Sustained release metformin where standard metformin is not tolerated
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Sustained release
metformin where
standard metformin is
not tolerated
Julie Brake
Article points
Research has found that few people will put up with unwanted side
1. Few people will continue
taking medication while effects from a prescribed medication for more than a month (ICM
experiencing side effects. Research, 2004). The most common side effects of metformin
2. Hypoglycaemia does tablets are gastrointestinal (GI) and although the literature states
not usually occur with that these can easily be managed in most people by cautious dose
metformin when used as titration, administration after meals or dose reduction, many
monotherapy.
people with diabetes discontinue taking the drug. Sustained release
3. In the UKPDS metformin (Glucophage SR, Merck, West Drayton) is a slow release
metformin reduced
macrovascular
formulation that promises fewer GI side effects and allows once-
complications and daily dosing, both of which should provide better concordance
mortality in type 2 (Davidson and Howlett, 2004). This article looks at whether people
diabetes.
with type 2 diabetes who could not tolerate standard metformin
4. The DARTS study followed advice on administration and titration and if they could
showed that simple
regimens lead to
tolerate sustained release metformin. The effect this had on HbA1c,
significantly better weight and insulin or oral hypoglycaemic agents was also examined.
adherence.
M
5. If medication is not etformin is the only drug Association and Royal Pharmaceutical
tolerated we must not
available in the biguanide class. Society of Great Britain, 2006).
assume that the patient is
doing something wrong. Its positive effects are mainly Hypoglycaemia does not usually occur
caused by decreasing gluconeogenesis and with metformin when used as monotherapy,
Key words
increasing the peripheral utilisation of but can occur if used in conjunction with
- Type 2 diabetes glucose. Metformin is the first choice drug other oral hypoglycaemic agents (OHAs) or
- Sustained release in overweight people (BMI >25 kg/m 2) in insulin. Metformin is associated with lactic
metformin
whom strict lifestyle intervention has failed acidosis but is most likely to occur in people
- Once-daily dosing
to control their diabetes (NICE, 2002). with renal impairment and thus should
It is the drug of first choice in overweight not be used even in mild renal impairment
patients and is also used when diabetes is (British Medical Association and Royal
Julie Brake is a DSN at
the Royal Liverpool and inadequately controlled with sulphonylureas Pharmaceutical Society of Great Britain,
Broadgreen University (SU) and now with increased frequency in 2006).
Hospitals NHS Trust. combination with insulin (British Medical In addition to its glucose lowering effects,
32 Journal of Diabetes Nursing Vol 11 No 1 2007Sustained release metformin where standard metformin is not tolerated
metformin appears to have beneficial the period immediately after the initiation Page points
effects on other cardiovascvular risk factors of treatment and tends to diminish over 1. Metformin was shown
including dyslipidaemia, plasminogen time (Garber et al, 1997). Generally, GI side to reduce macrovascular
activator inhibitor-1 levels, monocyte effects can be easily managed in most people complications and
adhesion to endothelial cells, insulin by cautious dose titration, administration mortality in people with
type 2 diabetes.
resitance and hyperinsulinaemia (Cusi after meals or by reducing the total daily
and Defronzo, 1998; Nagi and Yudkin, dosage (Fujioka et al, 2005). 2. A low percentage of
1993; Uehara et al, 2001; Mamputu et Blonde et al (2004) retrospectively people will put up with
the long-term GI side
al, 2003). The UK Prospective Diabetes reviewed patient records to compare the
effects of immediate
Study (UKPDS) has also demonstrated frequency of adverse GI events in groups release (IR) metformin.
that metformin reduced macrovascular taking either IR metformin (n=158) or
3. Sustained release (SR)
complications and mortality in people with sustained release (SR) metformin (n=310).
metformin promises
type 2 diabetes (UKPDS, 1998). They concluded that the frequency of any fewer gastrointestinal side
GI adverse event during the first year of effects, thus improving
Concordance treatment was not significantly different concordance and diabetes
The Diabetes Audit and Research in Tayside between the two groups (11.94 % versus control.
Scotland (DARTS) study showed that only 11.39 %; P=not significant). 4. This study of 22 people
one-third of people with diabetes who are The SR metformin formulation promises aimed to investigate
prescribed one type of tablet collected their fewer GI side effects (Davidson and whether people unable
to tolerate IR metformin
medication as recommended (Donnan et Howlett, 2004), thereby providing better
had been taking their
al, 2002). People on combination therapy concordance and improved diabetes control medication appropriates,
with two types of tablets found it even as well as the potential cardiovascular whether they could
harder, with only one-tenth collecting risk reducing effects of metformin. Data tolerate SR metformin,
their prescriptions as recommended. The from previous studies confirms that and the effects SR
metformin had on their:
findings also reveal potential solutions, the antihyperglycaemic efficacy of SR
HbA1c, weight and
with those on simple regimens such as once- metformin is comparable to that of IR insulin or SU dose.
daily treatment showing significantly better metformin given in divided doses (Fujioka
adherence. et al, 2003; Fujioka et al, 2005). This work
Consumer research into attitudes towards also demonstrated that SR metformin
long-term medication for conditions such exerted little effect on body weight, with
as type 2 diabetes found that 11 % would mean changes in body weight being small
put up with unwanted side effects from a (reductions of up to 1 kg).
prescribed medication for a month and only
2 % would tolerate them for three months. Methods
Headaches were cited as the side effect with The aim of this study was to investigate
the most negative impact on life, closely whether people unable to tolerate IR
followed by diarrhoea and then nausea metformin:
(ICM Research, 2004). l had been taking IR metformin
It is well known that the principal side appropriately
effects of standard immediate release (IR) l could tolerate SR metformin
metformin tablets are gastrointestinal (GI) in l the effect SR metformin had on their:
nature (Howlett and Bailey, 1999). A double − HbA1c
blind, parallel group dose–response trial in − weight
a total of 451 people with type 2 diabetes − insulin or SU dose.
showed that the incidence of GI side effects Twenty-two participants were recruited
was approximately 20–30 % in participants through the general diabetes clinic within
randomised to receive IR metformin a large teaching hospital in Liverpool.
500–2500 mg/day. The incidence of such Any person not on metformin without
side effects with IR metformin is highest in contraindications were asked whether they
Journal of Diabetes Nursing Vol 11 No 1 2007 33Sustained release metformin where standard metformin is not tolerated
Page points had previously been taking IR metformin. Results
1. All participants were Any person who had previously been taking All patients, when questioned, had been
found to have been IR metformin and had stopped due to side prescribed and were taking metformin
taking IR metformin effects were questioned on the following according to the British National Formulary
according to guideline points: guidance when intolerance occurred. This
recommendations when
l initial dosage (in comparison to was to start on 500 mg with breakfast for
intolerance occurred.
administration advice by the at least one week, increasing to 500 mgs
2. Mean HbA1c was British Medical Association and Royal at breakfast and evening meal for at least
significantly lower after
Pharmaceutical Society of Great Britain, another week, then 500 mgs at breakfast,
12 weeks in the twelve
participants (55 %) who 2006) lunch and evening meal increasing as
could tolerate 1–1.5 g of l speed of titration (in comparison to tolerated to 2–3 g daily in divided doses
SR metformin. administration advice by the (British Medical Association and Royal
3. There was a significant British Medical Association and Royal Pharmaceutical Society of Great Britain,
weight gain observed, Pharmaceutical Society of Great Britain, 2006).
on average 1 kg per 2006) Thirteen participants (59 %) could not
participant. l when the metformin was taken tolerate any IR metformin, and nine (41 %)
(i.e. pre-meal, with meal or post-meal) could tolerate 1 g of IR metformin.
l maximum tolerated dose Upon completion 10 participants (45 %)
l side effects (if any). could tolerate 2 g of SR metformin and
If the person with diabetes was 12 (55 %) could tolerate 1–1.5 g of SR
administering IR metformin correctly and metformin.
had to stop due to side effects at a dose of 2 g Mean HbA1c was 9.0 % at commencement
or less they were prescribed SR metformin of SR metformin and was significantly
and included in the study. There were no lower at 12 weeks: 8.3 % (P=0.008).
other exclusion criteria and individuals on A significant reduction in mean insulin dose
any anti-diabetic medication, be it insulin was also noted, from 65 to 59 units per day
or other OHAs, were included. (P=0.041). There was a significant increase
Biomedical variables were measured in mean weight from 90.8 kg to 91.8 kg
on the individuals’ usual diabetes clinic (P=0.041). On comparison of insulin or
attendances and nurse-led follow-up clinics. OHA dose and HbA1c , 10 participants
(45 %) were able to reduce their doses
Measures without increasing their HbA1c (Table 1).
All measures were obtained in the clinic Increased weight was recorded in
environment on commencement of SR 10 people (45 %) who commenced on
metformin and at 12 weeks. The following SR metformin. Four (18 %) lost weight,
variables were measured: 8 (36 %) maintained weight. Comparisons
l HbA1c between changes in weight and changes in
l weight OHA or insulin levels are shown in Table 2,
l insulin or OHA dose. and between weight and HbA1c in Table 3.
Tolerance was measured by assessing
side effects. This also determined the dose Discussion
titration as the participants were maintained One may surmise that improvements in
on the highest dose tolerated (up to 2 g) blood glucose levels could potentially lead
without unwanted side effects. to a gain in weight, as glucose is removed
Other information was also noted: from the blood and is stored by the body.
maximum tolerated dose of immediate One may also surmise that improved blood
release metformin, maximum tolerated dose glucose levels accompanied by a reduction
of SR metformin, age, gender and type of in OHA or insulin dose would be associated
diabetes. with weight reduction or maintenance.
34 Journal of Diabetes Nursing Vol 11 No 1 2007Sustained release metformin where standard metformin is not tolerated
In this study there was significant weight
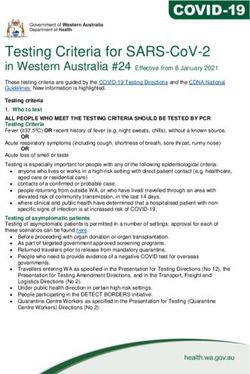
Table 1. Comparison of number of participants with changes in
gain, be it only an average of 1 kg. A weight
HbA1c and with changes in OHA or insulin doses.
gain of 1 kg may not appear to be a great
deal but literature suggests that it may Reduced Maintained Increased
increase cardiovascular risk by 3.1 % and OHA or insulin OHA or insulin OHA or insulin
diabetes risk by 4.5 % to 9 % (Willet et Reduced HbA1c 9 4 3
al, 1995; Ford et al, 1997; Mokdad et al, Maintained HbA1c 1 1 0
2000). The weight gain demonstrated in Increased HbA1c 0 3 1
this study may well have been significantly
greater if the same improvements in HbA1c
had been achieved with an increase in the
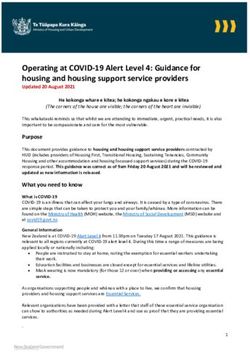
participants’ insulin or OHA doses rather Table 2. Comparison of number of participants with changes in
than with the addition of SR Metformin. weight and with changes in OHA or insulin doses.
On further analysis of weight compared Weight Weight Weight
with OHA or insulin dose all participants reduction maintained increased
who lost weight had a reduction in their
Reduced OHA or insulin 4 2 4
insulin or OHA doses, but an equal
Maintained OHA or insulin 0 5 3
number of people had a reduction in OHA Increased OHA or insulin 0 1 3
or insulin and gained weight. However,
those who lost weight showed the greatest
reduction in insulin or OHA at 12 weeks,
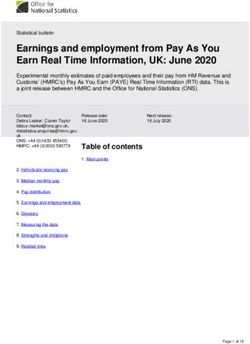
ranging from a 19 % reduction to a 100 % Table 3. Comparison of number of participants with changes in
reduction. The individual who had a 100 % HbA1c.
reduction had been taking an SU and was
Weight Weight Weight
able to cease administering the SU after reduction maintained increased
8 weeks due to hypoglycaemia. While it
is tempting to attribute this change to the Reduced HbA1c 4 3 8
SR metformin, it may also be due to other Maintained HbA1c 0 1 1
Increased HbA1c 0 4 1
variables not examined by this study, for
example changes in diet or activity levels.
In this study, those who could not tolerate
2 g of SR metformin after the evening similar short-term efficacy to IR metformin
meal had their dose split into 1 g twice and are not convinced on its improved Page points
daily. Even on dividing the dose, 55 % GI tolerability and are conscious of the 1. Even on dividing the dose
of participants could not tolerate 2 g per increased cost issues. There have been to 1 g twice daily, 55 %
day, but all patients could tolerate at least several studies looking at GI tolerability, of participants could
1 g of SR metformin per day. This study many of which show improved tolerability not tolerate 2 g per day,
demonstrated that SR metformin was with SR metformin, but the above bodies but all patients could
tolerate at least 1 g of SR
tolerated well by 10 people (45 %) who took argue that these were either retrospective, metformin per day.
the maximum 2 g dose and 12 people (55 %) not powered to detect differences in
tolerated 1–1.5 g, with significant reductions tolerability or that key assumptions were 2. Some professional bodies
do not recommend the
in HbA1c , and insulin or OHA dose. Also made for which the clinical evidence base use of SR metformin, but
demonstrated was a significant weight gain, was not convincing (Scottish Medicines in the author’s experience
of an average 1 kg: but this ranged between Consortium, 2005). people unable to tolerate
weight loss of 1.9 kgs to a gain of 6.3 kgs. In the author’s experience people who were IR metformin have
Some bodies, including the Scottish previously unable to tolerate IR metformin been able to take SR
metformin with improved
Medicines Consortium and a number have been able to take SR metformin with HbA1c and often a
of PCTs, do not recommend the use of improved HbA1c , along with the added reduction in insulin or
SR metformin as they feel that it has cardiovascular benefits of metformin, very OHA dose.
Journal of Diabetes Nursing Vol 11 No 1 2007 35Sustained release metformin where standard metformin is not tolerated
little weight gain, and often a reduction Fujioka K, Pans M, Joyal S (2003) Glycemic control
in patients with type 2 diabetes mellitus switched
in insulin or OHA dose. Local PCTs in from twice-daily immediate-release metformin to
the author’s district support the use of SR a once-daily extended-release formulation. Clinical
metformin if used appropriately along the Therapeutics 25: 515–29
same published guidelines as this study.
Conclusion Garber AJ, Duncan TG, Goodman AM et al (1997)
Efficacy of metformin in type 2 diabetes: results of
Education in relation to timing, a double-blind, placebo-controlled dose-response
administration and dose adjustment of trial. The American Journal of Medicine 103: 491–7
IR metformin is essential. This study has
highlighted the importance of healthcare Howlett HC, Bailey CJ (1999) A risk benefit
assessment of metformin in type 2 diabetes mellitus.
professionals not assuming that the Drug safety: an international journal of medical
person with diabetes is not following toxicology and drug experience 20: 489–503
administration advice if IR metformin is not
tolerated. Changing to SR metformin may Mamputu JC, Wiernsperger N, Reiner G (2003)
Metformin inhibits monocyte adhesion to
well improve tolerability and concordance, endothelial cells and foam cells formation. British
enabling most people to improve their Journal of Diabetes and Vascular Disease 3: 302–10
diabetes control and possibly reduce their
insulin or OHA dose. n Mokdad AH, Ford ES, Bowman BA et al (2000)
Diabetes trends in the US: 1990-1998. Diabetes
Care 23: 1278–83
Blonde L, Dailey GE, Jabbour SA et al (2004)
Gastrointestinal tolerability of extended release ICM Research, May 2004. Consumer research. Merck
metformin tablets compared to immediate release Pharmaceuticals: Data on file
metformin tablets: results of a retrospective cohort
study. Current Medical Research and Opinion 20:
565–72 Nagi DK, Yudkin JS (1993) Effects of metformin
on insulin resistance risk factors for CVD and
British Medical Association and Royal Pharmaceutical plasminogen activator inhibitor in NIDDM
Society of Great Britain (2006) British National subjects. A study of two ethnic groups. Diabetes
Formulary (BNF) 52: September 2006. BMJ Care 16: 653–5
Publishing Group and RPS Publishing, London
National Institute for Health and Clinical Excellence
Cusi K, Defronzo R A (1998) Metformin: a review of (2002) Management of type 2 diabetes - management
its metabolic effects. Diabetes Review 6: 89–131 of blood glucose. Available at: www.nice.org.
uk/36733 (accessed 05.01.07)
Davidson J, Howlett H (2004) New prolonged-release
metformin improves gastrointestinal tolerability.
The Bristish Journal of Diabetes and Vascular Disease Scottish Medicines Consortium (2005) Metformin
4: 273–7 hydrochloride prolonged release 500mg tablets,
Resubmission. No.148/04. NHS Scotland
Donnan PT, MacDonald TM, Morris AD et al
(2002) Adherence to prescribed oral hypoglycaemic
medication in a population of patients with type Uehara MH, Kohlmann NE, Zanella MT, Ferreira
2 diabetes: A retrospective cohort study. Diabetic SR (2001) Metabolic and haemodynamic effects of
Medicine 19: 272–84 metformin in patients with type 2 diabetes mellitus
and hypertension. Diabetes, Obesity & Metabolism 3:
318–25
Ford ES, Williamson DF, Liu S (1997) Weight
change and diabetes incidence: findings from a
national cohort of US adults. American Journal of United Kingdom Prospective Diabetes Study
Epidemiology 146: 214–22 (UKPDS) Group (1998) Effect of intensive blood-
glucose control with metformin on complications in
Fujioka K, Brazg RL, Raz I et al (2005) Efficacy, overweight patients with type 2 diabetes (UKPDS
dose-response relationship and safety of once-daily 34). Lancet 352: 854–65
extended-release metformin (Glucophage XR) in
type 2 diabetic patients with inadequate glycaemic
control despite prior treatment with diet and Willett, WC, Manson, JE, Stampfer, MJ et al
exercise: results from two double-blind, placebo- (1995) Weight, weight change and coronary heart
controlled studies. Diabetes, Obesity and Metabolism disease in women. Journal of the American Medical
7: 28–39 Association 273: 461–5
36 Journal of Diabetes Nursing Vol 11 No 1 2007You can also read