Strategies to support the COVID-19 response in LMICs - A virtual seminar series
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Strategies to support the COVID-19 response in LMICs A virtual seminar series
Therapeutics Landscape for COVID-19 Natasha Mubeen Chida, MD MSPH Associate Program Director, Infectious Disease Fellowship Program Assistant Professor, Division of Infectious Diseases Johns Hopkins University School of Medicine
Objectives • Review biological plausibility of Remdesivir for SARS-CoV-2 treatment • Review clinical data on Remdesivir • Review biological plausibility of Hydroxychloroquine for SARS-CoV-2 treatment • Review clinical data on Hydroxychloroquine • Discuss cytokine release syndrome in COVID-19 • Discuss use of anti IL-6 blockade for management of CRS • State ongoing clinical trials for Remdesivir, hydroxychloroquine, IL-6 blockade
Sample of COVID-19 Therapeutic
Landscape
Antivirals Immune Modulators Other
Baloxavir Anakinra ACEI/ARB
Chloroquine/Hydroxychloroquine Convalescent Plasma Ascorbic Acid
DAS-181 Corticosteroids Azithromycin
Favipiravir IVIG Epoprostenol
Interferon Lenzilumab Indomethacin
Lopinavir/Ritonavir Ruxolitinib Ivermectin
Neuraminidase inhibitors Sarilumab Niclosamide
Remdesivir Sirolimus Nitazoxanide
Ribavarin Tocilizumab Statins
Umifenovir Acalabrutinib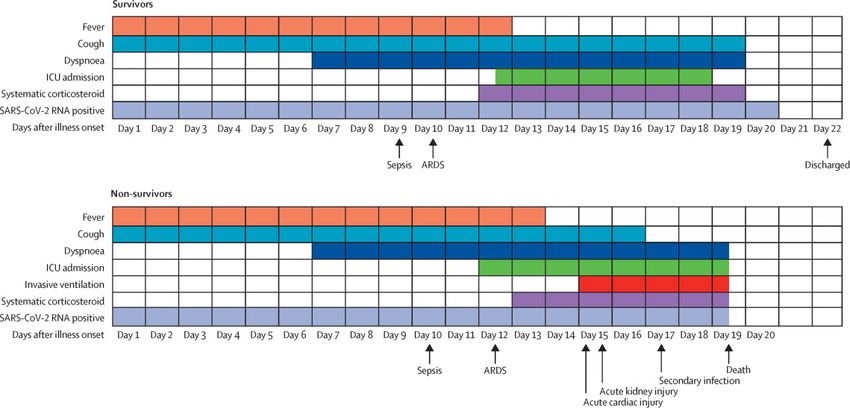
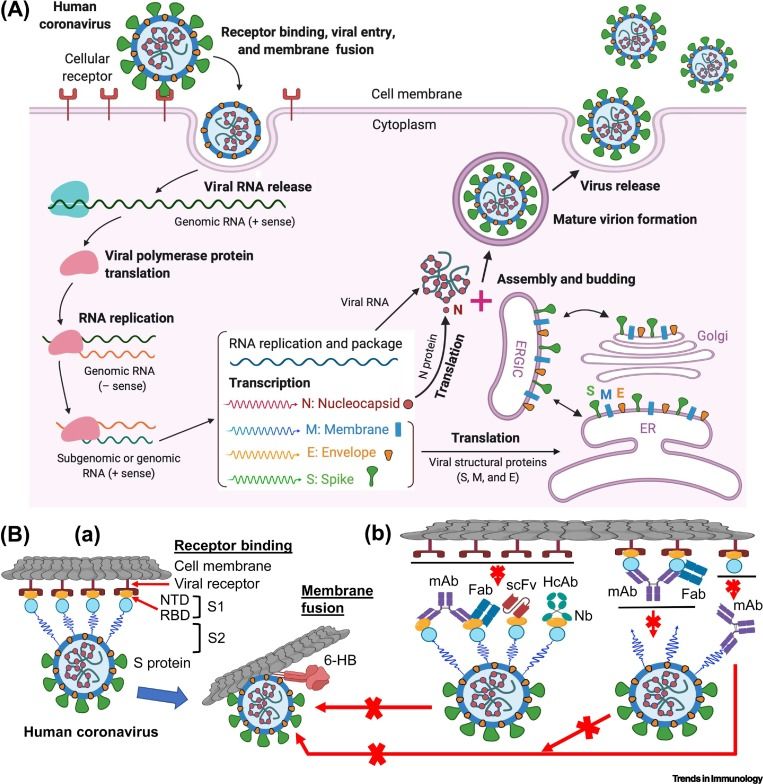
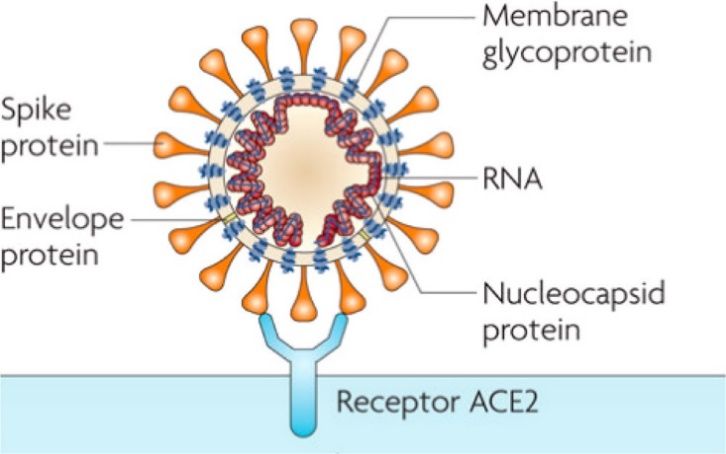
SARS-CoV-2
Liu C, et al. ACS Cent Sci. doi: 10.1021/acscentsci.0c00272 (2020). Jiang S, Hillyer C, Du L. Trends Immunol doi: 10.1016/j.it.2020.03.007 (2020).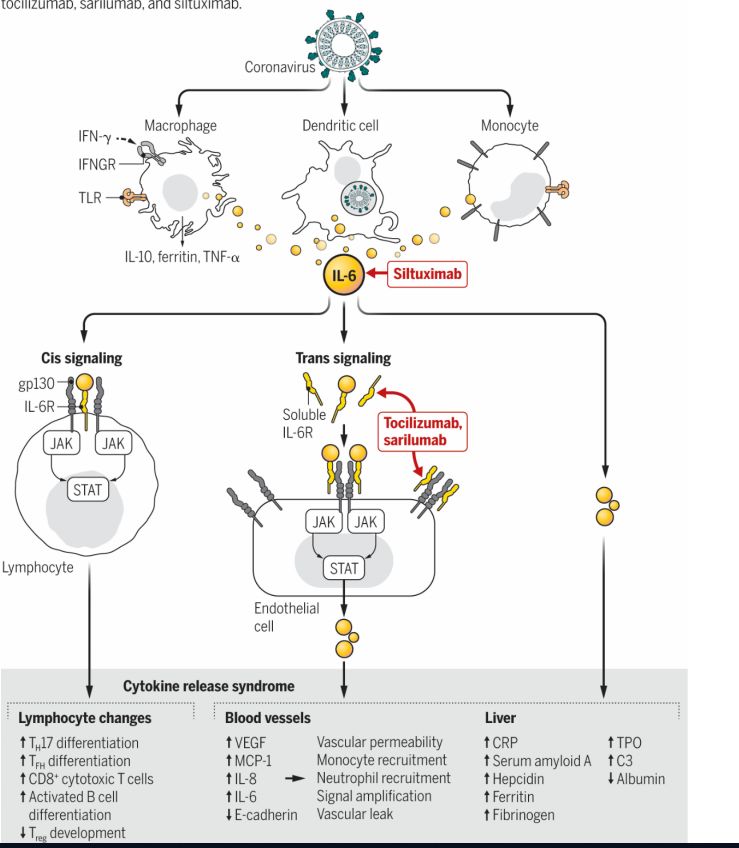
“Antivirals”
Remdesivir
• 2013 Ebola outbreak
• CDC/USAMRIDD/Gilead Sciences identified
nucleoside lead à prodrug, RDV
• Metabolized to active form, adenosine nucleoside
analog
• Interferes with RNA polymerase
• Evades viral exoribonuclease proofreading
• Decrease in RNA production
• In cell/animal models efficacious in MERS-CoV,
Remdesivir
SARS-CoV, Marburg, Nipah, more
• IV formulation
Warren TK, et al. Nature. 2016;531(7594):381-5. Sheahan TP, et al. Sci Transl Med. 2017;9(396).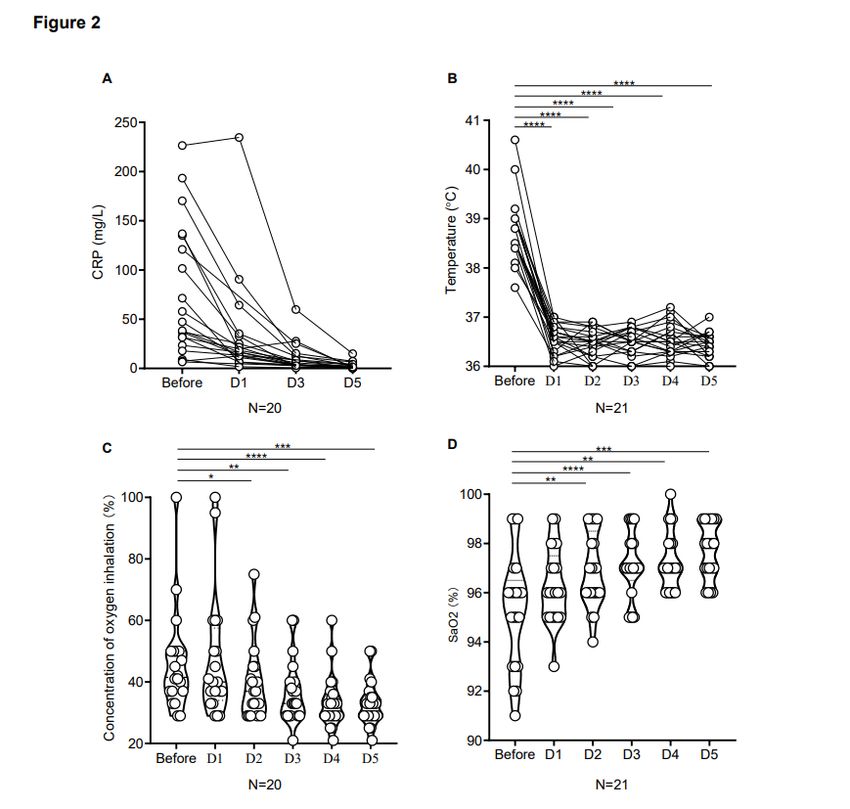
Remdesivir • Clinical trials • Compassionate use: pregnant women/children • Expanded access protocol
Remdesivir Clinical Trials: Examples
Remdesivir Clinical Data
• Report of patients Jan-
March-61 patients à 53
• 40 (75%) received the full 10-day
course of Remdesivir
• 34 (64%) ventilated at baseline
• Median duration of ventilation
prior to Remdesivir 2 days [IQR 1-8]
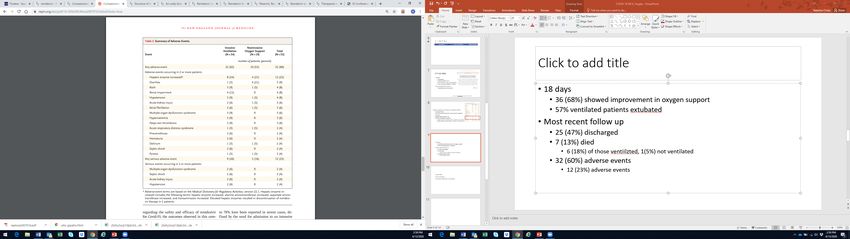
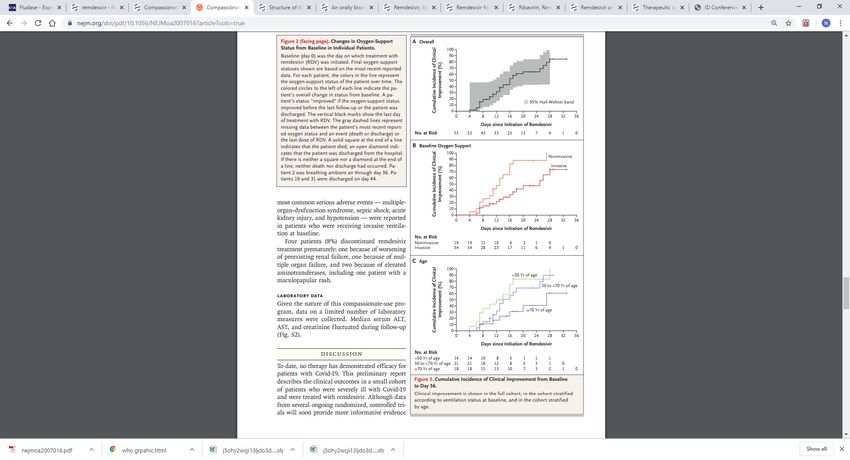
Grein J, et al. N Engl J Med. doi: 10.1056/NEJMoa2007016 (2020).Remdesivir Clinical Data
• 18 days
• 36 (68%) showed improvement in oxygen support
• 57% ventilated patients extubated
• Most recent follow up
• 25 (47%) discharged
• 7 (13%) died
• 6 (18%) of those ventilated, 1(5%) not ventilated
Grein J, et al. N Engl J Med. doi: 10.1056/NEJMoa2007016 (2020).Remdesivir Clinical Data
• 23% serious adverse events
Grein J, et al. N Engl J Med. doi: 10.1056/NEJMoa2007016 (2020).Lopinavir/Ritonavir
• In-vitro activity against SARs-CoV, MERS-CoV
• Hypothesis: inhibition of SARs/MERS protease
• Benefit in retrospective studies in SARs-CoV
• Some in vitro data SARS-CoV-2, but EC50 much
higher than levels reached in HIV dosing
• HIV protease different protease family Lopinavir/ritonavir
• Optimized to fit in a specific part of the catalytic site
of HIV protease, absent in coronaviruses
• Some benefit in animal studies MERS-CoV
• Widely used in China
• Numerous retrospective studies
Li G, De Clercq E. Nat Rev Drug Discov. 2020;19(3):149-150., Yao TT, et al. J Med Virol. doi: 10.1002/jmv.2572 (2020)., Jiang S, Hillyer C, Du L. Trends Immunol doi: 10.1016/j.it.2020.03.007 (2020)., Choy KT et
al. Antiviral Res. doi: 10.1016/j.antiviral.2020.104786 (2020).Lopinavir/ritonavir Data
• Post hoc analysis suggesting early
treatment may be efficacious
Cao B, et al. N Engl J Med. doi: 10.1056/NEJMoa2001282 (2020). , Ye XT, et al. Eur Rev Med Pharmacol Sci. 2020;24(6):3390-339Lopinavir/ritonavir Clinical Trials:
Examples
Clinicaltrials.govChloroquine Mechanisms Against
SARS-CoV-2
• Blocks viral infection by increasing
endosomal pH required for virus-
cell fusion
• Interferes with glycosylation of
SARS-CoV cellular receptors
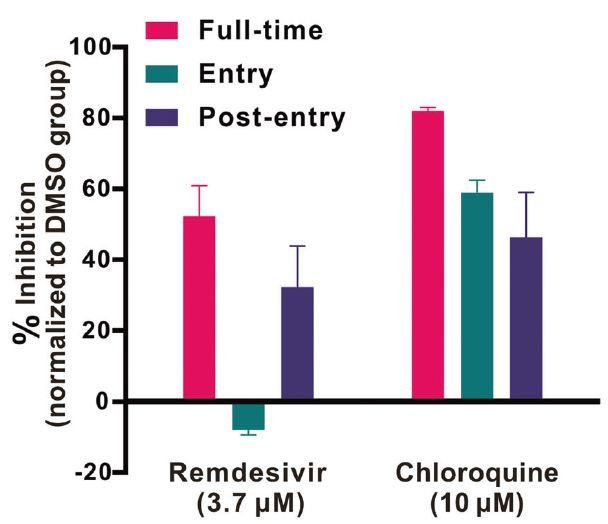
• Chloroquine interferes with entry
and post-entry stages of SARS-
CoV-2 infection in Vero E6 cells
Slide courtesy Michael Melia, MD
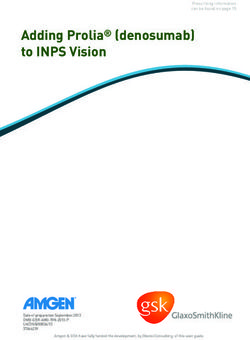
Wang M et al. Cell Research (2020) 30:269–271; https://doi.org/10.1038/s41422-020-0282-0. Vincent MJ et al. Virol J. 2005 Aug 22;2:69.Chloroquine Mechanisms Against SARS-
CoV-2
• Vero E6 cells infected with SARS-
CoV-2 at MOI 0.05
• Efficacy evaluated by quantification
of viral copy numbers in cell
supernatant by RT-PCR, confirmed
with visualization of virus
nucleoprotein expression through
immunofluorescence microscopy at
48h post-infection
• EC90 = 6.90 μM (clinically achievable)
Slide courtesy Michael Melia, MD
Wang M et al. Cell Research (2020) 30:269–271; https://doi.org/10.1038/s41422-020-0282-0.CQ versus HCQ in vitro
• Cytotoxicity in VeroE6 cells measured
• HCQ less potent than CQ at some MOI
Slide courtesy Michael Melia, MD
Liu J et al. Cell Discovery ( 2020) 6:16. https://doi.org/10.1038/s41421-020-0156-0Hydroxychloroquine Clinical Data
(Preprint)
• Randomized, parallel-group trial • Retinal disease
• Inclusion criteria: • Heart block
• Severe liver disease, including AST
• Age ≥18y >2x ULN
• SARS-CoV-2 RT-PCR positive • Pregnant or breastfeeding
• Chest CT with pneumonia • eGFR ≤30 or RRT
• SaO2:SpO2 >93% or PaO2:FiO2
>300 mm Hg
• Exclusion criteria:
• Severe, critical illness
Slide courtesy Michael Melia, MD
Chen Z. medRxiv preprint doi: https://doi.org/10.1101/2020.03.22.20040758Hydroxychloroquine Clinical Data
(Preprint)
• 62 patients • Outcomes
• 47% men • Time to clinical recovery = afebrile
• Mean age 44.7y ±15.3 and cough relief ≥72h
• Chest CT d0 vs d6
• All received standard therapy
• Initially planned PCR and T-cell
• Oxygen recovery data not reported
• Antiviral and antibacterial agents
• Immunoglobulin ± corticosteroids • HCQ: 9 no fever, 9 no cough
• Randomization to HCQ 200 mg • Control: 14 no fever, 16 no cough
BID x5d vs standard treatment
Slide courtesy Michael Melia, MD
Chen Z. medRxiv preprint doi: https://doi.org/10.1101/2020.03.22.20040758Hydroxychloroquine Clinical Data
(Preprint)
• Fever duration shorter with HCQ (2.2 ± 0.4d vs 3.2 ± 1.3d)
• Cough duration shorter with HCQ (2.0 ± 0.2d vs 3.1 ± 1.5d)
• More patients had radiographic improvement with HCQ [25/31 (81%)
vs 17/31 (55%), p=0.05]
• All 4 patients who progressed to severe illness were in control group
• 2 patients with mild adverse reactions in HCQ group (rash, HA)
Slide courtesy Michael Melia, MD
Chen Z. medRxiv preprint doi: https://doi.org/10.1101/2020.03.22.20040758Hydroxychloroquine Clinical Data
• 30 patients at a single center in China • No difference in primary endpoint
• Randomized to HCQ 400 mg daily x5d + between groups
conventional treatment or • 13/15 (87%) cases negative in HCQ group,
14/15 (93%) in control group
conventional treatment only
• Both groups received interferon • No difference in time from
• Most received umifenovir or lopinavir/ hospitalization to negative NP swab,
ritonavir fever resolution, radiographic findings,
• Primary endpoint: negative NP swab 7d diarrhea or abnormal liver enzymes
after randomization
Slide courtesy Michael Melia, MD
Chen J. J Zhejiang University. 2020:[Epub ahead of print]. https://doi.org/10.3785/j.issn.1008-9292.2020.03.03.
https://www.ashp.org/-/media/assets/pharmacy-practice/resource-centers/Coronavirus/docs/ASHP-COVID-19-Evidence-Table.ashx. Accessed 13 April 2020.HCQ + Azithromycin
• Open-label, non-randomized trial in France
• Patients aged ≥12y with NP SARS-CoV-2 carriage on admission
• Excluded: retinopathy, G6PD deficiency, QT interval prolonged, pregnancy
• HCQ 200 mg TID x10d ± azithromycin 500 mg x1 then 250 mg QD x4d
• Controls: untreated patients from another center, patients refused protocol
• NP swab VL measured daily
• End point: presence of virus at day 6 post-inclusion
Slide courtesy Michael Melia, MD
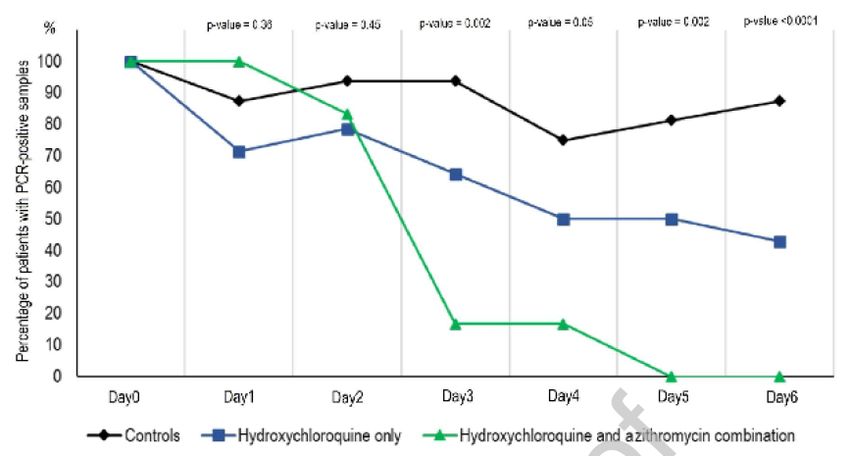
Gautret P and Lagier JC et al. Int J Antimicrob Agents (2020), doi: https://doi.org/10.1016/j.ijantimicag.2020.105949HCQ + Azithromycin
• 36* patients
• Mean age 45.1 ± 22y
• 42% (15/36) men
• 4.0 ± 2.6d between symptom onset & inclusion
• Clinical characteristics
• 8 patients with LRTI symptoms (all had evidence of pneumonia by CT scan)
• 22 patients with URTI symptoms (rhinitis, pharyngitis, fever, myalgia)
• 6 asymptomatic patients
Slide courtesy Michael Melia, MD
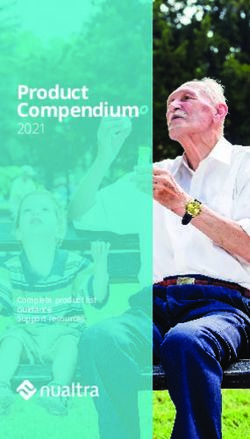
Gautret P and Lagier JC et al. Int J Antimicrob Agents (2020), doi: https://doi.org/10.1016/j.ijantimicag.2020.105949HCQ + Azithromycin
• At day 6 post-inclusion:
• 70% HCQ-treated patients
(vs 12.5% controls) tested NP
RT-PCR negative
• 100% HCQ + azithromycin-
treated patients (vs 57%
patients treated with HCQ
monotherapy) tested NP RT-
PCR negative
Slide courtesy Michael Melia, MD
Gautret P and Lagier JC et al. Int J Antimicrob Agents (2020), doi: https://doi.org/10.1016/j.ijantimicag.2020.105949HCQ + Azithromycin
• One patient treated with HCQ + azithromycin tested RT-PCR negative
at day 6 and then positive at day 8
• Patients treated with HCQ + azithromycin had lower viral RNA loads
at treatment initiation than HCQ and control groups
• Sites other than the primary site did not perform daily PCR testing
• 38% of data for control group imputed (vs 5% for treatment group)
• 6 treated patients omitted from analysis owing to ICU transfer (3),
death (1), hospital discharge (1), nausea (1)
Slide courtesy Michael Melia, MD
Gautret P and Lagier JC et al. Int J Antimicrob Agents (2020), doi: https://doi.org/10.1016/j.ijantimicag.2020.105949. Kim AHJ, Sparks JA et al. Ann Intern Med. Doi:10.7326/M20-1223HCQ + Azithromycin
• 11 consecutive patients
• 7 men, 4 women
• Mean age 59y (range 20-77)
• 8 with significant comorbidities
• HCQ 600 mg daily x10d + azithro 500 mg x1 then 250 mg QD x4d
• At treatment initiation, 10/11 had fever and were receiving oxygen
• Within 5d, one patient died, two transferred to ICU
• One course discontinued after 4d (QT 405 → 460-470)
• NP RT-PCR positive in 8/10 patients at 5-6d after treatment initiation
Slide courtesy Michael Melia, MD
Molina JM et al. Medecine et Maladies Infectieuses (2020), doi: https://doi.org/10.1016/j.medmal.2020.03.006HCQ + Azithromycin
• Case series of 80 patients at one institution
• All patients treated with HCQ 200 mg TID + azithromycin 500 mg x1 then 250 mg QD for ≥3d
& followed for ≥6d included
• Excluded: QTc >500 ms, ECG suggesting channelopathy
• HCQ 200 mg TID x10d ± azithromycin 500 mg x1 then 250 mg QD x4d
• Ceftriaxone added for pneumonia and NEWS score ≥5
• NP swab VL measured ~daily by RT-PCR
• Primary end points:
• Clinical outcome, including O2 therapy or ICU transfer after ≥3d treatment
• Contagiousness as assessed by PCR and culture
• Length of inpatient stay
Slide courtesy Michael Melia, MD
Gautret P and Lagier JC et al. https://www.mediterranee-infection.com/wp-content/uploads/2020/03/COVID-IHU-2-1.pdfHCQ + Azithromycin
• 80 patients • Clinical characteristics
• Median age 52.5y (IQR 42-62) • 54% LRTI symptoms
• 52.5% (42/80) men • 41% URTI symptoms
• 57.5% at least one chronic • 5% asymptomatic
condition • 15% had fever
• 4.9 ± 3.6d between symptom onset • 92% low NEWS score (0-4)
& treatment initiation
Slide courtesy Michael Melia, MD
Gautret P and Lagier JC et al. https://www.mediterranee-infection.com/wp-content/uploads/2020/03/COVID-IHU-2-1.pdfHCQ + Azithromycin
• 15% (12/80) received O2
• 81% (65/80) discharged
• 17% (14/80) still hospitalized
• 4% (3/80) transferred to ICU
• 1% (1/80) died
• Mean time from initiation to
hospital discharge 4.1d
• Mean LOS 4.6d
Slide courtesy Michael Melia, MD
Gautret P and Lagier JC et al. https://www.mediterranee-infection.com/wp-content/uploads/2020/03/COVID-IHU-2-1.pdfHCQ Clinical Trials: Examples
Name/Sponsor Pertinent Characteristics Estimated completion
ACTG 5396 Hospitalized Pending
ACTG 5395 Outpatients Pending
Multiple Prophylaxis trials HCWs or household contacts Ongoing
SOLIDARITY/WHO 8. Hospitalized March 2020-2022
DISCOVERY/INSERM 9. Hospitalized March 2020-2023On the Horizon
Antivirals Immune Modulators Other
Baloxavir Anakinra ACEI/ARB
Chloroquine/Hydroxychloroquine Convalescent Plasma Ascorbic Acid
DAS-181 Corticosteroids Azithromycin
Favipiravir IVIG Epoprostenol
Interferon Lenzilumab Indomethacin
Lopinavir/Ritonavir Ruxolitinib Ivermectin
Neuraminidase inhibitors Sarilumab Niclosamide
Remdesivir Sirolimus Nitazoxanide
Ribavarin Tocilizumab Statins
Umifenovir Acalabrutinib“Antiviral” Key Points
• Remdesivir has biological plausibility and in vitro data to support its
candidacy as a SARS-CoV-2 therapeutic agent
• Clinical trial data forthcoming
• Lopinavir/ritonavir has minimal supportive in vitro data in SARS-CoV-2
• Current clinical data does not support its candidacy as a SARS-CoV-2 therapeutic
agent
• Clinical trial data forthcoming
• In patients with non-severe disease, and as part of multi-component
therapy, HCQ may:
• Be associated with shorter durations of fever and cough
• Be associated with radiographic improvement
• Inadequate data to comment on impact of HCQ on viral RNA sheddingAnti IL-6 Agents
COVID-19 Cytokine Release Syndrome
• Similar to CRS seen in CART-T Therapy
• Driven by IL-6
• Anti IL-6 blockade: Tocilizumab utilized
• Like in CAR-T therapy, appears to be characterized by
• Fever
• Blood pressure abnormalities
• Progressive respiratory decline
• Elevation of certain inflammatory laboratories
• ARDS ≠ Cytokine Release Syndrome
Mehta P, et al. Lancet. 2020;395(10229):1033-1034.CRS
Moore BJB, June CH. Science. doi: 10.1126/science.abb8925
(2020).COVID-19 Clinical Course
Zhou F, et al. Lancet. 2020395(10229):1054-1062.Observational Cohorts: Published
• Retrospective observational study of
15 patients admitted to a hospital in
China
• Classified into moderately ill (13%),
seriously ill (40%), critically ill (47%)
• Median age 73 [IQR 62-80]
• Heterogeneous dosing, timing
• Half received methylprednisolone
Luo P, et al. J Med Virol. doi: 10.1002/jmv.25801 (2020).Observational Cohorts: Published
• 3 patients died (20%)
• When in clinical course did
patients receive
tocilizumab?
• Were they ARDS or
developing signs of CRS?
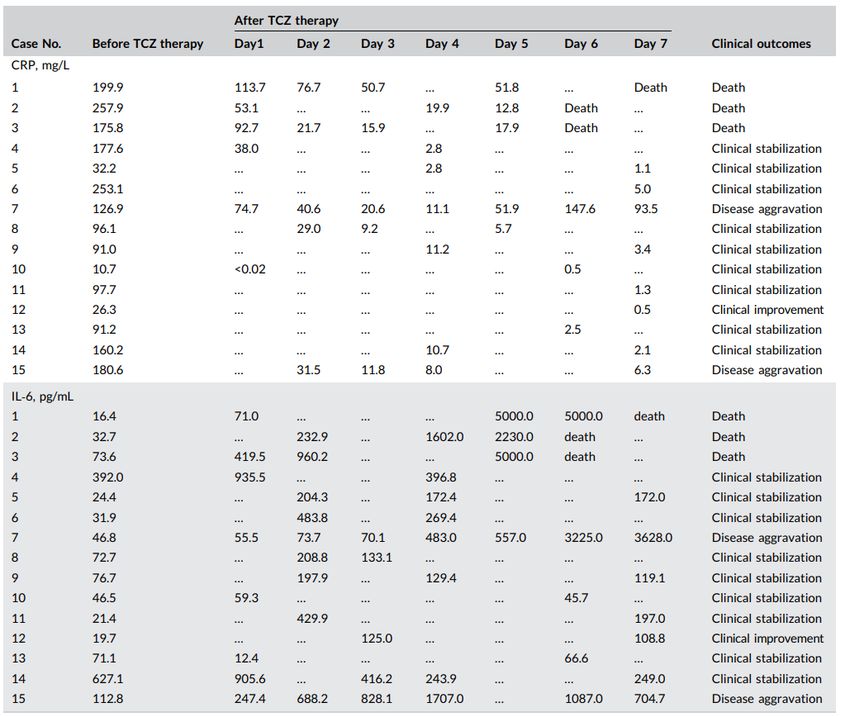
Luo P, et al. J Med Virol. doi: 10.1002/jmv.25801 (2020).Observational Cohorts: Preprint
• Retrospective observational
study of 21 patients with proven
COVID-19 admitted to 2 hospitals
in China
• Defined as
• Severe: RR ≥ 30 breaths/min, SpO2 ≤
93% on ambient air, PaO2/FiO2 ≤
300 mmHg
• Critical: Mechanical ventilation,
shock, organ failure requiring ICU
admission
• Patients received standard of care
+ tocilizumab
• Standard of care = lopinavir/
ritonavir, methylprednisolone,
oxygen
Xu X, et al. http://www.chinaxiv.org/abs/202003.00026 (Accessed 4/19/2020).Observational Cohorts: Preprint
• 19% discharged at time of paper
submission
• Based on this data National Health
Commission of China included
tocilizumab in COVID-19 therapy
recommendations
• When in clinical course did patients
receive tocilizumab?
• Were they ARDS or developing
signs of CRS?
Xu X, et al. http://www.chinaxiv.org/abs/202003.00026 (Accessed 4/19/2020).Observational Cohorts: Preprint
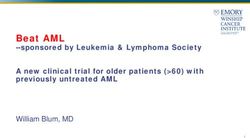
• 21 patients with COVID-19 and ARDS in Italy
• Using noninvasive ventilation
• Part of Siltuximab compassionate use program
• Median age 64 years [IQR 48-75]; 18 (85.7%) men
• Median IL-6 139.5 pg/mL, CRP 23.4 mg/dL
• Comorbidities
• Hypertension: 9 (42.3%)
• Diabetes 5: (23.8%)
• Cardiovascular disease 4 (19.1%)
• Median 3 days hospitalization prior to siltuximab
Gritti G, et al. https://www.medrxiv.org/content/10.1101/2020.04.01.20048561v2.full.pdf. Accessed 4/20/20Observational Cohorts: Preprint
Gritti G, et al. https://www.medrxiv.org/content/10.1101/2020.04.01.20048561v2.full.pdf. Accessed 4/20/20Themes Of Current Clinical Data • Outcome related to tocilizumab or natural history • Heterogeneity in patients • Variability in clinical course • Variability in administration • Dosing • Timing of administration • Concomitant use of other agents/anti-inflammatories • Heterogeneous outcomes
Anti IL-6 Clinical Trials: Examples >7 more trials between China, Europe
Anti IL-6 Key Points • Some patients with COVID-19 may develop a syndrome similar to the cytokine release syndrome seen in CAR-T therapy • Characterized by specific clinical findings and inflammatory laboratories • There is a paucity of reliable published data • Clinical trial data forthcoming • Anecdote: early administration appears more effective than late in the course of illness
Convalescent Plasma
• In the US, IND
• Clinical trials, Convalescent Plasma
expanded access,
emergency individual
use Chen Z. medRxiv preprint doi: https://doi.org/
10.1101/2020.03.22.20040758
• Current data: Case
reports/series
• Limitations: Plasma
• Study launching at JHHObjectives • Review biological plausibility of Remdesivir for SARS-CoV-2 treatment • Review clinical data on Remdesivir • Review biological plausibility of Hydroxychloroquine for SARS-CoV-2 treatment • Review clinical data on Hydroxychloroquine • Discuss cytokine release syndrome in COVID-19 • Discuss use of anti IL-6 blockade for management of CRS • State ongoing clinical trials for Remdesivir, hydroxychloroquine, IL-6 blockade
You can also read