THE ASEAN DENGUE DAY: SUSTAINING THE "UNITED FIGHT AGAINST DENGUE"
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

e-Health Bulletin Issue No. 11 | January - June 2017
Special Edition for ASEAN Dengue Day 2017
THE ASEAN DENGUE DAY:
SUSTAINING THE “UNITED FIGHT AGAINST DENGUE”
The ASEAN Dengue Day is an advocacy and other relevant stakeholders at the Member States, ASEAN Secretariat,
event held every 15 June to increase regional, national and community levels Development Partners, private
public awareness of dengue; to mobilize calls for a “United Fight Against Dengue”. sectors, civil society organisations, and
resources for its prevention and control; community groups or members.
and, to demonstrate the commitment of After the regional launching of ASEAN
ASEAN in to tackling the disease. Dengue Day including its core messages This ASEAN E-Health Bulletin Special
and logo in Indonesia in 2011, Myanmar Edition on Dengue is published to
The advocacy event was agreed upon hosted the regional conference and commemorate the ASEAN Dengue Day
during the 10th ASEAN Health Ministers observations of ASEAN Dengue Day 2017. The bulletin provides updates
Meeting in Singapore in 2010. Indonesia in 2012, followed by Viet Nam in 2013, from AMS highlighting the dengue
hosted the Launching of ASEAN Dengue Philippines in 2014, Lao PDR in 2015 situation, national prevention and control
Day in Jakarta in 2011. The event has and Thailand in 2016. These regional programmes, as well as challenges and
been commemorated simultaneously conferences and observations were future priorities.
through various activities that have been attended by representatives of ASEAN
conducted at regional, national and sub-
national levels amongst ASEAN Member
States. These activities have been
supported by WHO and international and
local partners.
As the most rapidly-spreading mosquito-
borne viral disease in the world, Dengue
is major public health concern in the
region. ASEAN is currently experiencing
increasing number of dengue infections.
Growing population densities, unplanned
urban development, poor water storage
and unsatisfactory sanitary conditions
contribute to the worsening burden of
this mosquito-borne disease.
The disease has significant impact on
the socio-economic status of the ASEAN
Member States (AMS). Dengue cannot
be fought by the health sector alone.
Tackling dengue is everyone’s concern.
As such, ASEAN together with WHO
ASEAN e-Health Bulletin 1
D engue Situation in disease notifications received from medical control of Dengue, amongst which
practitioners as well as laboratories. includes collaboration with other
Brunei Darussalam It is supported by the provision of the stakeholders and involvement of the
Infectious Disease Act Cap 204 which community. This is in line with one of the
Brunei Darussalam lies on the northwest
has a list of 59 communicable diseases strategic priorities of the MOH: “Health
coast of the Island of Borneo, facing the
gazetted for mandatory notification. All is Everyone’s Business”, whereby
South China Sea. The country has a land
health care providers from public and the community and other relevant
area of 5,765 sq km., and a coastline of
private healthcare settings, including stakeholders play an important role in
about 161 km1. It is divided into four main
laboratories, are required to notify all the fight against Dengue. A multisectoral
districts: Brunei Muara, Tutong, Belait
gazette diseases, including vector-borne approach, including participation and
and Temburong, with the largest district
diseases such as Dengue, to respective empowerment of the community through
being the Belait. The capital of Brunei
District Health Offices and Disease grassroots leaders, has been vital in
Darussalam, Bandar Seri Begawan, is
Control Division (DCD). Notifications ensuring private and public areas are
located in the smallest district of Brunei
are received through electronic kept in a clean state and in reducing
Muara, which is inhabited by more than
system, Bru-HIMS (Brunei Darussalam breeding sites for mosquito vectors.
70% of the total population.
Healthcare Information and Management
System), fax and dispatch-paper based Entomological surveillance is also
The Ministry of Health (MOH)
notifications. routinely carried out in villages, housing
is responsible for the provision,
and business premises throughout the
management, delivery and regulatory
DCD under Public Health Services is country to determine vector behavior,
functions of health in Brunei Darussalam.
the central level notification center for mosquito densities and its identification.
The Government of Brunei Darussalam
disease surveillance including data For areas identified as hotspots, other
provides free medical and health care to
collection, analysis, and communicable than provision of advice and health
the citizens. The MOH aspires to improve
disease case investigations including education, pesticide application such as
the health and wellbeing of the people of
contact tracing. DCD ensures timeliness, fogging and larviciding are carried out.
Brunei Darussalam through a high quality
complete reporting and information These pesticides are periodically tested
and comprehensive health care system
collection and also promoting awareness to ensure that the mosquito vectors
which is effective, efficient, responsive,
of occurrence of infectious diseases are susceptible and effective. Aedes
affordable, equitable and accessible to
locally and internationally. Albopictus has been identified as the
all in the country.
most common vector relevant to Dengue,
Disease prevention and control efforts and secondly Aedes Aegypti in certain
MOH equally places high priority on public
for vector borne diseases is mainly areas identified through entomological
health aspects to ensure that the people
implemented in coordination and surveillance throughout the country.
of Brunei Darussalam continue to enjoy
collaboration with Environmental Health
a high standard of living. As a result of
Division and Environmental Health Units Brunei Darussalam is also involved in
its monitoring and surveillance activities
in respective District Health Offices. regional surveillance of Dengue and
and various preventive programs, such
Vector control activities and entomological other vector borne diseases in sharing
as vector borne diseases surveillance,
surveillance are conducted particularly information on imported cases of vector
the country has a low burden of major
for vector-borne disease cases and in borne diseases especially Dengue Fever
communicable diseases.
hotspots where previous cases such as and Dengue Hemorrhagic Fever through
The Communicable Disease Surveillance Dengue have been reported. International Health Regulation (IHR)
System is well established based on National Focal points, World Health
Public Health Services follow the Organization and UNited In Tackling
1 Brunei Darussalam in brief. Department of principles underlying ‘Integrated Vector Epidemic Dengue (UNITEDengue).
Information, Prime Minister’s Office, Brunei Management’ in the prevention and
Darussalam. 2013.
Next Page
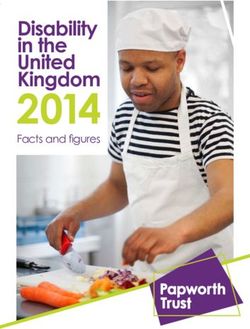
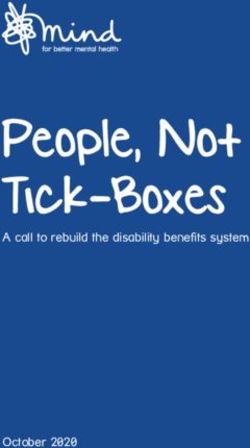
Figure 1: Monthly Number of Dengue Cases (2016-2017) Figure 2: Trend of Dengue Cases (2012-2017)
Monthly Dengue cases with epidemic threshold (2016-2017 )
120 Dengue trend by month 2012-April 2017
100
90
100 90
80 73
68
80 70 65
61
No. of cases
No. of cases
60 53 52 5456
60 50 44 44 42 40
3739
40 3234 3132 32 3029 30
40 30 25 26 25 26
21 20 2221
1717 16 1715
20 13 15
20 11 11 11 13 11 12
9 10 9
8 869 8 667
10 5 6 55 6 6
3 5
11 12 9 10 9 10
3
8 5 5 6 6 6 6 7 0
0 3 3
Sept
Sept
May
May
May
May
May
Nov
Nov
Nov
Nov
Nov
Sep
Sep
Sep
Mar
Mar
Mar
Mar
Mar
Mar
Jan
Jan
Jan
Jan
Jan
Jan
Jul
Jul
Jul
Jul
Jul
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
2012 2013 2014 2015 2016 2017
2016-2017 Warning Level Epidemic Threshold
© Ministry of Health, Brunei Darussalam © Ministry of Health, Brunei Darussalam
2 ASEAN e-Health Bulletin
Trend of Dengue cases (2012-2017) Figure 1: Cumulative Incidence of Dengue Cases by District in
Cambodia
In Brunei Darussalam, the number of
Dengue cases varies over the last few
years with the highest number of Dengue
cases recorded in 2014 at 436 cases.
The lowest number of Dengue cases
from 2012-2016 was recorded in 2016
at 84 cases. For the year 2017 until end
of April, the number of Dengue cases
remained low and below the epidemic
threshold as shown in Figure 1 (please
see page 2).
D
© Ministry of Health, Cambodia
engue Infections in Figure 2: Forecasting: Dengue Situation in Cambodia, 2015
Cambodia (IR:
WHO guideline these are “suspected” rash, and hemorrhagic signs. Leucopenia Data collection and analysis
dengue cases) and do not completed may be present. For DHF, besides the
from laboratory confirmation. For DF, the above listed DF-signs and hepatomegaly Surveillance data are collected and
presence of fever with 2 or more of the or abdominal pain the following analysed through the following:
following signs is required: Red face or hematological findings are required: • Passive surveillance (aggregating
conjunctival injection, headache, retro- Increase in hematocrit ≥20% and drop in forms) - since 1980, reporting from all
orbital pain, painful muscles or joints, platelets below 100,000/mm. public health facilities
• Active (Sentinel) surveillance (line-
listing forms) - since mid - 2001,
Figure 4
through three foundation pediatric
hospitals, AHC and KBH (in PP & SRp)
and four public pediatric hospitals: 1 in
Phnom Penh (NPH) and 3 in provinces
(Takeo, Kg Cham, Kampot)
• Sero-Virologic surveillance - since
2000, through five hospitals: NPH,
AHC, Kg Cham RH, Takeo RH and
Battambang RH, and Performed by
Institute Pasteur - Cambodia (IPC).
See Figure 3 for the flow reporting.
In Cambodia, the sentinel surveillance
system for dengue is aimed to:
• Acquire high quality surveillance
data from a relatively small number
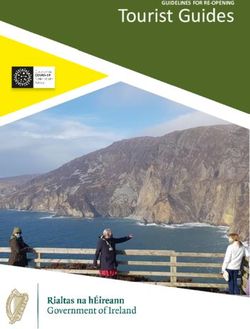
Proportion of Dengue Virus Serotype-Confirmed* by Years of the Five Sentinel Sites
Cambodia, 2002-2016
of facilities in order to monitor dengue
100.0 trends in Cambodia
• Rapidly detect large-scale epidemics
DNV-IV
90.0 DNV-III
80.0
70.0 See Figure 4 for details of the sentinel
surveillance system, including sero-virologic
% of DNV-Serotype
60.0
DNV-II
50.0
surveillance.
40.0
30.0 The system allows classification
20.0 between DF, DHF, or DSS through the
10.0
DNV-I
use of discharge data. Only hospitalized
0.0
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 cases are monitored, data from health
Laboratory name: Institut Pasteur du Cambodge (IPC)
Year
centers are excluded.
© Ministry of Health, Cambodia
For virologic surveillance, sentinel
hospitals collect blood samples to 5-10%
Figure 3 of the total suspected cares and send
these specimens to Pasteur Institute
(IPC).
• Data analysis regularly conducted on
a weekly basis at NDCP
• Types of output generated according
to the objectives of NDCP and the
surveillance system
• Analyses performed using Epi-info
and Excel software and MapInfo/GIS-
Arcview 3.3
• Individual data from the sentinel
hospitals are compiled weekly so that
routine analyses can be done in a
timely manner
© Ministry of Health, Cambodia
4 ASEAN e-Health Bulletin
1 House 1 Jumantik reducing dengue morbidity and mortality Plus means every effort to avoid human-
nationwide through strengthening local vector contact such as using repellent,
Movement a Call for and national capabilities, as well as mosquito net for kid when napping, using
Action regional coordination. larva predator (fish) in water container
and using mosquito repellent plants like
Introduction Dengue hemorrhagic fever in Indonesia lavender, etc.
firstly reported in 1968 from two big
Dengue infection is the most common cities: Jakarta and Surabaya. The All activites above need active
mosquito-borne viral disease of humans number of reported cases was 58 cases participation from the community. In the
that in recent years has become a major with 41% of them reportedly died. Since celebration of 2015 ASEAN Dengue Day,
international public health concern. then, the reported cases and the number Ministry of Health launched a movement
Globally, 2.5 billion people live in areas of infected districts/area are increasing. named 1 House 1 Jumantik as the
where dengue viruses can be transmitted. most effective way to prevent dengue
The geographical spread of both the Although National Dengue Prevention virus transmission. Jumantik stands
mosquito vectors and the viruses has and Control Program has been for Juru Pemantau Jentik (someone
led to the global resurgence of epidemic established and implemented, both who responsible for monitoring larvae
dengue fever and emergence of dengue the incidence and case fatality rate are mosquito). This activity is based on a
hemorrhagic fever (dengue/DHF) in the still high. There are still two challenges family approach, meaning that every
past 25 years with the development of that need to be handled, namely how household encourages to have 1
hyperendemicity in many urban centers to increase people awareness against Jumantik in that house called Jumantik
of the tropics. Transmitted by the main dengue and how to involve people rumah. For public places such as market,
vector, Aedes aegytpi mosquito, there directly to conduct vector control in their airport, seaport, mosque, church, etc
are four serotypes of virus that cause houses. the Jumantik is called as Jumantik
dengue. Recovery from infection by one Lingkungan.
provides lifelong immunity against that Preventing or reducing dengue virus
serotype but confers only partial and transmission depends entirely on Pic. 1. Declaration of 1 House 1 Jumantik in
transient protection against subsequent vectors control (aedes sp) or interrupt ASEAN Dengue Day 2015
infection by the other three. There is a the human–vector contact. Activities to
good evidence that sequential infection control transmission should target Ae.
increases the risk of a more serious aegypti (the main vector) in the habitats
disease resulting in DHF. of its immature and adult stages. Ae.
aegypti proliferates in many purposely-
National Dengue Control Programme filled household containers such as
in Indonesia is currently implementing those used for domestic water storage ROADSHOW PROGRAM 1 RUMAH 1 JUMATIK
WHO Global Strategy 2012-2020 that and for decorative plants, as well as
promotes coordination and collaboration in a multiplicity of rain-filled habitats –
among multisectoral partners, an including used tires, discarded food and
integrated vector management approach beverage containers, blocked gutters
and sustained control measures at all and buildings under construction.
levels. Dengue is an ecological disease
therefore coordination and collaboration 1 House 1 Jumantik Movement © Ministry of Health, Indonesia
by all sectors within the government,
communities, civil societies, private Since there are no vaccine and drugs to 1. Jumantik Rumah:
sectors, and media need to be treat this disease, the most effective way Jumantik rumah is one of the family
strengthened. All sectors should is to prevent dengue infection by cutting members living in one house who is
harmonize the prevention, surveillance the life cycle of vector. The main activity assigned to do monitoring larva once
(entomological and epidemiological) is to undertake the source reduction a week. They can be mother, father
and case management with the existing of mosquito habitats, both inside and or other family members. The task
health systems, in order to make the outside house. There are three activities, and role of Jumantik Rumah are as
program sustainable, cost-effective well known as 3M Plus in Indonesia to follows:
and ecologically sound. The goal of cut the life cycle of mosquito, namely: 1). Campaigning for PSN 3M to all
this Global Strategy is to reduce the 1. Menguras: Cleaning and brushing family member as the most
burden of dengue. Its specific objectives water container/water storage once effective way to prevent dengue
are: 1) to reduce dengue mortality by a week. 2). Collaborating with all family
at least 50% by 2020, 2) to reduce 2. Menutup: Covering all domestic members to do PSN 3M Plus
dengue morbidity by at least 25% by water storage once a week indoor and outdoors.
2020, 3) to estimate true burden of the 3). Checking possible breeding sites
3. Mendaur ulang: Reusing or recycling
disease by 2015 (the year 2010 is used and water container inside and
garbage such as: discarded food
as the baseline). The implementing
and beverage containers, used tires,
strategy is expected to pave the way for
plastic, bottle, can, etc. Next Page
ASEAN e-Health Bulletin 5
outside house from existing larva 1). Campaigning for PSN 3M Plus 1). Checking and supervising
mosquito to community individually or in a the work plan of the Jumantik
4). Recording the result of monitoring group. Coordinator.
in Jumantik card every week. 2). Mobilizing the community to 2). Providing technical guidance to
implement PSN 3M Plus in their Jumantik Coordinator.
2. Jumantik Lingkungan neighborhood. 3). Calculating Free larvae index in
Jumantik Lingkungan is one or more 3). Organizing a plan / schedule of its working area
persons assigned to monitor larva in visits to all buildings both house 4). Undertaking local area monitoring
public and working places. The task and public / working places at (PWS) and mapping per RW /
and role of Jumantik Lingkungan are least once in 2 weeks. area every month with Jumantik
as follows: 4). Conducting visits and coaching to Coordinator.
1). Checking the mosquito breeding houses / residences, public and 5). Reporting the results of Jumantik
sites and implement PSN 3M working places every 2 weeks. and PWS activities to the local
Plus in working places and public 5). Monitoring larvae inside and puskesmas.
places. outside houses and buildings 6). Conducting coaching and upgrading
2). Recording the result of larvae 6). Collecting data / recapitulation of of skills / training of PSN 3M Plus
inspection on Jumantik card once monitoring results of larvae house, activities to Jumantik Coordinator.
a week public and working places once a 7). Counting free larvae index
month. 8). Reporting Free Larvae Index to
3. Jumantik Coordinator 7). Reporting the results of larva primary health care center every
Jumantik Coordinator is one monitor to Jumantik Supervisor month.
person assigned in neighbourhood once a month.
association, the lowest level The structure of 1 House 1 Jumantik
administrative unit in community. One 4. Jumantik Supervisor organization can be seen as picture
Jumantik coordinator responsible for Jumantik Supervisor is one person below:
10 Jumantik Rumah. Task and role designed in hamlet / village or urban
Jumantik Coordinator as follows: village level. Task and role Jumantik Implementation of 1 House 1 Jumantik
Coordinator as follows: Action
After the declaration of 1 house 1
Jumantik as a national movement,
Pic. 2. Home Visit by Jumantik Coordinator
Ministry of Health started to socialize
and implement this project to some
districts. The implementation is not only
in residential area but also in working
area of health port office in airport and
seaport. Working area health port office
divided into perimeter area and buffer
area. Perimeter area means the center
of port activities (inside the port), the
location of warehouses, the loading and
unloading of goods, the government
and private offices, and buffer area is
outside of port radius of 400 m from the
perimeter limit.
This movement strongly need the
© Ministry of Health, Indonesia
participation from linked sector and
community and considered successful
Pic. 3. The Structure of 1 House 1 Jumantik Organization if free larvae index reached 95% or
more in residential area and in port area
reached 100% (perimeter area) and 99%
in buffer area.
© Ministry of Health, Indonesia
6 ASEAN e-Health Bulletin
D engue Newsletter detect irregularities so that epidemics will to communities. Students are asked to
be detected rapidly and early intervention participate in film making competition
for Lao PDR can be introduced. However, laboratory using their mobile phones to record
Dengue is one of the fastest growing testing for confirmation of dengue can prevention messages. During the school
emerging infectious diseases in the only be done at the central level. It will holidays, these students will be mobilized
world and Asia and the Pacific bears be good to strengthen testing capacity at to clean up their school compounds
75 per cent of the global burden. The the provincial level. regularly and participate in poster design
Association of Southeast Asian Nations competition to share dengue messages
This information enables the EOC to within their communities.
(ASEAN) has called for collective efforts recommend preparedness activities
at the 10th ASEAN Health Minister in provinces which shows increase Lao PDR is fully committed as a member
Meeting in 2010 and since then, ASEAN in dengue activity. Case in point - in of ASEAN to work towards dengue
Dengue Day is observed every 15th of January this year, some provinces had control and the Government and Ministry
June annually by all ASEAN Member dengue at epidemic level and immediate of Health have an instrument in engaging
States. actions were taken on larvae surveys the community. This year’s ASEAN
In Lao PDR, dengue is one of the 17 to be conducted in nine (9) districts as Dengue Day will be marked on the 15th
notifiable diseases reported under the a pilot project and community clean-up June and stakeholders are expected to
National Surveillance System. Dengue vector control activities were organized support this activity by advocating and
is being discussed in the monthly high- in these provinces. mobilizing them.
level government meeting and weekly at The Ministry of Health officials were
the Emergency Operation Centre (EOC), concerned of a possible repeat of 2013
the command and control centre of the dengue outbreak and the Health Minister
D
Ministry of Health where key decisions
are taken.
had issued an order at the beginning of engue Control
the year to enhance dengue control in
all provinces. There were collaborations Program in Malaysia
The ownership by the Ministry of Health
in organizing dengue preparedness with the Ministry of Education and Sport Dengue Epidemiology in Malaysia
activity can be seen with the and a signing of a Memorandum of
involvement of provincial and district Understanding was done to ensure that Dengue fever has remained as one of the
governors, local authorities, mass school compounds remain dengue-free major public health problem in Malaysia.
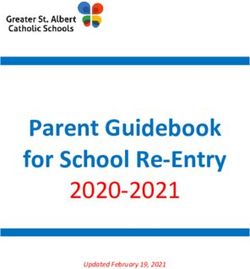
organization and key partners, including during school breaks. In the year 2016, a total of 101,357
the ASEAN-UNITEDengue, World confirmed dengue fever cases and 237
The regular updates and reports were dengue deaths were reported. This was
Health Organization (WHO), Asian shared with provincial governors
Development Bank (ADB), US Centre for however, a reduction of 16.1% in cases
and stakeholders, and strategies and 29.5% in deaths compared to the
Disease Control (US CDC), Microbiology were developed ahead of the rainy
Laboratory in Mahosot Hospital with the year 2015 (Figure 1). In 2016, dengue
season in case of an increase in cases had the incidence of 328 cases
Lao Oxford Wellcome Trust Research vector activity. Also, health officials
Unit, and Institut Pasteur du Laos per 100,000 populations, while the Case
were sent to coordinate with affected Fatality Rate (CFR) in the year 2016 was
(IPL). These partners have provided provinces to increase surveillance,
both monetary and technical support, 0.23%, a slight reduction compared to
risk communication and implement the previous year which was reported as
for larvae surveys, vector control, community clean-up activities. To date,
community mobilization, reagent and kit 0.28% (Figure 2).
the cumulative number of suspected
supplies and laboratory confirmation. Dengue from January 2017 is 847 cases Looking at age distribution and dengue
The Department of Disease Control (Week 18). Dengue 4 (66.0%) is mostly cases as well as deaths, it is apparent
(DCDC), National Center for Laboratory detected, followed by Dengue 1 (27.0%), that dengue occurrence is higher in the
and Epidemiology (NCLE) and Center Dengue 2 (6.0%) and Dengue 3 (1.0%) reproductive age groups. Meanwhile,
for Malaria Parasitology and Entomology as of 30 April 2017. CFR by age group was notably high with
under the Ministry of Health coordinate 0.72% in the 60 years old and above
Climate change is one of the major (Figure 3).
the dengue prevention and control challenges affecting dengue control
activities in the country. NCLE has been activities but the Ministry of Health Malaysia has all four serotypes of
closely monitoring the dengue situation will continue to take proactive steps dengue virus present in the population.
through Lao Early Warning System to implement dengue prevention and In the year 2016, several serotype shift
(LaoEWARN) and weekly surveillance control activities. With this, communities occurred, with DEN 1 more prominent in
report are being submitted to the central are being informed regularly by the media the early of the year and then shifted to
level for decision making. to participate in clean-up activities. DEN 3 at the end of the year (Figure 4).
The laboratory based dengue The Vientiane Capital Health Department
surveillance allows monitoring of dengue will mark the ASEAN Dengue Day this
trends and circulating dengue serotypes; Next Page
year by distributing 3 million guppy fishes
ASEAN e-Health Bulletin 7
Integrated Management a National Dengue Task Force was sustained implementation of Integrated
established to overcome issues Management, a significant impact
Focusing on environmental cleanliness regarding dengue including solid waste has been evident with the nationwide
is the way forward and long term management, environmental cleanliness reduction of dengue cases.
solution to overcome the dengue and architecture design that play a role
burden in Malaysia. Therefore, in the in being potential Aedes breeding sites Through this task force the dengue
effort to empowerment of the people that are beyond the Ministry of Health prevention activities such as source
and, community participation and social authority. reduction has been included in the
mobilization in dengue prevention school’s curriculum. Besides that,
and control will be strengthen through This task force consists of seven Guidelines for Dengue Prevention
the implementation of COMBI project Ministries which include the Ministry Education and Management in School,
especially in the hotspot areas will be the of Health, Ministry of Housing and Guidelines for Aedes Free Building
main focus of the dengue prevention and Local Government, Ministry of Human Structures and Guidelines for Dengue
control program. As of December 2016, Resource, Ministry of Education, Prevention in Construction Sites were
there are 3,082 COMBI projects with Ministry of Internal Affairs, Ministry of developed through this task force.
63,000 volunteers all over the country. Defence and Ministry of Works. The Ministry of Communications and
Besides that, other local agencies as concept of Integrated Management is Multimedia provides free periodical
well as neighbourhood groups also applied together in collaboration with media slots in radio & TV as well
assist in mass clean up activities in the multiple Ministries and agencies in as conducting dengue prevention
the community. Ministry of Health implementing dengue prevention and campaigns to increase community
of Malaysia also celebrates ASEAN control activities. This includes utilizing awareness.
Dengue Day every year in order to each Ministry resources and financial
promote dengue awareness and to gain allocations. The sustainability of this Dengue Virus Surveillance System
community participation. task force is very crucial and has been (DVSS) in Malaysia
proven till today. Initiated with weekly
In further efforts to reduce the dengue task force committee meeting from The Dengue Virus Surveillance System
burden in Malaysia, from July 2014, July 2014 until 2015 and later to two (DVSS) is an important strategy in the
following the national level meeting weekly meeting chaired by the Director National Dengue Strategic Plan (NDSP)
chaired by the Deputy Prime Minister, General of Health. After two years of
Next Page
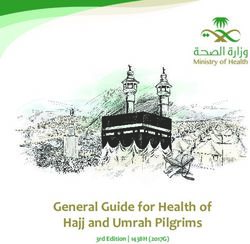
Figure 1: Reported Dengue Cases and Deaths in Malaysia Figure 3: Dengue Cases, Number of Death and Case Fatality Rate
(1995‑2016) (CFR) by Age Groups in Malaysia, in 2016
120,836
140,000 1000
Dengue Cases, No. of Deaths & CFR in 2016
108,698
101,357
900
120,000 16000 40
800 14000 35
No. of Cases
100,000 700 12000 30
No. of Deaths
10000 25
No. of deaths
600
No. of cases
80,000 8000 20
49,335
48,846
500 6000 15
46,171
43,346
41,486
39,686
38,556
60,000
336
4000 10
400
102 33,895
32,767
31,545
27,381
2000 5
10,146
16,368
237
19,429
21,900
215
32 14,255
300
7,103
36 19,884
40,000 0 0
6,543
60
134
Under 5 to 11 to 15 to 20 to 25 to 30 to 35 to 40 to 45 to 50 to 55 to
112
200
107
and
99
98
92
92
88
20,000 5 10 14 19 24 29 34 39 44 49 54 59
72
above
50
45
37
35
100
82
52
28
Dengue Cases 4751 7454 6686 11347 13913 12973 11625 8489 6378 4897 4186 3391 5267
0 0 Dengue Deaths 4 13 9 8 14 28 28 24 21 17 21 12 38
CFR 0.08 0.17 0.13 0.07 0.10 0.22 0.24 0.28 0.33 0.35 0.50 0.35 0.72
Cases Deaths
Source: Disease Control Division, MOH Source: Disease Control Division, MOH
Figure 2: Incidence Rate and Case Fatality Rate of All Reported Figure 4: Dengue Serotype Year 2013, 2014, 2015 and 2016
Dengue Cases in Malaysia, 2000-2016
450 0.7
0.62 396
400 361 0.6
350 328
0.5
Case Fatality Rate
300
250 0.4
Incidence Rate
0.31 0.3 0.3 160
180 178 0.28
200
0.27
145 147 146 0.23 0.3
134 0.23
133 0.2 0.2
150 0.18 0.16
0.23 0.29 0.2
100 69
152 0.24
32 126 0.21 0.21 0.1
50
67 76
0 0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
IR CFR
Source: Disease Control Division, MOH Source: Disease Control Division, MOH
8 ASEAN e-Health Bulletin
since its inception in 2009 and is Table 1: Samples Sequenced and and streamlining virus typing (serotype/
coordinated and monitored by the Analyzed for E Gene Using the Same genotype) protocols. However, the level
National Public Health Laboratory Laboratory Protocols by UNITEDengue of technical capacity and competency
(NPHL). The objectives of DVSS are No. of No. of Serotype composition No. of
among PHL varies. Noticeably we are
to monitor the circulating dengue Year
Cases cases cases also lacking in technical expertise in
tested serotyped DENV1 DENV2 DENV3 DENV4 genotyped
serotypes / genotypes, associate the for PCR bioinformatics as well as the capacity to
findings with clinical diagnosis, detecting 2015 6,258 5,101 2,741 1,631 643 86 595 analyse data to predict outbreaks.
impending outbreak and if possible to 2016 6,612 5,572 2,255 1,402 1,767 148 1,153
predict epidemics. It started with five Total 12,870 10,673 4,996 3,033 2,410 234 1,748 Even with the positive progress shown,
sentinel sites and by the year 2012 the © Ministry of Health, Malaysia a limited public health funding is still
virus surveillance system has expanded the biggest challenge to sustain the
There are many ongoing efforts in virus local DVSS to conduct virus typing/
to all 14 states with a total of 48 sentinel
characterisation since 2012. With the characterization on a routine basis
sites. Samples are collected on a weekly
help from Canada Global Partnership especially after the ASEAN-GPP fund
basis and sent to NPHL and four other
Programme (GPP) support funding in ends in September 2017. Other than
regional Public Health Laboratories
April 2015, laboratory capabilities in that, extra cost will incur to provide EQA
(PHL) for testing.
virus characterization were enhanced materials to regional PHL to strengthen
The circulating virus is being monitored specifically in sequencing and their competency.
via a web-based system as a common phylogenetic analysis of viral genes
regional database. This database to determine their genotypes. The Technology has advanced rapidly and
includes information on serotypes genotyping works have progressed well molecular method has been the major
and genotypes of the virus. In order in the past two years with increased role player to date due to limitations
to generate comparable data across number of samples sequenced by 93.7%, in serological diagnostic method.
the country, NPHL has developed a which were 595 and 1,153 samples in Serological method has been used as
standard protocol for serotyping and 2015 and 2016 respectively. Genotype a common test in detection of dengue
genotyping for all PHL. Apart from that, surveillance revealed that there were infection worldwide. However, Malaysia
intensive technical training together with 3 main strains – DENV-1 genotype Ic, being a dengue endemic country implies
consultations are provided to enhance DENV-2 Clade Ib and DENV-3 genotype a disadvantage in utilizing this method
the laboratory capability in respective I that were responsible for the dengue for other flaviviruses (e.g. Zika) in terms
PHL. Equipments, reagents and transmission in those years. of cross reactivity.
materials such as positive control and Despite close monitoring by NPHL,
UNITEDengue is an excellent
primers are also supplied to sustain the few sentinel sites have not been
platform which offers opportunities to
surveillance system. sending samples on weekly basis.
all AMS especially in strengthening
laboratory capacities. Malaysia was Therefore, sentinel site need to be
Achievements of DVSS honoured by ASEAN GPP Project to reviewed from time to time according
facilitate the technical training during to their performance. This is to ensure
Based on DVSS data in 2015 and
workshop in Lao PDR in March 2016. that the data collected are regionally
2016, a total of 12,870 sera were tested
It was a great opportunity to share our representative and will contribute
with RT-PCR to determine the DENV
knowledge and skill with all ten AMS. to future improvements in the
serotypes and 10,673 were positive
During the emergence of Zika virus, epidemiological knowledge in Malaysia.
(82.9%). Of them, 1,748 samples were
successfully sequenced and analyzed a teleconference was conducted and
for E gene using the same laboratory we have shared our information and The Way Forward
protocols by UNITEDengue (Table 1). experience to all AMS especially on
the technical aspect. Besides that, the In December 2016, Malaysia has
In sequence to achieve UNITEDengue’s considered Zika as a new starting point
aim, our data which comprises of cases meetings conducted in end of 2016
was a pathway in sharing the current to expand and enhance the existing
and virus information is deposited into DVSS beyond dengue with Flavivirus
the UNITEDengue web-portal on a protocols and testing algorithm for
dengue as well as the newly established surveillance. Funds are needed to
monthly basis. Aggregated data will be support this nationwide surveillance
manipulated to determine the disease flavivirus surveillance.
acitivity. A series of training that are
trend and dominant virus strain to be needed have been identified, namely
shared with fellow ASEAN Member Progress and Challenges
in bioinformatics and data analysis to
States (AMS) for further understanding predict an outbreak in a timely manner.
All regional PHL have been on the
of dengue transmission and mutual Besides that, in order to build and access
positive track by showcasing a
warning of impending outbreaks in the the competency, NPHL will provide EQA
significant progress in terms of setting
region. materials on dengue-like illness (e.g
up their sentinel surveillance system
dengue, chikungunya and zika) to all
PHLs.
ASEAN e-Health Bulletin 9
D engue Control Figure 1: Dengue Case Mapping
Programme in
Myanmar: Challenges
and Way Forward
The population of Myanmar is
51,486,253 according to Census 2014.
There are 1 Nay Pyi Taw Union Territory
and 14 States and Regions. In these 15
sub-national areas, there are also 330
townships which are key functional units
to deliver both public health and medical © Ministry of Health & Sports, Myanmar
care services.
noticed in the country. Also, mixed Myanmar. The most important challenge
Dengue is classified as notifiable serotypes are found. This is important is limited engagement of the communities
disease since 1964 in Myanmar. In in clinical and public health because in both urban and rural settings. There
1970, first dengue outbreak occurred secondary infection with another are geographically hard to reach areas
in Yangon. It resulted in 1,654 cases serotype or multiple infections with such as remote villages and politically
and 91 deaths. Then, it spread to other different serotypes lead to severe forms hard to reach areas such as non-
States and Regions (Figure 1). In 2015, of dengue such as dengue hemorrhagic governmental control areas. In addition,
all States and Regions have reported fever and dengue shock syndrome. the hard-to-reach areas do not
dengue cases. The highest number of necessarily mean for remote villages
cases (42,913) was reported in 2015 Obviously dengue endemicity has only, but it also means those areas which
and highest number of death (444) was increased year by year up from 1970 to are tightly locked urban sky-rocketing
reported in 1994. In 2016, the dengue 2015 (1,654 in 1970 to 42,913 in 2015). buildings. Currently, the dengue
cases and deaths were 10,770 and Fortunately, CFR dramatically decreased surveillance only captures Dengue
58, respectively. The dengue cases from 5.50% in 1970 to 0.33% in 2015. Hemorrhagic Fever (DHF) admitted in
and deaths declined by 75% and 59%, the hospitals. Actual number of Dengue
respectively in 2016 compared to 2015. Just like the other dengue prevention
cases is undermined as the programme
In 2017 (January to 4 April 2017) there and control programmes of ASEAN
does not capture the majority of
are 663 cases and 2 deaths. Member States, there are significant
outpatient cases.
challenges to actualize dengue
Generally, dengue cases increase prevention and control activities in
Next Page
during rainy season and are usually
at the highest peak in July (week 27- Figure 2: Top: Seasonal Outbreak of Dengue;
29) (Figure 2, top). Previously, there Bottom: Age Distribution of Dengue Cases
were no reported cases before March
and after September, but nowadays
dengue case is recorded throughout the
year. Children under 15 years old are
mostly affected from dengue, especially
those in 5-9 years age group (figure
2, bottom). Infants under six months
were also affected. Adult dengue cases
were reported from public and private
hospitals, but it is noted that adult
dengue cases are under-reported. Both
males and females are equally affected
from dengue.
Aedes (Stegomyia) aegypti (Ae. aegypti)
and Aedes (Stegomyia) albopictus (Ae.
albopictus) are the two most important
vectors of dengue. Aedes albopictus has
been recognized as a secondary vector
that is also important for the maintenance
of the viruses. In Myanmar, all four
serotypes of dengue virus in circulating
and the serotypes changes are being
© Ministry of Health & Sports, Myanmar
10 ASEAN e-Health BulletinFigure 3: Trends of Dengue Cases and CFR in Myanmar (1970-2015) deterioration of its equipment and loss of
technical expertise.
Recognizing these gaps, a 5-year plan
was proposed to the Dengue control
program mainly to: 1) To increase
the capacity of the NRL to be able to
respond to the needs of the country; 2)
To establish a network of sub-national
laboratories in order to decentralize
testing; 3) To standardize and improve
the quality of case detection and
diagnosis through training on clinical
© Ministry of Health & Sports, Myanmar management and laboratory detection.
As a developing country, Myanmar in comparison to 2015 baseline Activities
encounters widespread water storage (42,913 cases in 2015);
practices and poor waste disposal (2). To reduce dengue mortality by at 1. Laboratory capacity building
management. These situations lead to least 50% by 2020 and 90% by 2025
effective vector breeding. Now, Ministry In 2012, the World Health
in comparison to 2015 baseline (140
of Health and Sports has developed Organization (WHO) provided
deaths in 2015) and
new communicable disease law and by- grants to the NRL to be trained by
(3). To maintain Case Fatality Rate world renowned leader in arbovirus
laws which is yet to be submitted to the
(CFR)Figure 1: Incidence of Reported Dengue Cases, 2012-2016 2.2. Increased capacity for
40,000
Suspect Probable Confirmed virologic detection through
35,000 UNITEDengue
30,000
In 2014, through the invitation of
No. of Cases
25,000
20,000 the National Environmental Agency
15,000
(NEA) in Singapore, the Philippines
10,000
5,000 became part of the UNITEDengue.
0 This is data sharing platform that
Jan
Mar
Apr
May
Jun
Jul
Aug
Sep
Jan
Mar
Apr
May
Jun
Jul
Aug
Sep
Jan
Mar
Apr
May
Jun
Jul
Aug
Sep
Jan
Mar
Apr
May
Jun
Jul
Aug
Sep
Jan
Mar
Apr
May
Jun
Jul
Aug
Sep
Feb
Feb
Feb
Feb
Feb
Oct
Dec
Nov
Dec
Oct
Oct
Oct
Oct
Nov
Dec
Nov
Dec
Nov
Dec
Nov
2012 2013 2014 2015 2016
allows free flowing information
Note: Data from the Epidemiology Bureau, Philippine Integrated © Department of Health, Philippines among member countries, usually
Disease Surveillance and Response (PIDSR)
ASEAN Member States (AMS) on
epidemiological data and viral strains.
Figure 2: Incidence of Dengue by Serotype, 2014-2017
Through this platform, Dengue virus
250
serotyping assay was improved and
the genotyping procedures were
200 established using the reagents and
protocols provided.
150
For 2015, Dengue 1 genotype
II (D1 GII) was circulating while
100
Cosmopolitan genotype for Dengue
2, Dengue 3 was genotype I and
50 Dengue 4 genotype II. This is same
with 2016 virus strains with the
0 addition of Dengue 1 genotype I
Jan-14
Jan-15
Jan-16
Jan-17
Des-16
Mar-14
Apr-14
Okt-14
Des-14
Nov-14
Mar-15
Apr-15
Okt-15
Des-15
Nov-15
Okt-16
Nov-16
Mar-17
Agu-14
Agu-15
Mar-16
Apr-16
Mei-14
Mei-15
Jul-14
Jul-15
Mei-16
Agu-16
Feb-14
Jul-16
Jun-14
Sep-14
Feb-15
Jun-15
Sep-15
Feb-16
Jun-16
Sep-16
Feb-17
being detected.
Dengue 1 Dengue 2 Dengue 3 Dengue 4
© Department of Health, Philippines 3. Expansion of Dengue testing to
the Sub-national Laboratory (SNL)
Through a collaboration with Dengue is one of the 26 notifiable
In 2010, as a response to the
the Pediatric Infectious Disease diseases. However, large proportion
Influenza pandemic, the Department
Society of the Philippines of the cases was detected through
of Health established 5 Subnational
(PIDSP), physicians and medical the clinical symptoms and sample
laboratories (SNL) located in major
technologists from the sentinel collection for confirmation was limited
cities in the country to decongest
hospitals attended with the following and unsystematic. Therefore in 2014,
RITM in the testing of samples. To
outcome: increased awareness in a laboratory-based surveillance was
maximize the infrastructure and
the proper clinical management established in 21 sentinel hospitals
capabilities that were built, the NRL
of Dengue following the standard throughout the country. In order
proposed to expand their capacity
Dengue treatment guidelines thus to monitor the Dengue serotypes
to include Dengue testing using
enabling the hospitals to increase trends, the sentinel hospitals collects
real-time polymerase chain reaction
detection rate and decrease mortality 5 samples from suspect Dengue
(PCR). Likewise, additional two (2)
rates for patients with Dengue cases per week and sends them to
SNLs were added to the network:
infection; increased knowledge in the the NRL for testing using real-time
the Bicol Public Health Laboratory
laboratory diagnosis of Dengue in the PCR methods. Feedback on the
(BPHL) in Legaspi (Region 5) and
performance of different diagnostic serotypes is then provided to EB for
Western Visayas Medical Center
methods available, maintaining analysis after a week.
(WVMC) in Iloilo (Region 6).
quality assurance, interpretation, From 2008 to 2011, Dengue
and selection of testing methods serotype 3 remained to be the
appropriate for the different phases Way Forward
predominant serotype, followed
of the infection. by the predominance of Dengue The Philippines is at its strategic position
serotype 1 starting 2011 to 2013. as it implements the school based
2. Improving evidence-based
From 2014, Dengue 2 emerged Dengue vaccination program and at
decision making
as the most common while both the same time faces the threat of a Zika
2.1. Establishment of a Laboratory- Dengue 1 and 2 were common in outbreak. With the full support from the
based Surveillance 2015. In 2016, a serotype switch was Department of Health, the laboratory
observed around August, leading to capacity has increased and is now ready
In 2008, the Epidemiology Bureau
the predominance of Dengue 3 in to respond to the needs of the country.
(EB) launched the Philippine
succeeding months until early 2017 Nevertheless, use of new and emerging
Integrated Disease Surveillance
(Figure 2 and Figure 3). technologies should still be pursued to
and Response (PIDSR), which
Next Page
12 ASEAN e-Health BulletinL aboratory-based Dengue
Figure 3: Distribution of Dengue Serotypes confirmed by using either NS1 antigen or
in the Philippines, 2008-2016 polymerase chain reaction (PCR) assays.
Surveillance Programme Virus surveillance, on the other hand,
in Singapore: Situation monitors the serotype and genotype
of circulating virus strains by PCR
Update, Challenges and and genome sequencing on a weekly
Future Priorities basis [3]. The overall aim is to provide
timely updates on the composition and
Introduction to laboratory-based distribution of Dengue virus (DENV) to
surveillance programme detect any emergence and replacement
Dengue has been endemic in Singapore of predominant serotype/genotype.
since the first recorded outbreak in 1901. Replacement of predominant serotype
Dengue became a legally notifiable has been associated with outbreaks in
disease in 1966, subsequent to the first the last 12 years [4].
outbreak of dengue haemorrhagic fever
(DHF) in 1960 [1]. The nationwide Aedes Current update
prevention and control programme was
In 2016, there were 13,091 dengue fever
launched in 1969. The programme,
(DF), 24 DHF cases and nine (9) fatalities
which was fully implemented in 1973,
(0.07% mortality). In comparison, 11,282
was strategized on the source reduction,
DF, 12 DHF cases and five (5) fatalities
health education and law enforcement.
(0.04% mortality) were reported in 2015.
Subsequent programme reviews led to
© Department of Health, Philippines Of them, serotypes were confirmed in
an enhanced approach that included
6,094 (46.6%) cases and genotypes
Figure 4: Capacity Building Activities of the current integrated surveillance
in 2,841 (21.7%) infections. All four
the NRL framework supported by four main
serotypes circulated in the country,
pillars; 1) enhanced case surveillance
indicating hyper endemic transmission.
that improved operational response; 2)
DENV-2 was the most dominant
virus surveillance for early warning of
serotype (51%), followed by DENV-
outbreaks; 3) entomological surveillance
1 (27%), DENV-3 (19%) and DENV-4
for understanding the distribution of
(3%). The genotype analysis revealed
vectors and their density in time and
consistently high overall virus diversity.
space; 4) environmental parameters for
However, DENV-2 population was highly
understanding the relationship between
homogenous, with 93% of 1,495 DENV-
these parameters and outbreak risk by
2 viruses genotyped belonging to a
statistical modelling [2].
© Department of Health, Philippines genetically similar group of cosmopolitan
The case surveillance relies on an island genotype. In comparison, DENV-1
further improve pathogen detection and wide network of general practitioners, population (n=693) consisted of three
data analysis. public and private hospitals and major strains; two belonging to genotype
laboratories that mandatorily notify all I (50%) and a remaining genotype III
While efforts have been made to the
clinically-suspected and laboratory- strain (32%).
laboratory capacity, this is but one piece
of the overall strategy. The only way to confirmed dengue cases and deaths
effectively control dengue is through a to the Ministry of Health within 24
unified effort among the national control hours of detection. Dengue cases are
Next Page
programme, surveillance, virology and
Figure 1: Weekly Dengue Case Trend from 2012 to 2017
entomology experts, and much remains
to be done. The current system needs to
be fully integrated and to evolve to one
that can not only control, but also, predict
and prevent future outbreaks.
Note: Data was gathered through the island wide surveillance © Ministry of Health, Singapore
programme. All cases are laboratory-confirmed.
ASEAN e-Health Bulletin 13R eported Dengue
Challenges and future priorities enables a fast-track, high population
penetration, its effectiveness in the
Even though the control strategies local dengue landscape is yet-to-be Fever (DF)/ Dengue
implemented in 1970’s lead to a sharp determined. Hemorrhagic Fever
reduction in Aedes premises index and
low disease incidence [5], epidemics (DHF) Cases in Thailand
References
have occurred every 5-6 years since
1. Chan YC, Lim KA, Ho BC: Recent epidemics of Introduction
late 1980’s despite a consistently low
haemorrhagic fever in Singapore. Japanese
Aedes house index (below 1%) [6]. journal of medical science & biology 1967, 20 Dengue Fever / Dengue Hemorrhagic Fever
However, dengue serotype prevalence Suppl:81-88. (DF / DHF) case is an endemic disease
among residents has continued to fall in tropical and subtropical countries in Asia,
2. Shi Y, Liu X, Kok SY, Rajarethinam J, Liang
over the decades [7], implying potential S, Yap G, Chong CS, Lee KS, Tan SS, Chin Africa, America and South America. In
success of control efforts. This is CK, et al: Three-Month Real-Time Dengue Thailand, the dengue cases have been
supported by the declining estimates Forecast Models: An Early Warning System widespread transmitted across the country
of force of infection (per capita rate of for Outbreak Alerts and Policy Decision reported by Bureau of Epidemiology,
acquiring infection) since the 1960s [8]. Support in Singapore. Environmental health Department of Disease Control, Ministry
These observations suggest that the perspectives 2015. of Public Health (Fig.1). In 2016, a total
apparent increase in case burden could 3. Hapuarachchi HC, Koo C, Rajarethinam of 63,310 cases were reported in 77
be attributable to improved diagnostic J, Chong CS, Lin C, Yap G, Liu L, Lai YL, Ooi provinces and morbidity rate was 96.76 /
and notification rates over the years. PL, Cutter J, Ng LC: Epidemic resurgence of
100,000 population. There were 61 death
Nevertheless, the widening susceptible dengue fever in Singapore in 2013-2014: A
virological and entomological perspective. cases and the percentage of death was
age range [9], geo-expansion of Aedes 0.10
BMC infectious diseases 2016, 16:300.
aegypti, the primary vector of DENV
4. Lee KS, Lai YL, Lo S, Barkham T, Aw P, Ooi Dengue is now one of the important
in the country and introduction of new
PL, Tai JC, Hibberd M, Johansson P, Khoo SP,
viruses through trade and travel [3, public health problems in Thailand.
Ng LC: Dengue Virus Surveillance for Early
10] will continue to be challenging. Warning, Singapore. Emerg Infect Dis 2010,
There is an outbreak every two years
While mitigating the local factors, the 16. because of the changing of dengue
borderless nature of dengue spread serotype predominant. This may produce
5. Goh KT, Yamazaki S: Serological survey
emphasizes the importance of cross- on dengue virus infection in Singapore. epidemics and severe dengue diseases
border surveillance and capacity building Transactions of the Royal Society of Tropical (Fig.2). The recirculation pattern seems
through projects involving regional Medicine and Hygiene 1987, 81:687-689. to be predictable for dengue outbreaks.
stakeholders (ASEAN Member States) 6. Goh KT: Changing epidemiology of dengue
and collaborators (ASEAN Secretariat in Singapore. Lancet 1995, 346:1098. Thailand has just participated in the project
and Global Partnership Programme, 7. Low SL, Lam S, Wong WY, Teo D, Ng LC, Tan of ASEAN-Canada’s Global Partnership
Canada) that ride on platforms such LK: Dengue Seroprevalence of Healthy Program (GPP) UniteDengue (year 2014-
as UNITEDengue (UNited in Tackling Adults in Singapore: Serosurvey Among 2016) in March 2016 led by Malaysia
Epidemic Dengue). On the other hand, Blood Donors, 2009. Am J Trop Med Hyg
these challenges also indicate the need 2015, 93:40-45. Figure 1: The Morbidity Rate of DF / DHF
for novel approaches to support the 8. Ng LC, Tan HK, Tan LK, Chong CS, Ho D: Cases in Thailand from 2016
conventional control strategies. Evolving dengue control programme in
Singapore. Epedemiological News Bulletin
The release of Ae. aegypti carrying 2016, 42:11-15.
1
Wolbachia bacterial strains is a novel 9. Low SL, Lam S, Wong WY, Teo D, Ng LC,
technology used either to replace or Tan LK: Dengue seroprevalence of healthy
to suppress the indigenous vector adults in Singapore: serosurvey among
populations. Project Wolbachia– blood donors, 2009. The American journal of
Singapore is evaluating the use of male tropical medicine and hygiene 2015, 93:40-
45.
Wolbachia-Aedes mosquitoes to further 2
suppress Ae. aegypti mosquitoes in 10. Lee KS, Lo S, Tan SS, Chua R, Tan LK, Xu H, Ng
the local community. A small-scale field LC: Dengue virus surveillance in Singapore
reveals high viral diversity through multiple
study was launched in October 2016,
introductions and in situ evolution. Infect
involving releases of Wolbachia-carrying Genet Evol 2011, 12:77-85.
male Ae. aegypti mosquitoes to test
various parameters and pave the way
for further trials that would be necessary 3
before actual field deployment of this
new technology. Singapore has already
licensed the tetravalent vaccine for
DENV (Dengvaxia®). Even though a © Ministry of Public Health, Thailand
vaccine is an ideal preventive tool that
Next Page
14 ASEAN e-Health BulletinFigure 2: DF/DHF Reported Cases and Circulation of the NIH website and DMSc website for
Dengue Serotypes in Thailand between 2006 - 2016 more information to the community.
Table 1: Circulation of Dengue Serotypes in
3 Sentinel Sites of Thailand in 2016
Province Month D1 D2 D3 D4
Lampang Feb 1
(1 in Fig.1) Mar 1
Apr 2
May 1 2
Jun 1
Jul 7 3 2
Aug 13 1 3
Sep 4
Oct 1 1
© Ministry of Public Health, Thailand
Nov 1 1
and Singapore. The three sentinel sites Genotyping: The positive samples Dec 1
have been established for surveillance of from both virus isolation and RT-PCR Total 2 27 6 11
dengue serotypes in Lampang province testing were then being genotyped. Ratchaburi Jan 1 1 2 2
(Northern region), Ratchaburi province Complementary DNA was amplified (2 in Fig.1) Feb 1
(Central region) and Phuket province from extracted dengue RNA for PCR Apr 1 1
(Southern region) (Fig.1). The specimens products of E gene at the Arbovirus Jul 1
have been collected from suspected laboratory, Thailand. The PCR products Sep 1 1
patients who have been diagnosed with were further sent to the ASEAN-GPP Nov 1 1 1
dengue infection by clinician hospital. The project in UNITEDengue web-portal in Total 5 2 4 4
container of patient specimens were then Singapore for performing sequencing Phuket Feb 1 2
stored in liquid nitrogen tank and sent to and analysis. (3 in Fig.1) May 1 1
Arbovirus section, National Institute of Jul 4 1
Health, Department of Medical Sciences, Results: There are 30 cases qualified Aug 6 3
Thailand by public transportation. specimens that is out of 99 dengue virus Sep 1 2 2
positive (VI&RT-PCR) specimens for Oct 1 2
sequencing in this project and their virus Nov 3 1
Process of Diagnosis
data from the three sentinel sites that are Dec 1 6
Virus isolation and identification: the shown in the Table 1. The sequencing Total 3 25 2 8
patients’ specimens collected at the acute analysis has shown (data not shown) © Ministry of Public Health, Thailand
stage were inoculated into mosquito the dengue 4 serotypes being common Table 2: Genotypes of Dengue Serotype 2
cell line (C6/36 cells) in a 24-well plate in Asia. The predominant genotype in Sentinel Sites of Thailand, 2016
and rocked for 90 minutes. The culture of DENV1 is Genotype I (GI), DENV3 Public ID Genotype Serotype
Location
Month/2016
as genotype III (GIII) and DENV4 as
Regional Province
media (L-15; Gibco-BRL, NY, USA) 1|THA|D2AsianI
2|THA|D2AsianI
Asian I
Asian I
DENV2
DENV2
Northern Lampang
Northern Lampang
Aug
Aug
containing 1% heat-inactivated fetal genotype I (GI). Those genotypes were 3|THA|D2CosmoIb_13
4|THA|D2CosmoIb_13
Cosmopolitan clade1b
Cosmopolitan clade1b
DENV2
DENV2
Sounthern
Sounthern
Phuket
Phuket
Sep
Sep
bovine serum was subsequently added. circulated in three regions. For DENV2, 8|THA|D2CosmoIb_13
9|THA|D2CosmoIb_13
Cosmopolitan clade1b
Cosmopolitan clade1b
DENV2
DENV2
Sounthern
Sounthern
Phuket
Phuket
Jul
Aug
After the 7-day incubation at 28 °C, the it is separated to two genotypes which 10|THA|D2AsianI
11|THA|D2AsianI
Asian I
Asian I
DENV2
DENV2
Northern Lampang
Northern Lampang
Jun
Aug
infected fluid was collected for further the first one is genotype Asian I that is 21|THA|D2AsianI
22|THA|D2AsianI
Asian I
Asian I
DENV2
DENV2
Central Ratchaburi
Central Ratchaburi
Jan
Jan
dengue PCR products genotyping. The circulated in the north and central region 23|THA|D2CosmoIb_13
24|THA|D2CosmoIb_13
Cosmopolitan clade1b
Cosmopolitan clade1b
DENV2
DENV2
Sounthern
Sounthern
Phuket
Phuket
May
Feb
of Thailand. The second was genotype
25|THA|D2AsianI Asian I DENV2 Northern Lampang Jul
remaining infected cells were detected 26|THA|D2AsianI
27|THA|D2AsianI
Asian I
Asian I
DENV2
DENV2
Northern Lampang
Northern Lampang
Aug
Sep
for dengue serotypes identification by cosmopolitan clade1b circulated in the © Ministry of Public Health, Thailand
immunofluorescence assay (IFA). southern region (Table 2).
Acknowledgments
Molecular detection: Reverse Summary • National Institute of Health, DMSc,
transcription-polymerase chain reaction Thailand
(RT-PCR)/real time RT-PCR was The number of reported dengue cases in • Bureau of Epidemiology, Department
finally used for confirmation of negative Thailand in 2016 are 63,310 cases. The of Disease, Thailand
specimens from virus isolation and cumulative number of cases compared • ASEAN Canada’s GPP Project
identification. Extraction of viral RNA was to the morbidity rate in the year 2015
then performed with their acute plasma/ is less than 2.3-folds (142,925 cases)
serum specimens using QIAamp viral shown on the website of the Bureau of
RNA mini kit (Qiagen, Hilden, Germany). Epidemiology, Department of Disease
RT-PCR was done by using the one- Control. All the laboratory results of
step RT-PCR kit with dengue-specific dengue serotypes circulated in every
oligonucleotide primer while Real time region of Thailand has been posted on
RT-PCR was using commercial kit.
ASEAN e-Health Bulletin 15You can also read