed, given the pain and swelling in a prosthetic joint
concern for a hematogenous infection, was appropriately treated urgently
and revealed a WBC count of 6,700/µL as a presumed PJI. Histopathologic
(62% neutrophils). She began antibiotics examination of the surgical specimen,
(daptomycin and ceftriaxone) for an showing polymorphonuclear leukocytes
anticipated 6-week course, without superimposed on the chronic inflammatory
significant improvement. Synovial fluid changes, was critical in pointing to the
samples taken from both knees were diagnosis of inflammatory arthritis. The
cultured and found to be negative for RA diagnosis was corroborated by the
bacteria, acid-fast bacilli, and fungi. patient’s lack of response to antibiotics,
the subsequent serology results, and her
Histopathologic examination of the left clinical evolution to polyarthritis.
knee tissue showed a proliferative and
exudative synovitis with lymphoplasmacytic
inflammation and scattered superficial
neutrophils (Fig. 1A, 1B), as well as
binucleated plasma cells and Russell
bodies (Fig. 1C). These findings were
suggestive of rheumatoid arthritis (RA).
5 | Management of Complex Cases
November 2021 | Volume 10 Issue 2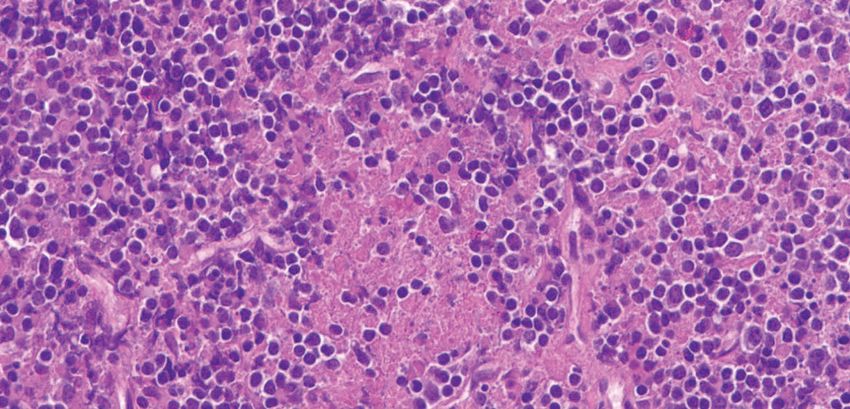
Case 2: Incident Rheumatoid Arthritis in a 64-Year-Old Woman with a Prosthetic Joint Case Images
Figure 1A
Synovial tissue with marked
lymphoplasmacytic inflammation,
abundant superficial fibrinous exudate,
and scattered neutrophils (arrows).
Hematoxylin-eosin (H&E) stain, original
magnification ×200.
Figure 1B
The synovial lining layer is well
preserved in this area with marked
lymphoplasmacytic inflammation
and increased number of superficial
neutrophils (arrows). H&E stain,
original magnification ×200.
6 | Management of Complex Cases
November 2021 | Volume 10 Issue 2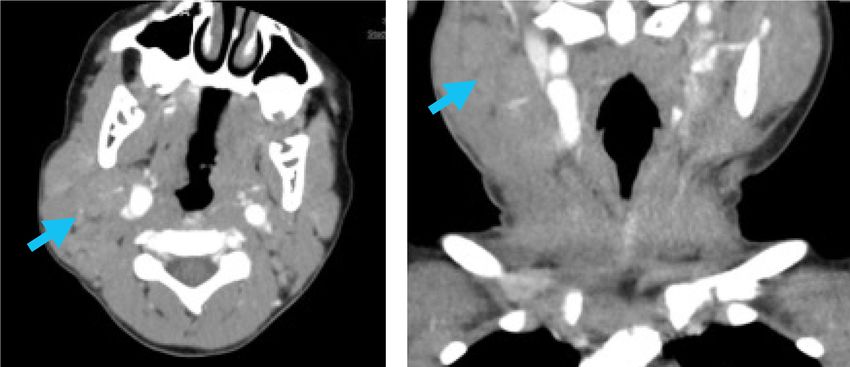
Case 2: Incident Rheumatoid Arthritis in a 64-Year-Old Woman with a Prosthetic Joint Case Images Continued
Figure 1C
High magnification of the
lymphoplasmacytic infiltrate with
binucleated plasma cells (arrows) and
a Russell Body (arrowhead). H&E stain,
original magnification ×400.
Figure 1D
Granulation tissue with loss of the
synovial lining layer and superficial
fibrin; inflammatory infiltrate includes
lymphocytes, plasma cells, and scattered
neutrophils (arrows). H&E stain, original
magnification ×200.
7 | Management of Complex Cases
November 2021 | Volume 10 Issue 2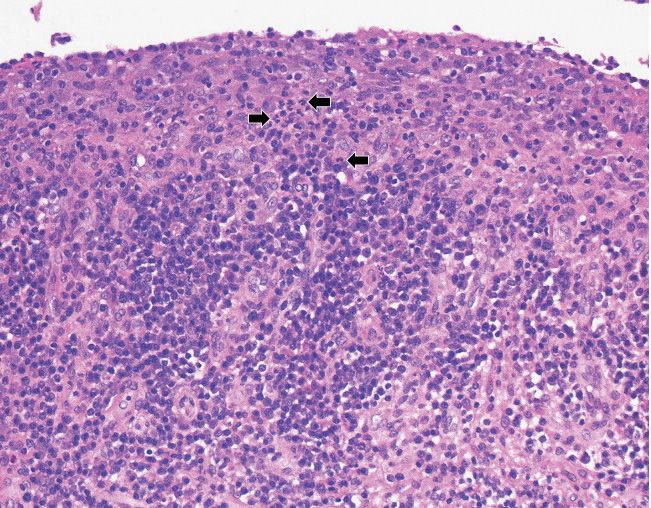
Case 2: Incident Rheumatoid Arthritis in a 64-Year-Old Woman with a Prosthetic Joint Case Images Continued
Figure 2A
The articular surface demonstrates
complete loss of the cartilage with
moderate sclerosis of the exposed
subarticular bone and a myxoid
pseudocyst. H&E stain, original
magnification ×25.
Figure 2B
The synovium and meniscus
demonstrate calcium pyrophosphate
dihydrate crystal deposition. H&E stain,
original magnification ×100.
8 | Management of Complex Cases
November 2021 | Volume 10 Issue 2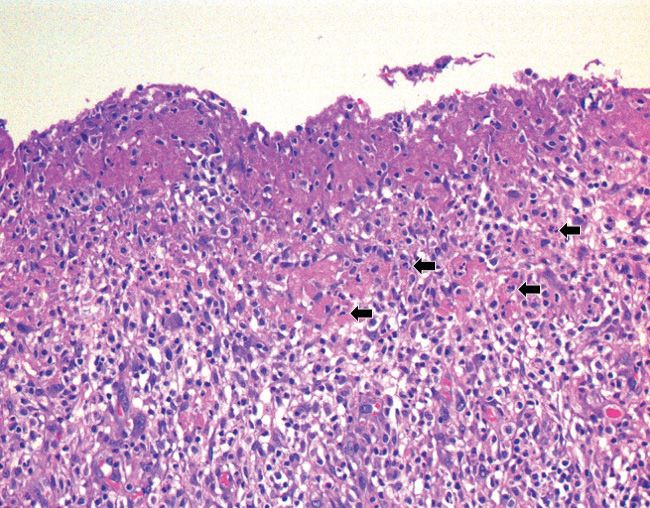
Case 3: An Overlap of Drug-Induced Subacute Cutaneous
Lupus Erythematosus and Dermatomyositis in an
80-Year-Old Woman
severe fatigue and subtle weakness, most This case highlights the value of nailfold
Case presented by: noticeable as modest difficulty in climbing capillary assessment in the diagnosis
David R. Fernandez, MD, PhD steps and dyspnea on exertion. of DM [4], as some other features of the
Assistant Attending Physician patient’s presentation were suggestive
Assistant Professor Examination confirmed proximal
of systemic lupus erythematosus (SLE),
of Medicine muscle weakness, rash, and marked
and skin biopsy was insufficient for
Weill Cornell Medicine nailfold capillary changes (Fig. 2), with
distinguishing between SLE and DM.
hyperkeratotic cuticles, extensive dropout,
Additionally, while the annular rash of the
and enlarged capillaries. Laboratory
Case Report An 80-year-old woman lower extremities appearing as an atypical
testing revealed normal creatine kinase
developed a pruritic rash on her scalp, manifestation of DM cannot be ruled out,
but elevated lactate dehydrogenase levels,
prompting a dermatology evaluation its resolution with diltiazem cessation,
lymphopenia, and mild eosinophilia.
after several weeks. A biopsy found along with the persistence of other DM
interface dermatitis and prominent Based on these findings, she was manifestations, suggests that these were
tissue eosinophils, perhaps consistent diagnosed with DM and a second, distinct separate phenomena. ■
with a drug reaction. Her past medical rash provoked by diltiazem exposure,
history included Hashimoto’s thyroiditis, suggestive of SCLE. She was treated with Images on page 10
hypertension, knee osteoarthritis, tapering prednisone, beginning at 40 mg
collagenous colitis, mitral regurgitation daily, and hydroxychloroquine.
requiring mitral valve replacement, atrial REFERENCES:
Later, the annular rash and peripheral
fibrillation for which she was taking eosinophilia faded with diltiazem 1. Crowson AN, Magro CM. Subacute
coumadin, and a distant history of breast discontinuation, but the DM rashes and cutaneous lupus arising in the setting of
cancer, with no evidence of active disease. weakness persisted. Two months later she calcium channel blocker therapy. Hum
Several medications were discontinued, Pathol. 1997;28(1):67–73.
was found to be positive for antibodies
including diltiazem 2 months after the rash to transcription intermediary factor 1-γ, 2. Seidler AM, Gottlieb AB. Dermatomyositis
appeared, losartan–hydrochlorothiazide a which was not part of the initial myositis induced by drug therapy: A review of
month after that, followed by atorvastatin, assessment. This antibody can be case reports. J Am Acad Dermatol.
guaifenesin, loperamide, and omeprazole. associated with malignancy in patients 2008;59(5):872–880.
Nonetheless, her rash progressed. with DM, but no cancer has been identified 3. Zeidi M, Chansky PB, Werth VP. Acute onset/
She developed periorbital edema and on subsequent annual screenings. Four flares of dermatomyositis following ingestion
years after her initial symptoms, the of IsaLean herbal supplement: Clinical and
erythema, rash of the anterior chest and
patient is still experiencing mild skin and immunostimulatory findings. J Am Acad
lateral thighs, periungual erythema, diffuse Dermatol. 2019;80(3):801–804.
erythema of the dorsum of her hands, and muscle symptoms despite prednisone
coarseness and fissuring of the skin of her 5 mg daily and hydroxychloroquine. Trials 4. Cassius C, Le Buanec H, Bouaziz JD, Amode
lateral fingers. Hydroxychloroquine 200 mg of azathioprine and methotrexate were R. Biomarkers in adult dermatomyositis:
complicated by repeated infections and so tools to help the diagnosis and predict
twice daily was added 5 months after
were discontinued. She is also managing the clinical outcome. J Immunol Res.
symptoms appeared, with little benefit. 2019;2019:9141420.
Given the increasingly classic presentation her symptoms through structured physical
of the rash, she was thought to have therapy.
dermatomyositis (DM). A skin biopsy taken Discussion This case presents an
from the thigh showed interface dermatitis interesting overlap of SCLE and DM.
with karyorrhexis, a finding consistent with Drug-induced lupus is a well-characterized
subacute cutaneous lupus erythematosus phenomenon, classically associated with
(SCLE), although DM or a drug reaction anti-histone antibodies; management
could not be ruled out. Serologic testing involves removing the offending agent.
was notable for a positive antinuclear SCLE can be associated with medications,
antibody titer (1:2560) and antibodies to most commonly calcium channel blocker
single-stranded DNA and thyroglobulin, therapy [1].
but testing was otherwise negative,
including for anti-Ro/SSA and anti-histone Drug-induced DM is less well characterized
antibodies and a limited myositis panel. but can occur in the setting of a variety
of medications [2], including statins,
A re-introduction of diltiazem several hydroxyurea, or supplements [3], although
months later to treat hypertension resulted diltiazem has not been reported as a
in a dramatic surge in her pruritic rash, with potential cause. In this case, diltiazem
more diffuse erythema covering most of may have had a role in the onset of DM and
her body. The rash was mostly confluent in SCLE, although removing it did not resolve
the upper body but consisted of coalescing all clinical findings, even with the addition
papules and annular plaques of the lower of hydroxychloroquine and prednisone.
extremities (Fig. 1). She also reported
9 | Management of Complex Cases
November 2021 | Volume 10 Issue 2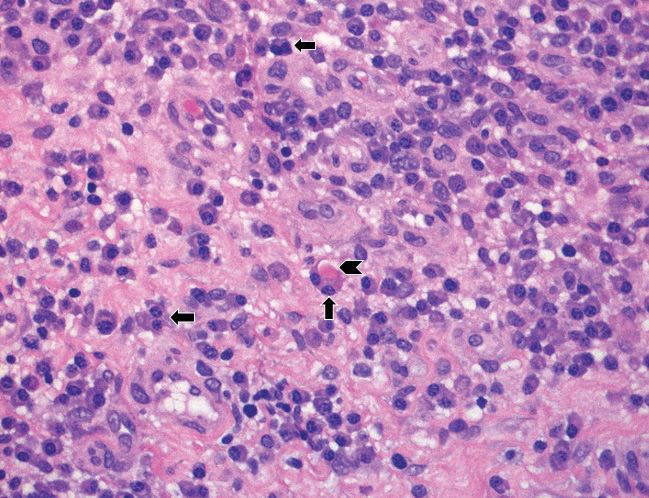
Case 3: An Overlap of Drug-Induced Subacute Cutaneous Lupus Erythematosus and Dermatomyositis
in an 80-Year-Old Woman Case Images
Figure 1
Annular plaques of the lower extremities.
Figure 2
Nailfold changes, including hyperkeratotic cuticles, extensive
dropout, and enlarged capillaries.
10 | Management of Complex Cases
November 2021 | Volume 10 Issue 2Case 4: Kikuchi–Fujimoto Disease in a 6-Year-Old Boy
with a History of Macrophage Activation Syndrome
complicated by MAS. Genetic testing for Hydroxychloroquine has been suggested
Case presented by:
underlying autoinflammatory disease or for use in severe or recurrent disease in
Lauren Robinson, MD immunodeficiency was unrevealing. children [6]. ■
Rheumatology Fellow
He was treated initially with 2 mg/kg Image on pages 12–13
prednisone daily and 100 mg anakinra
daily for 3 days, with rapid resolution of
fever and stabilization of cytopenias. He REFERENCES:
Sarah Faith Taber, MD was discharged on a slow steroid taper,
Assistant Attending Physician 1. Kim TY, Ha KS, Kim Y, Lee J, Lee K, Lee J.
but his fever returned and daily anakinra
Assistant Professor of Pediatrics Characteristics of Kikuchi-Fujimoto disease
Weill Cornell Medicine was re-initiated and titrated up to 100 mg
in children compared with adults. Eur J
BID. He subsequently remained afebrile;
Pediatr. 2014;173(1):111–116.
all laboratory parameters normalized
and lymphadenopathy remitted, 2. Ogata S, Bando Y, Saito N, Katsuoka K, Ishii
Case Report A 6-year-old boy with allowing for gradual discontinuation M. Kikuchi-Fujimoto disease developed into
a remote history of massive cervical of steroids. After 2 months, treatment autoimmune disease: a report of two cases.
Mod Rheumatol. 2010;20(3):301–305.
lymphadenopathy and macrophage with hydroxychloroquine was begun for
activation syndrome (MAS) presented recurrent Kikuchi–Fujimoto disease. After 3. Ahn SS, Lee B, Kim D, et al. Evaluation
with 1 month of fever and cervical an additional 6 months he remains well and of macrophage activation syndrome in
lymphadenopathy suspicious for recurrent is tolerating a gradual taper of anakinra. hospitalised patients with Kikuchi-Fujimoto
MAS. After his birth he had been well until disease based on the 2016 EULAR/ACR/
Discussion Kikuchi–Fujimoto disease is PRINTO classification criteria. PLoS One.
age 2, when he developed fever, rash,
seen increasingly in children, who often do 2019;14(7):e0219970.
lymphadenopathy, elevated inflammatory
not fit the classical disease presentation. 4. Duan W, Xiao ZH, Yang LG, Luo HY.
markers, and cytopenias. Extensive
Among children there is predominance Kikuchi’s disease with hemophagocytic
infectious and oncologic workups,
in boys (1.4:1 male to female) compared lymphohistiocytosis: a case report and
including cervical lymph node biopsy, at
to a predominance in women among literature review. Medicine (Baltimore).
that time were unrevealing. His symptoms
adults. Additionally, children with Kikuchi– 2020;99(51):e23500.
resolved with treatment with steroids and
Fujimoto disease are more likely to present 5. Selvanathan SN, Suhumaran S, Sahu VK,
anakinra, which were discontinued within
with fever and leukopenia and less likely to Chong CY, Tan NW, Thoon KC. Kikuchi-
5 months.
have a positive antinuclear antibody test Fujimoto disease in children. J Paediatr Child
Having been off medication for several result than adults with the disease [1]. Health. 2020;56(3):389–393.
years, at age 6 he developed daily
It is hypothesized that Kikuchi–Fujimoto 6. Lin YC, Huang HH, Nong BR, Liu PY, Chen
fever and massive bilateral cervical
disease is driven by a cytotoxic T-cell YY, Huang YF, Chiou YH, Lee HS. Pediatric
lymphadenopathy. Laboratory test results Kikuchi-Fujimoto disease: a clinicopathologic
mediated inflammatory response to a
showed elevated erythrocyte sedimentation study and the therapeutic effects of
viral trigger in genetically predisposed
rate (ESR) (peak: 130 mm/hr), hydroxychloroquine. J Microbiol Immunol
individuals. About 3% of patients later
hyperferritinemia (peak: 1228 µg/L), and Infect. 2019;52(3):395–401.
develop systemic autoimmune disease,
mild cytopenias (hemoglobin nadir:
which may be triggered by immune system
8.5 g/dL; platelet nadir: 191 × 109/L;
exposure to autoantigens via the apoptotic
white blood cell count nadir: 2.9 × 109/L).
debris created in affected lymph nodes [2].
Computed tomography (CT) scanning
Diagnosis is based on excisional lymph
of the neck showed bilateral cervical
node biopsy, which shows areas of
lymphadenopathy with a confluent
necrosis surrounded by histiocytes and
appearance (Fig. 1). Infectious workup was
plasmacytoid dendritic cells.
again unrevealing, and repeat excisional
cervical node biopsy was performed. Kikuchi–Fujimoto disease is widely
The pathology findings showed areas believed to be a benign and self-limited
of necrosis with surrounding CD123+ process. However, retrospective studies
plasmacytoid dendritic cells and mixed have shown that up to 30% of hospitalized
cellular infiltrates, consistent with Kikuchi– patients with this diagnosis may develop
Fujimoto disease (Figs. 2, 3, 4). Review MAS, often requiring immunosuppressive
of his initial biopsy performed at age 2 therapy [3,4].
showed similar mixed cellular infiltrate with Kikuchi–Fujimoto disease in children is
high staining for CD123+ plasmacytoid often recurrent (10%-42% of cases),
dendritic cells but did not show the with up to 3 recurrences in a single
necrosis characteristic of Kikuchi–Fujimoto patient [5]. Treatment consists of
disease. It was determined that his current supportive care for mild disease and
presentation was likely a recurrence of glucocorticoids for severe or persistent
his earlier illness, most consistent with disease, with no treatment trials available.
recurrent Kikuchi–Fujimoto disease
11 | Management of Complex Cases
November 2021 | Volume 10 Issue 2Case 4: Kikuchi–Fujimoto Disease in a 6-Year-Old Boy with a History of Macrophage Activation Syndrome Case Images
Figure 1
CT (without IV contrast) of the soft tissues of the neck shows right > left enlarged, confluent, bilateral cervical lymph nodes,
with arrows pointing to the area of greatest lymphadenopathy.
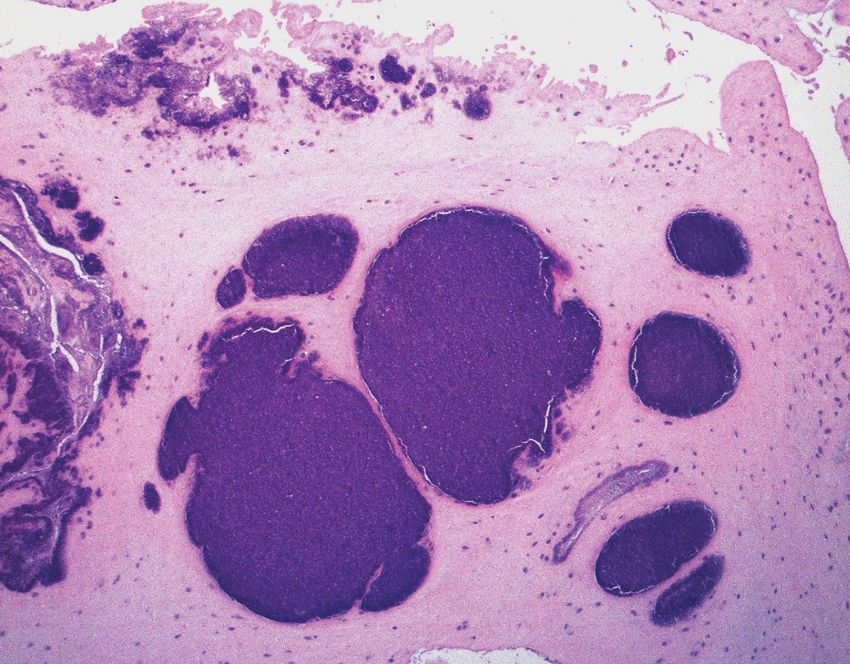
Figure 2
High power, hematoxylin-eosin (H&E) stain shows abundant apoptotic debris and mixed cellular infiltrate comprised of
histiocytes, immunoblasts, and small lymphocytes. Neutrophils and plasma cells are essentially absent.
12 | Management of Complex Cases
November 2021 | Volume 10 Issue 2Case 4: Kikuchi–Fujimoto Disease in a 6-Year-Old Boy with a History of Macrophage Activation Syndrome Case Images Continued
Figure 3
CD123 stain shows many plasmacytoid dendritic cells, predominantly around areas of necrosis.
Figure 4
CD3 stain shows abundant T lymphocytes in the infiltrate.
13 | Management of Complex Cases
November 2021 | Volume 10 Issue 2Management of Complex Cases
Grand Rounds from HSS | Rheumatology
HSS Editorial Board
Editors Laura Robbins, DSW
Karmela Kim Chan, MD Senior Vice President
Assistant Attending Physician Education Institute & Global Partnerships
Assistant Professor of Medicine Associate Professor
Weill Cornell Medicine Graduate School of Medical Sciences
Memorial Sloan Kettering Cancer Center Clinical Epidemiology and
Health Services Research
David M. Dines, MD Weill Cornell Medicine
Attending Orthopaedic Surgeon
Clinical Professor of Orthopaedic Surgery Joy Jacobson, MFA
Weill Cornell Medicine Director, Academic Publications
Managing Editor, HSS Journal
HSS Education Institute
Consultants
Andy O. Miller, MD
Design/Production
Chief, Division of Infectious Diseases
Associate Attending Physician Marcia Ennis
Associate Professor of Clinical Medicine Senior Creative Director
Weill Cornell Medicine Education Marketing & Digital Communications
HSS Education Institute
Sarah Faith Taber, MD
Assistant Attending Physician Randy Hawke
Assistant Professor of Pediatrics Associate Director
Weill Cornell Medicine Education Marketing & Digital Communications
HSS Education Institute
Board Produced by Education Marketing
Dalit Ashany, MD & Digital Communications
Assistant Attending Physician
Assistant Professor of Clinical Medicine
Weill Cornell Medicine
Anne R. Bass, MD
Attending Physician
Professor of Clinical Medicine
Weill Cornell Medicine
Bryan T. Kelly, MD, MBA
Surgeon-in-Chief and Medical Director
Chief Emeritus, Sports Medicine Institute
Attending Orthopaedic Surgeon
Professor of Orthopaedic Surgery
Weill Cornell Medicine
Carolyn M. Sofka, MD, FACR
Attending Radiologist
©2021 Hospital for Special Surgery. 535 East 70th Street,
Director of Education New York, NY 10021. Hospital for Special Surgery, HSS and the
Department of Radiology and Imaging HSS logo are trademarks or registered trademarks of Hospital for
Professor of Radiology Special Surgery in the United States and other countries.
Weill Cornell Medicine
HSS Education Institute
14 | Management of Complex Cases
November 2021 | Volume 10 Issue 2You can also read

















































