STI Update Screening and Treatment - Leah A. Stem, MD, MSEd MUSC Department of Family Medicine 5/13/22 Evidence-Based Drug Therapy Update ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

STI Update
Screening and
Treatment
Leah A. Stem, MD, MSEd
MUSC Department of Family Medicine
5/13/22
Evidence-Based Drug Therapy Update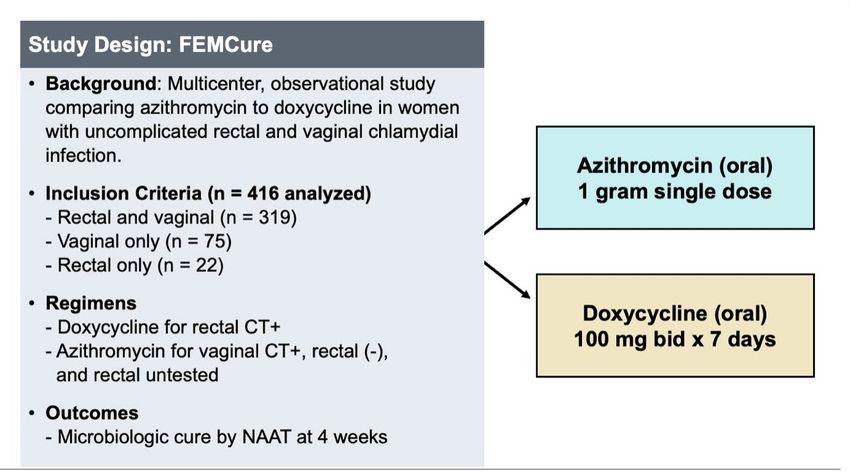
Describe new treatment approaches for
gonorrhea and chlamydia
Objectives Review STI detection for HSV and syphilis
Identify patients who are candidates for
PrEP
Contact: Stemle@musc.edu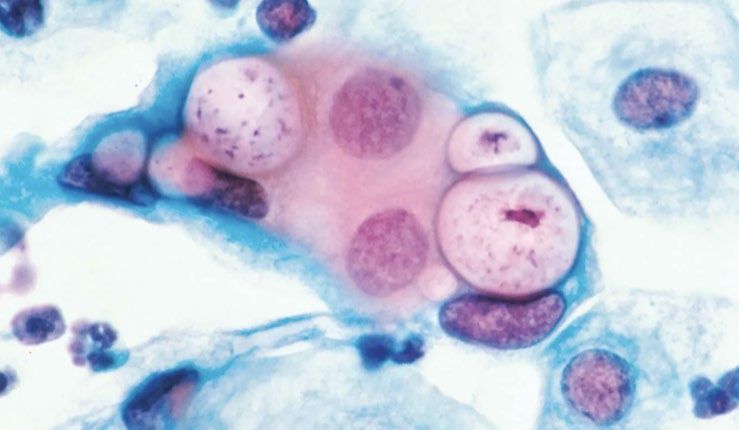
CDC Sexually Transmitted Infections (STI) Treatment Guidelines Updated evidence-based prevention, diagnosis, and treatment; 2015---> 2021 South Carolina updated legislation for expedited partner treatment Chlamydia Gonorrhea Syphillis 1.6 Million Cases/yr 677K Cases/yr 134K Cases/yr Down 1.2% Up 45% Up 52%
Chlamydia — Rates of Reported Cases by Region,
United States, 2011–2020
* Per 100,000
Gonorrhea — Rates of Reported Cases by Region,
United States, 2011–2020
* Per 100,000
Primary and Secondary Syphilis — Rates of Reported
Cases by Region, United States, 2011–2020
* Per 100,000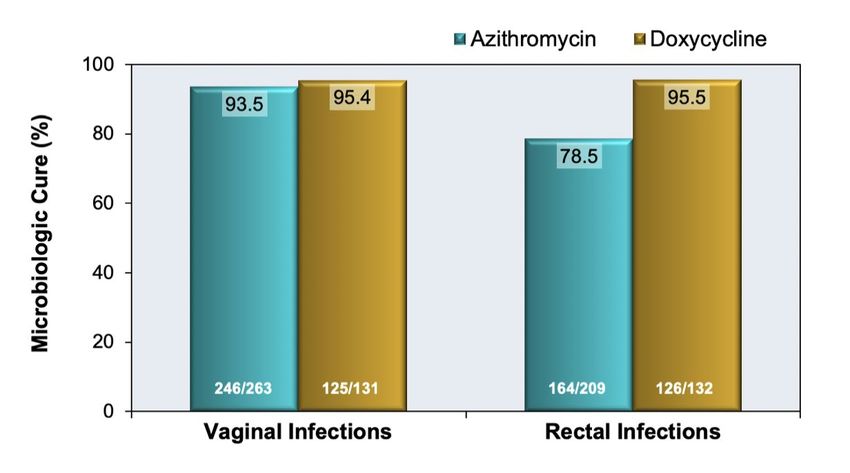
Follow updated screening and treatment
guidelines
Address STIs Utilize expedited partner treatment
as public
health issue If positive, counsel and insist on re-testing in
90 days
Promote safe sex practices: condoms, PrEP
Higher risk:
STIs are Women
present in all Ages 15-24
age groups and Men who have sex with men (MSM)
demographics Regions with high rates22yr F with no PMH establishing care for pap
smear, sexually active with 1 male partner.
She is asymptomatic and has never had STI
screening
Clinical What do you order?
Scenario Perform an STI screen:
Highest evidence: Vaginal Swab with NAAT
Gonorrhea and Chlamydia
If never performed: HIV-1,2 ab
Depending on area: Syphilis IgG IgMSerologic testing for HSV has low specificity and a high false-positive A positive test causes anxiety and disruption of personal relationships If symptomatic- unroof a lesion and obtain swab for virologic testing- HSV PCR
Syphilis Screening
The CDC now Past: screen with RPR (non-treponemal
recommends test) follow with treponemal test
screening patients (immunoassay syphilis IgG and IgM)
using a specific
treponemal test and FDA recall of RPR Test Kit due to COVID-
confirming with a 19 vaccine interference with false
non-treponemal test reactive RPR
Screening order: Syphilis IgG, IgMClinical Importance
Testing Guidelines
Treatment
Follow-up
Chlamydia and GonorrheaAsymptomatic Consequences if
Clinical untreated:
infection with manifestations:
GC or Chl is Pelvic inflammatory
common disease
among both cervicitis, urethritis,
proctitis, lower Ectopic pregnancy
men and abdominal pain, Chronic pelvic pain
women dyspareunia Infertility
Epididymitis
Peri-HepatitisScreening CDC and USPSTF
for
Gonorrhea •Annual Screen: sexually
and active women < 25yrs old
Chlamydia
CDC
•Annual screen: in MSMWomen > 25yrs old?
Continue annual screen if increased risk:
Screening new sex partner, more than one sex
for partner, exchanging sex for money or drugs
Gonorrhea
and Men?
Chlamydia Consider annual screen in clinical settings with
a high prevalence of chlamydia:
adolescent clinics, correctional facilities, or STD
specialty clinicsGuidelines for MSM
Annual screen for GC/Chl
Screening Site specific- urethral, rectal, pharyngeal
for “triple site screen”
Gonorrhea
and
Chlamydia Self collected swab at any site just as reliable as
provider collectedUse molecular based testing techniques
Nucleic Acid Amplification Tests (NAAT) preferred testing method
High sensitivity, very high specificity
Multiple NAATs are FDA cleared for use on
Urine specimens
Urethral secretions
Endocervical swab
Some cleared for vaginal swab
Aptima Combo 2 Assay and Xpert/Ct/NG cleared for pharynx and rectumFor urogenital infections, optimal specimen types for screening GC/Chl using NAATs include: Men: first-void urine for men (“dirty” urine, prior to cleansing) Women: vaginal swab (slightly more sensitive than urine) Current studies and some evidence on acceptability for diagnosis of GC/Chl from clean catch urine in adolescents with dysuria Pickett et al. Journal of Adolescent Health 2021
Treatment of +Chlamydia test result, asymptomatic or uncomplicated 2015: Azithromycin 1g PO once 2021 Update: Doxycycline 100mg PO BID x7 days
Lau et al. New Engl J Med. 2021
Lau et al. New Engl J Med. 2021
Treatment of a +Chlamydia test result
Recommended:
Doxycycline 100mg PO BID for 7 days
Alternative:
Azithromycin 1g orally single dose
Levofloxacin 500mg PO daily for 7 days
Pregnant:
Azithromycin 1g orally single doseDue to antimicrobial resistance concerns, the treatment recommendations for gonorrhea have recently changed.
Treatment of +Gonorrhea test result, asymptomatic
or uncomplicated
Ceftriaxone Azithromycin 1g
2015: 250mg IM PO
No need for dual therapy for
Increase dose of Gonorrhea; may be needed for
2021 Update:
ceftriaxone Chlamydia txRecommended Treatment for Gonorrhea Patients 150kg Ruled out chlamydia- no further medications needed Unknown chlamydia or +chlamydia: Treat with doxycycline 100mg BID x 7 days
Alternative Treatment Regimens for Gonorrhea
Hx IgE-mediated Gentamicin Azithromycin 2g
analphylaxis to 240mg IM PO
PCN
Unavailable for IM Cefixime 800mg
PO Single DoseGonococcal Isolate Surveillance Project (GISP)
monitors for drug resistant Gonorrhea
The higher the minimum inhibitory
concentrations (MIC) in clinical
isolates, the greater the antimicrobial
concentration needed to inhibit
growth of N. gonorrhea
GISP tracks trends to 7 microbials:
Azithromycin, Cefixime, Ceftriaxone,
Ciprofloxacin, Gentamicin, Penicillin,
TetracyclineGISP Outcomes
Azithromycin
2010-2013: 5% isolates reduced susceptibility
2019: in MSM 8.8% isolates with reduced susceptibilityGISP Outcomes Ceftriaxone 2009-2018:
GISP Outcomes Cefixime 2010: isolates with reduced susceptibility (MIC ≥0.25 μg/mL) peaked in 2010 at 1.4% 2011-2019:
GISP Outcomes Ciprofloxacin 2019: 35.4% isolates resistant Penicillin 2019: 12.8% isolates resistant Tetracycline 2019: 27.8% of isolates resistant
+Chlamydia
Recommended: Doxycycline 100mg BID PO x 7 days
Treatment Alternative: Azithromycin 1g PO once OR
summary Levofloxacin 500mg PO for 7 days
+Gonorrhea
Recommended: 150kg 1g Ceftriaxone IM once
Alternative: Cefixime 800mg PO single dose
PCN allergy: Gentamicin 240mg IM once + Azithro 2g
PO onceCounseling for positive STI diagnosis
It is important that all of your sexual partners in the prior 60 days
are tested and treated
Do not have sex of any kind for 7 days
If your sexual partners is positive for an STI, you must not have
sex with them until 7 days after treatment
You need to be re-tested for Gonorrhea and Chlamydia in 90 daysTesting positive for an STI is an indication for
offering Pre-Exposure Prophylaxis for HIV (PrEP)
PrEP decreases transmission of HIV >90%
Prior to prescribing:
Exclude acute or chronic HIV infection
Test for HBV and HCV
Assess renal function
• Not recommended for Cr ClEvery 3 months
After • Perform HIV testing
prescribing • Test for pregnancy
• Test for STIs if necessary
PrEP
At 6 months
• Test renal function
Every time:
• Encourage condom useExpedited Partner Therapy
Expedited (EPT)
Partner Therapy
Treats the sex partners of
(EPT) decreases patients diagnosed with
rate of recurrent chlamydia or gonorrhea
or persistent STI
Provides prescriptions or
medications to the patient to
take to his/her
partner without the health
care provider first examining
the partnerAccording to CDC data from 2018,
per capita, South Carolina ranks 4th
Issued “Post-Exposure in the nation in cases of chlamydia
Prophylaxis Policy” allowed EPT and 3rd in cases of gonorrhea
2011 2012 2018 Feb. 2021
“Establishment of Physician- Updated interpretation of
Patient Relationship as S.C. Code Ann. § 40-47-
Prerequisite to Prescribing 113(B) to allow for the use of
Drugs” ; rescinded EPT EPT.Expedited Partner Therapy: Patient
Write a separate prescription with name
diagnosed with STI delivers treatment
and info or just “EPT”
or the prescription to a recent sex
partner
NOT giving a refill to index patient
Recommended for all partners within the
last 60 days
Give a written document on exposure,
medication, signs of complications,
possible allergic reactions and adverse
effects
Decreases rate of recurrent or
persistent STIsExpedited Partner Therapy: Patient
Contraindications to EPT
diagnosed with STI delivers treatment
or the prescription to a recent sex
For female partner with signs of partner
symptoms of PID
Partner needs prompt evaluation and
possibly extended regimen
May be inappropriate
Use EPT in MSM on a shared decision
basis
High risk for co-existing infections
(HIV, syphilis) that could get tested at a
clinic visitFor sexual partners of patient with:
+Chlamydia
Doxycycline 100mg PO BID x 7 days*
+Gonorrhea
Cefixime 800mg PO as a single dose
EPT regimens
+GC and Chl OR Chlamydia result unavailable
Cefixime 800mg PO as a single dose, +
Doxycycline 100mg PO BID x 7 days*
*if concern for taking multiple doses, can give
Azithromycin 1g PO single doseTreatment should be initiated for sexually
active young women and other women at risk
for STIs if they are experiencing
Pelvic or lower abdominal pain
Presumptive
Treatment: No cause for the illness other than PID can be
PID identified
If one or more of the following three clinical
criteria are present on pelvic examination:
cervical motion tenderness, uterine
tenderness, or adnexal tenderness.Presumptive Treatment: PID Negative endocervical screening for GC/Chl does not rule out upper genital tract infection Recommended empiric treatment Ceftriaxone 500mg IM single dose + Doxycycline 100mg PO BID x 14 days + Metronidazole 500mg orally x14 days Reassess in 72 hours, admit for parenteral therapy if no improvement
EPT of PID patient Treat empirically with regimens effective against both C. trachomatis and N. gonorrhoeae, regardless of index patient testing results Coverage for GC and Chl: Cefixime 800mg PO as a single dose + Doxycycline 100mg PO BID x 7 days
Describe new treatment approaches for
gonorrhea and chlamydia
Objectives Review STI detection for HSV and syphilis
Identify patients who are candidates for
PrEP
Contact: Stemle@musc.eduReferences David H. Spach, MD, Stephen Jordan MD, PhD. Chlamydia Infections. National STD Curriculum. 2022. https://www.std.uw.edu/go/comprehensive-study/chlamydial-infections/core-concept/all David H. Spach, MD. Gonorrhea Infection. National STD Curriculum. 2022. https://www.std.uw.edu/go/comprehensive-study/gonococcal- infections/core-concept/all Dombrowski JC, Wierzbicki MR, Newman LM, Powell JA, Miller A, Dithmer D, Soge OO, Mayer KH. Doxycycline Versus Azithromycin for the Treatment of Rectal Chlamydia in Men Who Have Sex With Men: A Randomized Controlled Trial. Clin Infect Dis. 2021 Sep 7;73(5):824-831. doi: 10.1093/cid/ciab153. PMID: 33606009; PMCID: PMC8571563 Lau A, Kong FYS, Fairley CK, Templeton DJ, Amin J, Phillips S, Law M, Chen MY, Bradshaw CS, Donovan B, McNulty A, Boyd MA, Timms P, Chow EPF, Regan DG, Khaw C, Lewis DA, Kaldor J, Ratnayake M, Carvalho N, Hocking JS. Azithromycin or Doxycycline for Asymptomatic Rectal Chlamydia trachomatis. N Engl J Med. 2021 Jun 24;384(25):2418-2427. doi: 10.1056/NEJMoa2031631. PMID: 34161706. Michelle L. Pickett, Alexis Visotcky, Ruta Brazauskas, Nathan A. Ledeboer, Amy L. Drendel. Can a Clean Catch Urine Sample Be Used to Diagnose Chlamydia and Gonorrhea in Adolescent Females?. Journal of Adolescent Health. Volume 69, Issue 4, 2021 Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep 2021;70(No. RR-4):1–187. DOI: http://dx.doi.org/10.15585/mmwr.rr7004a1external icon
Which one of the following is the recommended therapy for a positive
Chlamydia trachomatous result in a nonpregnant adult?
A. Doxycycline 100mg orally twice a day for 7 days
B. Azithromycin 500mg orally once a day for 5 days
C. Ceftriaxone 1g IM once
D. Metronidazole 500mg orally BID for 7 daysWhich one of the following statements is true for recommendations for managing the sex partners of a person diagnosed with gonorrhea with EPT? A. Only the most recent sex partner needs treatment B. Only symptomatic partners need treatment C. All sex partners during the 60 days preceding the onset of symptoms should receive treatment D. All sex partners during the 365 days preceding the onset of symptoms should be treated
You can also read

















































