The Dolutegravir Transition in West Africa - Best Practices, Lessons Learned, Next Steps - CQUIN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The Dolutegravir Transition in West Africa
Best Practices, Lessons Learned, Next Steps
A CQUIN & CHAI Webinar
April 5, 2022
Welcome
Maureen Syowai
Regional Technical Specialist
ICAP in Kenya
The CQUIN Project 2
Welcome/Bienvenue/Bem-vindos • Be sure you have selected the language of your choice using the “Interpretation” menu on the bottom of your screen. • Assurez-vous d’avoir sélectionné la langue de votre choix à l’aide du menu en bas de votre écran Zoom. • Certifique-se de ter selecionado o idioma à sua escolha usando o menu de interpretação na parte inferior do seu ecrã The CQUIN MCH Workshop May 25-27, 2021

Moderators
Marco Vitoria Aleny Couto
Medical Officer, Treatment & Care Director, STI and HIV/AIDS Control
Global HIV, Hepatitis, & STI Programme
Programmes Ministry of Health (MISAU)
World Health Organization Mozambique
The CQUIN Project 4
Presenters
Carolyn Amole Djahoury Mathurin Kouadjale Etiobhio Ehimen
Senior Director Soins et Traitementa/Chef de Senior Medical Officer
HIV Access Program Service MOH/NASCP, Nigeria
CHAI PNLS, Cote d’Ivoire
The CQUIN Project
Accelerating access to DTG-based regimens for adults and
children in West Africa
Carolyn Amole
April 2022
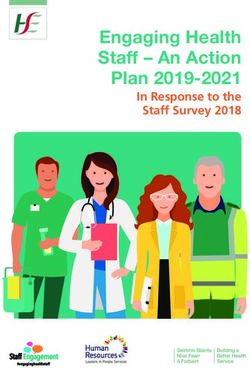
In West Africa, significant efforts have contributed to increasing treatment coverage
for adults and children living with HIV
West Africa ART Coverage (2020)1,2
Adult Regional ART Coverage Pediatric Regional ART Coverage
100% West Africa 100% West Africa
West Africa (excl. Ni geria) West Africa (excl. Ni geria)
GA LMICs 79% GA LMICs
80% 70% 80%
64% 75%
Pediatric ART Coverage
Adult ART Coverage
55% 61%
60% 50% 53%
60% 49% 45% 48%
65% 41%
56% 36% 37%
40% 54% 40% 31% 34%
49% 30%
43% 23% 26%
20% 20%
0% 0%
2015 2016 2017 2018 2019 2020 2015 2016 2017 2018 2019 2020
1. West African countries include: Benin, Burkina Faso, Cape Verde, Cote d'Ivoire, The Gambia, Ghana, Guinea, Guinea-Bissau, Liberia,
Mali, Mauritania, Niger, Nigeria, Senegal, Sierra Leone, and Togo. Pediatric data unavailable for Cape Verde.
Country Highlights
Senegal doubled the number of
adults on ART between 2013 - 2020
In Nigeria, 86% of PLHIV were
receiving ART in 2020
Despite progress across the region, significant efforts are still required to ensure PLHIV have access to the best treatment options and to close
the treatment gap between adults and children
7
Source: UNAIDS AIDSinfo ; CHAI 2021 HIV Market Report.
A TLD ceiling price agreement set the stage for Dolutegravir (DTG) use, laying the
foundation for widespread adoption and impact
TLD comprised a majority of 1L adult market share within 3 years of product
introduction in GA LMICs, compared to an estimated 5 years for TLE/TEE
TLE/TEE and TLD Adult 1L Use in Generic Accessible (GA) LMICs*
25 M 90%
TLE**/TEE
80%
Est. Number of Patients
Number of Adults on ART (M)
Adult 1L Market Share (%)
20 M 13.3 M 70%
5.4 M
Market Share
60%
15 M .32 M
50% TLD
13.2 M 13.9 M 40% Est. Number of Patients
10 M 11.3 M 11.7 M
30% Market Share
9.3 M
5M 7.1 M 20%
6.1 M
Note: Market share may not
3.9 M 10%
2.5 M sum to 100% due to use of
.5 M 1.4 M
M 0% other regimens
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Achievement of >50% 1L
Adult Market Share: TLE/TEE: 5 years TLD: 3 years
Global Impact: By the Numbers
US $1B 18M+ 90 countries
Estimated Global TLD Savings Patients are accessing Initiated TLD Procurement
between 2018-2021 TLD in LMICs
* GA countries are defined as those LMICs that are
covered under voluntary licenses for generic TDF/TAF. 8
Source: CHAI Annual HIV Market Report Forecasts; APWG Order Summary. ** TLE includes TLE400 and TLE600
In West Africa, countries took unique approaches to TLD rollout; all countries are on track to reach over 85% of
1L adults on TLD by the end of 2022
Percentage of 1L Adults on TLD in Select Countries in WCA
100%
90% Early Adopter
80% Country
70%
GA LMICs
60%
50%
40%
30%
20%
10%
0%
2018 2019 2020 2021
Heterogeneity exists across the region, contributing to the diverse pace of TLD introduction
May 2018 NTD Safety Signal COVID-19 pandemic hindered
required countries to adapt in their rollout across several countries
country contexts and disrupted key services
Procurement and forecasting Donor and implementing
approaches vary, with some countries partner landscape varies
working to minimize TLE400 wastage across countries
before scaling up TLD
Source: National Program Data Shared with CHAI, CHAI Annual HIV Market Report Forecasts.
Lessons learned from TLD introduction are critical for informing future new product introduction in the region
Catalytic Procurement in Nigeria contributed to the rapid pace of and transition to DTG-
based regimens, offering global lessons for countries within and beyond West Africa
Countries in West Africa with
180-tab packs of TLD delivered1
Rollout and scale-up of MMD helped to ensure
continued access to ARVs during COVID-19
Burkina Faso Cote d’Ivoire Nigeria Togo
Refresher Trainings, including adapting to virtual modalities, and an increased use of
smartphone-based appointment systems ensured adherence during COVID-19
Active partnerships and engagements with PEPFAR and Global Fund, including through
development of transition plans, is enabling sustainable and continued access to TLD
PLHIV networks play a critical role in information
sharing, advocacy, and demand generation, ensuring
that national HIV programs meet the needs of PLHIV
Radio Broadcast on New Products – Togo
These factors will be critical as countries work to complete their adult TLD transitions and initiate DTG 10mg introduction for children
in 2022
Source: APWG Order Summary, Q1 2022.A public-private partnership between Unitaid, CHAI, ViiV, and generic suppliers
greatly accelerated the development and introduction of DTG 10mg
Key Enablers for DTG 10mg introduction:
Through an end-to-end development program and
partnership, two selected generic suppliers received a
financial incentive from CHAI and Unitaid, technical
knowledge transfer from ViiV, and engaged in an
innovative US FDA filing strategy
The tentative approval of DTG 10mg is the fastest ever
regulatory approval of a generic pediatric ARV. The
two suppliers – Viatris and Macleods – now have US
FDA tentative approval and no capacity or supply
challenges are anticipated
Through a Unitaid and CHAI pricing agreement,
DTG 10mg is available at EXW US$4.50/90 pack for Expedited development and
all public procurers for use in over 123 countries. delivery is enabling children
Reduced price could generate up to US$260 million
in global health savings over five years in LMICs to access optimal
treatment years before it
CHAI partnered with a global coalition of donors, would have otherwise been
WHO, Ministries of Health, and other partners to
plan catalytic procurement in early adopter countries available
Sources: Medicines Patent Pool (MPP) Dolutegravir – Paediatrics (DTG) webpage, Acc. Aug 2021. Link; CHAI press release
(Nov 30 2020). Link; DRUGS@FDA, Link; pDTG Pricing Agreement press release (Nov 2020). Link; CHAI analysis 11DTG introduction was greatly accelerated compared to previous pediatric products
Timeline of Pediatric Treatment Optimization
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
LPV/r recommended by WHO as first-line
LPV/r recommended NVP and d4T no
by WHO as longer recommended
Widespread
preferred first-line as first-line for 50% DTG use by
adoption adoption children on ART in GA LMICs
Development, approval, and adoption of DTG for children has been significantly
accelerated compared to historical products
Sources: CHAI analysis; with thanks to Dr. Christine Malati, USAID, whose analysis was an inspiration for this slide 12Globally, over 40 countries have placed orders for DTG 10mg, contributing to widespread adoption and introduction of DTG for children
Pediatric DTG is a game-changer, and it will be critical to apply learnings to close the treatment gap between
adults and children in West and Central Africa
Pediatric HIV progress in WCA lags Key Learnings for DTG 10mg Transition
significantly behind adults
Adults Training and Capacity Building
• Ensure caregivers and healthcare workers
have the tools and information to prescribe
81% 77% 62%
DTG 10mg
Enhanced Implementation Monitoring
Children
• Strength data systems and conduct close
monitoring to rapidly identify gaps, generate
feedback, and document early evidence to
35% 35% 24% inform national and global scale-up
Stakeholder Coordination
Know Status On ART VLS
• Partner with key stakeholders, including
community, implementing partners, and donors
Gap to 95-95-95 Targets as of 2020 to 1) address any implementation challenges or
bottlenecks and 2) ensure children access DTG
10mg as soon as possible
Source: UNAIDS 2021 epidemiological estimates 14TRANSITION SOUS RÉGIMES OPTIMAUX CHEZ LES
ENFANTS VIVANT AVEC LE
A
VIH EN CÔTE D’IVOIRE :
LEÇONS APPRISES
Réunion Ouest africaine
Dr Kouadjalé. M
Chef de service soins et traitements
PNLS/MSHP-CMU
Abidjan, Côte d’Ivoire
15CONTEXTE
• Ministère en charge de la santé au travers du PNLS : Engagement National fort afin de
réduire l’infection à VIH chez les enfants et les adolescents par l’adhésion aux initiatives
nouvelles et stratégies innovantes mondiales en faveur de la prévention et du traitement de
l’infection à VIH avecl’appui des Partenaires Techniques et Financiers
• Engagement de Haut Niveau de la 1ère Dame, Mme Dominique Ouattara AMBASSADEUR
SPECIAL DE L’ONUSIDA POUR L’ELIMINATIONADE LA TRANSMISSION MERE-ENFANT DU VIH ET
POUR LA PROMOTION DU TRAITEMENT PEDIATRIQUE
• Quelques données (Fin 2020)
• 379 593 PVVIH dont 64,9 % de femmes et 5,6% d’enfants (0-14 ans) selon Spectrum
2021.
Fin Septembre 2021 le nombre d’enfants actifs sous ARV était de 11 288.
• 9 428 décès dont 45,90% femmes et 8,45% d’enfants de 0 à 14 ans
• Suppression de la charge virale chez les enfants 49% VS 61% chez les adultes 16ETAPES DE LA TRANSITION AU DTG 10 MG CHEZ
LES ENFANTS DE MOINS DE 20 KG
A
17DIRECTIVES NATIONALES TARV ENFANTS ❑Mise à jour des directives nationales du TARV chez les enfants et les adolescents infectés par le VIH (Note circulaire du MSHP-CMU :09 juin 2021) ❑Mi juin 2021 , un plan détaillé de transition au DTG 10mg a été élaboré avec l’ensemble des parties prenantes •Phase 1 (juillet à Décembre 2021) ✓Nouvelles inclusions sous TARV ✓10-14,9kg déjà sous TARV ✓Echec thérapeutique sous TARV depuis au moins 6 mois •Phase 2 à partir Janvier 2022 (mais anticiper en Novembre 2021) ✓Tous les autres enfants de moins de 20 kg en poursuivant la phase 1
PLAN DE TRANSITION AU DTG 10 MG 1/3 Plan de transition spécifique au DTG 10 mg pour les enfants de poids < 20 kg Activités/tâches Actions menées Période Responsable commentaires - Définition du type et étapes du - Rencontres avec les principales Avril – Juin 2021 EGPAF et PNLS Plan de transition en 2 phases plan de transition au pDTG parties prenantes • Phase 1 : juillet à Décembre - Identification des cibles - Elaboration et transmission des 2021 - Quantification des besoins en canevas aux PMOs pour la - Nouvelles inclusions sous TARV DTG 10 par structure de santé quantification des besoins de poids < 20 Kg - Elaboration des modules (adaptation de l’outil développé A - Enfant de 10-13,9 Kg déjà sous d’orientation sur l’utilisation du par CHAI) TARV DTG 10 - Enfant
PLAN DE TRANSITION AU DTG 10 MG 2/3
Plan de transition spécifique au DTG 10 mg pour les enfants de poids < 20 kg
Activités/tâches Actions menées Période Responsable commentaires
Elaboration et diffusion du - Analyse des besoins estimés 15 au 30 Juin 2022 PNLS La majorité des
plan d’allocation du pDTG par transmis pour chaque structures de santé ont
structure sanitaire EC structure de santé reçues leur 1ère
- Transmission du plan dotation en DTG 10
d’allocation du pDTG à la
NPSP (centrale nationale A NB: fin Dec 2021 la CI a
d’achat, de stockage et reçu un total de 47 070
livraison des produits de boites de 90 Cp de DTG
santé) 10 mg
Coaching des prestataires sur Les PMOs ont organisés des A partir de Juillet PMO ,PNLS et > 1260 prestataires
site sur l’utilisation, missions sur chacun des sites 2022 Districts coachés
dispensation et gestion des pour un renforcement des sanitaire Activité continue
stocks du pDTG avec un capacités (médecins,
accent sur l’identification et pharmaciens, conseillers
déclarations des effets communautaires…)
indésirables
20PLAN DE TRANSITION AU DTG 10 MG 3/3 • 1er Juillet 2021 : Début effectif de l’utilisation du DTG 10 mg au niveau des structures de santé pour les cibles de la phase 1 du plan de transition (Nouvelles inclusions, Cas d’échec thérapeutique et file active des 10-13,9Kg) • Mise en place du suivi de la mise en œuvre du plan de transition: % des enfants éligibles effectivement mis sous DTG 10, communication/interaction avec les familles de bénéficiaires, difficultés… • Mensuel par les PMO A • Trimestriel au niveau du PNLS • Mi Novembre 2021: Début de la phase 2 du plan de transition au DTG 10 pour tous les enfants < 20 Kg éligibles • Réception de DTG 10 mg (boite de 90 Comprimés dispersibles) au niveau de la NPSP • Avril 2021: 6 870 • Mai 2021: 7 700 Au total: 47 070 boites de 90 Cp de DTG 10 mg reçus à fin Dec 22 • Novembre 2021: 32 500
TRANSITION AU DTG 10 MG: RÉSULTATS
• Mise en place du suivi de la mise en œuvre du plan de transition sous DTG 10:Mensuel
par les PMO et Trimestriel au niveau du PNLS
• % des enfants éligibles effectivement mis sous DTG 10
• Suppression virale
• communication/interaction avec les familles de bénéficiaires, difficultés rencontrées…
• Nombre d’enfants actifs sous ARV était de 11 288 à fin septembre 2021
• Proportion d’enfants sous régimes optimaux (à base de DTG ou LPV/r) est passé de 52% à
A
fin Septembre 2019 à 72% à fin septembre 2021
• Suppression virale (CV≤1000 copies) chez les enfants est passée de 50,5% en Sept 2019 à
67,5% en Sept 2021
Suppression virale chez les enfants de 0-14 ans
80% 72%
63% 59%
60% 49% 53% 52%
40%
20%
0%
0-4 ans 0-14 ans
Fin septembre 2019 fin décembre 2020 fin septembre 2021 22SUPPRESSION VIRALE CHEZ LES ENFANTS SOUS TARV
Total enfants CV
# Enfants par
Régimes ARVPROCESSUS DE TRANSITION AU DTG 10: LEÇONS APPRISES
• Bonne implication des autorités sanitaires ce qui a permis la célérité dans la mise à
jour des directives, l’élaboration et l’exécution du plan de transition au DTG 10
• Bonne communication avec toutes les parties prenantes avec l’appui continue des
partenaires techniques de mise en œuvre facilitant l’application des directives
• Renforcement des capacités des acteurs (cliniciens, pharmaciens et acteurs
communautaires) avec la mise à disposition A d’outils d’aide à la prescription ont été
le gage d’une mise en œuvre optimale avec des services de qualité offerts aux
bénéficiaires
• Quantification des besoins (médicaments et autres intrants) facilité par la mise à
disposition d’outils de qualité. A ce jour, disponibilité suffisante et continue de
ARVs bonne adhésion des prestataires et patients au processus d’optimisation du
TARV chez les enfants et pas d’occasions manquées
24PROCESSUS DE TRANSITION AU DTG 10: DEFIS
• Continuer à monitorer la suppression virale, le respect des RDV clinique et
biologique notamment pour la réalisation de la charge virale
• Accroitre la suppression virale chez les enfants de âgés de 0 à 4ans sur toute
l’étendue du territoire quelque soit le partenaire technique d’appui à la mise en
œuvre des directives
A
• Renforcer le suivi au sein de la communauté et l’accompagnement apporté aux
enfants et à leurs familles pour une bonne observance optimale du TARV, la
satisfaction des besoins et la résolution des difficultés
25CONCLUSION
• L’optimisation des traitements ARV chez les enfants et adolescents
en Côte d’Ivoire est une réalité.
• Les protocoles à base de Dolutégravir ont contribués à une
amélioration de la suppression virale chez les enfants.
A
• Le passage au DTG 10 mg depuis Juin 2021 pour les enfants pesant
moins de 20 kg va renforcer l’adhésion des familles aux plans de
traitement, faciliter l’observance auprès des enfants et accroitre la
suppression virale
Nos remerciements aux partenaires de mise en œuvre, au PEPFAR, au Fond mondial de lutte contre le VIH,
TB et Paludisme, aux organisations du système des nation unies et aux personnes vivant avec le VIH
26Pediatric DTG Transition in Nigeria Dr. Etiobhio Ehimen Senior Medical Officer Federal Ministry of Health (NASCP)
Introduction
Background
2020 Guideline Recommendation
• WHO approved DTG for use in children less than 20kg
in 2019. NEONATES CHILDREN
• Pediatric DTG (pDTG) received US FDA approval in
2020. Preferred AZT+3TC+RAL1 ABC+3TC+DTG2
• 2020 National treatment guidelines recommends
AZT+3TC+LPV/r ABC+3TC+LPV/r
DTG-based regimen as preferred for children. Alternatives
ABC+3TC+RAL1
• Transition plan for dolutegravir 10mg for children less
than 20kg was developed and incorporated into the ABC (or AZT)+3TC+EFV
ABC (or AZT)+3TC+RAL
national HIV supply plan. Special AZT+3TC+NVP
AZT+3TC+LPV/r
circumstances3
AZT+3TC+RAL
AZT+3TC+NVP
28pDTG Transition Consideration Transition consideration Goal of transition • Transition started late Sept 2021. • Improve outcomes • It involves existing 1L and all treatment • Regimen harmonization and naive patients who are over 4 weeks of age simplification. and weighing between 3 < 20kg. • Enhance supply security • Eligible existing 1L pediatric patients Eligibility for transition weighing 20 – 29.9kg and ≥ 30kg were • Existing or new patients who can recommended to be transitioned to DTG tolerate DTG based regimen. 50mg and TLD respectively. • Clinically stable and unstable and on • Those on 2L and stable on LPV/r can be 1L regimen. transitioned to DTG50mg when they reach 20kg and to TLD when they reach 30 kg 29
Nigeria pDTG Supply overview
• Nigeria is one of the early adopter countries.
• Adequate stock in-country to support and sustain transition.
o Over 300K packs of DTG 10mg already received in-country.
o About 165K distributed to the health facilities so far.
o More shipment are on course to be delivered in-country within the year.
• Strategic delivery of DTG10mg to facilities will continue during May 2022 LMD cycle while supply of
pediatric LPV/r products have been limited.
30382
CLHIV ARVs DISAGREGATED BY
1ST, 2ND AND 3RD REGIMEN (Dec, 2021)
Chart Title Female-3rd
Female-2nd Regimen
Regimen 0%
3%
Female-1st Male-1st Regimen
Regimen 47%
48%
Male-2nd
Male-3rd Regimen Regimen
0% 2%
Male-1st Regimen Male-2nd Regimen Male-3rd Regimen
Female-1st Regimen Female-2nd Regimen Female-3rd Regimen
32VIRAL LOAD SUPPRESSION BY
AGE AND SEX (Dec, 2021)
89% 92% 90%92%
87% 85% 86%
80% 80%83% 81%83% 83%
74% 75%
65%
< 1yr 1-4 yrs 5-9 yrs 10-14yrs 15-19 yrs 20-24 yrs 25-49 yrs 50+ yrs
Male Female
33Progress
34Facilitators of the Transition
• Revised treatment guideline to accommodate usage of pediatric DTG 10mg
• Development of a transition plan (feedback mechanism)
• Availability of sufficient stock
• Training of HCWs
• Follow up by IPs and States (engagement meetings)
• Monitoring and Supportive Visits to states and fcailities
35Barriers
• Available of Lopinavir remnant in the system
• Hesitant of Clinicians to transition
• Data quality issues
36Recommendations to Countries
• Update ART Treatment guidelines to include paediatric DTG
• Develop transition plan to align with the procurement system
• Ensure availability of adequate stock of DTG10mg
• Training of HCWs
• Adequate monitoring of the transition progress
• Conduct an operational research on p DTG to ascertain its tolerability/acceptability
and adverse effect
37THANK YOU!
38Q&A Discussion
Carolyn Amole Djahoury Mathurin Kouadjale Etiobhio Ehimen
Senior Director Soins et Traitementa/Chef de Senior Medical Officer
HIV Access Program Service MOH/NASCP, Nigeria
CHAI PNLS, Cote d’Ivoire
The CQUIN ProjectPanel Discussion
Nandita Sugandhi Patricia Fassinou Christine Malati Valentin Nassara Bineta Coulibaly
Pediatrician & MCH Ekouevi Senior Clinical Secretary General MOH Senegal
Advisor, CQUIN Pediatrician Pharmacist Benin Network of
ICAP at Columbia EGPAF, Cote d’Ivoire USAID Associations of Persons
University Living with HIV
The CQUIN Project 40Next Steps
Slides and recordings from today’s session will be
posted on the CQUIN website:
https://cquin.icap.columbia.edu/
The next CQUIN Webinar on TPT & DSD on May 3You can also read